Researchers at Karolinska Institutet and KTH Royal Institute of Technology have developed an improved method for creating insulin-producing cells from human stem cells. The results, published in Stem Cell Reports, demonstrate that these cells effectively regulate blood sugar levels in laboratory tests and can reverse diabetes in mice.
Type 1 diabetes occurs when the immune system destroys insulin-producing cells in the pancreas, meaning the body can no longer absorb glucose from the blood and regulate blood sugar levels. One possible treatment is to replace these cells with new ones. However, previous methods of producing such cells from stem cells have often yielded mixed results.
“We have developed a method that reliably produces high-quality insulin-producing cells from multiple human stem cell lines. This opens up opportunities for future patient-specific cell therapies, which could reduce immune rejection,” says Per-Olof Berggren, professor at the Department of Molecular Medicine and Surgery, Karolinska Institutet, and corresponding author alongside Siqin Wu, researcher at Spiber Technologies AB (formerly at Karolinska Institutet).
Optimised cell production
The optimised production process yields more mature and purer insulin-producing cells than previous methods. In a laboratory setting, the cells were able to secrete insulin and responded strongly to glucose. When the researchers transplanted these cells into diabetic mice, the animals gradually regained the ability to regulate their blood sugar. The transplantation was performed in the anterior chamber of the eye.
“This is a technique we use to monitor the development and function of the cells over time in a minimally invasive way,” explains Per-Olof Berggren. “We observed that the cells gradually matured after transplantation, retaining their ability to regulate blood sugar for several months, which demonstrates their potential for future treatments.”
Stem cell therapy for type 1 diabetes is already being tested in several clinical trials. However, a challenge with previous methods is that the stem cells often develop into a combination of the desired and undesired cell types, increasing the risk of complications. Another challenge is that the insulin-producing cells created are often not mature enough to respond well to glucose.
Solving previous problems
By adjusting the culture steps and allowing the cells to form three-dimensional clusters themselves, many unwanted cell types are eliminated and the cells gain a better ability to respond to glucose, according to the researchers.
“This could solve several of the problems that have previously hindered the development of stem cell-based treatments for type 1 diabetes. Building on this, we will work towards clinical translation aiming at treating type 1 diabetes,” says Fredrik Lanner, professor at the Department of Clinical Science, Intervention and Technology, Karolinska Institutet, and last author of the paper.
From genetics to stress myths, researchers reveal what really drives greying and the breakthroughs pointing to natural colour restoration
Photo by Ravi Patel on Unsplash
Grey hair is more than a cosmetic concern – it drives a booming industry, influences how people are perceived, and can affect confidence. Globally, the hair colour market was valued at nearly USD 28 billion in 2025, with over half of purchases linked specifically to concealing greys. In South Africa, spending on hair colourants is projected to grow from roughly USD 172 million in 2021 to over USD 228 million by 2028, highlighting the demand for solutions that go beyond temporary cover-ups.
By age 50, roughly 50-70% of adults have visible grey hair, while premature greying can appear in some as early as the 20s. The psychological weight is clear: studies indicate grey hair can make people appear 20-30% older, influencing workplace perception, social interactions, and self-esteem. Studies show faces with grey hair are consistently perceived as more subdued than the same faces without greys, confirming that hair colour alone can shape social impressions.
“Many popular beliefs about greying hair are misleading,” says Dr Kashmal Kalan, Medical Director at Alvi Armani. “Stress does not turn hair grey overnight, plucking one strand won’t trigger several more, and no supplement or home remedy has been proven to restore pigment reliably. The reality is far more biological – genetics and pigment cell behaviour are the keys we are finally beginning to understand.”
At the heart of greying are melanocyte stem cells (McSCs) within hair follicles. In youth, these cells migrate and maintain melanin production, the pigment responsible for hair colour. With age, many become inactive or “trapped,” interrupting pigment delivery and causing grey strands. In mouse models, freeing these cells restored pigment production in roughly half of cases – a major step toward therapies that could reawaken natural colour without dyes.
Emerging research aims to tackle the root cause rather than just the appearance of grey hair. Scientists are exploring topical agents that target dormant pigment cells, metabolic modulators that influence follicle behaviour, and activation therapies designed to revive pigment production. These innovations could allow hair to regain its natural shade – not just cover it – while supporting overall follicle health.
“We are witnessing science that was once purely theoretical become reality,” says Dr Sunaina Paima, aesthetic and hair-restoration physician at Alvi Armani Johannesburg. “For patients, this could mean seeing grey strands regain their original shade naturally – a moment the hair science world has long dreamed of. The potential impact on confidence and self-esteem is enormous, because this isn’t just about covering colour, it’s about restoring it at a biological level.”
While most pigment-restoring therapies remain in development, advances in genetics, dermatology, and biotechnology are converging at unprecedented speed. “For decades, grey hair was seen as an irreversible hallmark of ageing,” adds Dr Kalan. “Today, that assumption is being seriously challenged. We’re on the brink of options that rejuvenate hair from the inside out, not just cosmetically.”
These breakthroughs signal a new era in hair science: ageing hair may no longer be inevitable or purely cosmetic, but a biological process that can be understood, guided, and ultimately restored.
New method for the targeted production of specific cells
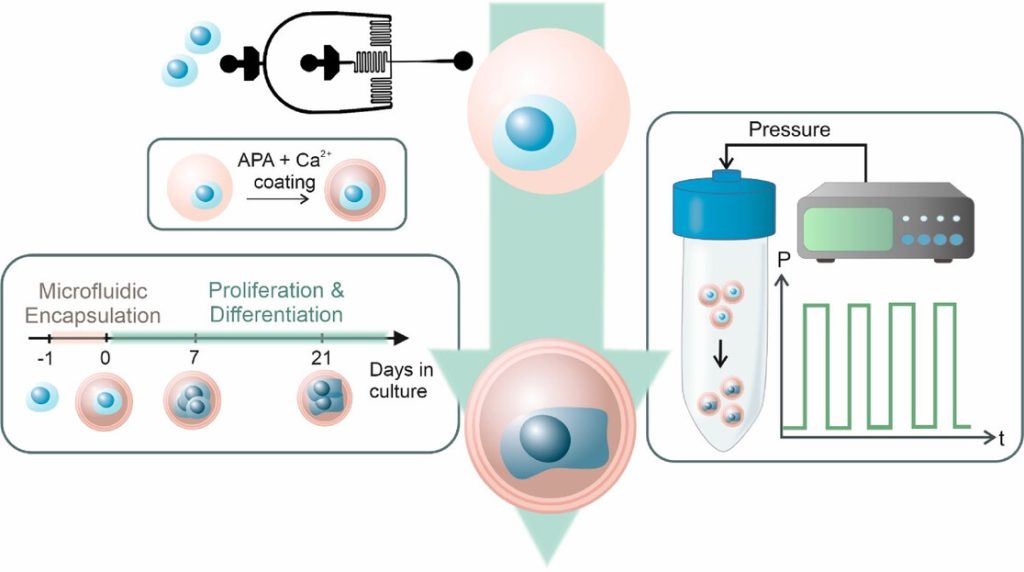
Figure 1 Schematic overview of the experimental workflow. MSCs (blue) were singly encapsulated using a microfluidic approach within calcium-crosslinked, RGD-functionalized alginate microgels (pink), followed by a secondary APA and calcium coating to enhance stability. Encapsulated cells were cultured for 21 days and subjected to cyclic hydrostatic pressure in regular cell culture media without any growth factors. Source: İyisan et al., Small Science, 2025.
For the first time, researchers at the Technical University of Munich (TUM) have succeeded in using nanorobots to stimulate stem cells with such precision that they are reliably transformed into bone cells. To achieve this, the robots exert external pressure on specific points in the cell wall. The new method offers opportunities for faster treatments in the future.
Prof Berna Özkale Edelmann’s nanorobots consist of tiny gold rods and plastic chains. Several million of them are contained in a gel cushion measuring just 60 micrometres, together with a few human stem cells. Powered and controlled by laser light, the robots, which look like tiny balls, mechanically stimulate the cells by exerting pressure. “We heat the gel locally and use our system to precisely determine the forces with which the nanorobots press on the cell – thereby stimulating it,” explains the professor of nano- and microrobotics at TUM. This mechanical stimulation triggers biochemical processes in the cell. Ion channels change their properties, and proteins are activated, including one that is particularly important for bone formation.
Heart and cartilage cells: finding the correct stress pattern
If stimulation is carried out at the right rhythm and with the right (low) force, a stem cell can be reliably triggered to develop into a bone cell within three days. This process can be completed within three weeks. “The corresponding stress pattern can also be found for cartilage and heart cells,” asserts Berna Özkale Edelman. “It’s almost like at the gym: we train the cells for a particular area of application. Now we just have to find out which stress pattern suits each cell type,” says the head of the Microbiotic Bioengineering Lab at TUM.
Mechanical forces pave the way for transformation into bone cells
The research team produces bone cells using mesenchymal stem cells. These cells are considered to be the body’s ‘repair cells’. They are approximately 10 to 20 micrometres in size and are generally capable of developing into bone, cartilage or muscle cells, for example. The challenge: The transformation into differentiated cells is complex and has been difficult to control until now. “We have developed a technology that allows forces to be applied to the cell very precisely in a three-dimensional environment,” says TUM scientist Özkale Edelmann. “This represents an unprecedented advance in the field.” The researchers believe that this method can even be used to produce cartilage and heart cells from human stem cells.
Automation is the next step
For treatments, doctors will ultimately need far more differentiated cells – around one million. “That’s why the next step is to automate our production process so that we can produce more cells more quickly,” says Prof Özkale Edelmann.
Technique may be a valuable add-on procedure for patients with weak heart function after a heart attack, say researchers
Right side heart failure. Credit: Scientific Animations CC4.0
Patients with weak heart function who receive stem cell therapy shortly after a heart attack are at lower risk of developing heart failure and related hospital stays compared with standard care, finds a clinical trial published by The BMJ.
The researchers say the findings suggest this technique may be a valuable add-on procedure for this particular group of patients after a heart attack to prevent subsequent heart failure and reduce the risk of future adverse events.
Advances in heart attack management have improved survival rates considerably, but this has also led to rising rates of subsequent heart failure. While recent studies have indicated that stem cell therapy may reduce rates of heart failure after a heart attack, clinical trials are needed to confirm these benefits.
To address this gap, the researchers set out to assess the impact of delivering stem cells directly into coronary arteries (known as intracoronary infusion) after a heart attack on the development of heart failure over three years.
Their findings are based on 396 patients (average age 57-59 years) with no previous heart conditions at three teaching hospitals in Iran. They had all experienced a first heart attack (myocardial infarction) leading to extensive heart muscle damage and weakened heart function – where the left ventricle, the heart’s main pumping chamber, is too weak to pump blood out to the body as effectively as it should.
Of these, 136 patients in the intervention group received an intracoronary infusion of allogenic Wharton’s jelly derived mesenchymal stem cells within 3-7 days of their heart attack in addition to standard care. The remaining 260 control group patients received standard care alone.
Factors such as age, sex, baseline heart function, smoking status, obesity, existing high blood pressure, diabetes, or kidney problems were taken into account, and patients were monitored for an average of 33 months.
Compared with the control group, intracoronary infusion of stem cells was associated with reduced rates of heart failure (2.77 vs 6.48 per 100 person years), readmission to hospital for heart failure (0.92 vs 4.20 per 100 person years), and a combined measure of cardiovascular death and readmission for heart attack or heart failure (2.8 vs 7.16 per 100 person years).
The intervention did not have a statistically significant effect on readmission to hospital for heart attack (1.23 vs 3.06 per 100 person years), death from any cause (1.81 vs 1.66 per 100 person years), or cardiovascular death (0.91 vs 1.33 per 100 person-years).
However, by six months heart function in the intervention group showed a significantly greater improvement from baseline at six months compared with the control group.
This was a large trial with long term follow-up and clinically meaningful outcome measures, but the researchers acknowledge several limitations to their findings. These include the inability to do a sham procedure for the control group, which would have allowed for a double blinded study design instead of a single blinded format. Nor did they assess heart failure biomarkers or investigate the physiological effects of the intervention on heart tissue.
Nevertheless, they say these results suggest that this technique “may serve as a valuable adjunctive procedure after myocardial infarction to prevent the development of heart failure and reduce the risk of future adverse events.”
Additional trials confirming this finding are needed as well as further research “to explore the underlying mechanisms of mesenchymal stem cells therapy and to optimise its application in clinical practice,” they add.
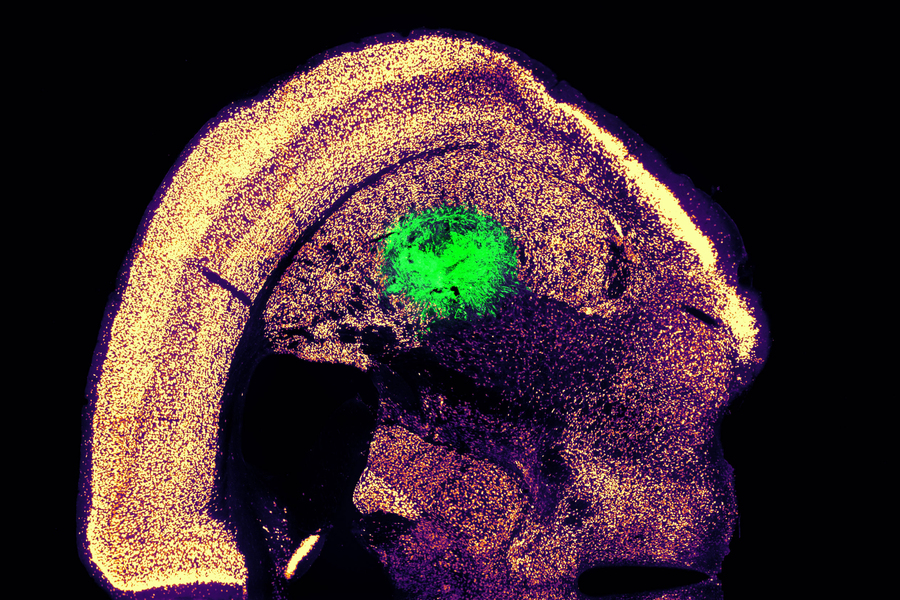
This image shows a coronal section through the mouse brain after stroke and neural stem cell transplantation. The dashed circle indicates the stroke area. The neurite projections of the transplanted human cells are stained in dark brown. Neurites extend locally into the cortex (CX) but also via the corpus callosum (CC) into the other brain hemisphere. (Image: UZH)
One in four adults suffer a stroke in their lifetime, leaving around half of them with residual damage such as paralysis or speech impairment because internal bleeding or a lack of oxygen supply kill brain cells irreversibly. No therapies currently exist to repair this kind of damage. “That’s why it is essential to pursue new therapeutic approaches to potential brain regeneration after diseases or accidents,” says Christian Tackenberg, the Scientific Head of Division in the Neurodegeneration Group at the University of Zurich (UZH) Institute for Regenerative Medicine.
Neural stem cells have the potential to regenerate brain tissue, as a team led by Tackenberg and postdoctoral researcher Rebecca Weber has now compellingly shown in two studies that were conducted in collaboration with a group headed by Ruslan Rust from the University of Southern California. “Our findings show that neural stem cells not only form new neurons, but also induce other regeneration processes,” Tackenberg says.
The studies employed human neural stem cells, from which different cell types of the nervous system can form. The stem cells were derived from induced pluripotent stem cells, which in turn can be manufactured from normal human somatic cells. For their investigation, the researchers induced a permanent stroke in mice, the characteristics of which closely resemble manifestation of stroke in humans. The animals were genetically modified so that they would not reject the human stem cells.
One week after stroke induction, the research team transplanted neural stem cells into the injured brain region and observed subsequent developments using a variety of imaging and biochemical methods. “We found that the stem cells survived for the full analysis period of five weeks and that most of them transformed into neurons, which actually even communicated with the already existing brain cells,” Tackenberg says.
Brain regenerates itself
The researchers also found other markers of regeneration: new formation of blood vessels, an attenuation of inflammatory response processes and improved blood-brain barrier integrity. “Our analysis goes far beyond the scope of other studies, which focused on the immediate effects right after transplantation,” Tackenberg explains. Fortunately, stem cell transplantation in mice also reversed motor impairments caused by stroke. Proof of that was delivered in part by an AI-assisted mouse gait analysis.
Clinical application moving closer to reality
Human neural stem cells in culture. Cell nuclei are stained in blue, the neural stem cell-specific filament protein Nestin is shown in green, and the neural stem cell transcription factor Sox1 in red. (Image: UZH)
When he was designing the studies, Tackenberg already had his sights set on clinical applications in humans. That’s why, for example, the stem cells were manufactured without the use of reagents derived from animals. The Zurich-based research team developed a defined protocol for that purpose in collaboration with the Center for iPS Cell Research and Application (CiRA) at Kyoto University. This is important for potential therapeutic applications in humans. Another new insight discovered was that stem cell transplantation works better when it is performed not immediately after a stroke but a week later, as the second study verified. In the clinical setting, that time window could greatly facilitate therapy preparation and implementation.
Despite the encouraging results of the studies, Tackenberg warns that there is still work to be done. “We need to minimize risks and simplify a potential application in humans,” he says. Tackenberg’s group, again in collaboration with Ruslan Rust, is currently working on a kind of safety switch system that prevents uncontrolled growth of stem cells in the brain. Delivery of stem cells through endovascular injection, which would be much more practicable than a brain graft, is also under development. Initial clinical trials using induced stem cells to treat Parkinson’s disease in humans are already underway in Japan, Tackenberg reports. “Stroke could be one of the next diseases for which a clinical trial becomes possible.”
A new, highly efficient process for performing this conversion could make it easier to develop therapies for spinal cord injuries or diseases like ALS.
Anne Trafton | MIT News
Researchers at MIT have devised a simplified process to convert a skin cell directly into a neuron. This image shows converted neurons (green) that have integrated with neurons in the brain’s striatum after implantation.
Credits :Image: Courtesy of the researchers
Converting one type of cell to another – for example, a skin cell to a neuron – can be done through a process that requires the skin cell to be induced into a “pluripotent” stem cell, then differentiated into a neuron. Researchers at MIT have now devised a simplified process that bypasses the stem cell stage, converting a skin cell directly into a neuron.
Working with mouse cells, the researchers developed a conversion method that is highly efficient and can produce more than 10 neurons from a single skin cell. If replicated in human cells, this approach could enable the generation of large quantities of motor neurons, which could potentially be used to treat patients with spinal cord injuries or diseases that impair mobility.
“We were able to get to yields where we could ask questions about whether these cells can be viable candidates for the cell replacement therapies, which we hope they could be. That’s where these types of reprogramming technologies can take us,” says Katie Galloway, the W. M. Keck Career Development Professor in Biomedical Engineering and Chemical Engineering.
As a first step toward developing these cells as a therapy, the researchers showed that they could generate motor neurons and engraft them into the brains of mice, where they integrated with host tissue.
Galloway is the senior author of two papers describing the new method, which appear today in Cell Systems. MIT graduate student Nathan Wang is the lead author of both papers.
From skin to neurons
Nearly 20 years ago, scientists in Japan showed that by delivering four transcription factors to skin cells, they could coax them to become induced pluripotent stem cells (iPSCs). Similar to embryonic stem cells, iPSCs can be differentiated into many other cell types. This technique works well, but it takes several weeks, and many of the cells don’t end up fully transitioning to mature cell types.
“Oftentimes, one of the challenges in reprogramming is that cells can get stuck in intermediate states,” Galloway says. “So, we’re using direct conversion, where instead of going through an iPSC intermediate, we’re going directly from a somatic cell to a motor neuron.”
Galloway’s research group and others have demonstrated this type of direct conversion before, but with very low yields – fewer than 1 percent. In Galloway’s previous work, she used a combination of six transcription factors plus two other proteins that stimulate cell proliferation. Each of those eight genes was delivered using a separate viral vector, making it difficult to ensure that each was expressed at the correct level in each cell.
In the first of the new Cell Systems papers, Galloway and her students reported a way to streamline the process so that skin cells can be converted to motor neurons using just three transcription factors, plus the two genes that drive cells into a highly proliferative state.
Using mouse cells, the researchers started with the original six transcription factors and experimented with dropping them out, one at a time, until they reached a combination of three – NGN2, ISL1, and LHX3 — that could successfully complete the conversion to neurons.
Once the number of genes was down to three, the researchers could use a single modified virus to deliver all three of them, allowing them to ensure that each cell expresses each gene at the correct levels.
Using a separate virus, the researchers also delivered genes encoding p53DD and a mutated version of HRAS. These genes drive the skin cells to divide many times before they start converting to neurons, allowing for a much higher yield of neurons, about 1100 percent.
“If you were to express the transcription factors at really high levels in nonproliferative cells, the reprogramming rates would be really low, but hyperproliferative cells are more receptive. It’s like they’ve been potentiated for conversion, and then they become much more receptive to the levels of the transcription factors,” Galloway says.
The researchers also developed a slightly different combination of transcription factors that allowed them to perform the same direct conversion using human cells, but with a lower efficiency rate – between 10 and 30 percent, the researchers estimate. This process takes about five weeks, which is slightly faster than converting the cells to iPSCs first and then turning them into neurons.
Implanting cells
Once the researchers identified the optimal combination of genes to deliver, they began working on the best ways to deliver them, which was the focus of the second Cell Systems paper.
They tried out three different delivery viruses and found that a retrovirus achieved the most efficient rate of conversion. Reducing the density of cells grown in the dish also helped to improve the overall yield of motor neurons. This optimised process, which takes about two weeks in mouse cells, achieved a yield of more than 1000 percent.
Working with colleagues at Boston University, the researchers then tested whether these motor neurons could be successfully engrafted into mice. They delivered the cells to a part of the brain known as the striatum, which is involved in motor control and other functions.
After two weeks, the researchers found that many of the neurons had survived and seemed to be forming connections with other brain cells. When grown in a dish, these cells showed measurable electrical activity and calcium signaling, suggesting the ability to communicate with other neurons. The researchers now hope to explore the possibility of implanting these neurons into the spinal cord.
The MIT team also hopes to increase the efficiency of this process for human cell conversion, which could allow for the generation of large quantities of neurons that could be used to treat spinal cord injuries or diseases that affect motor control, such as ALS. Clinical trials using neurons derived from iPSCs to treat ALS are now underway, but expanding the number of cells available for such treatments could make it easier to test and develop them for more widespread use in humans, Galloway says.
The research was funded by the National Institute of General Medical Sciences and the National Science Foundation Graduate Research Fellowship Program.
Dr Yvonne Holt, Chief Medical Officer of Next Biosciences (left) with Kim Hulett, Founder and CEO of the company (right) celebrating 20 years of innovation and leadership in stem cell banking, genetic testing and regenerative medicine.
As Next Biosciences celebrates its 20th anniversary, the pioneering South African biotech company reflects on two decades of significant advancements in science and healthcare.
From its roots in medical innovation to its transformative contributions in regenerative medicine, genetic testing and wellness, Next Biosciences has not only shaped the local industry, but also positioned itself as a leader in Africa’s growing biotech sector.
Founded by Kim Hulett, an entrepreneur with a background in finance and technology, and Dr Yvonne Holt, the company has expanded its range of products and services that cover biologics, stem cells, exosomes, genetic testing, longevity and reproductive health.
“The journey of Next Biosciences has been about bringing cutting-edge science and technology to South Africa, and making advancements in health and wellness accessible,” says Dr Holt, Chief Medical Officer at the company. “Every innovation we develop is driven by our mission to positively impact people’s health with science, by transforming lives, improving health outcomes and shaping the future of medicine on the continent.”
With a team of 90, Next Biosciences stands as one of the country’s leading biotech innovators. Women make up 80% of the workforce, with 20% of them being scientists – underscoring the company’s strong commitment to diversity and inclusion. Their lab is accredited by the Association for the Advancement of Blood and Biotherapies (AABB) and ISO 13485 standards, a testament to their excellence in stem cell banking, cord blood services and other biotechnological advancements.
From its beginnings with Netcare, Next Biosciences’ focus on research and development has enabled the company to expand beyond local borders, bringing its innovative healthcare solutions to a wider audience. They now lead initiatives that support regenerative medicine with products like OptiSerum, a revolutionary umbilical cord blood serum for ophthalmic use, and AmnioMatrix, used in a range of medical applications from ophthalmology and wound care to dentistry.
Next Biosciences’ state-of-the-art Netcells storage lab, ensuring the safe preservation of precious stem cells for future medical advancements.
“Biotechnology and regenerative medicine are advancing at an unprecedented pace, offering new possibilities for treating diseases that were once thought incurable. Our focus remains on harnessing these innovations responsibly, ensuring that the latest advancements in cellular therapies, genetic diagnostics and biologics translate into real, life-changing solutions for patients,” says Dr Holt.
The biotechnology landscape has evolved worldwide, and South Africa has not been left behind.
Credit: Global Biotech Indus
The global biotechnology industry is currently valued at $546 billion, growing at approximately 13% per annum. Remarkable advancements have been achieved in genetic research, stem cell therapies and personalised medicine. “The potential for biotechnology over the next decade is extraordinary,” says Hulett, CEO of Next Biosciences. Breakthroughs in regenerative medicine and longevity science are revolutionising healthcare as we know it.”
Next Biosciences’ path hasn’t been without challenges. From navigating regulatory hurdles to sourcing cutting-edge technologies, the company’s growth has been driven by passion, resilience and innovation. As a majority female-led team, the company exemplifies the power of women in science and business, and they have become a beacon for female entrepreneurs looking to make a mark in the science and technology sectors.
“Building a biotech company in SA, with all its complexities, required tenacity and a relentless commitment to our mission. Over the years, we have witnessed our industry evolve and we are proud to have been at the forefront of that change,” says Hulett. “The future holds great promise and we are excited to see what the next 20 years will bring.”
Looking ahead, Next Biosciences aims to expand its footprint in Africa, focusing on reproductive, regenerative and longevity health to empower individuals to invest in their health and live their best lives. With a strong commitment to innovation, accessibility, convenience and sustainability, Next Biosciences plans to integrate cutting-edge biotechnologies, while maintaining a patient-centric approach. By staying at the forefront of the biotech industry, the company is set to strengthen its position as a trusted leader in African healthcare.
Right side heart failure. Credit: Scientific Animations CC4.0
Pathways to new treatments for heart failure take time – as long as four decades for two now accepted therapies. So, new attempts to repair scar tissue in infarcted hearts using cells or cell products need more time to develop clinical therapies that can reduce risk of death from heart failure after a heart attack.
This message is part of a critical review of cell-based and cell product-based therapies for the treatment of heart failure. The review details 20 years of completed and ongoing clinical trials. While none has gained medical approval, they have proven safe and some have shown beneficial effects.
More importantly, the reviewers note, it took longer, nearly 40 years, to optimise two current therapies to reduce mortality in heart failure: implantable cardioverter–defibrillators and guideline-directed medical therapy.
“The history of the development of life-saving medical therapies for heart failure serves as an important lesson that we should remain hopeful of the promise of cell therapy in heart failure,” Jianyi “Jay” Zhang, MD, PhD, and colleagues write in the review, “Trials and tribulations of cell therapy for heart failure: an update on ongoing trials,” published in Nature Reviews Cardiology. Zhang is professor and chair of the University of Alabama at BirminghamDepartment of Biomedical Engineering.
Heart failure is responsible for 13% of deaths worldwide. Half of patients with heart failure die within five years. The most common cause of heart failure is blockage of coronary arteries leading to death of the cardiomyocyte heart muscle cells. When that muscle tissue is replaced by dense scar tissue with little blood circulation, the infarcted heart loses contractile power, leading to heart enlargement, progressive loss of pumping ability, increased chance of ventricular arrhythmias and clinical end-stage heart failure.
The problem is that shortly after birth, human heart muscle cells lose their ability to divide, so a damaged infarcted heart cannot repair itself by growing new muscle cells. Thus, the simple idea behind initial cell therapies was to add or inject replacement cells to the scar area to restore muscle tissue.
The two decades since has been a long road, with bumps and turns. The three parts of the Nature Reviews Cardiology paper describe the journey.
First is a history of the slow development, obstacles, setbacks and scepticism for two current heart failure therapies, implantable cardioverter–defibrillators and guideline-directed medical therapy. The next two sections, and main focus of the review, survey 13 completed clinical trials published in the last 12 years and 10 very recently initiated and ongoing clinical trials that are based on the lessons learned from the past 20 years of research, to assess the safety and efficacy of cell- and cell products-based therapy approaches.
While several randomised, double-blind, multicentre phase II or III trials published in the past 20 years support the concept that even a single dose of cell products has beneficial effects in patients with heart failure on optimal medical therapy, the ongoing trial are taking novel directions, Zhang says.
These include:
New cell types — pluripotent stem cell-derived cardiomyocytes/ spheroids and umbilical cord-derived mesenchymal stem cells
Repeated intravenous injections as a noninvasive cell delivery method
New cell products, such as engineered epicardial cardiomyocyte patches
Novel cell-free products — extracellular vesicle-enriched or exosome-enriched secretomes.
“The results of these trials will continue to define and refine our understanding of cell and cell product therapy as a novel addition in the treatment of patients with heart failure,” Zhang said.
The review acknowledges scientific criticism during the slow but consistent progress and evolution of cell therapy. Some have questioned the use of public funding to support cell therapy research for heart failure treatment, due to poorly designed or underpowered clinical trials and very modest improvements in cardiac function in preclinical studies that are not always substantiated in large-scale clinical trials.
“These criticisms must be addressed in future trials that are adequately powered and rigorously designed to ensure continued progress of the field,” Zhang said. “Critique is an essential part of science, and the basis for growth, innovation and evolution – this is no less true for the field of cell therapy.”
Yet Zhang is confident that current research will yield clinical translation. “In the past 20 years, cell therapy has emerged and evolved as a promising avenue for cardiac repair and regeneration,” he said. “Cell therapy has encountered substantial barriers in both preclinical studies and clinical trials, but the field continues to progress and evolve through lessons learned from such research.”
A novel drug holds promise for treating Duchenne muscular dystrophy (DMD), a rare genetic disorder that causes severe muscle degeneration.
McGill University researchers have discovered that an experimental compound called K884 can boost the natural repair abilities of muscle stem cells. Current treatments can slow muscle damage, but don’t address the root problem.
DMD affects about one in 5000 boys worldwide, often leading to wheelchair dependence by the teenage years and life-threatening complications in early adulthood.
“By strengthening muscle repair rather than just slowing degeneration, therapies that stimulate muscle stem cell function have the potential to improve quality of life for DMD patients. It may help restore muscle function and, ultimately, offer greater independence,” said senior author Natasha Chang, Assistant Professor in McGill’s Department of Biochemistry.
Building stronger muscles from stem cells
Biotechnology company Kanyr Pharma originally developed the drug for cancer and metabolic diseases, but it has not yet been approved for any specific use. This preclinical study marks the first time the drug has been tested in DMD cells.
The researchers put DMD-affected muscle stem cells from humans and mice under the microscope to see how they responded to the drug. They observed that experimental drug blocks specific enzymes, allowing muscle stem cells to develop into functional muscle tissue.
“What makes K884 particularly promising is its precision. It targets DMD-affected cells without affecting healthy muscle stem cells,” said Chang.
Unlike gene therapy, which targets specific genetic mutations and isn’t suitable for all patients, K884 works at the cellular level, restoring muscle repair regardless of the mutation causing the disease. This makes it a potential treatment option for all DMD patients, she added.
A new understanding of DMD
The findings, published in Life Science Alliance, add to a growing body of evidence that challenges previous assumptions about DMD’s root cause.
“This disease has historically been seen as a muscle problem caused by a missing protein called dystrophin,” said Chang. “But new research, including our own, shows that restoring stem cell function is just as critical for repairing muscle.”
The team plans to keep testing the drug, focusing on its safety and long-term effects, while also exploring other related compounds, some of which are already involved in early human trials.
Photo by Towfiqu barbhuiya: https://www.pexels.com/photo/person-feeling-pain-in-the-knee-11349880/
Cell therapy has been explored as a new regenerative treatment for osteoarthritis, but the efficacy of stem cell transplantation from different sources for the treatment of knee osteoarthritis (KOA) remains controversial. A recent analysis of all relevant published studies indicates that stem cell transplantation from different sources is effective for treating knee osteoarthritis, the most prevalent chronic joint disease.
The review and meta-analysis, which is published in the Journal of Orthopaedic Research, included 16 studies involving 875 patients with knee osteoarthritis (441 in the stem cell transplantation group and 434 in the control group). Stem cell treatment was associated with significant reductions in patient-reported pain from the third month onwards. The most significant pain relief at different postoperative months came from fat-derived and umbilical cord–derived stem cells. A patient’s own fat-derived stem cells resulted in better pain alleviation compared with those from other donors. Also, a patient’s own fat-derived stem cells led to the most effective recovery of knee joint function.
“Stem cell transplantation proved safe and effective for knee osteoarthritis treatment,” the authors wrote. “Different sources stem cells have a good effect on alleviating knee joint pain, restoring knee joint function, and minimising patient trauma.”