Ischaemic and haemorrhagic stroke. Credit: Scientific Animations CC4.0
A new study by researchers at the Department of Molecular Medicine at SDU sheds light on one of the most severe consequences of stroke: damage to nerve fibres – the brain’s “cables” – which leads to permanent impairments. The study, which is published in the Journal of Pathology, used unique tissue samples from Denmark’s Brain Bank located at SDU, may pave the way for new treatments that help the brain repair itself.
The brain tries to repair damage
Following an injury, the brain tries to repair the damaged nerve fibres by re-establishing their insulating myelin sheaths. Unfortunately, the repair process often succeeds only partially, meaning many patients experience lasting damage to their physical and mental functions. According to Professor Kate Lykke Lambertsen, one of the study’s lead authors, the brain has the resources to repair itself. “We need to find ways to help the cells complete their work, even under difficult conditions,” Prof Lykke said.
The researchers have thus focused on how inflammatory conditions hinder the rebuilding. The study has identified a particular type of cell in the brain that plays a key role in this process. These cells work to rebuild myelin, but inflammatory conditions often block their efforts.
How researchers used the brain collection
-Using the brain collection, we can precisely map which areas of the brain are most active in the repair process, explains Professor Kate Lykke Lambertsen.
This mapping has enabled researchers to analyse tissue samples from Denmark’s Brain Bank and gain a deeper understanding of the mechanisms that control the brain’s ability to heal itself.
Through advanced staining techniques, known as immunohistochemistry, the researchers have been able to detect specific cells that play a central role in the reconstruction of myelin in the damaged areas of the brain.
The samples were analysed to distinguish between different areas of the brain, including the infarct core (the most damaged area), the peri-infarct area (surrounding tissue where rebuilding is active), and tissue that appears unaffected.
The analysis provided insight into where repair cells accumulate and how their activity varies depending on gender and time since the stroke.
Women and men react differently
An interesting discovery in the study is that women’s and men’s brains react differently to injuries.
-The differences underscore the importance of future treatments being more targeted and taking into account the patient’s gender and individual needs, says Kate Lykke Lambertsen.
In women, it seems that inflammatory conditions can prevent cells from repairing damage, while men have a slightly better ability to initiate the repair process. This difference may explain why women often experience greater difficulties after a stroke.
The brain collection at SDU is key to progress
The researchers behind the study emphasise that the discoveries could not have been made without the Danish Brain Bank at SDU. The collection consists of tissue samples from humans, used to understand brain diseases at a detailed level.
With access to this resource, researchers can investigate the mechanisms behind diseases like stroke and develop new treatment strategies.
Ischaemic and haemorrhagic stroke. Credit: Scientific Animations CC4.0
People who have had a stroke may be more likely to sleep too much or too little compared to those without prior stroke, according to a study published in Neurology®, the medical journal of the American Academy of Neurology. The study does not prove that stroke causes abnormal sleep; it only shows an association.
“Sleeping the right amount is considered essential for ideal brain and heart health,” said study author Sara Hassani, MD, of Duke University School of Medicine in Durham, North Carolina, and member of the American Academy of Neurology. “We know that abnormally long or short sleep after stroke can affect recovery and deteriorate quality of life, so these results should prompt us to screen for these issues and look at how we can help people improve their sleep habits.”
The study involved 39 559 participants, of whom 1572 had a stroke and 37 987 without stroke history. Every two years, participants were asked how much sleep they usually get at night on weekdays or workdays. Sleep duration was divided into three categories: short, less than six hours; normal, six to eight hours; and long, eight or more hours of sleep.
Researchers looked at how often participants had normal sleep, defined as six to eight hours. Normal sleep duration was less common for people who had a stroke than for those with no prior stroke for all age groups with 32% vs 54% for people age 18-44; 47% vs 55% for people age 45-64; and 45% vs. 54% for people over age 65.
After adjusting for factors that could affect sleep such as age, weight and high blood pressure, researchers found people who had a stroke were 54% more likely to report more than eight hours of sleep per night compared to those without stroke. Those with stroke were 50% more likely to get less than six hours of sleep per night when compared to those without stroke.
“In previous research, stroke has been linked to abnormal sleep, in particular sleep apnea,” said Hassani. “Conditions like insomnia and excessive sleepiness are common in stroke patients and may occur as a direct or indirect consequence of stroke itself. Future research should explore the links between stroke and duration of sleep and determine the effect of sleep duration on outcomes after stroke.”
One limitation of the study was that hours of sleep were self-reported, so participants may not have remembered accurately how much they slept.
Nurses play a key role in helping patients manage emotional and social health challenges, or psychosocial health, after a stroke, and improved screening and assessment for psychosocial needs are essential to provide optimal patient care. These findings are highlighted in a new statement from the American Stroke Association, a division of the American Heart Association, published in the Association’s peer-reviewed scientific journal Stroke.
While there have been significant advances in stroke prevention and treatment, stroke remains the second leading cause of death globally and a major cause of disability. The latest research indicates that 16% to 85% of stroke survivors experience psychosocial symptoms, such as depression, anxiety, stress, fatigue and/or a decreased quality of life during their recovery.
“Stigma often surrounds discussions about psychosocial health. Therefore, it is crucial for nurses and all health care professionals to create a safe and therapeutic environment for patients and offer hope and comprehensive education on the topic,” said Chair of the scientific statement’s writing group Patricia A. Zrelak, PhD, RN, FAHA, a regional stroke program quality nurse consultant for Kaiser Permanente Northern California and a member of the American Heart Association’s Council on Cardiovascular and Stroke Nursing.
The scientific statement details a comprehensive review of the latest evidence published from 2018-2023 about psychological health in patients who experienced a stroke. The statement addresses the effects, underlying causes, screening, diagnosis and treatment for five key emotional and social health factors, including depression, stress, anxiety, fatigue and quality of life. The scientific statement aims to establish a guide for nursing care throughout a patient’s recovery after a stroke, from prevention of adverse psychosocial health conditions to identifying and managing symptoms.
“Emotional, cognitive, behavioural and/or personality changes may occur after a stroke,” Zrelak said. “These conditions can emerge immediately after a stroke or have a delayed onset, sometimes occurring more than a year later, and they may also fluctuate in intensity over time. In addition, psychosocial symptoms are interrelated, and patients who experience one are at higher risk of developing other mental health conditions. Effective and regular screening are vital for early detection and treatment.”
Depression
Depression affects about 30% of stroke survivors and is particularly common within the first three months after a stroke. Symptoms of depression may include persistent sadness, anxious or “empty” mood; restlessness and irritability; loss of interest or pleasure in hobbies and activities; difficulty in concentrating and thinking; increased or decreased sleep; changes in appetite; and weight gain or loss. Post-stroke depression worsens cognitive and functional recovery and increases the risks of death and/or another stroke.
The AHA/ASA Guidelines for the Early Management of Patients With Acute Ischemic Stroke recommend routine depression screening for all patients after a stroke. Nurses can help educate stroke survivors and their families on symptom recognition, prevention and treatment options, such as medication management and/or cognitive behavioural therapy.
Stress
A 2022 study found that post-stroke stress and post-traumatic stress disorder (PTSD) affects about one in six (about 16.5%) stroke survivors. These conditions may increase the risk of additional health issues, including anxiety and poor medication adherence. Screening stroke patients for stress and PTSD should occur when they are hospitalised and continue during rehabilitation and outpatient visits after hospital discharge.
Nursing interventions that may help lower patients’ distress include stroke education and self-management strategies, such as mindfulness and meditation. Nurses may also consider stroke survivors’ coping styles. People with high-anxious coping styles face a significantly higher risk of experiencing PTSD after a stroke in comparison to people with low-anxious coping styles.
Anxiety
The frequency of anxiety ranges from 20%-25% in the first months after stroke, increasing to 32% as the year progresses, with a five-year prevalence of 34%. Factors such as younger age at the time of the stroke, lower income, inability to work, social isolation, previous mental health conditions and/or severity of the stroke are factors that increase the risk of developing anxiety. Anxiety is also linked to a higher risk and severity of depression.
Standard screening for anxiety and prompt detection may lead to early treatment, greater patient engagement and improved recovery for stroke survivors. Although established clinical guidelines for treating general anxiety exist, more research is needed on anxiety interventions after different types of strokes.
Fatigue
Post-stroke fatigue may develop anytime, however, it is most common within the first six months after a stroke. Symptoms of fatigue may include reduced physical and mental energy levels that interfere with daily activities and difficulty with self-control, emotions and memory. Women and people with depression, sleep problems, anxiety and/or multiple health conditions are at higher risk for developing post-stroke fatigue.
More research is needed for effective management strategies for post-stroke fatigue, as there are currently no proven treatments. However, interventions focused on improving general physical fitness may help prevent, reduce or treat post-stroke fatigue and other components of psychosocial health.
Quality of life
Returning to the same quality of life after a stroke is challenging and even more so after a severe stroke. Physical strength, speech, depression, anxiety and the ability to return to work and social activities are factors that contribute to a stroke survivor’s quality of life. However, conditions such as chronic pain can negatively impact recovery and return to independent living.
Physical activities that also include interpersonal engagement, such as yoga and tai chi, have shown positive effects on patients’ quality of life. Nurses can help stroke survivors improve their post-stroke quality of life by linking patients to social services in their local area, such as post-stroke support groups and community-based organisations.
“Mental and emotional well-being are crucial for recovery, and nurses play an important role in supporting patients after a stroke,” Zrelak said. “It’s important to engage stroke survivors and their caregivers so they are aware of these psychosocial conditions and ways they can help. Early detection of symptoms and treatment have the potential to improve post-stroke recovery.”
The statement also highlights existing research that shows stroke outcomes vary significantly among people in different racial and ethnic groups. Social determinants of health, such as structural racism, socioeconomic status, inadequate housing and/or limited access to health care including mental health services, may all influence a stroke survivor’s recovery.
Zrelak added, “The stroke care team is crucial in addressing these health inequities, using targeted interventions and customised treatments to improve mental health support and overall care coordination for those most at risk. More research is needed to help us understand how best to support psychosocial well-being for people after a stroke, so they are better able to return to their routine daily activities and have a better quality of life.”
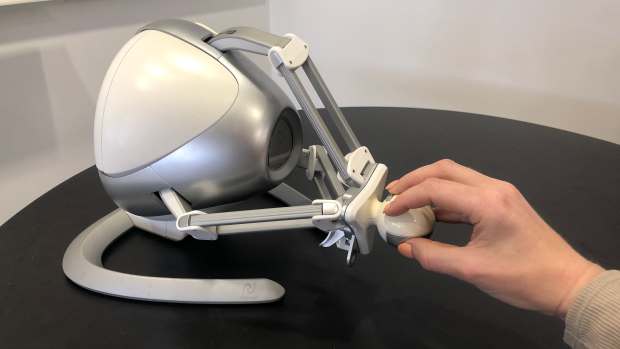
The Novint Falcon, a desktop robot typically used for video games, can guide users through specific arm motions and track the trajectory of its controller.
For recovering stroke survivors, getting intensive, frequent rehabilitation therapy to help restore fine motor skills can be challenging and expensive.
Now, researchers at NYU Tandon School of Engineering are developing a new technology that could allow stroke patients to undergo rehabilitation exercises at home by tracking their wrist movements through a simple setup: a smartphone strapped to the forearm and a low-cost gaming controller called the Novint Falcon.
The Novint Falcon, a desktop robot typically used for video games, can guide users through specific arm motions and track the trajectory of its controller. But it cannot directly measure the angle of the user’s wrist, which is essential data for therapists providing remote rehabilitation.
“Patients would strap their phone to their forearm and manipulate this robot,” said Maurizio Porfiri, NYU Tandon Institute Professor and director of its Center for Urban Science + Progress (CUSP), who is the paper’s senior author. “Data from the phone’s inertial sensors can then be combined with the robot’s measurements through machine learning to infer the patient’s wrist angle.”
The researchers collected data from a healthy subject performing tasks with the Falcon while wearing motion sensors on the forearm and hand to capture the true wrist angle. They then trained an algorithm to predict the wrist angles based on the sensor data and Falcon controller movements.
The resulting algorithm could predict wrist angles with over 90% accuracy, a promising initial step toward enabling remote therapy with real-time feedback in the absence of an in-person therapist.
“This technology could allow patients to undergo rehabilitation exercises at home while providing detailed data to therapists remotely assessing their progress,” Roni Barak Ventura, the paper’s lead author who was an NYU Tandon postdoctoral fellow at the time of the study. “It’s a low-cost, user-friendly approach to increasing access to crucial post-stroke care.”
The researchers plan to further refine the algorithm using data from more subjects. Ultimately, they hope the system could help stroke survivors stick to intensive rehab regimens from the comfort of their homes.
This study adds to NYU Tandon’s body of work that aims to improve stroke recovery. In 2022, Researchers from NYU Tandon began collaborating with the FDA to design a regulatory science tool based on biomarkers to objectively assess the efficacy of rehabilitation devices for post-stroke motor recovery and guide their optimal usage. A study from earlier this year unveiled advances in technology that uses implanted brain electrodes to recreate the speaking voice of someone who has lost speech ability, which can be an outcome from stroke.
Cerebrovascular accidents, or strokes, are the most common cause of aphasia, a speech disorder of cerebral origin. People with aphasia have a reduced ability to understand or produce speech or written language. An estimated 40% of people who have had a stroke have aphasia. As many as half of them experience aphasia symptoms even a year after the original attack.
Researchers at the University of Helsinki previously found that sung music helps in the language recovery of patients affected by strokes. Now, the researchers have uncovered the reason for the rehabilitative effect of singing. The recently completed study was published in the eNeuro journal.
According to the findings, singing, as it were, repairs the structural language network of the brain. The language network processes language and speech in the brain, which has been damaged.
“For the first time, our findings demonstrate that the rehabilitation of patients with aphasia through singing is based on neuroplasticity changes, that is, the plasticity of the brain,” says University Researcher Aleksi Sihvonen from the University of Helsinki.
Singing improves language network pathways
The language network encompasses the cortical regions of the brain involved in the processing of language and speech, as well as the white matter tracts that convey information between the different end points of the cortex.
According to the study results, singing increased the volume of grey matter in the language regions of the left frontal lobe and improved tract connectivity especially in the language network of the left hemisphere, but also in the right hemisphere.
“These positive changes were associated with patients’ improved speech production,” Sihvonen says.
A total of 54 aphasia patients participated in the study, of whom 28 underwent MRI scans at the beginning and end of the study. The researchers investigated the rehabilitative effect of singing with the help of choir singing, music therapy and singing exercises at home.
Singing is a cost-effective treatment
Aphasia has a wide-ranging effect on the functional capacity and quality of life of affected individuals and easily leads to social isolation.
According to Sihvonen, singing can be seen as a cost-effective addition to conventional forms of rehabilitation, or as rehabilitation for mild speech disorders in cases where access to other types of rehabilitation is limited.
“Patients can also sing with their family members, and singing can be organised in healthcare units as a group-based, cost-efficient rehabilitation,” Sihvonen says.
A new study by a global team of researchers has revealed that areas of age-related damage in the brain relate to motor outcomes after a stroke – a potentially under-recognised phenomenon in stroke research. The study was published in Neurology.
A stroke often leads to motor impairment, which is traditionally linked to the extent of damage to the corticospinal tract (CST), a crucial brain pathway for motor control. Signaling along the CST is involved in a variety of movements, including walking, reaching, and fine finger movements like writing and typing. However, stroke recovery outcomes aren’t fully predicted by damage to the CST, suggesting other factors are at play.
The new observational from the Enhancing Neuroimaging Genetics through Meta-Analysis (ENIGMA) Stroke Recovery working group. It examines how one such factor could be white matter hyperintensities (WMHs) – areas of age-related damage in the brain’s white matter, which represent vascular dysfunction and are known to impact cognitive functions. The goal of the ENIGMA Stroke Recovery working group is to understand how changes in the brain after stroke relate to functional outcomes and recovery. ENIGMA Stroke Recovery has data from over 2100 stroke patients collected across 65 research studies and 10 countries, comprising the most extensive multisite retrospective stroke data collaboration to date.
Study leader Sook-Lei Liew, PhD, said: “We are grateful for our many collaborators around the world who lead independent stroke research programs and who are willing to come together and enable large-scale investigations into these critical questions about the role of overall brain health in stroke recovery and rehabilitation.” Dr Liew is an associate professor at the Keck School of Medicine of USC.
The study analysed data from 223 stroke patients across four countries and found that larger WMH volumes were associated with more severe motor impairment after a stroke (e.g., difficulty moving or using their arm for daily tasks), independent of CST damage. WMHs are related to chronic hypertension, diabetes, high cholesterol, and smoking, among other factors and conditions, and have been strongly related to cognitive impairment, but not extensively studied in the context of motor impairment. Interestingly, the relationship between CST damage and motor impairment varied based on WMH severity. Patients with mild WMHs showed a typical relationship between CST damage and motor impairment, while patients with moderate to severe WMHs did not have this relationship. Instead, motor impairment was related to WMH volume, not CST damage.
These findings suggest that WMHs, indicative of cerebrovascular damage from a variety of sources, could provide additional context to understand an individual’s potential for recovery post-stroke. Therefore, assessing WMH volume could improve predictive models for stroke recovery.
“WMHs are related to overall cardiovascular and brain health as we age. By integrating assessments of age-related brain health, we may be better able to predict stroke recovery and tailor rehabilitation to individual needs. This personalised approach could open avenues to improve outcomes after stroke,” says lead author Jennifer K. Ferris, PhD, of Simon Fraser University.
The researchers’ next step is to pursue longitudinal studies to confirm their findings. This insight lays the groundwork for developing more accurate markers for recovery, which could transform post-stroke care and rehabilitation.