The Health Justice Initiative today reported an important court victory in their attempts to lift the veil of of secrecy over government’s vaccine procurement contracts. The result is a court ruling which orders the Department of Health to disclose these contracts, which will shed light on important questions such as whether these vaccines were purchased at inflated prices and unfavourable terms. They detail the court victory in a press release:
Health Justice Initiative v The Minister of Health and Information Officer, National Department of Health (Case no 10009/22).
Today, South African courts upheld the principles of transparency and accountability when our government procures health services using public funds. The Pretoria High Court ruled in our favour in our bid to compel the National Department of Health to provide access to the COVID-19 vaccine procurement contracts. The Court ordered (per Millar J) that all COVID-19 vaccine contracts must be made public within 10 days.
This is a massive victory for transparency and accountability. The contracts concern substantial public funds, and the contracting process has been marred by allegations that the government procured vaccines at differential, comparatively inflated prices and that the agreements may contain onerous and inequitable terms including broad indemnification clauses, export restrictions, and non-refundability clauses.
This significant moment comes as we begin to emerge from the devastation of the COVID-19 pandemic. It sets an important precedent, especially as our government pursues National Health Insurance (NHI). With increasing reports of corruption within the healthcare sector, we cannot have a healthcare system shrouded in secrecy. Procurement must be held in check, as it will involve powerful multinational companies, particularly from the pharmaceutical industry.
The secrecy surrounding COVID-19 vaccine procurement at the height of the pandemic continues to be a global issue, not just limited to SA – it is important to know what was agreed to in our name at the behest of powerful vaccine manufacturers who have been reported to have bullied governments in the Global South especially, insisting on contracts that ultimately made them huge profits, without maximum accountability and openness. Therefore, this judgment can be leveraged by other countries to demand open contracting in their jurisdictions.
We believe that in the current Pandemic Treaty negotiations, where worrying attempts are being made to water down transparency, this judgment will support Pandemic Preparedness measures by bolstering provisions on transparency and accountability in these negotiations.
This case demonstrates that all governments should and can be held accountable when spending public funds, this also includes the parties it entered into contracts with. It is in the public interest to know what was agreed to. The judgment has affirmed that today.
We look forward to the Department of Health’s cooperation by making available all the records HJI requested within the time period set out in the judgment (10 court days from 17 August 2023).
Scanning electron micrograph of human respiratory syncytial virus (RSV) virions (colourised blue) and labelled with anti-RSV F protein/gold antibodies (colourised yellow) shedding from the surface of human lung epithelial A549 cells.
Credit: National Institute of Allergy and Infectious Diseases, National Institutes of Health (NIH)
Respiratory syncytial virus (RSV) is a dangerous early childhood viral infection, but results of a vaccine trial promise to change things radically.
A new study published in the New England Journal of Medicine, the world’s most prestigious medical journal, on 5 April that examined the effect of an RSV vaccine on pregnant women found that it reduced the risk of severe lower respiratory tract infections in newborns by 82%.
RSV is the most common cause of acute lower respiratory infection – or pneumonia – in infants. Globally, it was responsible for just over 100,000 deaths (with a lower bound of 84,000 deaths and an upper bound of 126,000 deaths) of children under five in 2019. Of these deaths 45% were infants (younger than six months), and nearly all deaths occurred in lower income countries (half in Africa alone). In an article in Spotlight in June 2022, Professor Cheryl Cohen, head of the Centre for Respiratory Diseases and Meningitis at the National Institute for Communicable Diseases (NICD), said that, pre-COVID, RSV led to 44 615 hospitalisations and 490 deaths in children under five each year in South Africa.
RSV causes cold-like symptoms, but can lead to severe symptoms like pneumonia. At present, there is no licensed RSV vaccine, though the virus was first identified in the 1960s.
The study was a phase three, double-blind trial (which compares a new treatment to standard care, and leads the way to regulatory approval and production) conducted in 18 countries, led by Beate Kampmann, Professor of Paediatric Infection and Immunity at the London School of Hygiene and Tropical Medicine, Shabir Madhi, Dean of the Faculty of Health Sciences and Professor of Vaccinology at the University of the Witwatersrand, and Iona Munjal, Director of Clinical Research & Development at Pfizer. It builds on earlier work by Madhi and others.
Women who were between 24 and 36 weeks pregnant were given an injection of a protein–based vaccine (RSVpreF) and a placebo. Pregnant women can passively transfer their immunity to viruses and diseases to their foetuses in utero.
They were then monitored to see if they suffered a severe RSV-associated lower respiratory tract illness that required medical attention, and if their newborns required medical attention for RSV-associated lower respiratory tract illness up to six months after birth.
A total of 7,358 women participated across the two trial groups, and 7,128 babies were monitored, and no safety concerns were identified over the course of the trial.
In November last year, Pfizer announced that it planned to submit a licence application to the US Food and Drug Administration after trials showed that the vaccine was highly effective at reducing severe RSV cases in the first 90 days of an infant’s life.
In a Twitter thread announcing the results, Madhi said that the next challenge would be to ensure that the vaccine is licensed across lower income countries, where most infant RSV deaths occur. Madhi said that there is a “moral responsibility on pharma to licence [the RSV] vaccine in LMIC [Lower and Middle Income Countries] at [an] affordable price.” Governments in poorer countries, “need to act to protect children in their counties by funding and deploying the vaccine timeously,” he said.
Madhi also informed GroundUp that coincidentally in the same issue of the New England Journal of Medicine, a medicine called nirsevimab was found to protect infants against RSV-associated hospitalisation and severe lower respiratory tract infections. Madhi and his team at Wits also participated in this trial.
This medicine is “administered as a single dose at the onset of RSV season,” Madhi explained. “The two approaches [the vaccine and nirsevimab] will be complementary.”
A new way to significantly increase the potency of almost any vaccine has been developed by researchers from the International Institute for Nanotechnology (IIN) at Northwestern University, which they describe in Nature.
The scientists used chemistry and nanotechnology to change the structural location of adjuvants and antigens on and within a nanoscale vaccine, greatly increasing vaccine performance. The antigen targets the immune system, and the adjuvant is a stimulator that increases the effectiveness of the antigen.
“The work shows that vaccine structure and not just the components is a critical factor in determining vaccine efficacy,” said lead investigator Chad A. Mirkin, director of the IIN. “Where and how we position the antigens and adjuvant within a single architecture markedly changes how the immune system recognises and processes it.”
This new heightened emphasis on structure has the potential to improve the effectiveness of conventional cancer vaccines, which historically have not worked well, Mirkin said.
Mirkin’s team has studied the effect of vaccine structure in the context of seven different types of cancer to date, including triple-negative breast cancer, papillomavirus-induced cervical cancer, melanoma, colon cancer and prostate cancer to determine the most effective architecture to treat each disease.
Conventional vaccines take a blender approach
With most conventional vaccines, the antigen and the adjuvant are simply blended and injected into a patient, giving no control over the vaccine structure, and, consequently, limited control over trafficking and processing of the vaccine components. Thus, there is no control over how well the vaccine works.
“A challenge with conventional vaccines is that out of that blended mish mosh, an immune cell might pick up 50 antigens and one adjuvant or one antigen and 50 adjuvants,” said study author and former Northwestern postdoctoral associate Michelle Teplensky, who is now an assistant professor at Boston University. “But there must be an optimum ratio of each that would maximise the vaccine’s effectiveness.”
Enter SNAs (spherical nucleic acids), which are the structural platform, invented and developed by Mirkin, used in this new class of modular vaccines. SNAs allow scientists to pinpoint exactly how many antigens and adjuvants are being delivered to cells. SNAs also enable scientists to tailor how these vaccine components are presented, and the rate at which they are processed. Such structural considerations, which greatly impact vaccine effectiveness, are largely ignored in conventional approaches.
Vaccines developed through ‘rational vaccinology’ offer precise dosing for maximum effectiveness
Mirkin came up with this approach to systematically control antigen and adjuvant locations within modular vaccine architectures, and called it ‘rational vaccinology’. It is based on the concept that the structural presentation of vaccine components matters as much as the components themselves in driving efficacy.
“Vaccines developed through rational vaccinology deliver the precise dose of antigen and adjuvant to every immune cell, so they are all equally primed to attack cancer cells,” said Mirkin. “If your immune cells are soldiers, a traditional vaccine leaves some unarmed; our vaccine arms them all with a powerful weapon with which to kill cancer. Which immune cell ‘soldiers’ do you want to attack your cancer cells?”
Building an (even) better vaccine
The team developed a cancer vaccine that reduced tumour growth by more than four times compared to checkpoint inhibitor monotherapy, and led to a 40% extension in median survival.
By reconfiguring the architecture of a vaccine containing multiple targets, the SNA enables the immune system to find tumour cells. The team investigated differences in how well two antigens were recognised by the immune system depending on their placement, on the core or perimeter, of the SNA structure. For an SNA with optimum placement, they could increase the immune response and how quickly the nanovaccine triggered cytokine (an immune cell protein) production to boost T cells attacking the cancer cells. The scientists also studied how the different placements affected the immune system’s ability to remember the invader, and whether the memory was long-term.
“Where and how we position the antigens and adjuvant within a single architecture markedly changes how the immune system recognises and processes it,” Mirkin said.
The most powerful structure throws two punches to outsmart the tumour
The study data show that attaching two different antigens to an SNA comprising a shell of adjuvant was the most potent approach for a cancer vaccine structure. These engineered SNA nanostructures stalled tumour growth in multiple animal models.
“It is remarkable,” Mirkin said. “When altering the placement of antigens in two vaccines that are nearly identical from a compositional standpoint, the treatment benefit against tumours is dramatically changed. One vaccine is potent and useful, while the other is much less effective.”
Many current cancer vaccines are designed to primarily activate cytotoxic T cells, only one defence against a cancer cell. Because tumour cells are always mutating, they can easily escape this immune cell surveillance, quickly rendering the vaccine ineffective. The odds are higher that the T cell will recognise a mutating cancer cell if it has more antigens to recognise it.
“You need more than one type of T cell activated, so you can more easily attack a tumour cell,” Teplensky said. “The more types of cells the immune system has to go after tumours, the better. Vaccines consisting of multiple antigens targeting multiple immune cell types are necessary to induce enhanced and long-lasting tumour remission.”
Another advantage of the rational vaccinology approach, especially when used with a nanostructure like an SNA, is that it’s easy to alter the structure of a vaccine to go after a different type of disease. Mirkin said they simply switch out a peptide, a snippet of a cancer protein with a chemical handle that “clips” onto the structure, not unlike adding a new charm to a bracelet.
Towards the most effective vaccine for any cancer type
“The collective importance of this work is that it lays the foundation for developing the most effective forms of vaccine for almost any type of cancer,” Teplensky said. “It is about redefining how we develop vaccines across the board, including ones for infectious diseases.”
In a previously published paper, Mirkin, Teplensky and colleagues demonstrated the importance of vaccine structure for SARS-CoV-2 by creating vaccines that exhibited protective immunity in 100% of animals against a lethal viral infection.
“Small changes in antigen placement on a vaccine significantly elevate cell-to-cell communication, cross-talk and cell synergy,” Mirkin said. “The developments made in this work provide a path forward to rethinking the design of vaccines for cancer and other diseases as a whole.”
More than 600 000 people worldwide still die from malaria every year, according to the WHO. The vast majority of fatal cases of malaria are caused by the single-celled pathogen Plasmodium falciparum, which so far has only one approved vaccine against it, and its efficacy, which is already rather low, is also short-lived. A new study in Science Immunology may have the explanation: a lack of cross-reactivity in T helper cells.
The vaccine targets CSP, the quantitatively dominant protein on the surface of the “sporozoites”. Sporozoites are the stage of the malaria pathogen which is transmitted with the bite of the mosquito and enters human blood. “To improve the vaccine, we need to understand which protective antibodies are induced by the immunisation. But the production of such antibodies depends to a large extent on help from the so-called follicular T helper cells,” explained Dr Hedda Wardemann, immunologist and senior author of the study. “They ensure that B cells transform into antibody-producing plasma cells and memory B cells.”
To study the T helper cell response against CSP in detail, Dr Wardemann’s team examined the blood of volunteers infected with killed P. falciparum sporozoites from the vaccine strain. The volunteers were of European descent and had no prior contact with malaria pathogens. The researchers analysed the induced Plasmodium-specific follicular T helper cells at the single cell level. They focused on which sequences of CSP are recognised by the T helper cells’ receptors.
The analyses revealed that the T-cell receptors mainly targeted amino acids 311 to 333 of the CSP. But the researchers were stunned by another finding: there was virtually no cross-reactivity between the individual T-cell clones. “The receptors highly specifically bind only the CSP epitopes of the vaccine strain used. Even deviations of only a single amino acid component were not tolerated in some cases,” Dr Wardemann explained.
The immunologist points out that in the natural population of P. falciparum, sequence polymorphisms occur to a high degree in this region of the CSP. “The specificity of the T-cell clones prevents the constantly recurring natural infections with the pathogen from acting as a natural ‘booster.’ This could possibly explain why the protective effect of the malaria vaccine wears off so quickly,” Dr Wardemann said. The researcher recommends that further development of the vaccine should test whether inducing a broader spectrum of T helper cells could generate longer-lasting immune protection.
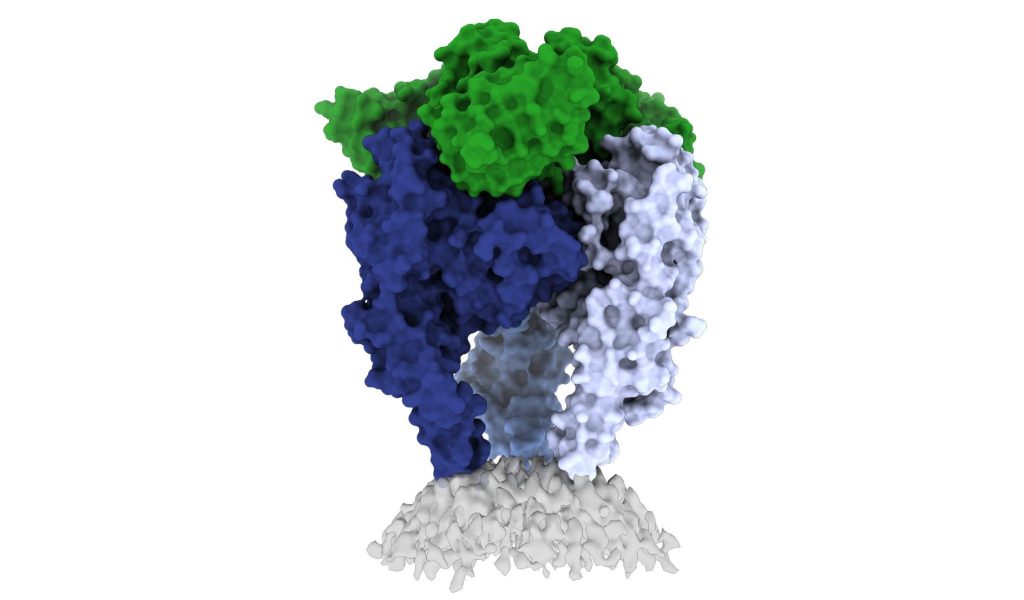
Scientists from La Jolla Institute for Immunology and the Institut Pasteur have shed light on the structure of the rabies virus glycoprotein, seen here. Credit: Heather Callaway, Ph.D., LJI
In a new study, researchers from La Jolla Institute have unveiled one of the first high-resolution looks at the rabies virus glycoprotein in its vulnerable ‘trimeric’ form. These new images, published in Science Advances, may open up a new vaccine for the deadly virus.
The CDC estimates that 59 000 people die from rabies virus every year, with 40% of those bitten by rabid animals being under 15. Some victims, especially kids, don’t realise they’ve been exposed until it is too late. The intense rabies treatment regimen is not widely available and the average $3800 is out of the reach of less well-off families.
Rabies vaccines, rather than treatments, are much more affordable and easier to administer. But according to Professor Erica Ollmann Saphire, PhD, of the La Jolla Institute, lead researcher of the new study, those vaccines also come with a massive downside.
“Rabies vaccines don’t provide lifelong protection. You have to get your pets boosted every year to three years,” she said. “Right now, rabies vaccines for humans and domestic animals are made from killed virus. But this inactivation process can cause the molecules to become misshapen – so these vaccines aren’t showing the right form to the immune system. If we made a better shaped, better structured vaccine, would immunity last longer?”
“The rabies glycoprotein is the only protein that rabies expresses on its surface, which means it is going to be the major target of neutralising antibodies during an infection,” said LJI Postdoctoral Fellow Heather Callaway, PhD, the study’s first author.
“Rabies is the most lethal virus we know. It is so much a part of our history – we’ve lived with its spectre for hundreds of years,” added Prof Saphire. “Yet scientists have never observed the organisation of its surface molecule. It is important to understand that structure to make more effective vaccines and treatments – and to understand how rabies and other viruses like it enter cells.”
Shapeshifting Rabies virus evades antibodies
Why rabies vaccines don’t provide long-term protection is still unclear, but they do know that its shape-shifting proteins are a problem.
The rabies glycoprotein has sequences that unfold and flip upward when needed, like a Swiss Army knife. The glycoprotein can shift back and forth between pre-fusion (before fusing with a host cell) and post-fusion forms. It can also come apart, changing from a trimer structure (where three copies come together in a bundle) to a monomer (one copy by itself).
This shapeshifting can make rabies invisible to human antibodies, which are built to recognise a single site on a protein. They cannot follow along when a protein transforms to hide or move those sites.
The new study gives scientists a critical picture of the correct glycoprotein form to target for antibody protection.
Capturing the glycoprotein at last
Over the course of three years, Callaway worked to stabilise and freeze the rabies glycoprotein in its pre-fusion form.
Callaway paired the glycoprotein with a human antibody, which helped her pinpoint one site where the viral structure is vulnerable to antibody attacks. The researchers then captured a 3D image of the glycoprotein using cutting-edge cryo-electron microscope equipment at LJI.
The new 3D structure highlights several key features researchers hadn’t seen before. Importantly, the structure shows the fusion peptides, the way they appear in real life. These two important sequences link the bottom of the glycoprotein to the viral membrane, but project into the target cell during infection. Getting stable image of these sequences is challenging: other rabies researchers have had to cut them off to try to get images of the glycoprotein.
Dr Callaway solved this problem by capturing the rabies glycoprotein in detergent molecules. “That let us see how the fusion sequences are attached before they snap upward during infection,” said Prof Saphire.
Now that scientists have a clear view of this viral structure, they can better design vaccines to create antibodies with a better picture of the targt.
“Instead of being exposed to four-plus different protein shapes, your immune system should really just see one – the right one,” said Dr Callaway. “This could lead to a better vaccine.”
Preventing a family of viruses
More images are needed of rabies virus and its relatives together with neutralising antibodies, and could reveal common antibody targets for lyssaviruses, which can also infect humans and animals. According to Dr Callaway, scientists are working on solving several of these structures, which could reveal antibody targets that lyssaviruses have in common.
“Because we didn’t have these structures of the rabies virus in this conformational state before, it’s been hard to design a broad-spectrum vaccine,” Dr Callaway said.
Scanning Electron Micrograph image of a human T cell. Credit: NIH/NIAID
In a groundbreaking new study, scientists report training T cells to protect against SARS-CoV-2 even without an antibody response. This could open the way to more broadly effective vaccines.
Current vaccines prompt the creation of antibodies and immune cells that recognise the spike protein. However, these vaccines were developed using the spike protein from an older variant of SARS-CoV-2, reducing their effectiveness against newer variants. Researchers have found that immune cells called T cells tend to recognise parts of SARS-CoV-2 that don’t mutate rapidly. T cells coordinate the immune system’s response and kill cells that have been infected by the SARS-CoV-2 virus.
A vaccine that prompted the body to create more T cells against SARS-CoV-2 could help prevent disease caused by a wide range of variants. To explore this approach, a research team led by Dr Marulasiddappa Suresh from the University of Wisconsin studied two experimental vaccines that included compounds to specifically provoke a strong T-cell response in mice.
The team tested the vaccines’ ability to control infection and prevent severe disease caused by an earlier strain of SARS-CoV-2 as well as by the Beta variant, which is relatively resistant to antibodies raised against earlier strains.
When the researchers vaccinated the mice either either nasally or by injection, the animals developed T cells that could recognise the early SARS-CoV-2 strain and the Beta variant. The vaccines also caused the mice to develop antibodies that could neutralise the early strain. However, they failed to create antibodies that neutralised the Beta variant.
The mice were exposed to SARS-CoV-2 around 3 to 5 months after vaccination. Compared to the controls, vaccinated mice had very low levels of virus in their lungs and were protected against severe illness, which was true of infection with the Beta variant too. This showed that the vaccine provided protection against the Beta variant despite failing to produce effective antibodies against it.
To understand which T cells were providing this protection, the researchers selectively removed different types of T cells in vaccinated mice prior to infection. When they removed CD8 (killer) T cells, vaccinated mice remained well protected against the early strain, although not against the Beta variant. When they blocked CD4 T (helper) cells, levels of both the early strain and Beta variant in the lungs and severity of disease were substantially higher than in vaccinated mice that didn’t have their T cells removed.
These results suggest important roles for CD8 and CD4 T cells in controlling SARS-CoV-2 infection. Current mRNA vaccines do produce some T cells that recognize multiple variants. This may help account for part of the observed protection against severe disease from the Omicron variant. Future vaccines might be designed to specifically enhance this T cell response.
“I see the next generation of vaccines being able to provide immunity to current and future COVID variants by stimulating both broadly-neutralising antibodies and T cell immunity,” Dr Suresh predicted.
In a news release, pharma giant Aspen has announced that it has concluded an agreement with Johnson & Johnson to manufacture an Aspen-branded COVID vaccine, Aspenovax, and to make it available throughout Africa.
This follows on from the November 2021 announcement of an agreement of terms between the two companies. This new agreement will expand the existing technical transfer and manufacturing agreements between the companies.
The agreement will grant Aspen’s South African subsidiary the rights to manufacture finished Aspenovax product from drug substance supplied by J&J. It will also make Aspenovax available to markets in Africa through transactions with designated multilateral organisations and with national governments of member states of the African Union.
Under the agreement, Aspen has secured the necessary intellectual property from Johnson & Johnson for production. There is also a good faith undertaking between the companies to expand the agreement to cover any new versions of the drug substance, such as those developed for new variants or a different formulation for administration as a booster.
The agreement will last through to the end of 2026.
Commenting on this agreement, Dr Matshidiso Moeti, World Health Organization Regional Director for Africa said: “This important agreement on sharing know-how and technologies for the production of COVID vaccines is a huge leap forward towards realising our shared vision for medicines and vaccines to be manufactured on the African soil for the African people. Vaccines are our best way out of this pandemic and local production is an essential recipe for our success.”
Stephen Saad, Aspen Group Chief Executive said: “Even with all the support in the world, none of this would be possible without the competence of our teams at Gqeberha. They knew the weight of a continent’s ambitions rested on their shoulders. They persevered and succeeded in becoming a significant supplier within the Johnson & Johnson network. Aspenovax has become a reality due to the confidence placed in their abilities. They are our African heroes.”
Researchers have found that a 90 minute bout of mild- to moderate-intensity exercise directly after a receiving a flu or COVID vaccine may provide an extra immune boost.
In the paper, published in Brain, Behavior, and Immunity, participants who cycled on a stationary bike or took a brisk walk for an hour-and-a-half after receiving a vaccine injection produced more antibodies in the following four weeks compared to participants who sat or continued with their daily routine post-immunisation. When the researchers ran the experiment with mice and treadmills, similar results were observed.
“Our preliminary results are the first to demonstrate a specific amount of time can enhance the body’s antibody response to the Pfizer-BioNtech COVID vaccine and two vaccines for influenza,” said Kinesiology Professor Marian Kohut, lead author of the study.
The vaccine recipients would be able to benefit people who could not cope with such exercise. Nearly half of the participants in the experiment had a BMI in the overweight or obese category. During 90 minutes of exercise, they focused on maintaining a pace that kept their heart rate around 120–140 beats per minute rather than distance.
However, the exercise duration appeared to be important: the researchers also ran the experiment with just 45-minutes of exercising. The shorter workout did not increase the participants’ antibody levels. Prof Kohut said a follow-up study might test whether 60 minutes is sufficient.
As to why prolonged, mild- to moderate-intensity exercise could improve the body’s immune response, Prof Kohut said there may be multiple reasons. Exercise increases blood and lymph flow, which helps circulate immune cells. As these cells move around the body, they’re more likely to detect antigens. The mouse experiment data also suggested that interferon alpha produced during exercise helps generate virus-specific antibodies and T- cells.
“A lot more research is needed to answer the why and how,” said Prof Kohut. “There are so many changes that take place when we exercise – metabolic, biochemical, neuroendocrine, circulatory. So, there’s probably a combination of factors that contribute to the antibody response we found in our study.”
The researchers are continuing to track the antibody response in the participants six months post-immunisation and have launched another study that focuses on exercise’s effects on people who receive booster shots.
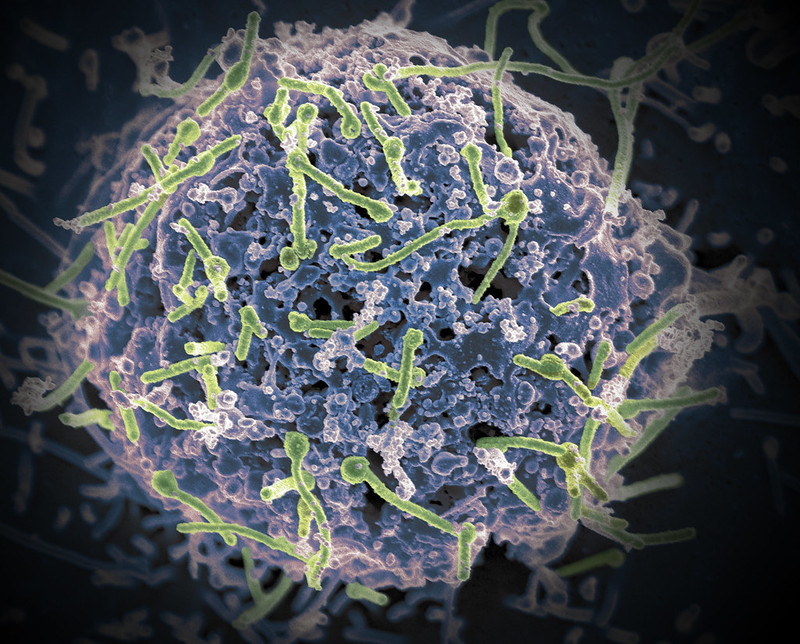
Ebola virus (green) is shown on cell surface. Credit: National Institutes of Allergy and Infectious Diseases, NIH
A new study has shown that the Ebola vaccine known as rVSVΔG-ZEBOV-GP instils a robust and enduring antibody response among vaccinated individuals in areas of the Democratic Republic of Congo that are experiencing outbreaks of the disease.
The study, published in PNAS, is the first to examine post–Ebola-vaccination antibody response in the DRC, a nation of nearly 90 million. Long-term analyses of the study cohort will continue, but in the meantime, the findings will help inform health officials’ approach to vaccine use for outbreak control, the researchers said.
Ebola, one of the world’s deadliest viral diseases known to infect humans, was first identified in 1976 following an outbreak near the Ebola River in then Zaire (now DRC). Since then, outbreaks have occurred intermittently in sub-Saharan Africa, including 12 outbreaks in the DRC, where the disease remains endemic.
The single-dose rVSVΔG-ZEBOV-GP vaccine was administered to more than 300 000 individuals in the DRC during outbreaks between 2018 and 2020. However, studies examining the antibody response of vaccinated Congolese populations had been lacking.
US and DRC researchers studied individuals who received the vaccine during an Ebola outbreak in the DRC’s North Kivu Province. Between August and September 2018, 608 eligible individuals were vaccinated. In an approach known as “ring vaccination”, these participants were contacts of people infected with Ebola or contacts of those contacts as well as health care and frontline workers in affected or potentially affected areas. Blood samples were taken at the time of vaccination, 21 days later and again after six months. They found that after 21 days, 87.2% of the study participants showed an antibody response and antibody persistence was seen in 95.6% after six months.
US researchers have shown that a Zika virus vaccine candidate is effective at preventing the Zika virus passing from mother to foetus in preclinical animal studies, according to a new study published in npj Vaccines.
“The vaccine has been shown to be safe for non-pregnant humans, but of course we need to know if it is safe and effective for the people at greatest risk: pregnant women and their fetuses,” said first author In-Jeong Kim, PhD, a viral immunologist at Trudeau Institute. “Our proof-of-concept studies conducted at Trudeau and Texas Biomed show very promising results that the vaccine given before pregnancy will provide high levels of protection for mothers and babies.”
The 2015–2016 Zika outbreak in Brazil and other countries in the Americas caused a surge in miscarriages and a constellation of birth defects, called Congenital Zika Syndrome, including abnormally small heads and neuro-developmental disorders.
“It’s important to test vaccines before the next large outbreak, because there will be another,” said senior author Jean Patterson, PhD, a virologist at Texas Biomed. “Zika is part of a family of viruses known to go through cycles. These viruses tend to spread rapidly through naïve populations that have never been exposed to the virus before, then infections drop down for years because most people have been exposed. As more and more people are born, there is a new group of naïve individuals in which the virus can once again wreak havoc. We want to help break that cycle.”
The purified, inactivated Zika vaccine (ZPIV) candidate was been tested in non-pregnant animals, showing it effectively clears the virus from blood. In Phase 1 human trials, it has been shown to be safe and elicit a protective immune response.
However for ethical and safety reasons, it is not possible to test whether the vaccine protects women and their foetuses from both infection and severe malformations, so animal models are used as a substitute.
Researchers tested the vaccine in pregnant mice and marmosets, respectively. The mouse studies, led by Dr Kim and Marcia Blackman, PhD, a viral immunologist at Trudeau, showed the vaccine prevented around 80% of foetal malformations, and neutralising antibodies were detected in foetal blood samples eight days after infection.
“We were able to detect maternal antibodies in the fetus during pregnancy and the results suggest the antibodies play a critical role in protecting fetuses from Zika virus,” Dr Kim said.
Marmosets are more sensitive to Zika infection than other nonhuman primates; previous research showed foetuses were aborted within two weeks of maternal infection.
In this study, four marmosets were immunised with the ZPIV vaccine and then exposed to Zika virus after they became pregnant. Only 1 of 12 offspring tested positive for Zika virus, demonstrating more than 90% effectiveness.
“Because the animals became pregnant at different times, our study was able to show the vaccine confers protection for at least 18 months after vaccination, which is important for showing long-lasting immunity,” Dr Patterson said.
The researchers are already testing what happens when the vaccine is administered during pregnancy.
“These studies add evidence that the Zika vaccine WRAIR developed not only protects animals against Zika virus infection, but also the congenital defects that mimic what has been observed in people,” says Kayvon Modjarrad, MD, PhD, who leads the US Army Zika vaccine programme. “Together with the early phase clinical trials, we believe these data lend even more support that this vaccine platform is a viable approach for countering the persistent threat of Zika.”