Antibiotic resistance tends to stabilise over time, according to a study published April 3, 2025 in the open-access journal PLOS Pathogens by Sonja Lehtinen from the University of Lausanne, Switzerland, and colleagues.
Antibiotic resistance is a major public health concern, contributing to an estimated 5 million deaths per year. Understanding long-term resistance patterns could help public health researchers to monitor and characterise drug resistance as well as inform the impact of interventions on resistance.
In this study, researchers analysed drug resistance in more than 3 million bacterial samples collected across 30 countries in Europe from 1998 to 2019. Samples encompassed eight bacteria species important to public health, including Streptococcus pneumoniae, Staphylococcus aureus, Escherichia coli, and Klebsiella pneumoniae.
They found that while antibiotic resistance initially rises in response to antibiotic use, it does not rise indefinitely. Instead, resistance rates reached an equilibrium over the 20-year period in most species. Antibiotic use contributed to how quickly resistance levels stabilised as well as variability in resistance rates across different countries. But the association between changes in drug resistance and antibiotic use was weak, suggesting that additional, yet unknown, factors are at play.
The study highlights that continued increase in antibiotic resistance is not inevitable and provides new insights to help researchers monitor drug resistance.
Senior author Francois Blanquart notes: “When we looked into the dynamics of antibiotic resistance in many important bacterial pathogens all over Europe and in the last few decades, we often found that resistance frequency initially increases and then stabilises to an intermediate level. The consumption of the antibiotic in the country explained both the speed of initial increase and the level of stabilisation.”
Senior author Sonja Lehtinen summarises: “In this study, we were interested in whether antibiotic resistance frequencies in Europe were systematically increasing over the long-term. Instead, we find a pattern where, after an initial increase, resistance frequencies tend to reach a stable plateau.”
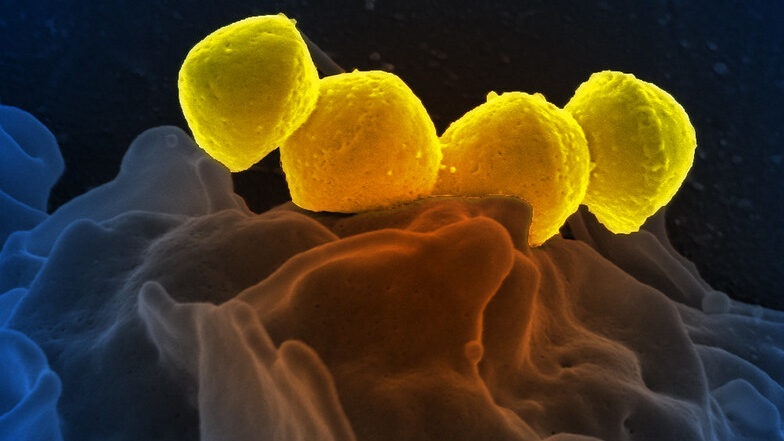
Streptococcus Pyrogenese bound To human neutrophil. Credit: NIH
A new study published in Nature Communications reveals a novel approach to mitigating tissue damage caused by Streptococcus pyogenes, the flesh-eating bacterium responsible for severe infections such as necrotising fasciitis. The research highlights how disrupting bacterial metabolism can help the body better tolerate infection and heal more effectively.
The study was led by Wei Xu, PhD, an assistant professor of biomedical sciences at the Marshall University Joan C. Edwards School of Medicine, and colleagues at Washington University School of Medicine and Central China Normal University. The team discovered that S. pyogenes manipulates the body’s immune response through its aerobic mixed-acid fermentation process, which produces metabolic byproducts, such as acetate and formate, that impair immune cell function, delay bacterial clearance and slow wound healing.
By inhibiting this bacterial metabolic pathway with a pyruvate dehydrogenase inhibitor, the team successfully reduced tissue damage in a mouse model of necrotising skin infection. These findings suggest that reprogramming bacterial metabolism could serve as a novel therapeutic approach, not only to improve host tolerance but also as a potential adjuvant therapy alongside antibiotics. This strategy could enhance the effectiveness of existing treatments, particularly in severe infections where antibiotic resistance or excessive inflammation worsens patient outcomes.
“This study sheds light on how bacterial metabolism influences the immune system,” Xu said. “By understanding these interactions, we can develop new treatment strategies that protect tissues, enhance antibiotic efficacy and improve patient outcomes.”
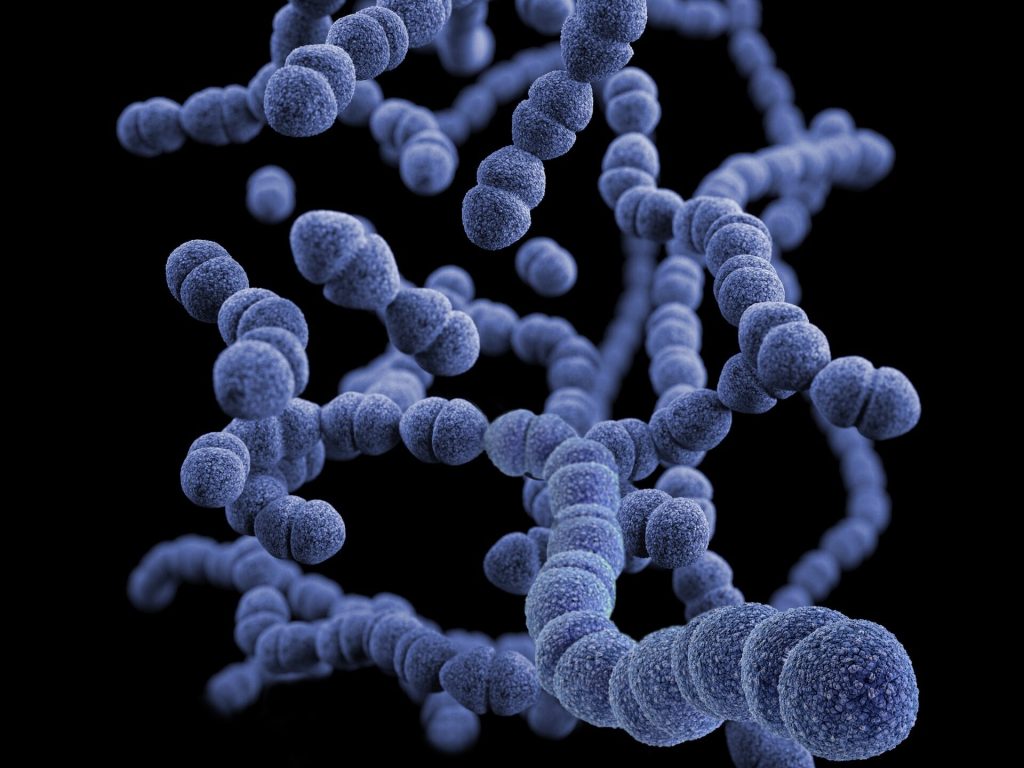
This illustration depicted a three-dimensional (3D), computer-generated image, of a group of Gram-positive, Streptococcus pneumoniae bacteria. The artistic recreation was based upon scanning electron microscopic (SEM) imagery.
Doctors typically treat paediatric ear infections with antibiotics, but children don’t always complete the full course, accelerating resistance to these medications. Today, researchers report developing a single-use nanoscale system that’s unlikely to generate resistance. Using a compound similar to bleach in test animals, they show it can kill off Streptococcus pneumoniae, a common cause of ear infections, and it could someday be easily applied as a gel.
The researchers will present their results at the meeting of the American Chemical Society (ACS).
“We initially conceived of this idea by looking at the household cleaner bleach. Even though it has been used since the 19th century, bacteria do not appear to have developed any widespread resistance to this cleaner,” says Rong Yang, PhD, the project’s principal investigator.
But Yang quickly warns that people should not treat infections with bleach. The solution sold at stores is highly concentrated and caustic, but when used in a properly controlled manner at extremely low concentrations, the active ingredient in bleach is considered compatible with living tissue.
After realising that the active ingredient in the household cleaner could circumvent antibiotic resistance, the Cornell University researchers, set out to tackle a nearly universal childhood scourge: acute ear infections. These infections affect more than 95% of children in the US, and treatment typically requires taking antibiotics for five to 10 days. However, these regimens can cause problematic side effects, leading some families to discontinue the medication prematurely, particularly if symptoms resolve. But using these medications improperly can speed up the development of antibiotic resistance, which makes infections more difficult, if not impossible, to treat. This issue ranks among the biggest threats to global health, according to the World Health Organization.
Bacteria have more success fighting against some substances than others. Hypochloric acid from bleach belongs to a family of compounds, known as hypohalous acids, to which bacteria have yet to develop any significant resistance; most likely because of the numerous ways these highly reactive acids damage microbial cells, Yang says.
Because these substances break down quickly, Yang and her colleagues sought to generate one of them on an as-needed basis behind the eardrum in the middle ear, where ear infections occur. They found inspiration in an enzyme from giant kelp, which converts hydrogen peroxide (H2O2) to hypobromous acid (HOBr), a chemical relative of bleach.
Streptococcus pneumoniae, a frequent cause of ear infections, produces H2O2 to fight off other microbes. To mimic the kelp enzyme, which contains the metal vanadium, Yang and her colleagues designed nanowires made of vanadium pentoxide (V2O5). These produce HOBr only in the presence of the H2O2-producing bacteria, and their rod-like shape helps to keep them in place by reducing their ability to diffuse into body fluids.
In tests on chinchillas, which contract ear infections from the same pathogens as human children, they succeeded in eliminating most of the S. pneumoniae. Yang and colleagues found that after treatment with the nanowires, the animals’ once-inflamed eardrums returned to normal. Meanwhile, tests in healthy animals found evidence that the treatment did not interfere with hearing.
For these experiments, the researchers injected the nanowires directly into the middle ear. In more recent work in chinchillas, they developed a less invasive, more practical method for delivering the wires. By decorating the nanowires with peptides known to transport small particles across the eardrum, Yang and her team found they could deliver the treatment topically as a gel deposited into the ear canal. Once the gel was applied, the nanowires within it went through the intact tissue. They are also exploring other approaches for passing the nanowires through the eardrum.
Because other ear-infection-causing bacteria do not produce H2O2, the researchers are currently examining whether this system is effective in the presence of microbes other than S. pneumoniae, and how they might adapt it to fight the other bugs.
The researchers have not yet done studies to determine how long the system stays in place, although their evidence suggests the nanowires drain out of the middle ear after the infection clears. However, Yang suspects they could adapt the nanowires’ properties to stay in place for long periods afterward. This latter approach could make it possible to prevent recurrent infections that plague many children.
“If the bacteria return, the system could restart, so children wouldn’t need antibiotics repeatedly and breed more resistance along the way,” Yang says.
A new study details the step-by-step cascade that allows bacteria to break through the brain’s protective layers, the meninges, and cause meningitis, a highly fatal disease. Published inNature, the mouse-based research shows that bacteria exploit nerve cells in the meninges to suppress the immune response and allow the infection to spread into the brain.
“We’ve identified a neuroimmune axis at the protective borders of the brain that is hijacked by bacteria to cause infection – a clever manoeuvre that ensures bacterial survival and leads to widespread disease,” said study senior author Isaac Chiu, associate professor of immunology in the Blavatnik Institute at Harvard Medical School.
The study identifies two central players in this molecular chain of events that leads to infection – a chemical released by nerve cells and an immune cell receptor blocked by the chemical. The study experiments show that blocking either one can interrupt the cascade and thwart the bacterial invasion.
If replicated through further research, the new findings could lead to much-needed therapies for this hard-to-treat condition that often leaves those who survive with serious neurologic damage.
Such treatments would target the critical early steps of infection before bacteria can spread deep into the brain.
“The meninges are the final tissue barrier before pathogens enter the brain, so we have to focus our treatment efforts on what happens at this border tissue,” said study first author Felipe Pinho-Ribeiro, a former post-doctoral researcher in the Chiu lab, now an assistant professor at Washington University in St. Louis.
A recalcitrant disease in need of new treatments
More than 1.2 million cases of bacterial meningitis occur globally each year, according to the US Centers for Disease Control and Prevention. Untreated, it kills seven out of 10 people who contract it. Treatment can reduce mortality to three in 10. However, among those who survive, one in five experience serious consequences, including hearing or vision loss, seizures, chronic headache, and other neurological problems.
The meninges are three membranes that lie atop one another, wrapping the brain and spinal cord to shield the central nervous system from injury, damage, and infection. The dura mater, outermost of the three layers, contains pain neurons that detect signals. Such signals could come in the form of mechanical pressure: blunt force from impact or toxins that make their way into the central nervous system through the bloodstream. The researchers focused on the dura mater as the site of initial interaction between bacteria and protective border tissue.
Recent research has revealed that the dura mater also harbours a wealth of immune cells, and that immune cells and nerve cells reside right next to each other – a clue that captured Chiu’s and Pinho-Ribeiro’s attention.
“When it comes to meningitis, most of the research so far has focused on analysing brain responses, but responses in the meninges – the barrier tissue where infection begins – have remained understudied,” Ribeiro said.
What exactly happens in the meninges when bacteria invade? How do they interact with the immune cells residing there? These questions remain poorly understood, the researchers said.
How bacteria break through the brain’s protective layers
In this particular study, the researchers focused on two pathogens – Streptococcus pneumoniae and Streptococcus agalactiae, leading causes of bacterial meningitis in humans. In a series of experiments, the team found that when bacteria reach the meninges, the pathogens trigger a chain of events that culminates in disseminated infection.
First, researchers found that bacteria release a toxin that activates pain neurons in the meninges. The activation of pain neurons by bacterial toxins, the researchers noted, could explain the severe, intense headache that is a hallmark of meningitis. Next, the activated neurons release a signalling chemical called CGRP. CGRP attaches to an immune-cell receptor called RAMP1. RAMP1 is particularly abundant on the surface of immune cells called macrophages.
Once the chemical engages the receptor, the immune cell is effectively disabled. Under normal conditions, as soon as macrophages detect the presence of bacteria, they spring into action to attack, destroy, and engulf them. Macrophages also send distress signals to other immune cells to provide a second line of defence. The team’s experiments showed that when CGRP gets released and attaches to the RAMP1 receptor on macrophages, it prevented these immune cells from recruiting help from fellow immune cells. As a result, the bacteria proliferated and caused widespread infection.
To confirm that the bacterially induced activation of pain neurons was the critical first step in disabling the brain’s defences, the researchers checked what would happen to infected mice lacking pain neurons.
Mice without pain neurons developed less severe brain infections when infected with two types of bacteria known to cause meningitis. The meninges of these mice, the experiments showed, had high levels of immune cells to combat the bacteria. By contrast, the meninges of mice with intact pain neurons showed meagre immune responses and far fewer activated immune cells, demonstrating that neurons get hijacked by bacteria to subvert immune protection.
To confirm that CGRP was, indeed, the activating signal, researchers compared the levels of CGRP in meningeal tissue from infected mice with intact pain neurons and meningeal tissue from mice lacking pain neurons. The brain cells of mice lacking pain neurons had barely detectable levels of CGRP and few signs of bacterial presence. By contrast, meningeal cells of infected mice with intact pain neurons showed markedly elevated levels of both CGRP and more bacteria.
In another experiment, the researchers used a chemical to block the RAMP1 receptor, preventing it from communicating with CGRP, the chemical released by activated pain neurons. The RAMP1 blocker worked both as preventive treatment before infection and as a treatment once infection had occurred.
Mice pretreated with RAMP1 blockers showed reduced bacterial presence in the meninges. Likewise, mice that received RAMP1 blockers several hours after infection and regularly thereafter had milder symptoms and were more capable of clearing bacteria, compared with untreated animals.
A path to new treatments
The experiments suggest drugs that block either CGRP or RAMP1 could allow immune cells to do their job properly and increase the brain’s border defenses.
Compounds that block CGRP and RAMP1 are found in widely used drugs to treat migraine, a condition believed to originate in the top meningeal layer, the dura mater. Could these compounds become the basis for new medicines to treat meningitis? It’s a question the researchers say merits further investigation.
One line of future research could examine whether CGRP and RAMP1 blockers could be used in conjunction with antibiotics to treat meningitis and augment protection.
“Anything we find that could impact treatment of meningitis during the earliest stages of infection before the disease escalates and spreads could be helpful either to decrease mortality or minimize the subsequent damage,” Pinho-Ribeiro said.
More broadly, the direct physical contact between immune cells and nerve cells in the meninges offers tantalizing new avenues for research.
“There has to be an evolutionary reason why macrophages and pain neurons reside so closely together,” Chiu said. “With our study, we’ve gleaned what happens in the setting of bacterial infection, but beyond that, how do they interact during viral infection, in the presence of tumour cells, or the setting of brain injury? These are all important and fascinating future questions.”
Streptococcus pyogenese bound to a human neutrophil.
Credit: National Institute of Allergy and Infectious Diseases, National Institutes of Health
Researchers at Lund University in Sweden have discovered an antibody that could potentially protect against Strep A infection, as well as a rare form of antibody binding, that leads to an effective immune response against bacteria. The discovery could explain why so many Group A strep vaccines have failed.
Group A streptococci have several ways in which they evade the body’s immune system and, when they infect us, can cause both common throat infections (strep throat), scarlet fever, sepsis, swine pox and skin infections. So far, antibiotics work against these bacteria, but should they become resistant, they will pose a major public health threat.
One strategy that the scientific community uses to find new ways of fighting bacterial infections is to create target-seeking antibodies. First, the antibodies that the body’s immune system produces in the event of an infection are mapped, and then their effect on the immune system is studied. In this way, antibodies can be identified that can be used both for preventive treatment and for treatment during an ongoing infection. It is a difficult process, though, with many attempts to develop antibody-based treatments against Strep A ending in failure.
The current study shows an unexpected way that antibodies interact with group A streptococci and, more specifically, how they hook onto the probably most important bacterial protein, the M protein, on the cell surface.
“We found that it happens in a way that has never been described before. Normally, an antibody binds via one of its two Y arms to its target protein at a single site, regardless of which of the two arms is used for binding. But what we have seen- and this is vital information – is that the two Y arms can recognise and hook on to two different places on the same target protein,” explains study author Pontus Nordenfelt.
This means that the two arms of the antibody – which are identical – can bind to two different sites on a target protein. It turns out that it is precisely this type of binding that is required for effective protection, and since it is probably rare, the researchers believe, it could explain why so many vaccine attempts have been unsuccessful. It could also be a reason why the bacteria manage to escape the immune system.
It has long been known that the streptococcal bacteria’s M protein is of great importance for how disease occurs and develops in the body. Finding an antibody that attaches to this protein, thereby flagging it up to the immune system, can prevent the bacteria from infecting the body’s cells. Since we know that the human body can fight the infection, such antibodies exist, but it is hard to locate them.
The researchers therefore focused on examining antibodies in patients who had recovered from group A streptococcal infection. They managed to identify three so-called monoclonal antibodies from a patient who recovered from a Strep A infection. Monoclonal antibodies are identical copies of each other, and in this case target a single protein (the M protein) of the group A streptococci. The researchers then investigated in animal studies whether it is possible to use the antibodies to strengthen the immune system in its fight against group A streptococcus. It turned out that the antibody with the newly discovered binding mechanism produced a strong immune response against the bacteria. The researchers have now applied for a patent based on the findings in the article, and will continue to study the antibody.
“This opens up possibilities where previous vaccine attempts have failed and means that the monoclonal antibody we used has the potential to protect against infection,” concludes study author Wael Bahnan.
A new study has found that children with chronic tic disorders, mainly Tourette syndrome, do not have tic exacerbations when exposed to group A Streptococcus.
No significant association with tic exacerbations emerged across four definitions of pharyngeal strep exposure with a mean follow-up of 16 months, though a weak link was observed in trend, reported Davide Martino, MD, PhD, of the University of Calgary, and co-authors.
Strep was however significantly associated with longitudinal changes in hyperactivity-impulsivity symptom severity of 17% to 21%. “The link between Streptococcus and tics in children is still a matter of intense debate,” Martino stated. “We wanted to look at that question, as well as a possible link between strep and behavioral symptoms like obsessive-compulsive disorder and attention deficit hyperactivity disorder.
“While our findings suggest that strep is not likely to be one of the main triggers for making tics worse, more research is needed into other possible explanations. For example, the social stress of having this disorder could be implicated in making tics worse more than infections. It’s also possible another pathogen might be triggering an immune response associated with tic worsening.”
In an invited editorial, Andrea Cavanna, MD, PhD, of the University of Birmingham, and Keith Coffman, MD, of Children’s Mercy Hospital in Kansas City, observed that group A Streptococcus had been posited as a potential environmental factor in tic disorders for the past two decades.
The editorialists noted that, on the basis of isolated clinical observations, tic disorders should be included as a collateral feature in conditions which are known as pediatric autoimmune neuropsychiatric disorders associated with Streptococcus (PANDAS) infections. However, the results of longitudinal clinical studies were inconclusive, with a case control study even arguing against the association.
Drawing data from the EMTICS study, recruiting children with chronic tic disorders from 2013 to 2016, one arm of the study prospectively examined associations between new group A Streptococcus throat exposures and tic exacerbations, obsessive-compulsive disorder (OCD), and attention deficit hyperactivity disorder (ADHD) symptoms.
Four definitions of strep exposure were used: new definite (newly positive throat swab regardless of serological results), new possible (elevated anti-streptolysin O [ASOT] or anti-DNAseB [ADB] titers with negative or no throat swab), ongoing definite, and ongoing possible.
Initially, 59 children had a positive throat swab; as the study progressed, 103 children had new definite strep exposure. During follow-up, 308 children (43%) had tic exacerbations. The proportion of exacerbations temporally associated with strep exposure ranged from 5.5% to 12.9%, depending on exposure definition. No association between OCD symptoms and strep exposure was seen.
“Our study of the largest prospective cohort of youth with chronic tic disorders ever documented to date provides evidence against a temporal association between group A Streptococcus exposure and clinically relevant tic exacerbations,” the researchers wrote.
“This result indicates that specific diagnostic work-up or active management of group A Streptococcus infections in the context of worsening of tic severity in patients with chronic tic disorders is not warranted,” the researchers added.
The researchers noted that limitations included the data being collected from specialist centres in different countries, and that some cases of strep may have been missed.
Journal information (article): Martino D, et al “Association of Group A Streptococcus Exposure and Exacerbations of Chronic Tic Disorders: A Multinational Prospective Cohort Study” Neurology 2021; DOI: 10.1212/WNL.0000000000011610.
Journal information (editorial): Cavanna A, Coffman K “Streptococcus and Tics: Another Brick in the Wall?” Neurology 2021. DOI: 10.1212/WNL.0000000000011608.