Mycobacterium tuberculosis drug susceptibility test. Photo by CDC on Unsplash
With resistance to chemical antibiotics on the rise, the world needs entirely new forms of antibiotics. A new study published in Microbiology Spectrum, a journal of the American Society for Microbiology, shows that an enzymatic cocktail can kill a variety of mycobacterial species of bacteria, including those that cause tuberculosis. The research was carried out by scientists at Colorado State University and Endolytix Technologies.
“We have a mycobacterial drug that works for Nontuberculous Mycobacteria and M. tuberculosis that is biological, not phage therapy, and not small molecule antibiotics,” said Jason Holder, Ph.D., a study coauthor and Founder and Chief Science Officer at Endolytix Technology.
“Mycobacterial infections are particularly hard to treat due to poor efficacy with standard of care drugs that are used in multidrug regimens resulting in significant toxicities and treatments lasting 6 months to years. This is often followed up by reemergence of the bacterial infection after a year of testing negative.”
In the new proof of principle study, the researchers took a biological approach instead of a chemical one to develop a cocktail of enzymes that attack the cell envelope of mycobacteria.
The cocktail of enzymes contains highly specific biochemical catalysts that target and degrade the mycobacteria cell envelope that is essential for mycobacterial viability.
To increase efficacy, the researchers delivered the enzymatic drug inside of host macrophages where mycobacteria grow. In laboratory experiments, the drug was effective against M. tuberculosis and Nontuberculous Mycobacteria (NTMs), both lethal pulmonary lung diseases (PD). TB kills roughly 1.5 million people per year.
“We characterised the mechanism of bactericide as through shredding of the bacterial cells into fragments,” Holder said.
“We’ve shown we can design and develop biological antibiotics and deliver them to the sites of infection through liposomal encapsulation. By combining drug delivery science with enzymes that lyse bacteria, we hope to open up treatment options in diseases such as NTM pulmonary disease, tuberculosis pulmonary disease and others.”
According to study coauthor Richard Slayden, PhD, a professor in the Department of Microbiology, Immunology and Pathology at Colorado State University, the new therapy complements current standard-of-care drugs and does not have many of the drug-drug interactions that are problematic with many anti-mycobacterial drugs in use. “Endolytix enzymes work powerfully with standard-of-care antibiotics to kill bacteria with lower drug concentrations,” Holder said. “This has the potential to reduce the significant toxicities associated with multi-drug regimens that are the standard for mycobacterial infections and hopefully lead to more rapid cures.”
A massive and long-awaited study of an experimental tuberculosis vaccine has kicked off in South Africa. Marcus Low reports.
Photo by National Cancer Institute
By Marcus Low for Spotlight
The first jabs in a much-anticipated clinical trial of an experimental tuberculosis (TB) vaccine have been administered at a clinical trial site at the University of the Witwatersrand in Johannesburg. Up to 20 000 people are anticipated to take part in the study, according to study sponsor, the Bill and Melinda Gates Medical Research Institute (Gates MRI).
The study will be conducted at 60 different sites in South Africa, Zambia, Malawi, Mozambique, Kenya, Indonesia, and Vietnam. The researchers estimate that between 50% and 60% of the study participants will be in South Africa.
The experimental vaccine called M72/AS01E (M72 for short) made waves in 2018 and 2019 when it was found to be around 50% effective at preventing people with latent TB infection from falling ill with TB over a three-year period in a phase 2b clinical trial. In June 2023, it was announced that, after some delays, $550 million in funding had been secured for a phase 3 study of the vaccine. Medicines or vaccines are typically only registered and brought to market after being shown to be safe and effective in large, phase 3 clinical trials.
While most cases of TB can be cured using a combination of four antibiotics for four or six months, TB rates are declining relatively slowly and it is widely thought that an effective vaccine would help bring TB rates down much more quickly. The World Health Organization estimates that at the level of protection seen in the phase 2b trial, the vaccine could potentially save 8.5 million lives and prevent 76 million people from falling ill with TB over a 25-year period. The one TB vaccine we already have, called bacille Calmette-Guerin (BCG), is over a century old and only provides limited protection against severe illness for children and no protection for adolescents or adults.
“Reaching Phase 3 with an urgently needed TB vaccine candidate is an important moment for South Africans because it demonstrates that there is a strong local and global commitment to fight a disease that remains distressingly common in our communities,” said Dr Lee Fairlie, national principal investigator for the trial in South Africa, in a media statement released by Gates MRI.
“South Africa also has considerable experience with TB- and vaccine-related clinical trials and a strong track record for protecting patient safety and generating high quality data essential for regulatory approvals.”
Fairlie is also the Director of Maternal and Child Health at the Wits Reproductive Health and HIV Institute at Wits University.
The initial response from TB activists was positive.
“TB Proof (a South African TB advocacy group) is delighted that the M72 phase 3 trial has been launched,” the organisation’s Ruvandhi Nathavitharana and Ingrid Schoeman told Spotlight. “Having an effective TB vaccine is critical for TB elimination efforts.”
While he said it is good to finally see the phase 3 trial of M72 get underway, Mike Frick, TB co-director at Treatment Action Group, a New York-based TB advocacy organisation, went on to say:
“The fact that we had to wait so long between phase II and phase III says everything one needs to know about the headwinds – financial, political, commercial – that TB research is up against.”
How the study will work
Half of the up to 20 000 study participants will receive the M72 jab and the other half a placebo. The vaccine is administered as two intramuscular injections given a month apart. After being jabbed, study participants, all aged 15 to 44, will be followed for four years from the date of the first study participant being enrolled to see if they fall ill with TB.
“The plan is to complete enrolment in 2 years,” Fairlie and Alemnew Dagnew, clinical lead for the trial, told Spotlight in response to written questions. They explained that the actual duration of the trial will depend on how long it takes for 110 people in the study to fall ill with TB. According to the Gates MRI statement, the study is expected to take around five years to complete.
According to Fairlie and Dagnew, the majority of study participants (around 18 000 people) will be people who are HIV negative and who have latent TB infection – that is to say people who have TB bacteria in their lungs, but who are not ill with TB. Latent TB infection is thought to be very common in South Africa and only around 10% of people with latent infection ever fall ill with TB. In the study, latent infection will be tested for using a type of test called an IGRA (Interferon-Gamma Release Assay).
Around 1000 HIV negative people with no TB infection will also be recruited to the study. This is being done to make sure the vaccine is safe and effective in this group of people – while latent infection will be tested for in the study, in the real world such testing may not always be feasible prior to vaccination.
It is anticipated that 1000 of the 20 000 study participants will be people living with HIV. Establishing how well the vaccine works in people living with HIV is important since around 13% of people in South Africa are living with HIV and HIV substantially increases the risk of falling ill with TB. The main phase 2b study of M72 did not include people living with HIV although another phase 2 study looked specifically at the safety and immunogenicity of M72 in people living with HIV – according to Fairlie and Dagnew, “that trial “was completed and supported the inclusion of such participants in a phase 3 trial”.
Smaller than previously thought
When funding for the phase 3 trial was announced last year, it was estimated that 26 000 people would participate in the study. That number has now been revised down to 20 000.
“As a result of ongoing discussions between the institute and our funders, the decision was taken to review the study protocol with the intent of simplifying the study given its size and complexity. This will not affect the safety of the trial. It is common to continue to refine a protocol. We found a way to expedite the study that would potentially allow us to offer the public health impact of this vaccine to those in need sooner. All partners, including the trial funders, are fully aligned to the protocol refinements,” Fairlie and Dagnew explained to Spotlight.
“Some assumptions used to inform the design of the first protocol were deemed overly conservative, so the clinical team used slightly less conservative assumptions on vaccine efficacy and TB incidence rate, thus allowing for a reduction in the number of participants in the trial, while still retaining the primary goal of confirming the safety and efficacy of the M72/AS01-E-4 vaccine for prevention of TB, guided by the final results of the phase 2b study completed several years ago.”
Planning for access
The development of M72 has taken a somewhat unusual path – with the pharmaceutical company GSK leading development up to the end of phase 2b and then largely passing the baton to Gates MRI with the conclusion of a licensing deal in 2020. GSK has come in for some criticism for not moving more quickly after the initial publication of the phase 2b results in 2018. A ProPublica article published last year suggested that the development of M72 slowed because GSK were focussing on more profitable vaccines.
According to the Gates MRI statement, GSK continues to provide technical assistance to the Gates MRI, supplies the adjuvant component of the vaccine for the phase 3 trial, and will provide the adjuvant post licensure should the trial be successful. An adjuvant is an agent included in the vaccine that improves the immune response elicited by the vaccine – in the case of M72/AS01E the AS01E refers to the adjuvant made by GSK.
This ongoing dependence on a single company for the adjuvant has some activists worried. “We are concerned about reports that scaling this vaccine may be difficult due to limited availability of the vaccine adjuvant. Access for everyone who needs it should be part of the early phases of the research process – not an afterthought,” said Nathavitharana and Schoeman.
“The press release announcing the study’s start in several places refers to the ‘complexity’ of ‘developing and ensuring access’ to a new vaccine. Part of the unspoken complexity here is the opaque licensing deal GSK and Gates MRI signed in 2020 in which GSK gave rights to develop and commercialise M72 to Gates MRI while retaining control over the AS01E adjuvant,” Frick told Spotlight. “There are legitimate concerns that the fine print of this arrangement could work against equitable access, but terms of the licence remain unknown to the public.”
When asked about supply concerns, Gates MRI told Spotlight: “Gates MRI collaboration with GSK includes provisions to ensure there is sufficient supply of adjuvant for the clinical development and first adoption in low-income countries with high TB burden, at an affordable price, should the vaccine candidate be successful in phase 3 trials and approved for use. For broader implementation, GSK has committed to working with its partners to ensure there is sufficient supply.”
Disclosure: The Gates MRI is a non-profit subsidiary of the Bill and Melinda Gates Foundation. Spotlight receives funding from the Bill and Melinda Gates Foundation. Spotlight is editorially independent and a member of the South African Press Council.
Few realise the extent of the global burden of tuberculosis (TB) or know how many people still succumb to this disease every year. The Centres for Disease Control in the United States estimates that two billion people – a quarter of the world’s population – may be infected with TB, with 10.6 million becoming ill each year. Although TB is preventable and treatable, around 3 500 people lose their lives to it every day, making up an annual mortality rate of 1.3 million people. This means that TB ranks third to only COVID-19 and HIV/Aids as the world’s most deadly infectious disease.
These statistics are alarming and demand immediate attention from all sectors of society. It is crucial to recognise the potential of technology and digital platforms in revolutionising treatment outcomes. By harnessing the power of innovation, we can transform the way in which TB is diagnosed, treated and managed, ultimately saving lives and reducing the burden of this disease.
Equally as sobering is the fact that around 30 percent of people who become ill with TB are missed by healthcare screenings and do not get the care they need, leading to poor outcomes and an increased spread of the disease, especially in remote, rural and underserved communities. People infected with TB do not necessarily become ill but can pass on the bacteria that causes the infection to between ten and fifteen other people through coughing, sneezing or the transfer of saliva. Approximately 10% of those infected go on to develop an active form of disease at some time in their lives.
TB in South Africa
In South Africa, the first-ever National Tuberculosis Prevalence Survey, published in 2018, found that the country is one of 30 countries with the highest prevalence of TB in the world. When adjusted for population size, it is often ranked as the country with the highest prevalence in the word.
The power of digital healthcare has the potential to change this scenario radically. The greatest challenges we face are the low rate of diagnosis and poor access to – and compliance with – treatment. That’s where digital platforms have such a significant role to play.
How digital can make a difference
Digital health platforms have the potential to revolutionise the fight against TB by improving early detection, enhancing treatment adherence and strengthening healthcare delivery systems. Through the integration of mobile applications, telemedicine, artificial intelligence (AI) and big data analytics, we can address the key challenges of TB diagnosis, treatment access and patient support.
Firstly, digital tools enable early detection and diagnosis of TB cases. Advanced imaging techniques, supported by AI algorithms, can swiftly identify TB-related abnormalities in medical images, facilitating prompt intervention and preventing the progression of the disease. Predictive analytics can also forecast TB outbreaks and hotspot areas, enabling healthcare authorities to take proactive measures to contain the spread of the disease.
Secondly, digital health platforms facilitate remote consultations and monitoring, which is particularly beneficial for patients in remote or underserved areas. By providing timely medical intervention and personalised support, these platforms promote treatment adherence and improve patient outcomes.
Thirdly, mobile health applications empower patients to actively participate in their care management. Through features such as medication reminders, digital health checks and access to educational resources, individuals can adhere to treatment protocols better, ultimately contributing to improved health outcomes.
In addition, digital health platforms streamline healthcare delivery by facilitating data interoperability and real-time monitoring of TB trends. Innovative technologies such as TB Check, the free service application of the South African National Department of Health, are revolutionising TB testing as they are being used to determine the risk of contracting TB and to provide guidelines on how to access testing and treatment.
Further, applications such as One Impact, a comprehensive digital health platform, connects individuals with TB support groups, provides access to TB services and enables the reporting of difficulties in accessing care. By leveraging such platforms, national TB programmes can gain valuable insights into the needs and concerns of affected communities, leading to more responsive and effective service delivery.
TB is treatable and curable, especially when patients are diagnosed early, have access to the medication they need and can be carefully monitored throughout their treatment programme.
As we observe World TB Day on 24 March, it is encouraging to know that the integration of digital health platforms provides immense promise in transforming TB outcomes. To realise this potential, collaboration among governments, healthcare providers, technology companies and civil society organisations is essential. By prioritising investment in innovative solutions and leveraging digital technologies, we can accelerate progress towards the elimination of TB and save countless lives. It is time to harness the power of technology to combat TB and create a healthier, TB-free world for all.
While three new tuberculosis (TB) medicines have been registered in South Africa over the last decade, TB treatment still comes with several side effects and requires taking multiple different medicines, typically for six or more months. The search for better TB medicines got a boost last week with the presentation of promising findings from a study conducted in South Africa on an experimental drug called quabodepistat. Elri Voigt reports on this and other TB studies presented at a conference in Denver, Colorado.
Arguably, the biggest TB news at the Conference on Retroviruses and Opportunistic Infections (CROI) this year was that the experimental new TB drug quabodepistat performed well in a phase 2b/c clinical trial. This means the drug can now proceed to a pivotal phase 3 trial (medicines are typically approved by regulators only after positive results in phase 3 trials).
The interim study results presented at CROI indicated that quabodepistat in combination with bedaquiline and delamanid and given for four months to people with drug susceptible TB is safe and efficacious, when compared to the six-month standard of care regimen. The standard of care regimen, currently used in South Africa’s public sector, consists of the drugs rifampicin, isoniazid, ethambutol, and pyrazinamide.
Participants were split into four study arms to either receive 10mg, 30mg or 90mg of quabodepistat (along with delamanid and bedaquline) once a day for four months or the standard of care regimen for six months. In the quabodepistat arms, a total of 98 study participants completed treatment, compared to 19 in the standard of care arm.
Taken together, 96% of participants in the quabodepistat arms had sputum culture conversion compared to 91% in the standard of care arm. Sputum culture conversion means TB was no longer detected in sputum samples that people coughed up when those samples were grown in the lab.
The study was conducted at several sites in South Africa and was funded by the Japanese pharmaceutical company Otsuka.
‘Furthest along’
Lindsay McKenna, the TB Project Co-Director at Treatment Action Group (TAG – a New York-based NGO), explained to Spotlight that quabodepistat is a new drug with a new mechanism of action for inhibiting TB’s cell wall synthesis. Essentially, this means that the drug interferes with the TB bacteria’s cell wall structure.
While there are a few new drugs that work the same way, quabodepistat is the furthest along.
“It’s the first in a new class of TB drugs to reach this stage since bedaquiline and delamanid were in phase 2b over ten years ago,” McKenna said.
There is however still some way to go before we will know if quabodepistat is bound for wider use than just in clinical trials. “We need to see data on clinical outcomes first,” McKenna told Spotlight, adding that quabodepistat is also being assessed in another ongoing phase 2b/c clinical trial.
“Remember that we have only seen sputum culture conversion results. Follow up is ongoing and so we will learn more when we see the proportion of participants with favorable outcomes (for example relapse free cure) 12 months post randomisation,” she said. “In the meantime, I think Otsuka should immediately begin working to start up a pre-approval access programme to enable people with unmet needs to access quabodepistat.”
Safety signals
Dr Simbarashe Takuva, Associate Director of Clinical Development at Otsuka Novel Products GmbH (an affiliate of Otsuka), who presented the results on behalf of the study team, said that overall, the quabodepistat regimen was well tolerated and considered safe.
In terms of side effects, the adverse events reported were generally described as mild or moderate, but there were some concerning signals. Grade 3 adverse events stood at 15% in the quabodepistat 10mg arm, 12% in the 30mg arm, 11% in the 90mg arm and 5% in the standard of care arm. Grade 3 adverse events are typically serious enough to prevent someone from working.
Takuva said that there were no serious adverse events (which we understand to mean grade 4/life threatening adverse events) related to the study drugs. There were also no treatment discontinuations related to the drugs. There was a single death in the study, a 25-year-old man who had met all study eligibility criteria but got sicker during the study. The study drugs were halted and standard of care drugs were given instead but the participant later died in hospital.
The researchers also looked for signs that quabodepistat might adversely affect the liver and the heart, but no safety signals related to the drugs were seen in either the liver (hepatoxicity) or the heart (cardiotoxicity).
“The data presented didn’t raise concerns about any treatment related cardio- or hepatotoxicity signals, however, it was a relatively small study, and the inclusion criteria were conservative,” McKenna commented on these findings.
One snag is that the results presented at CROI did not provide a clear answer regarding which of the three quabodepistat dosages in the study is preferable. Based on the clinical data, Takuva said it is difficult to determine which dose is best to use. He did however point out that additional work is being done looking at Pharmacokinetic and Pharmacodynamic data which will hopefully help provide more information on the ideal dose.
“Follow up on this study is ongoing. We await the final results of our phase 2 trial toward the end of the year,” he told Spotlight.
No study participants with HIV
One big limitation of these results is that the study did not enroll any people living with HIV. According to Takuva, the study had a strict exclusion criterion for the CD4 count of enrolling anyone living with HIV. A person’s CD4 count is a measure of the state of one’s immune system – higher counts are better.
Initially, the CD4 count cut off for the study was set at above 500 cells/mm3, then was amended to 350 cells/mm3 and finally it was dropped to above 250 cells/mm3 but by that time it was too late to enroll anyone living with HIV.
“The interim results are encouraging. However, I was really surprised and disappointed that they weren’t able to enroll any people living with HIV in the trial,” McKenna told Spotlight.
When asked about this, Takuva told Spotlight that the protocol did include the provision to recruit people living with HIV, but it was not feasible to include any. However, people living with HIV will be considered as important to include in any phase 3 trials going forward.
“As with all studies, we need to balance patient safety and the goal of the study outcome. In this instance, despite our best efforts, recruitment of people living with HIV was not feasible, though as we consider the possibility of a phase 3 trial, people living with HIV will remain a population that we consider important to include as far as possible in the phase 3 trial,” he said.
Treating DR-TB in people living with HIV
In contrast to the lack of people with HIV in the quabodepistat study, research was also presented at CROI looking specifically at how people living with HIV did in the landmark endTB trial. Other results from endTB were previously reported and the trial is widely considered one of a hand full of key trials transforming the treatment of drug-resistant forms of TB. The researchers found that two nine-month regimens studied in endTB did particularly well in people living with HIV. Such findings are of particular importance in a country like South Africa where many people who fall ill with TB are also living with HIV. (For those interested in the details, the two regimens were bedaquiline/linezolid/moxifloxacin/pyrazinamide and bedaquiline/clofazimine/linezolid/levofloxacin/pyrazinamide)
Some disappointments
Mycobacterium tuberculosis drug susceptibility test. Photo by CDC on Unsplash
In a disappointing development, researchers presenting at CROI reported that a study testing a three-month regimen for the treatment of drug-susceptible TB was stopped early after an interim review found the regimen had poor efficacy compared to the six-month standard of care. The regimen contained the drugs clofazimine and rifapentine, among others. It means that for now the shortest regimen for treating drug-susceptible TB validated in a clinical trial remains a four-month regimen containing the medicines rifapentine and moxifloxacin, among others. That four-month regimen is not yet in wide use, even though findings confirming its safety and efficacy were reported in 2020.
We also received some bad news on an experimental TB vaccine called H56:IC31. The idea of H56:IC31 was to vaccinate people who were just cured of TB to prevent the TB from coming back – people whose TB is deemed to be cured are known to have an increased risk of falling ill with TB again. Despite promising signs in earlier studies, the vaccine failed to reduce TB recurrence in a phase 2 clinical trial of over 800 people. Much of this study was conducted at sites in South Africa.
TB treatment’s impact on mental and physical health
Another interesting study conducted in South Africa and presented at CROI looked at the changes in mental and physical health that people ill with TB experience before and after treatment. It found that the quality of life and physical fitness of participants was reduced at the start of TB treatment but did improve by the end of TB treatment.
The researchers looked at 200 study participants split between South Africa, Zambia, Malawi, Mozambique and Zimbabwe. Their mental and physical health was assessed when they started TB treatment through a standardised short form quality of life survey, depression assessed through a patient health questionnaire and their physical health was tested using a six-minute walk test. Participants were assessed again when treatment was completed, and data was compared to see what changed between the start and end of TB treatment.
Overall, participant’s physical quality of life increased by 39% by the end of TB treatment, mental quality of life increased by 19%, ability to do a six-minute walk increased by 15% and depression scores decreased by 26%.
Long-acting therapies for TB
Long-acting therapies have been making waves for some time in HIV treatment and a long-acting injection and ring are currently being offered in pilot projects in South Africa. Two studies of long-acting therapies in mice presented at CROI show that there is at least some movement in this area as well when it comes to TB. Such long-acting therapies have particular potential for TB preventive therapy – with for example what is now a three-month course of pills being administered as a single long-acting injection.
One study found that a long-acting injectable form of the drug rifapentine had similar efficacy to a one-month course of preventive therapy in pill form, while another had similarly promising findings for an injection using a long-acting formulation of a diarylquinoline (a class of TB drugs that include bedaquiline). It is anticipated these early proof of concept mouse studies will be followed by studies in humans.
La Jolla Institute for Immunology (LJI) is working to guide the development of new tuberculosis vaccines and drug therapies. Now a team of LJI scientists has uncovered important clues to how human T cells combat Mycobacterium tuberculosis, the bacterium that causes TB. Their findings were published recently in Nature Communications.
“This research gives us a better understanding of T cell responses to different stages in tuberculosis infection and helps us figure out is there are additional diagnostic targets, vaccine targets, or drug candidates to help people with the disease,” says LJI Research Assistant Professor Cecilia Lindestam Arlehamn, PhD, who led the new research in collaboration with LJI Professors Bjoern Peters, PhD, and Alessandro Sette, Dr.Biol.Sci.
The urgent need for TB research
According to the World Health Organization, more than 1.3 million people died of TB in 2022, making it the second-leading infectious cause-of-death after COVID. “TB is a huge problem in many countries,” says Lindestam Arlehamn.
Currently, a vaccine called bacille Calmette-Guerin (BCG) protects against some severe cases of TB. Unfortunately, BCG doesn’t consistently prevent cases of pulmonary TB, which can also be deadly.
Although there are drug treatments for TB, more and more cases around the world have proven drug resistant.
To help stop TB, Lindestam Arlehamn and her colleagues are learning from T cells. Instead of targeting an entire pathogen, T cells look for specific markers, called peptides sequences, that belong to the pathogen.
When a T cell recognises a certain part of a pathogen’s peptide sequence, that area is termed an “epitope.”
Uncovering T cell epitopes gives scientists vital information on how vaccines and drug treatments might take aim at the same epitopes to stop a pathogen.
T cells take aim at a range of TB epitopes
For the new study, the researchers worked with samples from patients who were mid-treatment for active TB. These samples came from study participants in Peru, Sri Lanka, and Moldova.
By looking at T cells in patients from three different continents, the researchers hoped to capture a wide diversity of genetics and environmental factors that can affect immune system activity.
In their analysis, the LJI team uncovered 137 unique T cell epitopes. They found that 16% of these epitopes were targeted by T cells found in two or more patients. The immune system appeared to be working hard to zoom in on these epitopes.
Going forward, Lindestam Arlehamn’s laboratory will investigate which of these epitopes may be promising targets for future TB vaccines and drug therapies.
A step toward better diagnostics
The new study is also a step toward catching TB cases before they turn deadly.
Because Mycobacterium tuberculosis is an airborne bacteria, a person can be exposed without ever realizing it. Once exposed, many people go months or years without any symptoms.
This inactive, or “latent,” TB can turn into active TB if a person’s immune system weakens, for example, during pregnancy or due to an infection such as HIV.
For the new study, the researchers also compared samples from active TB patients with samples from healthy individuals.
The scientists uncovered key differences in T cell reactivity between the two groups.
“For the first time, we could distinguish people with active TB versus those that have been exposed to TB – or unexposed individuals,” says Lindestam Arlehamn.
Lindestam Arlehamn says it may be possible to develop diagnostics that detect this tell-tale T cell reactivity that marks a person’s shift from latent to active TB. “Can we use this peptide pool to look for high-risk individuals and try and follow them over time?” she says.
An international research team has found a number of substances with a dual effect against tuberculosis (TB): They make the bacteria causing the disease less pathogenic for human immune cells whilst boosting the activity of conventional antibiotics. They published their findings in the journal Cell Chemical Biology.
Infectious disease specialist Dr Jan Rybniker and colleagues have identified new, antibiotic molecules that target Mycobacterium tuberculosis and make it less pathogenic for humans.
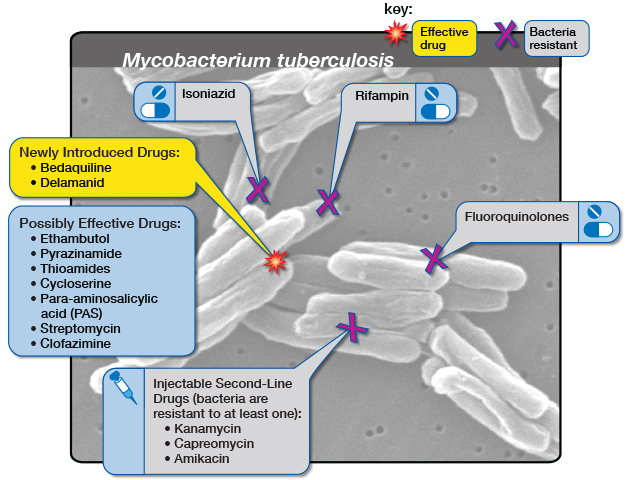
Diagram by the United States-based National Institute of Allergy and Infectious Diseases showing the medicine options for drug-resistant tuberculosis. (Via Flickr, CC BY 2.0 Deed)
In addition, some of the discovered substances may allow for a renewed treatment of tuberculosis with available medications – including strains of the bacterium that have already developed drug resistance.
Although treatable with antibiotics, it still ranks among the infectious diseases that claim the most lives worldwide: According to the World Health Organization (WHO), only COVID was deadlier than TB in 2022. The disease also caused almost twice as many deaths as HIV/AIDS. More than 10 million people continue to contract TB every year, mainly due to insufficient access to medical treatment in many countries.
Limited targets
Multidrug-resistant tuberculosis is emerging especially in eastern Europe and Asia. That is of particular concern to researchers because like all bacteria that infect humans, Mycobacterium tuberculosis possesses only a limited number of targets for conventional antibiotics.
That makes it increasingly difficult to discover new antibiotic substances in research laboratories.
Working together with colleagues from the Institute Pasteur in Lille, France, and the German Center for Infection Research (DZIF), the researchers at University Hospital Cologne have now identified an alternative treatment strategy for the bacterium.
The team utilized host-cell-based high-throughput methods to test the ability of molecules to stem the multiplication of bacteria in human immune cells: From a total of 10,000 molecules, this procedure allowed them to isolate a handful whose properties they scrutinized more closely in the course of the study.
Two-pronged attack
Ultimately, the researchers identified virulence blockers that utilise target structures that are fundamentally distinct from those targeted by classical antibiotics.
“These molecules probably lead to significantly less selective pressure on the bacterium, and thus to less resistance,” said Jan Rybniker, who heads the Translational Research Unit for Infectious Diseases at the Center for Molecular Medicine Cologne (CMMC) and initiated the study.
In deciphering the exact mechanism of action, the researchers also discovered that some of the newly identified chemical substances are dual-active molecules.
Thus, they not only attack the pathogen’s virulence factors, but also enhance the activity of monooxygenases — enzymes required for the activation of the conventional antibiotic ethionamide.
Ethionamide is a drug that has been used for many decades to treat TB. It is a so-called prodrug, a substance that needs to be enzymatically activated in the bacterium to kill it. Therefore, the discovered molecules act as prodrug boosters, providing another alternative approach to the development of conventional antibiotics.
In cooperation with the research team led by Professor Alain Baulard at Lille, the precise molecular mechanism of this booster effect was deciphered.
Thus, in combination with these new active substances, drugs that are already in use against tuberculosis might continue to be employed effectively in the future.
The discovery offers several attractive starting points for the development of novel and urgently needed agents against tuberculosis.
“Moreover, our work is an interesting example of the diversity of pharmacologically active substances. The activity spectrum of these molecules can be modified by the smallest chemical modifications,” Rybniker added.
However, according to the scientists it is still a long way to the application of the findings in humans, requiring numerous adjustments of the substances in the laboratory.
For decades, the standard way to prevent people who were exposed to tuberculosis (TB) from falling ill with the disease was to offer them a medicine called isoniazid, taken daily for six or more months. That changed in the last decade with the development of new preventive therapy regimens that are taken for four, three, or even just one month.
One complexity, however, is that both isoniazid and the new regimens are much better at preventing normal drug-sensitive TB than they are at preventing drug-resistant forms of TB. This is not surprising. As explained by Paediatric Infectious Disease doctor and Professor of Global Child Health at Imperial College London, Dr James Seddon, the two drugs that have mainly been used to prevent drug-susceptible TB are isoniazid and rifampicin (rifampicin’s sister drug rifapentine is also used). Now, by definition, he explains multidrug-resistant (MDR) TB is resistant to both these drugs so it’s unlikely to have any impact.
The situation is particularly tricky when it comes to children. In a 2020 statement the World Health Organization (WHO) says that it estimated that worldwide between 25 000 and 32 000 children develop MDR-TB each year, and mainly acquire it through transmission from close contact with an adult or adolescent who has MDR-TB. According to Seddon, while there is some emerging observational evidence on the use of drugs other than isoniazid and rifampicin to prevent MDR-TB, there has been no clinically tested regimen to give to children following MDR-TB exposure.
Now, much anticipated results from a phase three trial has shown that a single antibiotic pill, given daily for six months, is safe and effective to use in children who have been exposed to MDR-TB.
Results from TB CHAMP
The trial, called TB-CHAMP, looked at the efficacy and safety of using the antibiotic levofloxacin to prevent TB in children exposed to MDR-TB. Top-line findings from the study was presented last week at the Union World Lung Conference held in Paris, France.
“The paediatric population is probably the most neglected of all the populations affected by MDR-TB,” Dr Anneke Hesseling, Director of the Paediatric TB Research Programme at Stellenbosch University, told the conference. “Fewer than 20% who develop MDR-TB disease are actually diagnosed and treated, and so to find more cases and prevent more cases is really, really critical…So prevention is really key, and the TB-CHAMP trial is really a phase three efficacy trial looking at levofloxacin to prevent new cases of TB in children and also looking at the safety of levofloxacin.”
Hesseling, who is the Principal Investigator of the study, says that TB-CHAMP is the first trial to provide clinical data on what drug might be used to prevent TB in children who have been exposed to MDR-TB. It was conducted at five sites across South Africa, all with high MDR-TB burdens. The study was led by Stellenbosch University and the Desmund Tutu TB Centre. The findings have not yet been published in a peer-reviewed journal.
922 children were randomised to receive either levofloxacin or a placebo for six months. 453 children got levofloxacin and 469 got the placebo. The primary efficacy data featured data from 916 of those children, with 451 in the levofloxacin arm and 465 in the placebo arm.
Hesseling says that only children who were exposed to an adult in their household with confirmed MDR-TB were included in the study. At first children below the age of five were recruited, regardless of their TB infection status. Later children between the ages of five and 17 were included, but they had to either have a TB infection or be living with HIV. The majority of the children, 90%, were younger than five years. TB infection was confirmed with a blood test.
By 48 weeks, Hesseling says five children in the levofloxacin arm versus 12 in the placebo arm developed TB, which amounts to an incidence rate of 1.1% in the levofloxacin arm, and 2.6% in the placebo arm.
Implication of results
“While TB preventive therapy (TPT) has long been recommended and available for young child contacts of people with drug-susceptible TB, there has not been sufficient evidence to make strong recommendations for treatment that could prevent DR-TB. Therefore, the TB-CHAMP findings are critically important for a number of reasons,” says Professor Guy Marks, President and Interim Executive Director, International Union Against Tuberculosis and Lung Disease (The Union).
“The study provides the first high-quality evidence that DR-TB can be prevented in children by using six months of daily levofloxacin, and that this is a safe medication. Furthermore, this will encourage more community-based contact screening, which will also lead to early detection of children and contacts of all ages who already have disease, and initiate treatment,” he adds.
“The impact [of the TB-CHAMP results] is potentially tremendous as it would prevent DR TB among child contacts. DR TB is more complex to treat and cure and often children are marginalised, so this study puts the spotlight on an effective way to protect children. This is not just about the life and health of the child but the social, economic and mental health implications for the caregiver and the entire family,” says Dr Priashni Subrayen, Technical Director for TB at The Aurum Institute.
Seddon, who is also one of the Co-PIs for the study, tells Spotlight that it was important to establish the safety of levofloxacin since it belongs to a class of drugs called the fluoroquinolones, which were thought to have terrible side effects when used in children.
Results from TB-CHAMP show that this is not the case.
The side effects were mild, and the regimen was well tolerated, according to Hesseling, with only eight children having a grade one or higher adverse event in the levofloxacin arm compared to four in the placebo arm. Two deaths were reported, one in each study arm, but were unrelated to the study. Overall, six children in the levofloxacin arm discontinued treatment or left the study early.
Researchers from TB-CHAMP collaborated with researchers from the V-QUIN trial – a phase three study that looked at levofloxacin as TB prevention in adults in Vietnam – in order to combine their data which allowed them to show data for levofloxacin across different age groups. Seddon explains: “They’ve applied a novel analytic approach, which uses a Bayesian, or probabilistic, framework, where we take the results of TB-CHAMP and we say well, if we actually use some of the information from V-QUIN to inform the TB-CHAMP results, we can make that a slightly more confident estimate,” he says.
The combined results, according to Hesseling were able to also show that levofloxacin reduced the risk of TB by about 60% across the age spectrum but with a tighter confidence interval, indicating a more precise estimate of the effect.
Seddon tells Spotlight that the combined data showed that there were no serious adverse events, but the adult population experienced more grade one and grade two side effects than the children, but these went away either over time or when the drug was stopped. The side effects included inflammation in the joints and tendons, which is a known side effect of this class of drug.
Not a silver bullet
While the findings could be a game-changer and potentially inform MDR-TB prevention guidelines, particularly in children, the regimen is by no means a silver bullet. Seddon says that while the regimen was safe, when participants were asked whether they liked the medicine, more people said they didn’t like it in the levofloxacin group versus the placebo. Another downside is that the pill was an adult formulation and thus needed to be cut and/or crushed for the kids to swallow.
Seddon explains that the WHO, who have been provided with the data from both studies and expected to meet in early December, would need to consider a variety of factors before deciding what to recommend about the use of levofloxacin for prevention. That includes the fact that you need to treat a lot of children for six months who might not have TB despite being exposed in order to prevent a few cases.
“You have to weigh up the benefits versus the risks and the risks are low, but it is still giving a drug for six months to children and most of them don’t need it. But the consequences of getting MDR-TB are so bad that we really want to prevent that,” he says.
There is also the question around what effect using a broad antibiotic as preventive treatment will have on the microbiome of children and how this might drive resistance to the fluoroquinolones. Seddon says stool samples were collected from the study participants to determine how the drug affected a child’s microbiome and the potential for driving resistance. These data will also be provided to the WHO.
“I think that the evidence base is now very strong on the basis of these two trials. I think you can really say the issue of whether levofloxacin prevents MDR-TB, we’ve put that to bed,” he says. “Are there going to be other studies? Yes. I think that this is not over, levofloxacin is not the perfect drug for preventive therapy.”
Marks adds to this saying: “An important next step for TPT in DR-TB contacts will be studies that evaluate regimens that are shorter than six months – a long time to take medication every day, which can often be challenging. Effective and safe shorter regimens are now being used for child contacts of drug-susceptible TB and we hope the same progress can be made for contacts of DR-TB.”
As Marks has already stated, currently there are no strong recommendations for MDR-TB prevention by the WHO. In the 2020 TB prevention guidelines, it recommends that the preventative treatment for MDR-TB should be either a fluroquinolone or other second-line agent. It does however caution that these recommendations are based on low-quality evidence. Because of this, it recommends that the preventative treatment for MDR-TB should be individualised, and it be based on the drug resistance profile of the presumed contact. The drugs levofloxacin and moxifloxacin- both fluoroquinolones – may be used unless resistance is suspected. For levofloxacin a dosing schedule for both adults and children are proposed in the document.
Subrayen says that in South Africa the 2019 guidelines for the management of Rifampicin Resistant-TB (RR-TB) does indicate the use of levofloxacin as prevention treatment. The guidelines state that for prevention treatment a fluoroquinolone-based, multidrug regimen is preferred (either levofloxacin and high-dose isoniazid or levofloxacin, high-dose isoniazid and ethambutol). And if exposed to fluoroquinolone-resistant RR-TB, then high-dose isoniazid could be given. Delamanid could be considered as a potential option in very select cases. A training manual published this year by the Department of Health suggests that levofloxacin can be given on its own – but also stresses that the evidence base is weak, something that TB-CHAMP has presumably now changed.
Future of TPT
Seddon says that in a perfect world the ideal TB preventive regimen would be a so-called Pan regimen that could be given for a short period of time, to someone who has been exposed to TB and it works regardless of whether they had been exposed to drug-susceptible or drug-resistant TB.
“There are studies planned to use other drugs for prevention. There’s a study planned to use bedaquiline for a month or two and potentially using injectables that you just have to give once every couple of weeks. So, I think although this [levofloxacin] is a good option now, and it’s probably the best option we have now, this is not perfect,” Seddon says.
The study Seddon is referring to is the BREACH-TB study, a phase three trial that will look at whether a one-month treatment regimen of oral bedaquiline could prevent all forms of tuberculosis. It would be given to people exposed to both drug-resistant and drug-susceptible TB, and in people with HIV infection, including pregnant women and children.
Responding to questions from Spotlight earlier this year when this study was announced in the press, Sonya Krishnan, Assistant Professor of Medicine at Johns Hopkins University and Eric Nuermberger, Professor of Medicine at Johns Hopkins University, said that they anticipate recruiting between 1600 and 2 00 people to take part in the study – they expect around 400 to 500 of these will be people living with HIV. They also said that the control arm will receive the current standard of care in the country rather than placebo.
When asked whether any South African study sites will be included in the clinical trial, they said, “We very much plan to partner with study sites in South Africa. South Africa has a long-standing history of research excellence in TB.”
“A shorter regimen that fights both drug-resistant and drug-susceptible TB would be a game-changer for those living with TB and get us closer to our shared goal of ending the epidemic by 2030,” said Dr. Atul Gawande, USAID assistant administrator for Global Health, in a statement on the study. “This clinical trial will lay the foundation for a remarkable innovation in our fight against TB: a single-dose, long-acting injectable medicine.”
Indeed, if the science and development pans out as Gawande suggests it might, the future of TB preventive therapy might well be an entire course of therapy delivered through a single injection rather than a month or more of pills. As indicated in an article in the journal Clinical Infectious Diseases, work is already underway on the development of bedaquline, isoniazid, and rifapentine long-acting injections – though the research is for now still only in mice.
‘Communities need to be involved’
Hesseling raises the point that when treating or preventing TB, more than just the latest research advancement is needed to improve TB outcomes.
“For me treatment follows diagnosis, actually strengthening healthcare services, making communities more aware and creating demand for kids accessing diagnosis, preventive treatment and appropriate treatment, is actually where it starts,” she says. “So tools are amazing, but we actually need to have strong, effective healthcare services and knowledgeable, empowered communities.”
Seddon adds to this saying that results like those from TB-CHAMP are “a bit irrelevant if it is all kind of top down, paternalistic coming from the researchers, coming from the health system”.
“We really need to generate a community demand for this, where individuals living in communities where this is a problem are calling for this and getting angry about this and demanding it in a way that I think we’ve achieved very well with the HIV community,” he says. “It’s all well and good doing the science and then even better to get it [levofloxacin] into a guideline, but until there’s real demand for from the end user, I think it’s only going to have a certain amount of reach.”
Note: The terms DR-TB and MDR-TB are used somewhat interchangeably – Spotlight uses DR-TB to refer to drug-resistant forms of TB in general and MDR-TB to refer specifically to TB that is resistant to isoniazid and rifampicin.
Diagram by the United States-based National Institute of Allergy and Infectious Diseases showing the medicine options for drug-resistant tuberculosis. (Via Flickr, CC BY 2.0 Deed)
The South African government and pharmaceutical company Johnson & Johnson (J&J) have agreed to a lower price for bedaquiline, a medicine used to treat drug-resistant tuberculosis (DR-TB) in South Africa.
This comes off the back of mounting pressure from activists and amid an ongoing investigation by the Competition Commission, looking into J&J’s pricing of the drug.
An estimated 14 000 people in South Africa fell ill with DR-TB in 2019. Bedaquiline is one of the main drugs used to treat DR-TB. Before bedaquiline became available, treatment for DR-TB would consist of up to two years of injections with serious side effects. The bedaquiline-containing regimen has no injectables, far fewer side effects and is typically six months.
Bedaquiline has been provided by the South African government since 2018.
In July, J&J agreed to sell bedaquiline to lower and middle-income countries through the Stop TB Partnership’s Global Drug Facility for $130 (R2470) per six-month regime, but South Africa does not make use of this facility due to national procurement policies.
Instead, about the same time that J&J made this announcement, the National Health Department agreed to pay J&J R5500 for the drug.
The Competition Commission announced in September that it will be investigating Johnson & Johnson’s pricing of the drug. The commission assisted the Department of Health in renegotiating the price, says department spokesperson Foster Mohale.
This week the department sent out a circular indicating that it will be paying R3,148 for bedaquiline.
Bedaquiline is prescribed to 7000 to 8000 people a year, Mohale told GroundUp. Mohale says the new price amounts to a 40% saving on bedaquiline for the next two years.
Candice Sehoma, Access Campaign Advocacy Advisor for Medicines Sans Frontiere (MSF), told GroundUp that the “momentous” cost saving is a “big achievement”. Sehoma says it is a sign that the global campaign to ensure accessible and affordable treatment for TB is yielding results.
MSF has estimated that bedaquiline could be manufactured and sold for profit for as little as $102 (R1940).
Fatima Hassan, director of the Health Justice Initiative, says that while the price drop is a victory, it is important to ensure that this does not happen again.
“The significant price reduction emphasises why price scrutiny is significant,” Hassan told GroundUp.
Alleged “evergreening”
J&J’s patent for bedaquiline expired in July 2023, but J&J had already applied for a new patent for a slightly different version of bedaquiline, which was granted. This meant their patent protection continued in South Africa after the original patent expired.
This amounts to “evergreening”, says Hassan. Evergreening, as explained in this article in The Conversation, “is achieved by seeking extra patents on variations of the original drug – new forms of release, new dosages, new combinations or variations, or new forms”.
The Competition Commission will be looking into J&J’s alleged “evergreening” as part of its investigation.
After making its agreement with the Global Drug Facility, J&J has announced it will not be enforcing the new patent – a move that will allow generic versions of the product to enter the market and further lower the price.
GroundUp sent questions to J&J but received no response.
Professor Valerie Mizrahi, a world-leading tuberculosis researcher and director of the Institute of Infectious Disease and Molecular Medicine at the University of Cape Town, is retiring at the end of the year. PHOTO: Nasief Manie/Spotlight
World-leading tuberculosis researcher Professor Valerie Mizrahi was 35 when her mother Etty started losing weight and coughing furiously. After healthcare professionals in Johannesburg failed to accurately diagnose her, it was a doctor in Plettenberg Bay who told Etty: “The good news is you don’t have lung cancer, the bad news is that you have tuberculosis (TB).”
At the time, Mizrahi’s two infant daughters – aged one and three years old – had been spending much time with their granny. And so Mizrahi found herself crushing TB prevention tablets into her children’s porridge with honey.
Etty was treated at the then-Rietfontein Hospital, the precursor to Sizwe Tropical Diseases Hospital in Johannesburg. “My mom got very ill,” recalls Mizrahi. “She almost died of TB. And then 10 years later, she had to have a lobe from one of her lungs removed because she was one of those unfortunate people who got post-TB fibrosis.”
This was the early 1990s. Mizrahi was then with the South African Institute for Medical Research (SAIMR) linked to the University of the Witwatersrand, where she established the Molecular Biology Unit. She had identified TB as a lurking problem in South Africa, particularly in mines and in hospitals, calling it “a worthy foe ripe with opportunity for scientific investigation” – a problem she felt not enough people were talking about. It had been a pivotal moment when TB entered her own home, one that she says galvanised her thinking.
“It was a dramatic eye-opener for me as a basic scientist,” she says. “It was traumatic because of the time it happened in my career. Our family suddenly being thrust into the world of TB control. We had all these questions like we didn’t know where my mum got it, was her TB drug-susceptible, and why it would take so long to find this out. I got to see first-hand how difficult it was to get answers…”
Born in 1958 to Etty and Morris in Harare, Zimbabwe, Mizrahi studied at the University of Cape Town (UCT), forging an unusual career path, veering from mathematics and chemistry to biochemistry, genetics, and microbiology. In a male-dominated field, she became one of the first in South Africa to interrogate TB at a basic science level – that is to say, research aimed at advancing our understanding of the basic science of how TB bacteria survive, replicate, and resist attempts to kill it.
‘the only good TB bacillus is a dead one’
Discussing TB, Mizrahi’s passion is effervescent, her every second sentence punctuated with “okay”. These underscore her statements – subtle pauses allowing for her preceding words to sink in.
Source: CC0
…there’s a reason why TB has persisted for so long. The bacillus is pretty hard to kill. It’s built like Fort Knox.
Prof Valerie Mizrahi
A particular interest for Mizrahi is developing antibiotics “that can kill this bacterium stone cold dead”.
“To me, the only good TB bacillus is a dead one,” she says. “But there’s a reason why TB has persisted for so long. The bacillus is pretty hard to kill. It’s built like Fort Knox. So it’s a monumental challenge. We don’t know where all the bacteria are residing. We know that TB in an infected lung is sitting in really difficult places, hard places for drugs to get to. This notion of going after the bacillus with drugs and just slamming it is a tough problem. Not insurmountable, but there’s a lot of research that needs to be done.”
TB can be cured, but treatment typically takes at least six months and involves taking at least four different antibiotics, with side effects ranging from minor to serious. In addition to research on new antibiotics, there are also several experimental TB vaccines currently in late-phase studies. The only TB vaccine we have was developed more than a century ago and only has some moderate efficacy in kids.
The IDM
Since 2011 Mizrahi has served as director of the Institute of Infectious Disease and Molecular Medicine (IDM) – the University of Cape Town’s (UCT) largest cross-faculty research unit with over 800 affiliated staff and grants running into hundreds of millions of rands.
Mizrahi’s glass-encased office looks directly onto Table Mountain and hospital bend – where, at the time of our interview, N2 traffic out of Cape Town is already at a standstill. Behind her desk, Mizrahi quips. “Yes, this is the most beautiful office at UCT, everyone agrees…” Below, students can be seen milling about on the health sciences campus.
Last year in its Best Global Universities 2022-2023 survey, online portal US News ranked UCT as 24th best university in the world for studying infectious diseases. Mizrahi is ambivalent about the IDM taking credit for this accolade. She notes that this success is founded on problems of a “confounding and overwhelming” scope, with many diseases being proxies for poverty and inequality in South Africa.
The IDM’s focus includes TB, HIV/AIDS, COVID-19, other infectious diseases like sexually transmitted infections, and non-communicable diseases such as preventable cancers, cardiovascular, and psychiatric disorders.
Reflecting on the IDM, she says they have accrued a “research ecosystem – a concentration of expertise, something resembling critical mass” – bringing together specialists across the basic, clinical, and public health sciences, in one place.
“We’ve got Groote Schuur Hospital across the road,” she says. “We have geneticists and biochemists, virologists, and immunologists. There’s a clinician across the corridor from me, bioinformaticians, and microscopists downstairs. If you are the kind of researcher who revels in asking questions and finding people who can answer them, then this is the place for you.”
Going forward, multi-disciplinary research is what excites her. “HIV and TB have been so dominant in the narrative of this country. But now when you look at the figures and the data, we are dealing with a huge burden of non-communicable disease on top of infectious diseases,” she says. “The key question moving forward is how not to think in silos.”
Polymaths and dilettantes
This, she says, takes humility.
“To do this, one has to be very humble. You need to know what you don’t know. People who work really well in interdisciplinary spaces are those who understand the limits of their own specialist knowledge, and the need to listen to where another person is coming from.”
She distinguishes between polymaths and dilettantes. “You have to be careful not to be a dilettante, who knows a little about a lot. Research can be very superficial in that way. So I have my antenna out all the time to distinguish between polymaths, who really are people who know a lot about a lot, and dilettantes who know a little about a lot. And well, in this institute we have a lot of polymaths, brilliant researchers who move across disciplines, very interesting people to work with.”
With a string of awards and an A1-rating from South Africa’s National Research Foundation, earlier this year, Mizrahi was elected a fellow of the Royal Society, the United Kingdom’s National Academy of Sciences. However, she recalls humbling moments along the way – like the time she flew to London seven months pregnant with her second child, for her first-ever interview with the Wellcome Trust committee to secure funding. “I was so confident, but I was ill-prepared,” she says. “They savaged me! I tried to frame it not as a failure but as a learning experience.”
Passing the baton
At the end of this year, Mizrahi will pass on the baton when she retires. Of her achievements, she is proudest of young scholars she has helped to shape. “Their legacies will last much longer than a few more citations of a publication,” she says.
Mizrahi notes more and more women leaders in her field. For example, recently, while delivering a talk at the Weizmann Institute in Israel, she noticed chemist and Nobel laureate Ada Yonath in the room. “Talk about a role model; I was almost in tears.”
Studying at UCT, Mizrahi’s own mentors had mostly been men – something she didn’t even notice, she says, as male professors treated her no different. What did cut her was racial segregation at the time, prompting a political awakening and stints leaving South Africa to work in the United States. First as a postdoctoral fellow at Pennsylvania State University and then at drug company, SmithKline & French in Philadelphia.
Her own background makes her sensitive to marginalised groups, she says. Her grandparents were Sephardi Jews who fled Rhodes Island, today part of Greece, ten years before World War II, to find refuge in Zimbabwe.
Having just read former UCT vice-chancellor Max Price’s book Statues and Storms: Leading a University Through Change, she says, “It took me back to some very difficult times. It’s harrowing and brave and made me realise that even though I was here in the midst of it [#feesmustfall and #rhodesmustfall protests], a senior person of the university, how little I really knew of what was going on. It really is a lesson in crisis leadership.”
There’s no control experiment to life, you can’t go back and redo it.
Mizrahi lives in Sea Point with her one daughter. Her other daughter is based in Vancouver. Here, she likes to park her car at the end of the week, walking around – “either listening to a New York Times podcast or a beautiful piece of music and that’s when I think.”
She describes herself as an introvert who needs personal time to stay sane. She is deeply thoughtful about her roots, wondering about a sense of belonging. “As white people in Africa, I think this is part of the reckoning we go through. I truly identify as being African. Arriving at Johannesburg, just breathing in the air, it feels like home.”
Looking back, Mizrahi notes her mother as a major influence in her life. “Not a highly educated woman. But the wisest, smartest person I know.” Etty still lives in Johannesburg while Morris has passed away. To this day, Etty thinks of herself as a proud TB survivor, says Mizrahi.
On her retirement, the scholar says, “Now it’s about opening up opportunities for others, writing a few papers, and contributing to the TB drug discovery space.”
“I’ve done the best I can,” she says, “I don’t believe in having regrets… There’s no control experiment to life, you can’t go back and redo it. But I don’t know that I could have done it any differently.”
A massive and much-anticipated phase 3 trial of an experimental tuberculosis (TB) vaccine is set to proceed after funding for it has been secured from two large philanthropies. Wellcome and the Bill & Melinda Gates Foundation (BMGF) Wednesday announced they’d be investing a combined $550 million into the trial – around $150 million from Wellcome and the remaining from the Bill & Melinda Gates Medical Research Institute, a nonprofit subsidiary of the BMGF.
The vaccine, called M72/AS01E or just M72, made headlines in September 2018 when it was found to offer 54% protection against pulmonary TB disease in a phase 2B trial. That trial, of around 3 300 people, was conducted in South Africa, Zambia, and Kenya. Final results from that study were published in the New England Journal of Medicine in 2019 – efficacy in these final results was down to around 50%.
Medicines and vaccines are typically only brought to market once safety and efficacy have been confirmed in a large phase 3 trial. In this case, the phase 3 trial is set to have around eight times as many participants as the phase 2B trial.
26 000 study participants
“Conducted in collaboration with an international consortium of TB clinical investigators, the trial will enrol approximately 26 000 people, including people living with HIV and without TB infection, at more than 50 trial sites in Africa and Southeast Asia,” Wellcome and BMGF said in a statement announcing the trial.
They said the trial will “assess the candidate vaccine’s efficacy at preventing progression from latent TB infection to pulmonary TB”. In an online media conference on Wednesday Trevor Mundel, President for Global Health at BMGF, clarified that while most study participants will be people with latent TB infection, 4 000 people without TB infection would also be recruited. This is because establishing evidence of the vaccine’s safety in people without latent TB infection will be important if the vaccine is to be rolled out in areas with high background rates of TB without first having to test everyone for latent infection. “You’d want to be comfortable with vaccinating everyone in the community,” he said, “So we need to have that safety data in the uninfected as well in order to be able to have that usage, which will be the easiest way to use the vaccine at the end of the day.”
Mundel said that the study is scheduled to start early in 2024 and that it is expected to last for four to six years. Exactly how long the study will take will depend largely on how long it takes for 150 study participants to develop active TB – the number required for the study to have sufficient statistical power. By comparison, recruitment for the phase 2B trial started in 2014 and the first findings from that study were published in 2018.
According to the statement, additional details about the trial design and participants will be announced in the coming months.
Given that the phase 2B trial was partially conducted in South Africa and the country has substantial TB clinical trial capacity, it is almost certain that some of the 50 trial sites will be in South Africa – although know specific trial sites have yet been announced.
As pointed out in the statement, the only TB vaccine in use today, bacille Calmette-Guerin (BCG), was first given to people in 1921. It helps protect babies and young children against severe systemic forms of TB but offers limited protection against pulmonary TB among adolescents and adults. If the findings from the phase 3 trial of M72 are positive, m72 will become the first new TB vaccine in over a hundred years to be proven safe and effective.
According to the most recent figures from the World Health Organization (WHO), around 304 000 people fell ill with TB in South Africa in 2021. While TB rates are declining, they are declining relatively slowly and according to the most recent WHO World TB Report, a major technological breakthrough such as a new vaccine will be needed if ambitious TB control targets are to be met.
Announcement welcomed
“We’ve waited a long time for this study, so are happy to see the Bill & Melinda Gates Foundation and Wellcome taking up this important task,” said Patrick Agbassi, chair of the Global TB Community Advisory Board, in a comment included in the Wellcome/BMGF statement. “The question now becomes how we can enroll 26 000 people most quickly and ensure that all populations at risk of TB will ultimately be able to benefit from access to what could be the first new TB vaccine in over 100 years. A robust community engagement programme will be key, as will taking on studying this vaccine in younger adolescents, pregnant women, people with prior history of TB, and other key groups often underrepresented or left out entirely of TB trials and the benefits of scientific progress.”
Mark Harrington, executive director of New York-based advocacy organisation Treatment Action Group (TAG) said, “TAG welcomes this historic investment in TB vaccine development by Wellcome and the Bill & Melinda Gates Foundation. A Phase III clinical trial of the M72/AS01E TB vaccine candidate is a long-awaited milestone. We hope this funding commitment sparks governments and other funders to substantially increase investments in the TB vaccine pipeline, which contains a number of promising candidates in addition to M72/AS01E but faces a dire financial shortfall.”
“This Phase III trial,” Harrington said, “will take several years to complete. We encourage the Gates Foundation, Wellcome, GSK, country governments, and other partners to use this time to lay the groundwork for eventual vaccine adoption by ensuring the availability, affordability, and acceptability of M72/AS01E should it prove safe and effective.”
Initial development of M72 was driven by the pharmaceutical company GSK with support from several governments, philanthropies, and research organisations. The vaccine contains the M72 recombinant fusion protein, which the Wellcome/BMGF statement explains is derived from two Mycobacterium tuberculosis antigens (Mtb32A and Mtb39A) combined with the GSK proprietary Adjuvant System AS01E. According to the statement, GSK will continue to provide the adjuvant for the vaccine’s further development and potential launch.
NOTES: (1) The BMGF is mentioned in this article. Spotlight receives funding from the BMGF, but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council. (2) A representative of the Global TB Community Advisory Board is quoted in this article. Spotlight editor Marcus Low was previously a member of the Global TB Community Advisory Board.







{kind=link}