An international clinical trial has found three new safe and effective drug regimens for tuberculosis that is resistant to rifampin, the most effective of the first-line antibiotics used to treat TB. The research, published in the New England Journal of Medicine, was led by researchers at Harvard Medical School and other members of the endTB project.
The newly identified regimens take advantage of recently discovered drugs to expand the treatment arsenal and give physicians new ways to shorten and personalise treatment, minimise side effects, and treat patients using only pills instead of daily injections. They also offer alternatives in case of drug intolerance, medication shortages or unavailability, or drug resistance, the researchers said.
The endTB trial is one of four recent efforts to use randomised controlled trials to test new, shorter, less toxic regimens for drug-resistant TB. endTB uses two new drugs – bedaquiline and delamanid — which, when brought to market in 2012-2013, were the first new TB medicines developed in nearly 50 years.
To find shorter, injection-free drug combinations for people infected with TB resistant to rifampin, endTB tested five new, all-oral 9-month regimens using the two new drugs in combination with older medications.
A third drug, pretomanid, received emergency authorisation from the FDA for specific use within a regimen against highly drug-resistant TB in 2019, after the endTB clinical trial was underway, and is not included in the regimens used in these trials.
Trial regimens were considered effective if they performed at least as well as the control group, which received a well-performing standard of care composed in accordance with a stringent interpretation of World Health Organization (WHO) recommendations.
The three successful new regimens were successful for between 85 and 90% of patients, compared with 81% success for people in the control group. The control group was treated with longer treatments, which also included the recently discovered medicines.
The trial launched in 2017 and enrolled 754 patients across seven countries: Georgia, India, Kazakhstan, Lesotho, Pakistan, Peru, and South Africa. The goal was to improve treatment for patients with tuberculosis resistant to rifampin. The WHO estimates that some 410 000 people become sick with rifampin-resistant TB each year, including people who have multidrug-resistant TB (MDR-TB). Only 40% are diagnosed and treated, 65%of them successfully.
The study population included children as well as people infected with HIV or hepatitis C, both common in populations with high rates of TB. In another innovation, women who became pregnant while on treatment were included in the endTB trial. These groups are often excluded from clinical trials. In a special report published in August 2024, the WHO added the three noninferior regimens from the endTB trial to the list of treatment options for rifampin-resistant and multidrug-resistant TB (MDR-TB) treatment; the recommendations extend to these neglected groups as well as to pregnant women.
With recent efforts to end patent exclusivity on bedaquiline, two of the endTB regimens and the WHO-recommended pretomanid-containing regimen can all be purchased for less than $500, an access target set by activists more than 10 years ago, which has only just now been achieved. All of these innovations together mean the new shortened, all-oral regimens are available to more people than ever.
Mycobacterium tuberculosis drug susceptibility test. Photo by CDC on Unsplash
Multidrug-resistant tuberculosis (MDR-TB) poses a particular threat to global health. A study led by the Swiss Tropical and Public Health Institute (Swiss TPH) shows that resistance to the new MDR-TB treatment regimen recently recommended by the World Health Organization is already spreading between patients. The findings, published in NEJM, highlight the urgent need for better surveillance and infection control to counteract the rise in antimicrobial resistance.
The traditional treatment regimen for MDR-TB is lengthy, expensive, and comes with severe adverse event. In 2022, the World Health Organization (WHO) endorsed a new 6-month regimen, the BPaL(M), based on evidence of its improved safety and efficacy from numerous clinical studies, including TB-PRACTECAL.
Monitoring the implementation of a new treatment regimen
“While this new regimen is a game changer for patients suffering from MDR-TB, we knew that it will be difficult to outsmart Mycobacterium tuberculosis, the bacteria causing TB,” said Sébastien Gagneux, Head of the Department Medical Parasitology and Infection Biology at Swiss TPH and senior author of the study. “It was therefore crucial to study how the TB bacteria would react to the global roll-out of this new regimen.”
This new study led by Swiss TPH in collaboration with the National Centre for Tuberculosis and Lung Diseases in Tbilisi, Georgia, now examined in detail whether resistance to the drugs in the new regimen has already emerged since its introduction, and whether this resistance is transmitting between patients.
Over a quarter of resistant strains result from transmission between patients
The researchers analysed the genomes of close to 90 000 M. tuberculosis strains from Georgia and many other countries around the world. They identified a total of 514 strains that were resistant to TB drugs, including both the old and the new treatment regimens. These highly drug-resistant strains were found in 27 countries across four continents.
Alarmingly, 28% of these strains were transmitted directly from one patient to another. “We already had anecdotal evidence of resistance emerging to the new regimen, but we did not know to what extent transmission was responsible for the spread of these highly drug-resistant strains,” said Galo A. Goig, postdoctoral collaborator at Swiss TPH and first author of the study.
“The good news is that the total number of these cases is still low. However, the fact that more than a quarter of these highly drug-resistant cases are due to patient-to-patient transmission, only two years after WHO endorsed the new regimen, is worrying,” added Goig.
Call for better surveillance and infection control
These findings have important implications for public health policy and interventions. “These new drugs have taken many years to develop, and to prevent drug resistance from emerging, it is essential to combine the deployment of these new regimens with robust diagnostics and surveillance systems,” said Chloé Loiseau, postdoctoral collaborator at Swiss TPH and co-author of the paper.
The authors emphasise the need for improved diagnostic tools, better infection control and robust surveillance systems to curb the spread of these highly drug-resistant strains, and to safeguard the efficacy of the new treatment regimen.
Tackling antimicrobial resistance
While there are already new TB drugs in the pipeline, experts worry that M. tuberculosis will continue to find ways to evade new drugs. “The example of these highly drug-resistant TB strains further illustrates that antimicrobial resistance is one of the most critical threats to global health today,” said Gagneux. “We must stay ahead in this constant race between drug development and bacterial resistance, and take proactive steps to prevent a ‘post-antibiotic era’ for TB and other diseases.”
Though several South African companies are producing HIV and TB medicines, the active ingredients that go into these medicines are usually imported from India or China. Now, a local company is planning to break new ground by making the active ingredients for two important TB medicines in Pretoria. We zoom in on the company’s efforts and outline some of the obstacles to getting such local production off the ground.
South Africa has a relatively robust pharmaceutical sector. Approximately 60% of the medicines sold in South Africa are locally produced, according to Dr Senelisiwe Ntsele, writing in an opinion piece for the Department of Trade, Industry and Competition (dtic).
But most of the time we are not producing these medicines from scratch. In fact, like most countries in the world, we mostly import the ingredients that make the medicines work – commonly referred to as active pharmaceutical ingredients, or APIs. In addition to APIs, medicines contain other inactive substances that maintain their form and structure and assist in their delivery: such as binders, stabilisers, and disintegrants.
Around 98% of the APIs used in locally formulated medicines are imported and South Africa spends around R15 billion a year importing APIs, according to Ntsele.
Government has tried to address South Africa’s dependence on imported APIs as part of its broader strategy to bolster the local pharmaceutical industry, which is identified as a priority sector for investment in the country’s Industrial Policy Action Plan. Several government departments provide support to the local pharmaceutical sector, including for local establishment of API manufacturing capacity. These departments include the dtic, the Department of Science and Innovation (DSI), the Technology Innovation Agency (TIA), and the Industrial Development Corporation (IDC) – South Africa’s development finance instrument.
In a bid to reduce the country’s reliance on imported APIs, Ketlaphela – a state-owned API manufacturing company – was announced in 2012. The plan was that Ketlaphela would produce APIs used in HIV medicines, but after multiple setbacks the initiative never got off the ground. Spotlight reported on the history of Ketlaphela in more detail here.
Turning to the private sector
Less well known than Ketlaphela, are government’s efforts to support API manufacturing capacity in the private sector. One private company that has received such government support and seem set to start delivering is Pretoria-based Chemical Process Technologies Pharma (CPT Pharma) that was established in 2014.
CPT Pharma is a subsidiary of Chemical Process Technologies, a company with many years of experience in chemical manufacturing and synthesis, including manufacturing of APIs for animal medicines. Human medicines, CPT Pharma’s core business, have stricter production management and quality control standards than those for animal medicines.
Dr Hannes Malan, Managing Director of CPT Pharma, told Spotlight that the company has 14 APIs in its pipeline, with a strong focus on TB medicines.
CCPT Pharma is a subsidiary of Chemical Process Technologies. (Photo: Supplied)
In 2023, the company secured a license from USAID to produce API for rifapentine, a drug widely used for TB prevention, and in 2022 they secured a licence from the Medicines Patent Pool to produce API for molnupiravir, a treatment for COVID-19. Malan pointed out that these two licenses were agreed with organisations aiming to expand the presence of API manufacturers in Africa – unlike typical arrangements driven by pharmaceutical companies looking to secure their own supply chains.
“For all the other APIs that we’re working on [beyond molnupiravir and rifapentine], we’re either working on technical packs [technical information about the API] that were available in the public domain or technologies that we’ve developed ourselves,” said Malan.
“Our approach has always been to look at the molecules, look at the market value, look at the technology, and then see if there’s an opportunity for us to develop technology that allows us to produce these compounds cost competitively,” he said.
“We really believe that to be competitive and independent, you have to have your own technology. Doing a technology transfer from Big Pharma does not make you independent,” Malan added.
How to fund it all?
In 2017, the company completed a pilot plant for making APIs. Then in 2020 it received approval from the South African Health Products Regulatory Authority (SAHPRA) to produce APIs for human use. The plant was built for R50 million, funded jointly by the IDC, TIA, and CPT Pharma.
Malan said that that the IDC and TIA also supported trial runs to test CPT Pharma’s manufacturing processes and technology. These tests included several APIs in development, such as isoniazid, a drug commonly used to prevent and treat TB.
The company has also secured funding from several international donors. The Gates Foundation provided support to develop manufacturing technology for the anti-malarial drug amodiaquine, as well as tuberculosis medicines bedaquiline and pretomanid. GIZ, a German development agency involved in a European Union project to boost vaccine and health product production in Africa, supported the company’s work on molnupiravir and dolutegravir – a widely used HIV medicine. USAID and the DSI are supporting the company’s work on developing rifapentine API manufacturing capacity.
Most of this financial support has been in the form of grants.
Still building new plants
While CPT Pharma has secured local and international funding to help construct a pilot plant and to develop its API manufacturing technology and processes, Malan said more investment is needed to support the construction of two commercial-scale manufacturing facilities: an isoniazid API manufacturing plant and a multiple API manufacturing facility.
Construction of the isoniazid manufacturing plant has already commenced using existing land and infrastructure with support from the IDC, but it is short of around R20 million to complete it, said Malan.
Although the plant is not yet operational, he said a company has already expressed interest in buying CPT Pharma’s locally produced isoniazid API. This company, said Malan, is contracted to supply isoniazid to government. The plan is to initially supply the company with isoniazid API produced at its pilot plant
Malan said the commercial plant, when built, will be able to manufacture enough isoniazid API to supply around 60% of local demand.
Things are less far down the road with plans for a plant to produce multiple different APIs at commercial scale, and more work is needed to understand the financing requirements for this type of facility, said Malan. “We want to do a bankable study and a concept design for such a plant,” he said. Based on CPT Pharma’s own experience, published data, and the required complexity and capacity of the plant, Malan said it is estimated that construction for the multi-API plant will cost around US$100 million or R1.8 billion.
Plans to commercialise
Meanwhile, the company is moving forward with plans to commercialise isoniazid and rifapentine API from its pilot plant. Isoniazid and rifapentine is increasingly used together as TB preventive therapy.
“For rifapentine, our pilot plant is seen as the commercial plant,” said Malan. “At this stage, we can use the pilot facility and the pilot reactor to produce enough rifapentine to get into the market and to grow the market.” But in the long term he said the company hopes to transfer rifapentine manufacturing to a larger commercial plant.
The company is also planning to apply for World Health Organization (WHO) pre-qualification status for its rifapetine API. The goal is to conduct demonstration runs in the pilot plant by June 2025 and validate the WHO pre-qualification application in September 2025.
If achieved, WHO pre-qualification of CPT Pharma’s rifapetine API would show that the company’s APIs meet high-quality standards. It would also allow CPT Pharma to supply rifapentine API to companies producing medicines for the broader African market, for which a significant proportion of medicines are procured by donors requiring WHO PQ approval.
Note: The Gates Foundation is mentioned in this article. Spotlight receives funding from the Gates Foundation. Spotlight is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council.
Scientists from the University of Leicester have discovered that tuberculosis disrupts glucose metabolism in the body. The findings, which have now been published in PLoSPathogens complement the understanding that diabetes worsens the symptoms of tuberculosis. Importantly, they now say, undiagnosed tuberculosis could be pushing vulnerable patients towards metabolic disease such as diabetes.
Tuberculosis (TB) remains one of the most devastating infectious diseases worldwide, killing over 4,000 people every day. Prevention through the development of improved vaccines remains a priority for the World Health Organisation. Currently only one vaccine exists for TB and this is predominantly given to infants and young children to help protect them from severe forms of infection.
Scientists at the University are researching tuberculosis in the hope of creating improved vaccines and are specifically looking at ways in which undiagnosed and subclinical infection can impact health. This new discovery, they say, could pave the way to define the molecular pathways by which the immune response changes liver metabolism, thereby allowing for the creation of targeted interventions.
She said: “Our paper changes the focus from diabetes making TB worse to the possibility that late diagnosis of TB can contribute to disruption of glucose metabolism, insulin resistance and therefore can promote progress towards diabetes in those that are susceptible.
“As diabetes compromises drug treatment, our paper also supports the idea that metabolic screening should be involved in any drug or vaccine trials.”
The study first used laboratory models of pulmonary TB to examine the changes happening within the liver during the early stages of infection. It found that an immune response was triggered within the liver cells and glucose metabolism was altered.
First author Dr Mrinal Das then reanalysed published metabolic data from humans, where he found that liver glucose metabolism was also disrupted when people progressed to TB from latent infection.
Professor Cooper added: “Our future aim is to define the molecular pathways by which the immune response is changing liver metabolism, allowing us to potentially create targeted interventions.
“We will also be investigating how latent TB (which is infection with the bacterial agent of TB without significant symptoms) might be impacting metabolic health in humans.”
A therapy showing promise to help control tuberculosis (TB) does not interfere with combined antiretroviral therapy (cART), according to research by Texas Biomedical Research Institute (Texas Biomed) which was recently published in JCI Insight.
“This is an important hurdle that this host-directed therapy had to clear in order to help patients battling both HIV and TB,” said study leader Professor Smriti Mehra, PhD of Texas Biomed.
TB is responsible for more than 1.3 million deaths worldwide every year. Dr. Mehra and her team have been investigating a therapy currently used in cancer as a potential treatment for patients with drug-resistant TB and/or comorbid HIV. While many cases of TB can be controlled with months of antibiotics, the infection can return in people who are immunocompromised as a result of HIV. Now that cART is so effective at controlling HIV, a resurging TB infection can often be deadly to those individuals.
Dr Mehra is studying a host-directed therapy that blocks or inhibits an immune system protein naturally found in the body. The protein, called IDO (short for Indoleamine-2,3-dioxygenase), normally suppresses the immune system, preventing it from causing excessive inflammation and organ damage. Inhibiting IDO for short intervals of time has led to more successful cancer treatments. Dr. Mehra’s team has previously shown the same approach improves control of TB in conjunction with antibiotics.
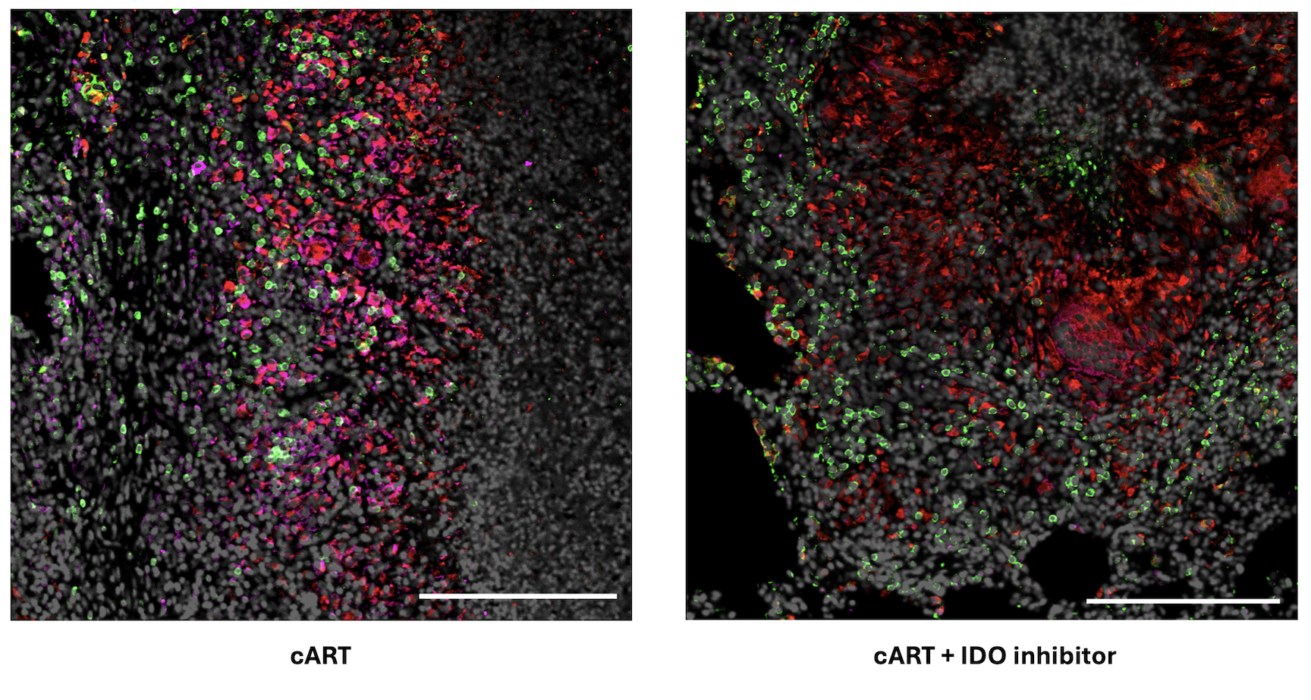
This current study in nonhuman primates with both TB and simian immunodeficiency virus, the nonhuman primate version of HIV, showed the IDO inhibitor does not interfere with cART.
Researchers compare the impacts of cART by itself versus cART plus the IDO inhibitor in lung tissue of nonhuman primates with both TB and SIV. Left: Following just cART, significantly more IDO is detected in pink. Right: With the IDO inhibitor and cART, immune cells recruited to fight bacteria are observed inside the granuloma, a hallmark structure of TB. Specifically, CD4+ T cells are in green and CD68 proteins expressed by macrophages are in red.
“There was no increase in viral load in animals given cART and the IDO inhibitor, compared with animals only given cART, proving the inhibitor is safe to give to patients with HIV,” Dr. Mehra said.
Now that the researchers have shown the inhibitor works well in conjunction with TB antibiotics and with cART separately, they plan to study how it performs when given in conjunction with both antibiotics and cART together. This treatment regimen is standard for patients with both HIV and active TB. Dr. Mehra said that longer-term studies are also needed to confirm there are no unintended side effects.
The IDO inhibitor is already FDA-approved for use in patients with cancer, which shortens the path to potential approval for patients with TB/HIV when compared with developing a brand-new drug.
Mycobacterium tuberculosis drug susceptibility test. Photo by CDC on Unsplash
A compound found in African wormwood – a plant used medicinally for thousands of years to treat many types of illness – could be effective against tuberculosis, according to a new study available online in the Journal of Ethnopharmacology.
The team, co-led by Penn State researchers, found that the chemical compound, an O-methylflavone, can kill Mycobacterium tuberculosis, or Mtb, that causes tuberculosis in both its active state and its slower, hypoxic state, which the mycobacteria enters when it is stressed.
Bacteria in this state are much harder to destroy and make infections more difficult to clear, according to co-corresponding author Joshua Kellogg, assistant professor of veterinary and biomedical sciences in the College of Agricultural Sciences.
While the findings are preliminary, Kellogg said the work is a promising first step in finding new therapies against tuberculosis.
“Now that we’ve isolated this compound, we can move forward with examining and experimenting with its structure to see if we can improve its activity and make it even more effective against tuberculosis,” he said. “We’re also still studying the plant itself to see if we can identify additional molecules that might be able to kill this mycobacterium.”
Tuberculosis is one of the world’s leading killers among infectious diseases, according to the Centers for Disease Control and Prevention. There are about 10 million cases a year globally, with approximately 1.5 million of those being fatal.
While effective therapies exist for TB, the researchers said there are several factors that make the disease difficult to treat. A standard course of antibiotics lasts six months, and if a patient contracts a drug-resistant strain of the bacteria, it stretches to two years, making treatment costly and time consuming.
Additionally, the bacteria can take two forms in the body, including one that is significantly harder to kill.
“There’s a ‘normal’ microbial bacterial form, in which it’s replicating and growing, but when it gets stressed – when drugs or the immune system is attacking it – it goes into a pseudo-hibernation state, where it shuts down a lot of its cellular processes until it perceives that the threat has passed,” Kellogg said. “This makes it really hard to kill those hibernating cells, so we were really keen to look at potential new chemicals or molecules that are capable of attacking this hibernation state.”
Multiple species of the Artemisia plant have been used in traditional medicine for centuries, the researchers said, including African wormwood, which has been used to treat cough and fever. Recent studies in Africa have suggested that the plant also has clinical benefits in treating TB.
“When we look at the raw plant extract that has hundreds of molecules in it, it’s pretty good at killing TB,” Kellogg said. “Our question was: There seems to be something in the plant that’s really effective – what is it?”
For their study, the researchers took raw extract of the African wormwood plant and separated it into “fractions” – versions of the extract that have been separated into simpler chemical profiles. They then tested each of the fractions against Mtb, noting whether they were effective or ineffective against the bacteria. At the same time, they created a chemical profile of all of the tested fractions.
“We also used machine learning to model how the changes in chemistry correlated with the changes in activity that we saw,” Kellogg said. “This allowed us to narrow our focus to two fractions that were really active.”
From these, the researchers identified and tested a compound that effectively killed the bacteria in the pathogen’s active and inactive states, which the researchers said is significant and rare to see in TB treatments. Further testing in a human cell model showed that it had minimal toxicity.
Kellogg said the findings have the potential to open new avenues for developing new, improved therapeutics.
“While the potency of this compound is too low to use directly as an anti-Mtb treatment, it may still be able to serve as the foundation for designing more potent drugs,” he said. “Furthermore, there appear to be other, similar chemicals in African wormwood that may also have the same type of properties.”
The researchers said that in the future, more studies are needed to continue exploring the potential for using African wormwood for treating TB.
A Competition Commission probe recently resulted in a patent on an important tuberculosis medicine being dropped in South Africa. Twenty years ago, a similar Competition Commission case resulted in a settlement that helped drive down the prices of several antiretrovirals, thereby helping to set the stage for the country’s HIV treatment programme. Fatima Hassan and Leena Menghaney connect the dots between the two landmark cases and map out what has and has not changed over the last two decades.
In the late 1990s and early 2000s, South Africa faced a major uncontrolled AIDS epidemic, worsened by state sponsored AIDS denialism. South Africa was at the epicentre of a global epidemic, with hundreds of thousands of people getting sick and dying, needlessly, because lifesaving antiretroviral medicines were out of reach.
This was in the main because of the Mbeki government’s deadly science denialism denying public sector patients antiretrovirals and the high cost of some of these medicines, which at the turn of the century was available in the private sector but only for the very rich or medically insured. The private sector price for the combination of three antiretrovirals needed by most people living with HIV was exorbitant.
This was because of patent monopolies held at the time by multinational pharmaceutical companies, particularly GlaxoSmithKline (GSK) and Boehringer Ingelheim (BI). In essence, people in South Africa living with HIV had to beg to live – by seeking donations and charity or pressuring their respective medical schemes to provide coverage. Meanwhile, lifesaving antiretrovirals were generally available in the Global North and in some parts of the Global South where governments like those in Thailand and Brazil had taken action to reduce prices.
Looking for a way to challenge the high prices of key antiretrovirals, activists turned to South Africa’s newly revamped post-apartheid competition law. In September 2002, the Treatment Action Campaign, Hazel Tau, a woman living with HIV and several others lodged a complaint with the country’s Competition Commission. They alleged that the price that GSK and BI were charging for important antiretrovirals was excessive and anti-competitive, undermining not just Competition Law but also the right to health as enshrined in the country’s still fairly new Constitution.
The Competition Commission agreed to investigate. Several months later, they announced that there was a prima facie case of excessive pricing and that they would be referring the matter to the Competition Tribunal (the next phase of a complaint to the Competition authorities). Almost immediately after that announcement, TAC was approached by GSK and BI to “settle” the matter. This meant there would be no public hearings, and the companies would not have to defend their pricing decisions in the dock.
The terms of the settlement, negotiated by the TAC’s legal team, mirrored what TAC had publicly demanded at the beginning of the case. Most importantly, GSK and BI agreed to grant voluntary licenses to several generic manufacturers that would allow them to make and sell the antiretrovirals in question. It was this generic competition that would drive down the prices of antiretrovirals in the years that followed.
Even though the Competition Commission only has jurisdiction in South Africa, the licenses included many other African countries, which meant those countries could also benefit from the generic competition and lower prices. The settlement (including the terms of the voluntary licenses) was agreed to by the Competition Commission, made an order and publicly announced, leading to the conclusion of the complaint.
The case, which came to be known as the Hazel Tau case, would in the years to come be recognised as one of the foundations that made large HIV treatment programmes possible in South Africa and other African countries. Despite this victory, the ongoing effects of AIDS denialism meant that it would in reality be several years before the more affordable generic antiretrovirals would be made widely available in South Africa.
20 years later, the spotlight is on TB drugs
HIV has not been the only health crisis to affect SA. According to the World Health Organization (WHO), Tuberculosis (TB) is one of the leading infectious causes of death globally, and drug-resistant TB (DR-TB) remains a public health crisis. The WHO estimates that around 304 000 people fall ill with TB in South Africa per year, and it claims over 50 000 lives, which means it remains one of the country’s top killers. While TB rates are slowly declining, there is concern that rates of drug-resistant forms of TB (DR-TB) are increasing. DR-TB requires newer, more expensive treatments.
Shared geographic origin between TB strain and human host could amplify risk for infection
Tuberculosis bacteria. Credit: CDC
For some forms of tuberculosis, the chances that an exposed person will get infected depend on whether the individual and the bacteria share a hometown, according to a new study comparing how different strains move through mixed populations in cosmopolitan cities.
Results of the research, led by Harvard Medical School scientists and published in Nature Microbiology, provide the first hard evidence of long-standing observations that have led scientists to suspect that pathogen, place, and human host collide in a distinctive interplay that influences infection risk and fuels differences in susceptibility to infection.
The study strengthens the case for a long-standing hypothesis in the field that specific bacteria and their human hosts likely coevolved over hundreds or thousands of years, the researchers said.
The findings may also help inform new prevention and treatment approaches for tuberculosis.
In the current analysis, believed to be the first controlled comparison of TB strains’ infectivity in populations of mixed geographic origins, the researchers custom built a study cohort by combining case files from patients with TB in New York City, Amsterdam, and Hamburg. Doing so gave them enough data to power their models.
The analysis showed that close household contacts of people diagnosed with a strain of TB from a geographically restricted lineage had a 14 percent lower rate of infection and a 45 percent lower rate of developing active TB disease compared with those exposed to a strain belonging to a widespread lineage.
The study also showed that strains with narrow geographic ranges are much more likely to infect people with roots in the bacteria’s native geographic region than people from outside the region.
The researchers found that the odds of infection dropped by 38 percent when a contact is exposed to a restricted pathogen from a geographic region that doesn’t match the person’s background, compared with when a person is exposed to a geographically restricted microbe from a region that does match their home country. This was true for people who had lived in the region themselves and for people whose two parents could each trace their heritage to the region.
This pathogen-host affinity points to a shared evolution between humans and microbes with certain biological features rendering both more compatible and fueling the risk for infection, the researchers said.
“The size of the effect is surprisingly large,” said Maha Farhat, the Gilbert S. Omenn, MD ’65, PhD Associate Professor of Biomedical Informatics in the Blavatnik Institute at HMS. “That’s a good indicator that the impact on public health is substantial.”
Why differences matter
Thanks to the growing use of genetic sequencing, researchers have observed not all circulating strains are created equal. Some lineages are widespread and responsible for much of the TB around the world, while others are prevalent only in a few restricted areas. Given that the complex nature of TB transmission in high-incidence settings where people often have multiple exposures to different lineages, researchers have not been able to compare strains under similar conditions and have been left to speculate about possible explanations for the differences between strains.
Many factors increase the risk of contracting tuberculosis from a close contact. One of the best predictors of whether a person will infect their close contacts is bacterial load, measured by a test called sputum smear microscopy, which shows how many bacteria a person carries in their respiratory system.
But the new study showed that for geographically restricted strains, whether a person has ancestors who lived where the strain is common was an even bigger predictor of infection risk than bacterial load in the sputum. In the cases analyzed in the study, this risk of common ancestry even outweighed the risk stemming from having diabetes and other chronic diseases previously shown to render people more susceptible to infection.
The findings add to a growing body of evidence of the importance of paying attention to the wide variation between different lineages of tuberculosis and to the details of how different lineages of tuberculosis interact with different host populations.
Previous studies have shown that some genetic groups of TB are more prone to developing drug resistance and that TB vaccines appear to work better in some places than others. There is also evidence that some treatment regimens might be better suited to some strains of TB than others.
“These findings emphasize how important it is to understand what makes different strains of TB behave so differently from one another, and why some strains have such a close affinity for specific, related groups of people,” said Matthias Groeschel, research fellow in biomedical informatics in Farhat’s lab at HMS; resident physician at Charité, a university hospital in Berlin; and the study’s first author.
In addition to the analysis of clinical, genomic, and public health data, the researchers also tested the ability of different strains of TB to infect human macrophages, a type of immune cell that TB hijacks to cause infection and disease. The researchers grew cells from donors from different regions. Once again, cell lines from people with ancestry that matched the native habitat of a restricted strain of tuberculosis bacteria were more susceptible to the germs than cells from people from outside the area, mirroring the results of their epidemiologic study.
Until now, most experiments of the interaction between human immune cells and TB have not compared how TB interacts with cells of hosts from different populations or places, the researchers said.
While this experiment was not designed to capture insights about the mechanism underlying the affinity between human and TB populations sharing geographic backgrounds, it highlights the importance of using multiple strains of TB and cells from diverse populations to inform treatment and prevention. It also points to the need for more basic research to understand the genomic and structural differences in how bacterial and host cells interface, the researchers said.
“It’s so important to appreciate that the great diversity of human and tuberculosis genetics can significantly impact how people and microbes respond to one another and to things like drugs and vaccines,” Farhat said. “We have to incorporate that into the way we think about the disease.”
“We’re at the very beginning of appreciating the importance of that diversity,” Groeschel said. “There’s so much more to learn about how it might impact the efficacy of drugs, vaccines, and the course that disease takes in different strains.”
Advances in gene sequencing create a new puzzle
While the closely related but distinct genetic groups of tuberculosis were discovered with more traditional methods of genotyping, the widespread use of whole genome sequencing by public health departments around the world allowed doctors and researchers to better profile TB germs and track outbreaks and drug resistance genetically.
The realization that highly localised stains didn’t spread well to other regions led researchers to speculate that regionally constrained strains were less infectious than widespread strains. Since the constrained strains persisted within their limited ranges, some researchers speculated that localised populations of the bacteria may have coevolved with their human hosts, making different human populations more susceptible to different types of TB. This could also mean, researchers hypothesised, that different strains of TB would have different susceptibility to different treatments and vaccines. For example, structural differences in the shape of the bacteria might prevent some drugs from binding effectively with bacteria from different strains.
Until recently, these hypotheses were nearly impossible to test, given the differences between cultural and environmental conditions that might affect infection rates in different communities and other parts of the world. Furthermore, the fact that the constrained stains strayed from home so rarely made it challenging to gather enough data to measure differences across strains.
Multidisciplinary science cracks the case
To overcome these obstacles, the research team collaborated with public health departments and research teams from the U.S., the Netherlands, and Germany to assemble a massive database integrating tuberculosis case reports, pathogen genetic profiles, and public health records of infection rates among close contacts. The analysis also incorporated demographic details about the social networks of infected people to assess how the different genetic lineages of tuberculosis spread in other populations. In total, the study included 5256 TB cases and 28 889 close contacts.
“This study is a great example of why it’s so important for researchers to collaborate with many different kinds of partners,” said Groeschel. “We were able to merge public health data from three big cities and use the powerful computational biology tools that we have access to in academic medicine to answer a complicated question that has important implications for public health and evolutionary biology, vaccine development, and drug research.”
Most tuberculosis (TB) tests still require a trip to the clinic. Now, new technology has made it possible to test people at home. This could be a big deal for South Africa, where much TB goes undiagnosed. We unpack the findings and implications of a recent study into such TB home testing.
One of the biggest challenges in combatting TB in South Africa is that many people who fall ill with the disease are diagnosed late, or not diagnosed at all.
The World Health Organization (WHO) estimates that 280 000 people fell ill with TB in the country in 2022. Of these, roughly 66 000 were not diagnosed, and accordingly also not treated. Apart from the damage to the health of the people who are not diagnosed and treated, this also has implications for the further spread of TB since untreated TB is often infectious TB – people become non-infectious within a few weeks of starting TB treatment.
Typically, people who fall ill with TB only get diagnosed once they turn up at clinics with TB symptoms – this is called passive case-finding. In recent years, there has been a growing recognition that passive case-finding alone is not good enough if we want to diagnose more people more quickly. As a result, many people in South Africa considered to be at high risk of TB are now offered TB tests whether or not they have symptoms – an approach called targeted universal testing. Screening for TB using new mobile X-ray technology has also been piloted in the country.
Now, in the latest such active case-finding innovation, researchers have been offering people TB tests in the comfort of their own homes.
Dr Andrew Medina-Marino, a senior investigator at the Desmond Tutu Health Foundation (DTHF), tells Spotlight no one in the world was testing for TB at home until they recently started doing so at the DTHF’s new research site in the Eastern Cape.
The testing is done using a molecular testing device, roughly the size of a two litre Coke bottle, called the GeneXpert Edge. The GeneXpert Edge is a portable version of the GeneXpert machines that have been used in labs across the country to diagnose TB for over a decade.
The GeneXpert Edge is a standardised testing device that detects TB DNA in sputum. (Photo: Nasief Manie/Spotlight)
One challenge with the device was that it needed to be plugged into a power outlet in a wall and not all homes in the area have power. “So what we did is, we hooked up a car-like battery to the device and we were able to take it into people’s homes,” says Medina-Marino.
‘Acceptable and feasible’
A study lead by Medina-Marino, and recently published in Open Forum Infectious Diseases, set out to determine the acceptability and feasibility of in-home testing of household contacts of people with TB.
The study was conducted among 84 households in Duncan Village, a township in the Buffalo City Metropolitan Municipality in the Eastern Cape. The Metro had an estimated TB incidence of 876 cases per 100 000 population in 2019, according to the National Institute for Communicable Diseases. This number is much higher than the latest WHO estimate of 468 per 100 000 for South Africa as a whole.
From July 2018 to May 2019, people diagnosed with pulmonary TB were recruited from six government health clinics in the area. They were asked for permission to visit their homes to screen their household contacts for TB. Household contacts were verbally assessed for signs or symptoms of TB, including night sweats, weight loss, persistent cough and a fever.
Households where people had any signs or symptoms of TB were randomised to either be referred to a local clinic for TB testing or tested immediately in their home. Of the eighty-four randomised households, 51 household contacts were offered in-home testing. Everyone accepted the offer for in-home testing.
For the test with the GeneXpert Edge, Medina-Marino says household contacts had to produce a sputum sample. About 47% (24/51) were able to produce sputum. This was then mixed with a reagent containing the required components for a polymerase chain reaction test. This solution was then loaded into a disposable cartridge/test module and inserted into the Edge device. Results were available in about 90 minutes. Anyone who received a positive test result in their home were immediately referred to a clinic for TB treatment.
Regarding the 47 household contacts referred for testing at the clinic, only 15% (7 people) presented for clinic-based TB evaluation, 6 were tested, and 4 out of 6 returned for their results.
Ultimately, the study found that in-home testing of household contacts for TB was acceptable and feasible.
“It’s feasible. If you compare the rate of uptake of treatment versus the rate of uptake for testing, it looks like it’s performing much better when you do home based testing versus referral for testing at the clinic,” says Medina-Marino.
Risk of stigma?
Similar to when HIV home-based testing studies were carried out, Medina-Marino says prior to their study, community members expressed concerns about stigmatising houses that were visited. “[A] lot of people were saying: ‘If you go to people’s houses, you’re going to stigmatise the household.’”
But what they actually found was that people didn’t feel stigmatised. Household contacts of people with TB felt that coming to the house to test people brought a sense of security in the home. He adds that it was easy for people to believe the results because everything was done in front of them.
In instances where people didn’t have TB, Medina-Marino says household contacts were comforted that they didn’t have to be scared of the person tested. In instances where people did have TB, he says the attitude of household contacts was supportive to start treatment.
How the test compares to other tests
Apart from testing for TB, the GeneXpert Edge can also detect whether someone’s TB is resistant to rifampicin. This is one of the medicines in the standard four-drug combination used to treat TB.
Unlike the latest lab-base GeneXpert tests, the GeneXpert Edge does not detect resistance to any TB medicines other than rifampacin. “It is hard to fit the probes needed to detect other forms of resistance into the cartridge,” says study co-author Professor Grant Theron, head of the Clinical Mycobacteriology and Epidemiology Research group at Stellenbosch University’s Molecular Biology and Human Genetics Unit.
Theron notes that the sensitivity and specificity of GeneXpert Edge is similar to that of lab-based GeneXpert machines if the tests are done on specimens from the same type of patient and the same test cartridge. (High sensitivity means the likelihood of false negatives is low wile high specificity means the likelihood of false positives is low.)
Performance may however differ because of differences between people who test at home and people who test at the clinic. Theron explains that in their study they tested people who did not yet feel sick enough to go to get tested at the clinic. People who are sicker, and who are accordingly more likely to go to the clinic, are likely to have more pathogen in their sputum samples and be easier to diagnose.
‘A breakthrough for TB’
Home-based tests is a significant breakthrough in TB because of its crucial role in detecting cases early and enabling timely tracing and testing of household contacts, says Dr Ntokozo Mzimela, a lecturer in integrated pathology in the Faculty of Health Sciences at Nelson Mandela University.
She tells Spotlight it also offers several advantages over clinic-based tests. “They are highly accessible, facilitate mass testing, reduce the risk of disease transmission, and address patient reluctance by allowing testing in the comfort and privacy of one’s home.”
Mzimela adds the GeneXpert Edge and portable X-ray screening serve complementary roles in TB diagnosis. “While the X-ray reveals lung abnormalities, the Edge confirms the presence of TB bacteria. Both tools are essential and should be used in conjunction to provide comprehensive diagnostic insights and ensure accurate and timely treatment for patients,” she says.
Professor Keertan Dheda agrees that home-based testing could link up neatly with portable X-ray, but adds it is still too early to determine where home-based TB testing will fit into the country’s TB testing programme. Dheda heads up the Division of Pulmonology at Groote Schuur Hospital and the University of Cape Town.
“We don’t yet know whether testing everyone is the right approach or whether reflex testing based on chest x-ray abnormalities is the right approach,” Dheda says. “Now that feasibility has been established, it means that more studies can be undertaken, and operational research can be commenced.”
Further studies are already underway, Medina-Marino tells Spotlight.
He says the study in Duncan Village found that about 60% of household contacts who had TB symptoms could not cough up a sputum sample. His team therefore decided to combine in-home testing with an oral swab.
“So in the study that we’re doing now in households, we found an additional 12 people who cannot produce sputum but on their swab test, they showed a positive swab result. Tongue swabs increase yield of case finding among those unable to produce sputum,” he says.
Besides preventing illness and death, tuberculosis prevention therapy is estimated to be highly cost effective. Yet, uptake of the medication is not what it could be in South Africa. Tiyese Jeranji asks how much has changed since the Department of Health last year decided to make TB prevention therapy much more widely available.
Many people who have the TB bug in their lungs are not ill with TB disease. Having the bug in your body, does mean however that you are at risk of falling ill, should the TB bacteria get the overhand in its battle with your immune system.
Fortunately, we have medications that can kill TB bacteria before one falls ill. A recent World Health Organization (WHO) investment case, suggests such TB prevention therapy, commonly called TPT, reduces the risk of falling ill with TB in those exposed to the bug by 60% to 90% compared to people who do not get the treatment.
In South Africa, TPT has been available in the public sector for years, but until the publication of new government guidelines last year, only kids aged five or younger and people living with HIV could get the medication. Under the new guidelines, everyone who has had close contact with someone with TB should be offered a TB test and if they test negative be offered TPT – if they test positive they should be offered TB treatment. These changes dramatically expanded the number of people in South Africa who are eligible for TPT.
The antibiotics used for TPT has also changed in recent years. For many years, the only option was a medication called isoniazid taken for six or more months. We now also have two three-month options – isoniazid and rifapentine given once weekly and rifampicin and isoniazid given daily. These shorter duration treatment courses should help more people complete the treatment.
Down and up?
Dr Norbert Ndjeka, Chief Director of TB Control and Management at the National Department of Health, tells Spotlight that in recent years, South Africa has seen a steady decline in the number of people initiated on TPT.
The decline has been substantial. In people living with HIV, initiation on TPT dropped from 454 000 in 2018 to around 241 000 in 2023. In children aged five and younger who have had contact with someone with TB, it fell from 25 357 in 2018 to 15 775 in 2023.
TPT enrolments per province for 2023
Province
People living with HIV
Contacts < 5 Years
Contacts > 5 Years
Eastern Cape
34 623
2 551
4 771
Free State
14 535
562
1 027
Gauteng
67 333
1 368
4 241
KwaZulu-Natal
62 362
3 168
8 519
Limpopo
15 871
391
452
Mpumalanga
25 618
669
2 006
Northern Cape
3 178
855
1 595
North West
9 433
596
1 425
Western Cape
8 532
5 615
1 278
South Africa
241 485
15 775
25 314
*Typically, provinces with higher numbers of people diagnosed with TB or those with high numbers of people living with HIV will report higher TPT initiations.
There are two significant reasons for this decline, according to Ndjeka. Firstly, declining TB incidence, and secondly, declining HIV incidence.
“With fewer people diagnosed with TB disease, fewer contacts will need TPT, and with fewer people being diagnosed with HIV, fewer people will initiate TPT regardless of TB exposure,” he says.
WHO figures have shown a significant downward trend in the estimated TB cases per year in South Africa and according to Thembisa, the leading mathematical model of HIV in South Africa, the number of people newly starting HIV treatment has dropped from a peak of over 700 000 in 2011, to well under 300 000 in 2023.
But the recent downward trend in people taking TPT may be coming to an end. “We believe that the implementation of the new guidelines within the current strategic framework will lead to increases in TPT enrolment,” says Ndjeka.
In line with the new guidelines, there are also changes to what TPT data is being collected. “For example, we never used to report on TPT provision to contacts 5 years and older, but now we do and in 2023 at least 25 314 TB contacts 5 years and older were initiated on TPT,” he says.
20% increase expected in 2024
Based on the data reported for January and February of this year, Ndjeka expects that overall TPT initiations will increase by at least 20% in 2024 compared to 2023. Moreover, as documented in the National Strategic Plan for HIV, TB and STIs 2023-2028, there is a plan to have a steady annual increase in TPT enrolments leading up to 2028.
Ndjeka says based on the NSP TPT targets, South Africa is exceeding TPT targets for people living with HIV, but reaching less than 25% of targets for TB contacts. He points out that performance varies by province, but that all provinces have a long way to go in terms of reaching TB contacts.
‘Cost saving over time’
“The aim of offering TPT is to reduce the TB incidence,” Ndjeka says. “So, if everyone eligible is offered TPT there will obviously be increased costs initially but cost saving over time. This looks at cost of treating people with TB, lives saved/ deaths prevented as well as costs to patients.”
For South Africa, he says, it is estimated that we can reduce the number of people with TB by 138 000 by 2050 at an estimated cost of R23 226.90 per TB episode prevented.
Ndjeka says it costs the health department an estimated at R1 498.51 to treat one person with drug-susceptible TB for 6 months and R16 612.82 to treat one person with the standard drug-resistant TB treatment for 6 months. “These costs are for medications alone, which can also go beyond R70 000 depending on the patient and the type of resistant TB. Moreover, when factoring in clinical consultations, hospitalisations, and costs to patients the costs go up considerably,” he says.
The cost of providing TPT also depends on the regimen. One person on TPT can cost as little as R608.77 for a course of three months of isoniazid and rifapentine given once weekly, and up to R1 358.02 for 12 months of isoniazid. “TPT also has much lower associated costs for example there is no hospitalisation, fewer clinic visits and consultations,” Ndjeka says.
“By preventing TB, the cost of TB treatment is avoided along with the costs of treating some of the acute and chronic conditions that someone with TB may experience even after being cured of TB. These include chronic obstructive pulmonary disease, bronchiectasis and pneumonia,” says Alison Best, communication manager at Cape Town-based NGO TB HIV Care.
“For children under five in particular, who are at increased risk of disseminated TB like TB meningitis, the cost of not preventing TB could be death or severe lifelong disability,” she says, adding that preventing TB in a single individual also prevents the costs associated with any onwards transmission of TB from that individual to others.
Questions over implementation
Expanded TPT eligibility has been widely welcomed, but questions have been raised over how well the new guidelines are being implemented.
Best says government austerity measures have made implementing new initiatives in the healthcare setting challenging.
“There is not much political will to implement the guidelines (to expand eligibility for TPT) at provincial and district levels and this has translated into the slow release of circulars, delays in training health workers, poor knowledge of the policy and its low prioritisation,” she says.
Ingrid Schoeman, Director of Advocacy and Strategy at TB Proof (a local advocacy group), says often when a national policy is released, there are delays at provincial-level in releasing circulars to enable health worker training.
“This results in these services not being available at district-level. In the Western Cape, civil society organisations, the [provincial] Department of Health, City of Cape Town and implementing partners are now all working together to support health worker training, and implementing community-led awareness campaigns so that all close TB contacts know they are eligible for TPT,” she says.
Best adds that tracking the data to show how many people are starting and completing TPT tends to be difficult. She notes there are many gaps in capturing the information. This includes, at times, the limited recording of information in patient folders by clinicians and suboptimal inputting of data by data capturers.
Ndjeka says the national department of health has been conducting training on the new guidelines with provincial and district TB and HIV programme managers, district support partners and other trainers.
“They are then responsible for training health care workers. The antiretroviral therapy guideline training also includes TPT. Webinars on the knowledge hub (an online training platform) have also conducted,” he says.
However, Ndjeka conceded that there is a lack of awareness about the value of TPT. “Additionally,” he says, “there is reluctance from clinicians to provide TPT. This result in poor demand for TPT. Treatment adherence is another problem especially for people on the long regimen (12 months)”.
Plans to address these challenges, among other things, include marketing TPT as treatment for TB infection rather than prevention, targeted communication strategies, community mobilisation, and ongoing training and mentoring of healthcare workers, says Ndjeka.