With only 22 090 nurses to serve the country’s public health sector of more than 50 million citizens1, urgent intervention is required to bolster their numbers and protect the wellbeing of our nation. After all, without their tireless dedication, who will be there to guide you through the corridors back to health? writes Bada Pharasi, CEO of the Innovative Pharmaceutical Association of South Africa (IPASA)
As the global healthcare industry commemorates International Nurses Day on 12 May, it is an opportune moment to reflect on the role of nurses as the heartbeat of healthcare systems globally. Amid turmoil and triumph, nurses stand as the unsung heroes and compassionate caretakers who embody empathy, endurance and expertise.
In South Africa, where healthcare challenges often loom large and resources are stretched thin, nurses serve as the frontline warriors, bridging the gap between suffering and healing. Yet, despite the invaluable role they play, a concerning trend looms.
Minister of Health, Joe Phaahla, recently revealed a pressing concern – the anticipation of a staggering 30% of South African nurses retiring within the next decade, and 38% retiring the decade thereafter. Compounding the issue, 5060 vacancies remain unfilled on the back of crippling budget constraints1.
Representing over 90% of global healthcare workers2, nurses are indispensable in the healthcare ecosystem, and addressing this impending crisis of their reducing numbers demands comprehensive and multifaceted solutions that approach the challenge from every angle.
The nurse shortage crisis in South Africa stems from multiple factors. Firstly, the escalating healthcare needs of a growing population, compounded by the burden of infectious diseases such as HIV/AIDS, have strained the healthcare system to breaking point.
Another factor is the restricted capacity of the private sector to train nurses comprehensively due to existing regulations. Moreover, poor working conditions, particularly in the public sector, and comparatively low salaries have led to high turnover rates, prompting nurses to explore alternative career paths or seek employment opportunities abroad3.
While there are many challenges to defusing the proverbial ticking time bomb which is the declining number of qualified nurses in South Africa, increased investment across the board is critical to strengthening their ranks.
Despite financial investment being central in realising this, addressing the problem demands a focus on improving the working conditions of nurses. Healthcare facilities must prioritise nurses’ well-being by offering competitive salaries, manageable workloads, and opportunities for career growth. By creating a supportive work environment, South Africa can retain more nurses and deter them from seeking opportunities abroad3.
Furthermore, granting private hospitals full participation in nurse training programmes is crucial. Private sector entities, such as Netcare, have the capacity to train as many as 3,500 nurses annually. However, limited accreditation from the government hampers their potential contribution to resolving the nurse shortage. Expanding private sector involvement in nurse training could substantially increase the number of trained nurses in the country3.
In addition to these measures, collaborative efforts between the government, healthcare institutions, and nursing organisations are essential. Such partnerships can identify and implement strategies to alleviate the shortage, including targeted recruitment drives, mentorship programmes, and initiatives to improve nurses’ job satisfaction and work-life balance3.
Innovative approaches to addressing the nurse shortage in South Africa extend beyond traditional solutions. Telemedicine platforms are emerging as a promising tool, allowing nurses to deliver care remotely and reach patients in underserved areas.
Additionally, community health worker programmes are being expanded to complement nursing services and extend healthcare access to marginalised communities. Furthermore, initiatives to empower and support nurse entrepreneurs are gaining traction, encouraging the development of innovative care models and healthcare solutions.
These diverse approaches reflect a multifaceted response to the nurse shortage crisis, leveraging technology, community engagement, and entrepreneurship to strengthen the healthcare workforce and improve access to care for all South Africans.
Creative artwork featuring colourised 3D prints of influenza virus (surface glycoprotein hemagglutinin is blue and neuraminidase is orange; the viral membrane is a darker orange). Note: Not to scale. Credit: NIAID
By Elri Voigt for Spotlight
COVID-19-related factors resulted in several years of lower-than-normal rates of the flu, but experts say that is now something of the past. As this year’s flu season gets under way, Elri Voigt asks several local experts what their expectations are, which flu vaccines are available this year, and whether we should be concerned about new strains of bird flu.
While most people who get the flu experience only mild to moderate symptoms, some can get severe symptoms and even die, especially the very young and the old. As Spotlight previously reported, the influenza virus causes around 11 000 deaths per year in South Africa, with around 40 000 people hospitalised.
Dr Sibongile Walaza, a medical epidemiologist and the Head of Epidemiology at the Centre for Respiratory Disease and Meningitis at the National Institute for Communicable Diseases (NICD), says that it is difficult to predict what a flu season will look like beforehand.
Nicole Jennings, spokesperson for the South African Pharmaceutical company Pharma Dynamics, agrees. “Influenza is a global disease and the spread of the virus in other parts of the world can influence the trajectory of flu seasons in different regions. For now, it’s too early to make any predictions,” she says.
It is difficult to predict the trajectory of flu seasons ahead of time, Jennings says, because of a “complex interplay” of factors, including the fact that influenza viruses are constantly mutating. This makes it difficult to accurately predict which strains of the influenza virus will dominate and how they will behave.
“The level of immunity in the population can also vary from year to year due to factors, such as vaccination rates, previous exposure to similar strains and so forth,” she adds. “However, surveillance efforts, modelling and ongoing research conducted by the NICD can help the public to prepare for the cold and flu season as best possible.”
NICD guidelines published in April 2023 already stated that since the COVID-19 pandemic, there have been some changes in the timing of flu transmission.
The transmission reduction strategies – like masking and social distancing – during the pandemic had an impact on the rates of flu transmission and the duration of the flu season between 2020 to 2022, according to Dr Jocelyn Moyes, a medical epidemiologist at the Centre for Respiratory Disease and Meningitis at the NICD.
Back to normal?
Although the numbers were still much lower, it appears that the winter flu season’s peak had started to return to levels seen pre-COVID-19 in 2022 and 2023, Walaza confirms.
“In 2023, the flu season was a little bit longer than we’d seen before [COVID-19], but it started on time. So, in terms of the timing, it was similar to what we would see before COVID-19,” she says.
When exactly the winter flu season starts each year varies, Walaza says, but on average it can start anytime from the third week of April and can circulate until August. It has been known to go on longer though.
At the time of the interview, the NICD had only detected sporadic cases of flu but had not yet seen the sustained uptick in transmission which usually signals the start of the flu season. The latest surveillance data published by the NICD indicate that 108 cases of influenza had been detected so far this year. The real number of flu cases will be much higher since most cases of flu are not diagnosed.
This year’s vaccines
Walaza explains that the flu vaccine is updated each year based on the World Health Organization’s (WHO) recommendations. This is to ensure it provides protection against evolving influenza viruses seen in global surveillance programmes.
Photo by National Cancer Institute
Flu shots used in South Africa are inactivated influenza vaccines. This means they do not contain live virus and cannot cause flu.
In the public healthcare sector, the government this year procured the trivalent vaccine which protects against three strains of the influenza virus – two influenza A strains (H1N1pdm 2009 and H3N2) and one influenza B strain (known as the B/Victoria), Walaza says. These jabs should be in public health clinics by the first week of May.
In the private healthcare sector, she says a trivalent and a quadrivalent vaccine are available. The quadrivalent shot includes protection against a second influenza B strain (B/Yamagata), but that strain has not been seen circulating in a few years. These flu shots are already available in the private healthcare sector.
The level of protection provided by the flu shot varies and generally it ranges in effectiveness against infection from about 30% to 60%, according to Walaza, but importantly it protects against severe illness.
How effective this year’s flu shot will be depends on which influenza strain or strains circulate in the country. “The hope is that if an individual gets infected by any of those strains [in the vaccine], then that individual is protected or has some level of protection [against these strains] and will have some protection against severe illness” she says.
However, she adds, it’s difficult to predict how effective this year’s flu shot will be against preventing someone from getting the flu or experiencing symptoms of the flu. This is because there is always the chance that the strains which do circulate this season are different from the ones in the vaccine or have mutated so the shot becomes less effective.
Should we worry about bird flu?
At the start of April, the WHO reported that one case of avian influenza A (H5N1), one of the avian/bird flu viruses, had been detected in a person in the United States after they had come into contact with a cow who was presumed to be infected. This was the second human case of influenza A (H5N1) detected in that country, and the first case of a person being infected with this strain after coming into contact with a non-avian species.
So far, the risk to the general public is low, according to the WHO.
“Since the virus [avian influenza A (H5N1)] has not acquired mutations that facilitate transmission among humans and based on available information the WHO assesses the public health risk to the general population posed by this virus to be low and for occupationally exposed persons, the risk of infection is considered low-to-moderate,” the WHO statement said.
There are many subtypes of influenza A viruses, Moyes tells Spotlight, and avian influenzas are similar to human influenza A viruses. And so, she explains, there is always a possibility that these viruses mutate, enabling them to infect humans, or more importantly develop the ability to transmit effectively from one person to another. This could potentially cause a pandemic.
She tells Spotlight that over the last decade sporadic cases of human avian influenza have been described related to global outbreaks in birds. These cases have all been in people who have had very close contact – usually during the culling process – with sick birds. She advises that people involved in the management of avian influenza outbreaks take precautions, such as using appropriate personal protective equipment to prevent infection.
When asked whether people in South Africa need to be concerned about a potential bird flu outbreak, Walaza says so far, no cases of bird flu infection in humans – even during the recent widespread outbreaks in birds – have been identified in the country. But it is something that the NICD is aware of and surveillance for human cases during outbreaks of bird flu in the country is being conducted.
“What’s important though to note is that even when cases have been detected [in other countries] the risk of person-to-person transmission is extremely low,” she adds.
Launch of Cough Watch SA
Walaza tells Spotlight that most of the data gathered by the NICD on influenza is from surveillance in healthcare facilities, which means that not all cases of influenza are necessarily identified.
To gather additional data, the NICD is in the process of rolling out an additional digital surveillance system to detect influenza cases, called Cough Watch SA. This online web application allows the public to report influenza symptoms.
People who sign up are asked to provide basic demographic data like age and postal code. Participants will then be sent a weekly prompt asking if they’ve had any flu symptoms. If they have had symptoms, according to Walaza, then they will be asked to provide more information. This data will then be linked to the NICD database where it will be compared to other surveillance data to see if the platform could serve as an early warning system for a flu outbreak.
Cough Watch SA will be launched in the week of 7 May, says Moyes, who urged the public to help keep an eye on flu by signing up.
Professor Bob Mash. (Photo: Division of Family Medicine and Primary Care, Stellenbosch University)
By Bob Mash for Spotlight
To drum up support as South Africans head to the polls, President Cyril Ramaphosa reportedly vowed to “end the apartheid that remains in healthcare” when he hit the campaign trail. Professor Bob Mash has three health reforms on his wishlist for the incoming administration to prioritise.
South Africa is battling a quadruple burden of disease that includes HIV and tuberculosis (TB), non-communicable diseases such as diabetes, hypertension and mental health problems, challenges with maternal and child health, as well as substantial trauma from interpersonal violence and road traffic accidents.
At least 80% of the population is dependent on public sector health services. However, currently, we are in a state of austerity, with substantial cuts to the health budget that undermine years of work to improve the quality and coverage of health services.
In this context, what health reforms can be recommended?
In 2008, the World Health Organization (WHO) told us that we need primary healthcare “now more than ever” and recommended four health reforms. Universal health coverage has become a mantra for governments and implies that everyone should have easy access to quality primary care without any significant financial barriers. They also recommended that services should move away from a focus on a few priority diseases (such as HIV) and selected health programmes (such as immunisations). Rather, services should be integrated and built around the needs of people, across the life course, and in a comprehensive approach that spans health promotion, disease prevention, treatment, rehabilitation, and palliative care.
The WHO also recommended that integrated primary care be combined with essential public health functions. In other words, we don’t just worry about the people who enter the doors of the clinic but think about the health needs of all the people living in the catchment area. Finally, they recommended transformation of the leadership in health to make it more collaborative and to dialogue on policy with multiple stakeholders.
In South Africa, our last set of reforms were known as primary healthcare re-engineering. This led to the establishment of specialist clinical teams in each district to improve maternal and child healthcare, the establishment of teams of community health workers to extend the work of the clinic into the community and a focus on better health services – like health screenings and HPV vaccinations – at primary and secondary schools.
Of course, the other major policy reform that is still on the table is the introduction of national health insurance (NHI) to improve health equity and universal health coverage.
Going forward, three areas need urgent reform and attention.
More family physicians
Firstly, notwithstanding the 2030 Human Resources for Health Strategy, South Africa does not really have a comprehensive policy on the human resources for health that are needed. Thinking on primary healthcare and district hospitals has been particularly flawed in relation to family physicians. South Africa created a new medical speciality of family medicine in 2008 which has led to the training of family physicians in all nine medical schools. These are doctors who spend four years of additional training to be specialists in family medicine and to work in primary healthcare and district hospitals.
Family physicians are known to improve the quality of primary and district hospital care. They bring expertise closer to the community, capacitate the whole clinical team, improve quality, patient safety and reduce litigation. Adding a family physician to the clinical team is a cost-effective intervention. Despite this, only one province has really gone to scale with the employment of family physicians. This is a wasted opportunity and a low-hanging fruit in terms of reform.
The South African Academy of Family Physicians has a medium-term goal of one family physician at every community health centre, every district hospital and subdistrict (without a health centre). To achieve this, we need provinces to incrementally create posts over the next 10 years and to support an increase in the number of training opportunities.
Community-orientated primary care
As previously mentioned, we have introduced community health worker (CHW) teams into primary healthcare across the country. Unfortunately, many of these teams are dysfunctional due, for example, to an absence of supportive supervision, lack of resources or poor collaboration with the local primary care facility. Often, they are regarded as just extensions of the facility-based services and expected to perform tasks allocated by the clinic nurses.
The presence of these community health worker teams is, however, a huge opportunity to introduce community-orientated primary care (COPC). This model of primary care makes the switch to a focus on the health needs of the whole population served. Introducing COPC requires commitment to nine essential principles for organising primary healthcare.
Firstly, there must be a clear delineation of the community served and CHWs given responsibility for designated households (typically 250 households per CHW). Facility-based and community-based health care workers must operate as one multidisciplinary team and offer a comprehensive approach as described earlier. The team must make a careful analysis of the health needs in their community and also the resources available (government, non-government and private, health and social services) to address these needs.
At this local level, the team should prioritise the health needs in a participatory process with community and other stakeholders, and develop interventions tailored to their community. This process requires a commitment to community and stakeholder engagement. It also requires data to provide information on the health needs and this can come from households, facilities, and other sources. Finally, the service should be built around the needs of people and ensure that equity is improved.
The implementation of CHWs across the country needs to be reframed within a clearer policy on COPC. One province has already published its intention to make COPC the model of care and other provinces have examples of best practice.
Honing in on diabetes, hypertension, and mental health care
The final area that needs reform with more resources and attention is non-communicable diseases – particularly diabetes, hypertension, and mental healthcare. Historically, we have focused on the challenges of HIV and TB in service delivery, research, and donor funding. We have also been mindful of the need to improve maternal and child health.
Diabetes is now the leading cause of death in women in South Africa. Hypertension, heart disease and stroke are together the largest cause of deaths across all causes. Mental health, substance abuse and psychosocial problems may not cause death, but are a huge cause of morbidity and illness.
There is a danger of inequity by disease, and we need to ensure that we allocate resources commensurate to the problem of non-communicable diseases. In particular, we need to ensure that we have patient education and counselling that empowers people for lifestyle change, self-management and better mental health. Interventions are also needed in communities and the population to make healthier choices (on problem-solving, physical activity, healthy eating, tobacco smoking, alcohol and substance use) the easier choice.
Improving people’s health and healthcare is essential for sustainable development in South Africa. As the country heads to the polls, the incoming government would do well to keep this in mind. Such reforms will lead to higher quality primary healthcare and help pave the way for the proposed national health insurance.
*Mash is the Executive and Divisional Head of the Department of Family and Emergency Medicine in the Faculty of Medicine and Health Sciences at Stellenbosch University. The views expressed are those of the author and do not necessarily reflect those of Stellenbosch University.
April 16 2024 – The Chris Hani Baragwanath Hospital School officially opened in its new location today, marking a key milestone in the partnership between Wits University and the academic hospital. The school caters for all learners in need of longer-term and chronic treatment for various paediatric conditions. Learners between Grades R and 12 are taught.
“Sick children have multiple needs, and it’s our duty to ensure that they don’t miss out on any schooling. Everyone deserves the right to be educated and to contribute meaningfully to their communities as adults,” said Professor Shabir Madhi, Dean of the Wits Faculty of Health Sciences.
Professor Madhi noted that the previous school building will be used as a campus for medical students and to grow the university’s teaching and learning footprint at Chris Hani Baragwanath Academic Hospital.
The school district representative for Johannesburg Central, Ronica Ramdath, said that often sick children forfeit their education, which can be mitigated through the correct teaching approach and through supportive facilities. “When I first came to the school some years back, I was amazed at the teachers’ dedication. I remember seeing a teacher load all their educational resources in a bag and walk to the paediatric ward to teach sick children. Today, these children all benefit from such support,” she said.
The Wits Faculty of Health Sciences heads of schools were present, together with hospital and teaching representatives.
Meanwhile, Professor Madhi said that the university’s wifi is available at Chris Hani Baragwanath Hospital, underpinning Wits’ commitment to invest in a world-class academic hospital facility. “We are very proud of our footprint at the hospital and hope to continue to add value through research and clinical work,” he said.
Twenty-five-year-old Amahle is a proud stem cell donor – despite her fear of needles. Photo: supplied.
South Africans in need of life-saving stem cell transplants face an uphill battle due to a high rate of donor attrition. While more than 30 000 South Africans registered as stem cell donors in 2023, a 43% increase year-on-year, more than half of matched donors changed their minds when they received the call.
Palesa Mokomele, Head of Community Engagement and Communications at DKMS Africa, says that donor attrition reduces the chances of survival for many patients. “Unlike other medical donations, such as donating blood, which take place immediately, stem cell donation is a multi-stage process, meaning that those who have registered may be contacted weeks, months, or even years after they have signed up if they are a possible match for a patient. “The uncertainty around whether and when they will be called on to donate therefore impacts donor availability.”
“If notified, they will be asked to undergo confirmatory typing to determine whether they are the best match for the patient and healthy enough to donate. It is usually at this point that they decide whether to proceed with the donation or not,” shares Mokomele.
“Finding a matching stem cell donor is already like searching for a needle in a haystack, so when they choose not to follow through, it further delays the process of locating suitable donors while also increasing wait times for transplants – putting patient survival at risk,” she points out.
To prevent this and help give patients a second chance at life as fast as possible, Mokomele urges those who have registered to regularly update their donor profile to reflect their current health status and availability. “Although it can take some time between registering and receiving the call that you’re a match, it is well worth the wait.”
Twenty-five-year-old Amahle, who recently answered the call, concurs, saying, “I couldn’t believe I was going to give another person a chance to live a healthy life.”
After receiving the news, she underwent confirmatory typing and a preliminary health check. She was also given a detailed briefing call on what to expect.
As with most cases, a Peripheral Stem Cell Donation was required, which is similar to a blood donation in 90% of cases. Blood is drawn and passes through a machine (apheresis machine) that collects the stem cells after which the rest of the blood is returned back into the body. This procedure does not require anaesthetic or admission to hospital and is normally completed within four to six hours. To help Amahle generate sufficient stem cell quantities, she was injected with a hormone-like substance called G-CSF in the lead up to the donation so her body can produce more stem cells for her genetic twin. G-CSF is safe and is a significant part of the process.
Finally, the big day arrived and although she was a ball of nerves (especially given her fear of needles), she pushed through. “I was strong. I knew I needed to continue because soon I was going to save a life.”
“We applaud Amahle’s selfless act. It is moments like these that remind us of the profound impact each individual can have on another’s life. At the same time, however, we are forced to acknowledge the sobering reality that 56% of registered donors drop out. With every registration, there is hope. But hope alone is not enough. Action is what truly makes a difference. We, therefore, urge South Africans between the ages of 17 and 55 who are in good health to not only register as a stem cell donor but to act when the call for donation comes,” concludes Mokomele.
Professor Shabir Madhi of Wits University. Photo: supplied.
The Sabin Vaccine Institute presented the Albert B. Sabin Gold Medal to physician-researchers Keith Klugman and Shabir Madhi.
Nicole Basta, an associate professor at Canada’s McGill University and Canada Research Chair in Infectious Disease Prevention, received Sabin’s 2024 Rising Star Award.
The awards were made on 18 April 2024 at a ceremony in the National Academy of Sciences building in Washington D.C.
Formidable Wits alumni are world leaders in vaccinology
Klugman and Madhi received the Sabin Gold Medal, one of the highest recognitions for vaccinologists globally, for their seminal combined contributions to the development of vaccines against pneumonia and diarrhoeal disease – major causes of death in children in low- and middle-income countries (LMICs).
Klugman is a Wits University alumnus who received an honorary doctorate from his alma mater in 2023.
Madhi, also a Wits alumnus, is currently Professor of Vaccinology and Dean of the Faculty of Health Sciences at Wits University.
The Gold Medal is Sabin’s highest scientific honour. It has been given annually for more than three decades to a distinguished member of the global health community who has made exceptional contributions to vaccinology or a complementary field.
Klugman first met his then-graduate student Madhi at Wits University, where Klugman established, and Madhi expanded, a now globally renowned infectious diseases research institute. Apart from pneumonia, their work focused on maternal and children’s vaccines including influenza, respiratory syncytial virus (RSV), typhoid, and Group B streptococcus (GBS).
The evidence produced by these two awardees has and continues to inform the World Health Organization’s recommendations for vaccines. Klugman and Madhi’s research has helped pave the way for the introduction of lifesaving vaccines in public immunization programs – including the pneumococcal conjugate vaccine where their findings were pivotal in influencing vaccination policy in many low- and middle-income countries (LMICs).
Klugman’s efforts help prevent babies from dying of pneumonia
Fuelled by an early interest in science as a child in South Africa – in part due to a physician father – Klugman holds both a medical as well as a science doctorate degree from Wits University and was the first student in the school’s history to obtain them simultaneously.
He began his research career nearly five decades ago investigating the typhoid vaccine and has since distinguished himself as a formidable infectious diseases’ scientist.
Klugman is widely known for his work on pneumonia, which still kills a child under five every 43 seconds, many in the world’s poorest countries.
As the director of the pneumonia programme at the Seattle-based Bill & Melinda Gates Foundation, Klugman orchestrates strategic initiatives aimed at reducing deaths from pneumonia, RSV, neonatal sepsis, and meningitis.
He has authored hundreds of publications that have been cited over 50 000 times to date and has been elected to the National Academy of Medicine in the United States. He is also a professor emeritus of global health at Atlanta’s Emory University.
His scientific achievements aside, Klugman has long championed the need for the world’s poorest children to have equitable access to vaccines. While in South Africa he joined in Wits University’s struggle to allow access to the institution for all students.
“It is absolutely wonderful to be receiving this award, especially together with Shabir,” he says. “When I look down the list of previous awardees, I recognize the great majority of them, and it is extraordinary to now be numbered among them.”
Past award recipients include leaders of vaccinology and vaccine advocacy such as Drs. Barney Graham, Carol Baker, Bill Foege, Anne Gershon, Stanley Plotkin, and Kathrin Jansen.
Madhi’s research informed WHO recommendations on universal rotavirus vaccination
With a career spanning more than 25 years, Madhi, also from South Africa, is a trained paediatrician whose research continues to be instrumental in prioritising the rollout of vital vaccines and guiding global public health policies. At Wits University, he led clinical trials focused on respiratory and meningeal pathogens, including vaccines targeted at pregnant women and their unborn babies.
Madhi led the first study showing that a rotavirus vaccine could significantly prevent severe diarrhoea during the first year of life in African infants. That research served as a key piece of evidence for the WHO’s recommendation of universal rotavirus vaccination. In addition, he also led the first two COVID-19 vaccine trials in Africa, and a number of COVID-19 epidemiology studies which led to the first evidence suggesting that infection-induced immunity and vaccinations played a role in reducing severity of disease.
In addition to serving as Professor of Vaccinology and Dean of Health Sciences at Wits University, Madhi heads South Africa’s widely respected South African Medical Research Council (SAMRC) Vaccines and Infectious Diseases Analytics Research Unit (Wits VIDA). He is also the co-founder and co-Director of the African Leadership Initiative for Vaccinology Expertise (ALIVE).
He has co-authored hundreds of publications which have been cited over 59 000 times. Madhi is a recipient of numerous lifetime achievement awards in South Africa, as well being bestowed an Honorary Commander of the Order of the British Empire (CBE) from the British Government for his services to science and public health in a global pandemic.
“It is really humbling for me to be acknowledged for my contributions in the field of vaccinology along with those who have received the Gold Medal award,” says Madhi. “It makes me realise that the work my team and I have done is acknowledged by my peers as being of substance. Most significantly, we contributed to protecting lives in those settings where a majority of death and suffering occurs, and that is in LMICs.”
Amy Finan, Sabin’s chief executive officer, says, “I am honoured to award the Sabin Gold Medal to Dr Klugman and D. Madhi for their extraordinary work on vaccines that have saved lives in communities most in need of these interventions. Their pneumonia research has been particularly transformative in shaping our understanding of the disease and strengthening global health strategies to protect children from this vaccine-preventable disease.”
The MOU between SAHPRA and Rwanda FDA will allow the regulators to develop a cooperative partnership towards ensuring access to safe, quality, and effective health products in the respective countries.
Areas of cooperation
SAHPRA and Rwanda FDA will cooperate in joint products reviews and inspections to enable efficient access to health products. The World Health Organization (WHO) has set up an initiative for establishing a mRNA technology transfer hub, together with six spokes, in Africa as a strategy to increase mRNA vaccine production capacity in under-served regions and thus promote regional health security. Rwanda is one of the spokes and South Africa being the hub. Thus, building on this model, SAHPRA and Rwanda FDA will collaborate in the area of mRNA vaccines regulatory oversight.
“The forging of partnerships with fellow African National Regulatory Authorities, namely the Rwanda Food and Drug Authority allows SAHPRA to further our drive in enhancing and building capacity on the continent,” says SAHPRA CEO, Dr Boitumelo Semete-Makokotlela.
“The signing of this MoU underscores the profound potential of collaboration among African NRAs, affirming that the solutions to our shared challenges lie within our continent. Rwanda FDA staunchly believes in the power of collaboration and strategic partnerships. This MoU symbolises the culmination of dedicated efforts and signifies our unwavering commitment to facilitating mutual exchange and enhancing regulatory oversight. Through collaborative efforts with SAHPRA, we aim to strengthen our regulatory capacity and promote public health. As we embark on this journey together, let us harness the collective strength of our agencies to advance the pharmaceutical sector in Rwanda and beyond,” shares Rwanda FDA Director-General, Professor Emile Bienvenu.
In addition to shedding light on what people actually die of, autopsies can also play an important role in helping us to better understand disease. Tiyese Jeranji unpacks tuberculosis-related autopsy research in the Western Cape and delves into some of the fascinating complexities of this branch of TB research.
Figuring out how many people in South Africa die every year of tuberculosis (TB) is not straight-forward. On the one hand, Stats SA’s frequent mortality reports put the number at under 30 000, on the other hand, the World Health Organization (WHO) estimates that it is over 50 000.
While this may at first glance seem like a large discrepancy, there is a simple explanation. The Stats SA figures are based on what is written on death notifications, and these notifications very often do not tell the full story of what a person died of. The WHO estimate, is derived using mathematical modelling that triangulates estimates based on several data sources.
Looking at the numbers from studies that determine the cause of death (or what people actually died of) is one of the ways we know that relying on death notifications result in an undercount of TB deaths. Such autopsy studies have consistently found that many people had undiagnosed TB at the time of death and that the undiagnosed TB was often the actual cause of death.
One review study published in the journal AIDS concluded that “in resource-limited settings, TB accounts for approximately 40% of facility-based HIV/AIDS-related adult deaths” and that “almost half of this disease remains undiagnosed at the time of death”. According to WHO figures, of the estimated 280 000 people who fell ill with TB in South Africa in 2022, over 65 000 were not diagnosed.
Importance of autopsy research
Dr Muhammad Osman, Academic Portfolio Lead and Senior Lecturer: Public Health at the University of Greenwich, tells Spotlight that it is important to do TB autopsy studies because it enables us to identify TB that was not diagnosed during life – and this helps us understand the true burden of the disease.
Osman says identifying TB at autopsies has significant benefits. He says by overlaying health seeking behaviour (how people visit clinics), we can identify missed opportunities for TB screening and design interventions to improve screening for TB. “We could trace family contacts of the deceased and offer TB screening and prevention. This is not taking place at present,” he says.
Osman and his colleagues published a paper in the International Journal of Infectious diseases in 2021 looking at TB in people with sudden unexpected death (SUD) in Cape Town. They found that active TB was identified at post-mortems in 6.2% of the 770 cases they studied. More strikingly, in around 92% of those cases the TB had not been diagnosed while the person was alive.
Osman says that these days there is an increasing awareness of undiagnosed and untreated TB. He points out that new interventions to improve TB testing and diagnosis have been implemented such as targeted universal testing — an approach by which people who do not have any TB symptoms, but who are considered to be at high risk of TB, are routinely offered TB tests.
He says these days healthcare worker risk is considered more carefully and he stresses the importance of protecting forensic and pathology teams. (Forensics focuses on determining the cause and manner of death while pathology is the study and diagnosis of disease through examination of tissue, cells, autopsies, and so on.)
Closing the gaps
Osman says their study also identified a gap between the pathology services and access to routine health service records. “We thought that this is an essential gap to close – the forensic/pathology services need access to routine health service. For a limited number of these deaths we were able to match their records to the public health clinic and hospital records – and many of them had contact with the health services in the six months before death,” he says.
“If forensic pathologists are given full access to the health records, they would know the timing of previous TB and the treatment outcomes of those episodes. The lung changes seen with TB are different in the case of active TB and healed/recovered TB. There are well documented macroscopic (what’s is seen by the examination) and microscopic (seen through histology and microbiology) findings,” says Osman.
A complex disease
The study of TB is complicated by the fact that TB can occur at several stages on a continuum and can impact several different parts of the body.
Professor Threnesan Naidoo, research pathologist at the African Health Research Institute (AHRI), tells Spotlight that when people think of TB, they usually think of the person who’s been coughing for a few months, loss of weight, loss of appetite, having night sweats, and maybe coughing up some blood. “But there’s a journey to that point and then generally beyond that point, and clinically, there’s a continuum of the disease. We refer to it as latent disease, subclinical, active and then healed TB,” he says. It is an area in which things are changing fast – a paper published in the Lancet medical journal last week proposed dividing TB into five stages.
Naidoo says autopsies provide an opportunity to study TB at different stages (latent, subclinical, active, healed) especially when someone with TB dies of another cause. He says they can encounter people at any stage along the TB continuum because at any point someone could be shot, stabbed, or involved in a motor vehicle accident. “You (pathologist) have a unique opportunity to study the effect of TB on cells and tissue physically under a microscope and not through imaging (x-ray),” Naidoo says.
Autopsies also presents the opportunity to look at TB disease not only in the lung, but also the brain, thyroid gland, kidney or urinary system since TB has the capacity to spread everywhere, explains Naidoo.
“Autopsy gives you the opportunity to study TB everywhere,” he says. “Clinically (when someone is alive), you don’t go about investigating the entire body. Neither is it practical nor feasible or safe. But [with an] autopsy you’re examining the entire body anyway. We study TB in totality,” he says.
How it is done
The standard manner of doing an autopsy involves a thorough examination of the body. Naidoo explains that the process starts with an external examination to document injuries, marks, and other physical characteristics that are visible. The internal examination involves dissecting organs, tissues, and body cavities to identify any abnormalities or signs of disease. Samples may be taken for further analysis, such as toxicology tests, histological examination, or TB research.
Any findings from the samples, Naidoo notes, must be interpreted taking into account changes that occur in a dead body. “[In] the living, you know, it’s a living person and they’re able to do things and you’re able to see things on imaging (X-Ray), but in the dead you have to account for the fact that the person has now demised and certain changes occur after death.”
Autopsy study at UCT
An ongoing study at the University of Cape Town is exploring the role of lymph nodes in the spread or containment of TB disease by looking at tissue of the deceased.
Much TB research so far have been done on animals and not on humans, points out Dr Virginie Rozot, research officer at the South African TB Vaccine Initiative (SATVI) and co-principal investigator of the UCT study. “We have great non-human primate and great mice studies that try to underline the mechanism of the disease progression. However, animal models are not a true reflection of what happens in humans.
“For the longest time in these human studies, most studies have been done in the blood and what is happening in the blood has been taken to correlate with what is happening in the lung.”
In short, autopsies allow researchers to look directly at lung, brain and other tissue in a way that simply isn’t feasible in living people.
“So the only way you can actually access tissues is to do post mortem studies. Post mortem studies have been happening since the beginning of last century. And they were like fantastic studies, but the tools were not the same as we have today. I think that should come back to the front of the scene of research because then you can ask all the questions we’ve been trying to answer on what is happening in the tissue by looking into the blood,” she says. “Autopsy allows us to study the exact part we want to study not just the blood.”
Collecting samples
In collaboration with the Western Cape Forensic Pathology Service, UCT has created a postmortem sample collection platform to help with TB research. By leveraging the Inquest Act of 1959, which states that people that die of unnatural causes must undergo a medico-legal investigation to determine the cause of death, Rozot and her team come in to conduct a post-mortem to get their samples. They aim to do the post-mortem in less than 24 hours after death.
Since starting this study about eight months ago, they have done 125 autopsies , with a consent rate of 64%. “I think our consent rate is incredible. We are still putting together our findings to determine how many cases of TB we have found so far by looking at autopsies,” says Rozot.
Representative samples
Dr Laura Taylor, forensic pathologist at the Western Cape Forensic Pathology Services, says the bodies that they look at, in line with the Inquest Act relating to unnatural deaths, are representative of people in South Africa. “However, they are not exactly representative of the entire South African population because there are certain socio economic groups that are more likely to die of unnatural deaths due to increased prevalence of trauma and violence in their communities,” she says.
Because there is no central database, Taylor couldn’t say how many cases of TB they find among the deceased. “[T]here are autopsy records or reports which are written for each case, but there is no central database for TB specifically detected [through] autopsy,” she says.
Forensic autopsy and other diseases
Rozot and Naidoo share the view that, if done well, TB autopsy studies can help shed light on other diseases.
The value of this information is that people dying with or from TB will also have any of the other conditions such as hypertension, HIV, and diabetes, Naidoo says.
“You can work out all those variables… [people] don’t just come with diabetes, the diabetes changes the face of TB, HIV changes the face of TB and TB changes the face of those diseases as well. So, the complexity of it becomes something that we need to pay attention to, and look at all the common variables, like the association of TB and HIV is a big one. So studies might look at HIV infection and how it may affect TB and vice versa. Same with diabetes, hypertension, any of the other non-communicable diseases as well,” he concludes.
The South African healthcare landscape is undergoing a transformative shift, driven by the rapid advancement of technology. At the forefront of this change is the rise of the “digital nurse,” a testament to the increasing integration of technology into the nursing profession. This transformation is not only streamlining processes; it is addressing critical challenges like the nation’s nurse shortage while ultimately improving patient care.
Embracing convenience and accessibility
Virtual platforms have become commonplace in the nursing world, facilitating efficient and accessible professional development for nurses through online meetings, networking opportunities, and educational resources. This fosters a more connected and knowledgeable nursing community, better equipped to serve patients.
Telehealth consultations, another facet of digital nursing currently revolutionising patient care, provide convenient and accessible medical consultations from the comfort of one’s home, eliminating long wait times and unnecessary travel.
Mitigating nurse shortages and ensuring quality care
South Africa grapples with a significant nurse shortage, placing a strain on the healthcare system to which digital nursing offers a practical potential solution. By leveraging technology, nurses can effectively manage larger patient volumes, reducing the burden on the existing workforce and optimising resource allocation. Remote monitoring systems and AI-powered tools further empower nurses by providing real-time patient data and facilitating early intervention, ultimately improving the quality of care delivered.
Additionally, embracing technology ensures that patients, even in underserved areas, receive quality care. The efficiency gained through virtual platforms allows nurses to allocate their time effectively, addressing minor health concerns remotely and reducing the strain on healthcare facilities for non-emergency cases.
However, it must be pointed out that although leveraging technology allows nurses to effectively manage larger patient volumes, which can alleviate the strain on the current system, this doesn’t necessarily mean fewer nurses are needed, but rather that technology empowers existing numbers to reach a wider patient base to deliver more efficient, personalised care.
Evolving alongside technology: the digital nurse of tomorrow
As the healthcare industry embraces digital technologies, the role of the nurse will continue to expand. While traditional nursing skills will remain essential, the “digital nurse” of the future must possess additional competencies. Acquiring proficiency in digital tools and equipment, along with the capability to interpret and analyse digital data, will be crucial for delivering effective patient care. However, the most critical attribute for the digital nurse will be the willingness to adapt and embrace constant technological advancements. This will require a mindset shift that comes with acknowledging that traditional methods might not be sufficient in the face of evolving patient needs.
The challenges and opportunities in change
While the adoption of digital nursing brings numerous benefits, challenges remain. Resistance from individuals accustomed to traditional healthcare practices is one hurdle. However, with the younger generation being more adaptable, the shift towards digital nursing is expected to gain wider acceptance as technology advances. To ensure the success of this digital-first healthcare, it will be necessary to focus our attention on upskilling, which means recognising that continuous training and development programs are vital for nurses to remain proficient in the face of change.
On the flip side, a change in perspective from nursing professionals themselves will be necessary. This means embracing a growth mindset and being open towards new technologies to adapt and thrive in the digital age. Lastly, healthcare professionals as a whole need to bear in mind that transformation is essential to meet the evolving needs of patients, which includes catering to a growing preference for digital healthcare solutions. Continuing to meet the needs of patients is the only guaranteed way for nursing professionals to ensure their relevance in the future. By embracing technology and fostering a culture of continuous learning, South Africa can empower its nurses to become the digital healthcare leaders of tomorrow.
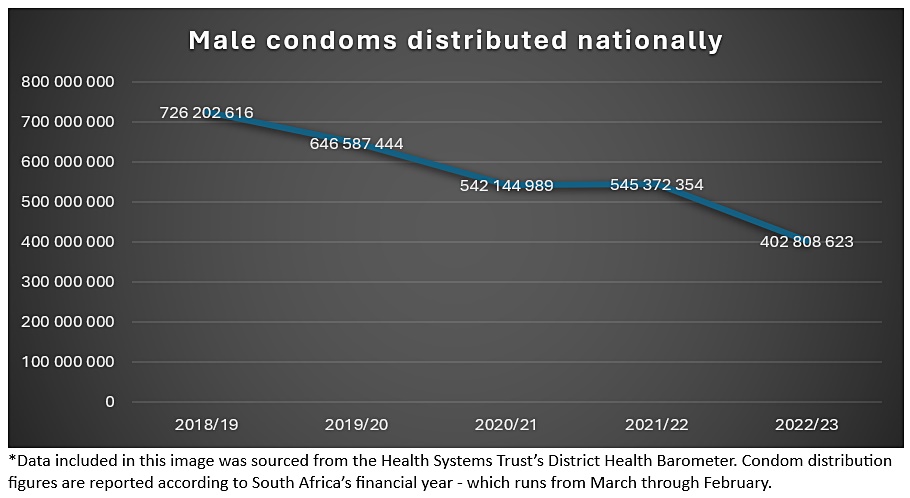
Condom distribution in South Africa has dropped dramatically over the last five years, finds a Spotlight analysis of data recently published in the Health System Trust’s District Health Barometer.
The South African government distributed 45% fewer male condoms in 2022 than it did in 2018. The total number of male condoms distributed dropped by over 300 million from 728 million in the financial year from March 2018 to February 2019 to 403 million in 2022/2023. Female condom supply also declined over this period, but not as sharply.
The full extent of the actual decline in condom supply across the country over the past five years has not previously been reported. The Democratic Alliance, though, did raise the alarm bells about condom supply challenges in Gauteng in April 2023.
Provincial departments of health have pin-pointed the time required for certification of condoms by the South African Bureau of Standards (SABS) following the start of a new condoms tender in 2022 as a key driver of the decline, yet Health System Trust’s District Health Barometer (DHB) data shows that condom distribution figures have in fact steadily declined over the past five years. Similarly, while COVID-19-related supply chain interruptions were a contributing factor to supply shortages at the height of the pandemic, the decline in government supplied condoms started before the pandemic and continued after COVID-19 supply chain disruptions were resolved (as shown in the below graph).
The large decline in condom distribution in South Africa is alarming in the context of the country’s ongoing fight against HIV. While other biomedical interventions are now available to protect against HIV (such as HIV prevention pills), condoms should remain a cornerstone of countries’ HIV prevention strategies according to the World Health Organization.
Research conducted by the University of Witwatersrand’s Health Economics and Epidemiology Research Office (HE2RO) has found that condoms are not only the most cost-effective intervention available to government to combat HIV, but that provision of condoms is in fact cost saving for the country’s health system.
Where did condom distribution fall the most in 2022?
According to the DHB data, all provinces except for the Free State saw a decline in condom distribution in 2022/2023 compared with 2018/19 levels (as shown in the below graph).
The Eastern Cape distributed 65% fewer condoms in 2022/23 than it did in 2018/19, Gauteng and the Northern Cape distributed around 60% fewer, Limpopo 52% fewer, and the Western Cape around 46% fewer. With a reduction of around 19% over the five years, the decrease was much less pronounced in KwaZulu-Natal than in South Africa’s other provinces with large populations.
Male condoms distributed by province
Province
2018/19
2019/20
2020/21
2021/22
2022/23
Eastern Cape
73 672 416
78 817 157
51 122 509
45 839 588
25 490 700
Free State
50 756 150
53 246 000
52 248 000
55 352 800
52 469 700
Gauteng
172 953 486
135 857 486
146 303 254
129 075 303
69 220 678
KwaZulu-Natal
111 028 599
108 503 920
96 529 200
106 967 000
89 664 600
Limpopo
82 563 322
67 818 200
53 325 900
52 862 900
38 910 442
Mpumalanga
67 150 600
51 749 400
38 316 000
31 364 066
35 627 000
Northern Cape
13 934 960
12 959 400
10 825 929
9 518 000
5 194 000
North West
50 820 283
55 579 921
39 841 971
42 361 097
30 810 803
Western Cape
103 322 800
82 055 960
53 632 226
72 031 600
55 420 700
*This table shows a breakdown of male condoms distributed by province, according to data from the Health Systems Trust’s District Health Barometer.
What caused the decline in condom supply?
Condoms are tendered nationally by the National Department of Health for a three-year period. Condoms procured by government must be tested and certified by the SABS before distribution.
Neither the National Department of Health, nor the Gauteng Department of Health responded to questions from Spotlight about the reasons for the decline in condom distribution. However, Gauteng’s Department of Health has previously pinpointed SABS certification processes as the culprit for condom supply shortages in the province. According to an April 2023 media statement by the Gauteng Department of Health, suppliers that received tenders to supply condoms to the public sector were unable to supply condoms to the province while awaiting SABS certification in 2022 – resulting in low condom stock in the province.
Spokesperson for the Eastern Cape Health Department, Sizwe Kupelo, told Spotlight in response to questions for this article that in 2022/23 “for most of the year there were no condoms to distribute”.
Kupelo said that the decline in condom distribution in the Eastern Cape was due to a combination of lags in supply availability while condom suppliers were awaiting SABS certification and challenges in delivering condoms to distribution sites in the province.
“2022/23 was the end of the condom supply contract and the period to award a new contract effective from 1st April 2022. This transition experienced a delay in availing the condoms due the SABS quality assurance process that could be finalised only around September 2022,” said Kupelo, adding that the province started to receive condoms from October of the same year.
“The second reason were related to suppliers who were not finding it easy to deliver to Eastern Cape areas due to the high cost of transportation to the identified 26 delivery distribution sites across the province. Suppliers are all based in Gauteng,” said Kupelo. This matter he said was now resolved.
Kupelo added that condom supply in the province is now improving. He said that the province had reached 96.7% of its target to distribute 17 million condoms in quarter 3 of 2023/24 (quarter 3 of 2023/24 is September to November 2023).
The SABS’ response
Lungelo Ntobongwana, acting CEO of the SABS, told Spotlight that all condoms that are distributed nationally by the Department of Health are tested at the SABS condom laboratory in Groenkloof, Pretoria. “The laboratory is an accredited and dedicated laboratory for the testing of condoms,” he said.
“Downtime or challenges to operations as a result of unplanned disruptions have been experienced on rare occasions and the SABS has incorporated contingency plans to ensure that the testing processes and deliverables would not be negatively impacted.
“The value chain, from the production of condoms to the distribution and usage of condoms, requires the intervention of various role players. When there is a shortage of condoms, it could be due to several reasons and chinks in the value chain. The SABS can categorically state that there are currently no challenges in its laboratory or deliverables regarding the testing of samples,” said Ntobongwana.
Did clinics run out of condoms in 2022/23?
The National Department of Health insisted in April 2023 that while Gauteng was facing low stocks of condoms, there were no serious condom shortages in the country.
Surveys conducted by community-lead clinic monitoring group Ritshidze also show that condoms remained available in most facilities – but not all – throughout the year, but also indicate a pattern of rationing by health care workers and clinics. In some cases, they say condoms are only available in public clinics on request, and key populations often face stigma and discrimination when seeking to access condoms and lubricant.
Surveys conducted by Ritshidze in 2022, found that only 55% of sex workers could get enough condoms at public facilities. Ritshidze recommends that “condoms and lubricants should be available at all facilities and can easily be placed in the toilets or other areas of the clinic where people could take them without the fear of being seen and judged by others, or being told to put some back”.
Anele Yawa, General Secretary of the Treatment Action Campaign (a member of Ritshidze), told Spotlight that the organisation faced challenges in accessing adequate condoms for its community outreach efforts. He said when TAC undertakes community outreach efforts, its members request condoms from public health facilities for distribution in communities but are sometimes told that there are not enough condoms for this.
Yawa added that people seeking condoms from public clinics are often told they can only take a limited number of condoms because of stock availability and that in some clinics “the condom box is empty, there are no condoms”.
Has the decline in condom availability impacted condom usage?
There are some concerning indicators that condom usage in the country is declining, which may in part be related to the drastic decline in condom supply.
The Human Science Research Council (HSRC), which conducts regular surveys of HIV knowledge and sexual behaviour in South Africa, recently released early data from its 2022 survey. The survey showed that teenagers and young adults between 15 and 24 years old reported lower rates of condom use at last sex than in previous survey years. The data presented did not pin-point a cause for the decline – apart from supply constraints, other factors like a decrease in people’s perceived risk of contracting and dying of HIV may also play a role.
The HSRC will release its full survey results in April 2024, which are expected to provide more insight into why condom use at last sex declined among 15- to 24-year-olds in 2022.
Another concerning indicator of declining condom usage is the reported rise in sexually transmitted infections (STIs) in Gauteng. Spotlight reported in February that the worried resurgence in reported cases of STIs in Gauteng in 2023 is a wake-up call that control and management strategies are not keeping pace with the growing disease burden in South Africa’s most populous province.
In response to the increase in STIs, Gauteng’s Health MEC Nomantu Nkomo-Ralehoko recommended expanded, consistent condom use – noting a number of factors including non-use of condoms, inconsistent use of condoms, and the forgoing of condoms by people using Pre-Exposure Prophylaxis (PrEP) as contributors to the rise in STIs. PrEP refers to antiretrovirals taken to prevent HIV infection.
Dismissing the conclusion of a causal relationship between a higher number of people being initiated on PrEP and the higher recorded number of STIs, Professor Linda-Gail Bekker, director of the Desmond Tutu Health Foundation, told Spotlight that there is no evidence to back up the claim that PrEP is leading to lower rates of condom usage. She added that the increase in STI diagnoses may be attributed to increased rates of testing, which has increased in the PrEP era.
“The notion that sexually transmitted infections have suddenly increased in the era of PrEP does not have evidence to support this,” said Bekker, adding “we have no strong evidence to suggest that people are having more condomless sex than before”.
“The value of condoms as a measure against sexually transmitted infections as well as unwanted pregnancy is not disputed and condoms remain the corner stone of the HIV response” said Bekker. “However, we know that for many people, and particularly young women and young men who have sex with men, the choice to use male condoms is not always a given and negotiating condom use may not be easy and can be dangerous,” she said.