A realistic update on the amount of funds lost to fraud, waste and abuse in the South African healthcare environment as well as a special address dedicated to the value and protection of whistle blowers will lead discussions during the annual Board of Healthcare Funders (BHF) Healthcare Forensic Management Unit (HFMU) Fraud, Waste and Abuse (FWA) Indaba at The Houghton in Johannesburg on Wednesday, 22 November.
Convened to coincide with International Fraud Awareness Week and to be moderated by BHF Forensic Unit chair, Dr Hleli Nhlapo, the Indaba spotlight will be on “Strengthening a Culture of Integrity and Accountability – New Strategies for a Corruption Resistant Future “ – subject of the keynote address.
The event will once again endorse the BHF’s representative role as a guardian of the interests of medical schemes, administrators and managed care organisations not only in South Africa but also Lesotho, Zimbabwe, Namibia, Botswana, Mozambique, Malawi and eSwatini.
To this end an unprecedented feature this year will be a panel discussion by Southern African Development Community (SADC) members on strengthening anti-corruption efforts in the SADC Region with cross-border co-operation.
“Promoting the culture of whistle blowing and the protection of whistle blowers” will be a significant key point on the Indaba agenda with the promise of a lively discussion on the encouragement of whistle blowing with the non-negotiable proviso that specific mechanisms should be put in place for corruption reporting without repercussions.
Until last year fraud, waste and abuse losses in South Africa were generally estimated at just under the R30-billion mark, but as pointed out by the Special Investigating Unit’s Advocate Andy Mothibi at the BHF Conference earlier this year, this figure was likely to be a lot higher.
Fraudulent activities relating to false claims was still a major contributing factor to these losses, he explained, alluding to an observation that anything between 5% and 15% of all medical aid claims could include elements of FWA.
Spurious activities in this regard will no doubt emerge in some of the answers to the Indaba agenda question “Is there ‘Rent Seeking’ in our Healthcare System?” – “rent seeking” being an economic term for an individual who or an entity which seeks to increase their own wealth without creating any benefits or wealth by activities which aim to obtain financial gains and benefits through the manipulation of the distribution of economic resources.
In the same vein, the discussion on “Cracking the Code: Uncovering and Combating Organized Crime Networks in Healthcare”, should shed light on current FWA challenges followed by collaborative measures to counter these such as the use of the HMFU FWA portal introduced four years ago with the prime objective of combating healthcare fraud, waste, and abuse.
Another important element of FWA which has risen to the fore particularly since the successes of the SIU, has been the recovery of lost funds. This will be the focal point of a presentation “Navigating the Road to Restitution: Strategies for Successful Civil Claims Recovery in Healthcare” during which a series of steps to recover losses from wrongdoing or fraud in healthcare are scheduled to be presented.
Going by previous deliberations on the topic, these are likely to emphasise the need for a dedicated legal team with healthcare law and fraud recovery expertise and a commitment to justice for fraud and misconduct victims.
The day’s proceedings will conclude with the SADC member panel discussion on “Cross border Co-operation: Strengthening Anti-Corruption Efforts in the SADC Region”.
Members are expected to deal with important issues such as, not least, the protection of whistle blowers, as well as encouraging healthcare workers in their specific countries to report corruption risk-free with the promotion of law enforcement capabilities and related awareness campaigns.
The National Health Insurance (NHI) will further widen the inequality gap, put even more pressure on the already overburdened taxpayer and lead to an outflow of medical expertise should it be implemented. AfriForum has detailed these and other consequences of the NHI in a new research report.
In its report, the organisation details, among other things, the ideological basis of the NHI, the place it occupies in the ANC’s National Democratic Revolution (NDR), the economic consequences of the centralisation of health financing and the vagueness in the bill itself. Furthermore, the report provides an overview of centralised health systems in a number of other countries and how they compare or contrast with the economic and policy environment in South Africa.
One of the biggest issues with the NHI Bill is its funding. According to the report, four possible sources of income are currently being investigated that will have a negative impact on taxpayers – including payroll tax. This option entails that the government will require employers to recover a portion of their employees’ salaries which will then be remitted to the government – this on top of the deductions that are already recovered from employees’ salaries. South Africa’s marginal income tax is already higher than that of most other countries such as Canada, the USA and Namibia. Although this is the same as Australia, Switzerland and South Korea’s marginal income tax, South Africa has little in terms of service delivery to show for it.
The research finds in almost all the areas of investigation that NHI will be harmful to the economy and negative for the well-being of most South Africans and concludes that the bill should be rejected by parliament and opposed by the health sector.
According to Louis Boshoff, Campaign Officer at AfriForum, this report appears at a critical time where the parliamentary battle over the NHI Bill rages on and many misconceptions about it are circulating. “NHI is easily summarized incorrectly with slogans such as ‘free health care for all’, but the report takes a step back to obtain a more sober and objective picture, namely that the policy is expensive, unmotivated and unworkable,” says Boshoff.
The full report is available at www.jougesondheid.co.za, where the latest information on NHI is posted.
Newly announced results of a pivotal phase 3 trial have demonstrated the effectiveness of a new one-dose treatment for gonorrhoea. The medicine, called zoliflodacin, is the first new drug developed to treat gonorrhoea in over 30 years. More than half of the 930 patients included in the trial were from South Africa, including women, adolescents, and people living with HIV.
Zoliflodacin, which was shown to be non-inferior to (as good as) the currently used treatment in treating uncomplicated gonorrhoea, provides an important new tool to combat rising rates of drug resistant gonorrhoea. It was found to be generally well tolerated and there were no serious adverse events or deaths recorded in the trial. So far, only top line results have been shared in a media release and the findings have not yet been published in a medical journal. (You can see some technical details of the study design on ClinicalTrials.gov)
The World Health Organization raised the alarm about increasing rates of drug resistant gonorrhoea in 2017, noting the emergence of cases of untreatable gonorrhoea resistant to all available antibiotics. According to the United States Centers for Disease Control and Prevention “medication to treat gonorrhoea has been around for decades, but the bacteria has grown resistant to nearly every drug ever used to treat it”. They say: “only one class of antibiotics known as cephalosporins remains to treat the infection”.
As a drug from a new class of antibiotics, zoliflodacin, offers a new potential treatment for patients whose gonorrhoea was previously untreatable, as well as a new tool for safeguarding the ongoing effectiveness of currently available antibiotics.
How zoliflodacin may change gonorrhoea treatment
Professor Sinead Delany-Moretlwe, Director of Research for Wits RHI and the National Principal Investigator for the trial in South Africa, told Spotlight that while zoliflodacin may be used to treat drug resistant gonorrhoea, it also provides an attractive new treatment option for first-line treatment of gonorrhoea in some countries (in other words, gonorrhoea that is not resistant to other treatments).
Zoliflodacin, which is taken as a single oral dose, is simpler to administer than the current standard of care, which involves a combination of injectable ceftriaxone and oral azithromycin. Removing the need for an injection could simplify the administration of gonorrhoea treatment and improve its uptake.
Using zoliflodacin as first-line gonorrhoea treatment can also help safeguard the ongoing effectiveness of cephalosporins (including ceftriaxone), according to Delany-Moretlwe, which she adds are needed not just for treatment of gonorrhoea, but also other infections.
According to Delany-Moretlwe, because zoliflodacin is the first of a new class of antibiotics with novel mechanisms of action and without existing cross resistance, the hope is that widespread use of zoliflodacin as first-line gonorrhoea treatment will slow the emergence of resistance compared with the medicines currently being used.
The Global Antibiotic Research and Development Partnership (GARDP), a non-profit that sponsored the trial, points out that: “Antimicrobial resistance [AMR] has been around for millions of years, long before the first man-made antibiotics. So, drug-resistant bacteria are inevitable and will eventually affect all antibiotics”. They state: “to beat AMR we need a steady supply of new antibiotics to be developed that are effective against drug-resistant bacteria, particularly for priority pathogens that have the greatest public health impact.”
Gonorrhoea in South Africa
South Africa has incredibly high rates of gonorrhoea, with an estimated 2 million new cases annually. While data on rates of drug resistance in the country is limited, the data that is available indicates that ceftriaxone resistance in the country is low, but azithromycin resistance is concerningly high in some parts of the country.
As there is no routine screening for gonorrhoea in South Africa, linkage to treatment remains a challenge. Currently, diagnosis is largely done through symptomatic reporting by patients. But this approach misses many cases as some patients do not self-report symptoms and some cases of gonorrhoea are asymptomatic.
In 2022, the Southern African HIV Clinicians Society released new guidelines for the management of sexually transmitted infections which called for provider-initiated symptomatic screening and provider-initiated diagnostic screening in high-risk populations.
The country’s new National Strategic Plan on HIV, TB and STIs has set a target to increase the number of pregnant women tested for gonorrhoea from 10% in 2023 to 80% by 2028 and has committed to implementing diagnostic testing in other priority populations, including adolescent girls and young women.
How will new gonorrhoea treatments be commercialised?
Zoliflodacin was developed by GARDP in collaboration with the company Innoviva Specialty Therapeutics. According to GARDP, it holds the rights to register and commercialise zoliflodacin in more than three-quarters of the world’s countries, including all low-income countries, most middle-income countries, and several high-income countries. While, Entasis Therapeutics Limited, an affiliate of Innoviva Specialty Therapeutics, “retains the commercial rights for zoliflodacin in the major markets in North America, Europe, Asia-Pacific, and Latin America”.
South Africa is one of the countries in which GARDP holds the rights to register and commercialise zoliflodacin. It is anticipated that this will be done through selection and licensing of companies to manufacture and supply zoliflodacin in South Africa and other countries where GARDP holds commercialisation rights.
GARDP recently launched a request for proposals from partners that are interested in commercialising zoliflodacin. GARDP has also signed a memorandum of understanding with two generic producers to explore opportunities to commercialise the medicine in low-and-middle-income countries.
While the price that will be offered by commercial partners for the product remains to be seen, it is anticipated that products will be made available at affordable prices in line with GARDP’s goal to ensure that “all GARDP products are available, affordable, and appropriately used across populations that need them”.
“This is the first study to address a World Health Organization priority pathogen that has been sponsored and led by a non-profit organization,” says GARDP.
“This demonstrates that GARDP’s model can play a crucial role in helping to fix the public health failure at the heart of the global AMR crisis,” says Professor Glenda Gray, GARDP board member and President of the South African Medical Research Council.
SA involvement
According to GARDP, South Africa had the highest number of participants in the global trial, across six sites in four provinces: Wits RHI in Hillbrow, Johannesburg; the Desmond Tutu HIV Foundation in Masiphumelele, Cape Town; Setshaba Research Centre in Soshanguve, Gauteng; the SAMRC’s clinical research sites in Botha’s Hill and Tongaat in KwaZulu-Natal; and Ndlovu Research Centre in Groblersdal, Limpopo.
“We have also been able to leverage our HIV experience to build capacity for trials of novel STI technologies, a previously neglected area. Undertaking this vital work on a new treatment for gonorrhoea has also given us the opportunity to focus sharply on the local situation in South Africa,” says Delany-Moretlwe.
By Matshidiso Lencoasa and Dominic Brown for Spotlight
In the context of weak economic growth, lower-than-expected tax revenues, and the implementation of measures to reduce public spending, there is “rising panic” ahead of this year’s Medium Term Budget Policy Statement (MTBPS). The concern for health care provision is palpable as anticipated budget cuts threaten the country’s already fragile and understaffed public healthcare system. There is only one nurse for every 224 patients in the public health system, and over 5 000 nursing posts remain unfilled (something primarily attributed to funding constraints).
In times of poor economic performance, difficult policy choices and trade-offs arise, and it may be tempting for fiscal policymakers to slash public health spending. However, without meaningful consideration of the impact of these decisions on our people and our constitutional right to access healthcare, the MTBPS risks exacerbating the hardships faced in our country.
Austerity context
South Africa’s economic outlook has been riddled with challenges permeating our healthcare system. Over the past decade, the country’s economic growth has underperformed, falling in real terms from 2.3% in 2013 to 0.1% in 2023. National Treasury has responded to this with cuts to social spending, including healthcare. Public health is receiving fewer resources in real terms, and our government spends more on debt-servicing (R340.5 billion in the 2023/24 Budget) than on healthcare (R259.2 billion in the 2023/24 Budget). Moreover, healthcare’s allocation of R259 billion in 2023/24 was the same as last year’s allocation, meaning that the value of resources allocated to healthcare this year is eroded by Consumer Price Index (CPI) inflation, which was projected to be 4.9% at the time of the Budget Speech in February this year.
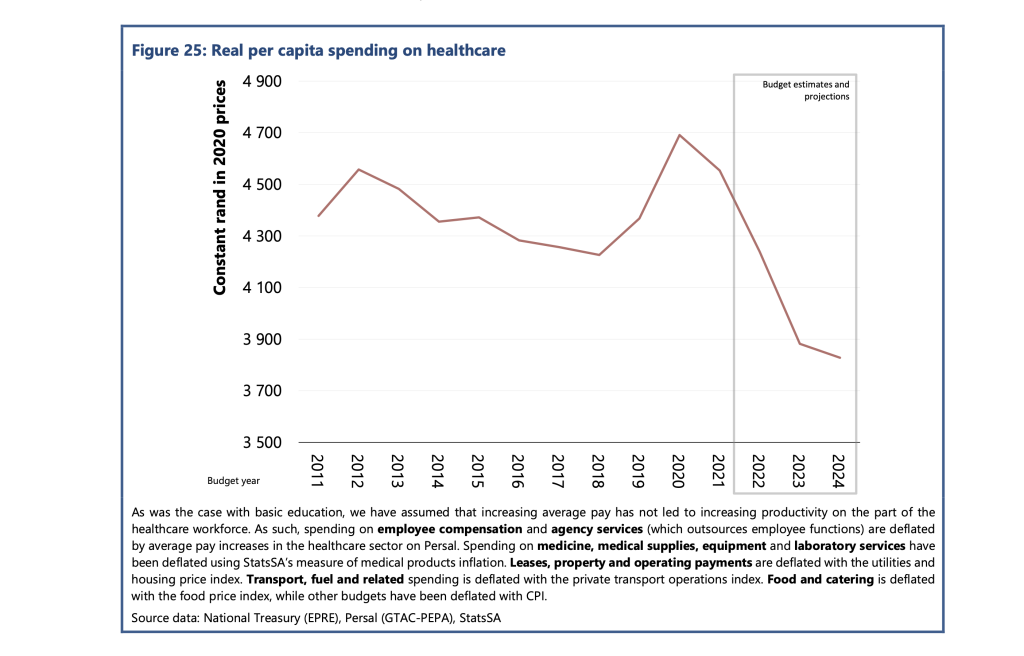
According to the Public Economy Project, the spending per healthcare user fell from approximately R4 600 in 2012 to R4 300 in 2018. PHOTO: Sourced from the Public Economy Project (PEP) Public services, government employment and the budget
Worse, this allocation needed to account for the rising demand projected for public healthcare services. Currently, about 84% of the population relies on the public health care system. This figure is projected to increase in response to population growth and rising unemployment making medical aid inaccessible for many in the country.
According to the Public Economy Project, after accounting for inflation and population growth, the spending per healthcare user fell from approximately R4600 in 2012 to R4300 in 2018. Based on current budget estimates, it is projected that real per capita public health spending will fall below R3 900 by 2024/25.
Implications for health care staffing
Although the 2023/24 budget proposed a measly 1.5% nominal increase to the public sector wage bill, President Cyril Ramaphosa approved a 3.8% increase for this year. However, Treasury’s cost containment measures have stipulated a hiring freeze for the rest of the 2023/24 financial year and no further allocations towards personnel expenditure. This is despite the Department of Health’s 2030 Human Resources for Health Strategy quantifying that 96 586 additional health workers are required to bolster the healthcare of all provinces to the same standard as the third-ranked province by 2025. This requires an additional cost of nearly R40 billion in total.
The real-life implications for South Africans are dire. Chris Hani Baragwanath Hospital – the largest hospital in Africa and the third largest hospital globally – faces significant staff shortages, cancelling almost 900 surgeries in 2022. The underpaid and overworked Chris Hani Baragwanath Hospital nurses have reported “pooling funds to buy patients bread.” Doctors at Nelson Mandela Bay’s Livingstone Tertiary Hospital have attributed “suboptimal, undignified patient care” to budget shortages and forecast higher medico-legal claims, which National Treasury described as a “sub-national risk”. However, budget measures that impede public health care’s ability to address staff shortages exacerbate the likelihood of errors by overstretched staff, worsening the medico-legal claims bill for health departments.
Gender and budget cuts
Health budget cuts disproportionately burden women. This burden is evident in the inordinate risk and prevalence of HIV that women face in the country. It is exacerbated by women’s higher and differentiated health needs (including those for reproductive and maternal health). Women-led households are 40% poorer, and unemployment is most prevalent among women. These socioeconomic factors make women more dependent on the public health system.
Budget cuts and underspending clearly have implications for gender equity in the country.
Furthermore, the Department of Health has recognised the healthcare workforce as a critical driver of inclusive economic growth and a means to create decent work for women, especially in rural and underserved communities. Over 90% of nurses in our public health system are women, and in our society of unequal gendered norms, it is also women who carry the care work burden in the home. Many will likely interpret any proposed MTBPS cuts without factoring gender equity implications as an under-appreciation of women’s labour in making a fragile healthcare system and society work.
A case for human rights budgeting
Although improving the country’s economic outlook is imperative, without consideration of the power that fiscal policy has in advancing human rights in the country, there is a likelihood of tabling an MTBPS that impedes the realisation of constitutionally guaranteed human rights in the country.
More than ever, our health system requires inculcation of human rights impact assessments as recommended by the UN Committee on Economic, Social and Cultural Rights, to which South Africa is a party. These assessments could compel policymakers to outline how the resources allocated will protect the right to access healthcare for all in the country, especially when budget cuts are considered. Including these considerations in budget policy may further advance meaningful public participation processes in fiscal policy.
Furthermore, a gender-responsive MTBPS is long overdue and a powerful means to protect the most vulnerable people in the country from reduced social investment. The health budget could be tagged to identify programmes with gender as a principal or significant objective and areas which would need to be protected and consideration of the gendered experience of healthcare to prevent fiscal policy from worsening gender inequities in the country. Budget policymakers should further promote the collection of gender-disaggregated data and establish indicators and benchmarks on gender and other socio-economic factors to advance a more equitable funding allocation.
Lastly, authentic public engagement will allow National Treasury and budget policymakers to solicit and table more equitable fiscal expansion alternatives. Increased public consultation could include extending the pre-budget consultations with the public.
Moreover, civil society organisations like the Institute of Economic Justice and the Alternative Information and Development Centre (AIDC) have proposed alternative approaches to fiscal constraints that could ensure sufficient resources to protect our frail public health system from threats to resource availability. These alternatives should be explored.
One strategy proposed is strengthening the country’s capacity to halt the significant revenue losses owing to to corporate tax abuses, including illicit financial flows (IFF) and base erosion and profit shifting (BEPS). IFF refers to the cross-border movement of illegally sourced funds while BEPS refers to when multinational companies shift the profits generated in South Africa to another jurisdiction that has lower or zero tax rates in order to minimise their tax burden.
The Financial Intelligence Centre estimates that between $15 billion and $25 billion is shifted out of our country to tax havens yearly. We call for greater urgency towards implementing publicly disclosed beneficial ownership registries based on country-by-country reporting and the automatic exchange of information, strengthening capital and exchange controls, and increasing South African Revenues Services (SARS) capacity to investigate corporations suspected to be involved in IFF and BEPS. These essential measures can contribute to curbing profit shifting, resulting in more than R100 billion in revenue each year.
The upcoming MTBPS will find National Treasury in a challenging position where various trade-offs will likely be made. In this harsh economic climate, if something has to give, it cannot be the constitutional right to health care for all in this country.
*Lencoasa is a Budget Researcher at SECTION27 and Steering Committee Member of the Budget Justice Coalition. Brown is Director of the Alternative Information and Development Centre and member of the Budget Justice Coalition.
Over the last decade, the National Health Department has rolled out a range of electronic surveillance systems to monitor medicine stocks throughout the country’s healthcare facilities. Many healthcare workers feel the new systems are making a positive impact, but stockouts persist due to a host of ongoing supply challenges.
“My problem with the clinic is that I get there as early as 7am and leave around 3pm. I [went] to the clinic to collect my hypertension tablets. We get into a long queue only to be told that they don’t have hypertension tablets. Not having my tablets poses a danger to my life. I get dizzy and I am unable to work. I [asked] for the day off from work to come [that day], then [had] to ask for another day off to do the same thing,” says a Klerksdorp resident interviewed by the community healthcare monitoring group Ritshidze.
According to a recent report from Ritshidze, between May and June this year, there were over 400 unique medicine stockouts reported in just 72 healthcare facilities across the North West province. In roughly the same period, doctors in the Eastern Cape reportedly struggled to treat patients with bone marrow cancer due to province-wide shortages of crucial chemotherapy drugs. And in August, Africa’s largest hospital, Chris Hani Baragwanath, allegedly faced a stockout of adrenaline for two days.
Though the problem is not exclusive to South Africa, recent news about medicine stockouts paints a gloomy picture of the country’s capacity to manage essential medicines. But the National Health Department’s Khadija Jamaloodien says these reports shouldn’t overshadow a broader trend. Instead, she argues that the health department has made significant strides to improve medicines availability through a series of national drug stock surveillance programs. (You can see Jamaloodien’s full and very informative response here.)
But what are these systems, and are they as effective as the health department claims?
Health department ramps up surveillance
In November 2013 a nation-wide survey of hospitals and clinics conducted by the Stop Stockouts Project found that more than 1 in 5 had experienced stockouts of ARVs or TB drugs in the previous three months alone. The National Health Department appeared to have little understanding of the severity of the problem – in April, 2014 they claimed that in the last 12 months there had been only a few stockouts of ARVs, restricted to two provinces.
As media attention on shortages grew, the department began to prioritise the issue and developed an extensive surveillance system to better monitor medicine levels throughout the country’s public healthcare facilities. One key program is RxSolution, a computer-based stock management system that pharmacists and nurses use to record the quantities of drugs that have been ordered, received and dispensed at their facilities.
The software was rolled out incrementally at hospitals from 2014 and is now used in healthcare facilities across the country. The data feeds back to a series of national, provincial and district-level dashboards which show medicine levels across facilities.
The central software platform that hosts these dashboards is called the National Surveillance Centre. According to Jamaloodien the platform “allows stakeholders at national and provincial levels to quantify or predict challenges in medicine supply…”.
Additionally, RxSolution generates reports which advise hospital staff on how much of a particular drug they need to order to prevent shortages or overstocking, and which medicines are due to expire.
A similar online tool is the Stock Visibility System, which is used to measure medicine levels at primary healthcare facilities across the country. Unlike RxSolution, it’s accessed on a cell phone app and the data is stored in the cloud (RxSolution requires an in-house server). Healthcare workers scan medicines using the app to capture stocks.
By October, 2021 3826 healthcare facilities had used the Stock Visibility System, RxSolution or other online systems to track drug stocks (roughly 90% of all public hospitals and clinics according to our calculations).
SA better at managing ARVs – trends unclear for other drugs
Evidently, shortages remain, but according to Jamaloodien, these systems have made a positive impact: “Good surveillance systems are one factor in a multifactor situation but do play an important role in reducing stockouts. This can be seen in the downward trend of major stockouts since introducing the surveillance systems…”
Verifying this is difficult however as the health department wasn’t able to provide data over a long period, and independent research has historically focused only on TB drugs or ARVs. Shortages of the latter do appear to have become less common. In 2013, a national survey found that 19% of healthcare facilities had a stockout of ARVs in the past three months. By contrast, interviews that were done with healthcare workers this year suggest that, depending on the quarter, only 5% to 9% could recall shortages of HIV medicines in the past three months.
Whether the surveillance systems played any role in this decline, and whether the same trend holds for stockouts of other drugs, is unclear.
Healthcare workers say software reduces stockouts
A paper published in June assessed the attitudes of 114 users of the National Surveillance Centre. These individuals, mostly managers and pharmacists at different levels in provincial health systems, are responsible for monitoring drug stocks and reporting shortages. Two-thirds of them said the introduction of the National Surveillance Centre in 2016 had improved medicines availability, as having so much data on drug stocks allowed them to be more proactive – for instance by redistributing stocks from facilities that contained an excess of a particular medicine to those with shortages.
Prior to the rollout of this system, many of these individuals had monitored medicine stocks by physically going to facilities or waiting for healthcare workers to notify them of a stockout.
Another paper published in May found positive attitudes toward the Stock Visibility System among healthcare workers who used the system at clinics in Kwazulu-Natal (mostly nurses and pharmacists). Almost three-quarters of the 206 surveyed staff felt that the phone app had improved stock management at their facility, though it had reportedly increased their workload.
This lines up with a national survey in 2017 which found that 87% of healthcare staff reported that the Stock Visibility System had reduced the frequency of stockouts.
Mncengeli Sibanda, a pharmacy expert at Sefako Makgatho Health Sciences University, says the application has clear benefits: “In the past we’d have to count stocks physically and write it by hand, now it’s captured electronically, limiting capture errors and allowing stock counts to be done more regularly…And at a national level, they can intervene [to prevent shortages] because they have data on stock levels at [most] clinics”.
Loadshedding hinders rollout
RxSolution – which is PC-based – appears to have been similarly well-received among some healthcare workers. Phelelani Dludla, the acting clinical manager of Benedictine hospital in Nongoma in KwaZulu-Natal, says that when the system was introduced at Benedictine in 2019 “it would assist us in making orders before we ran out of stock”. He explains that: “it would tell us [which] stocks would run out and so we’d…reorder them a week earlier than our usual routine”.
Dludla adds that it also assisted in reducing waste: “it helped with finding out which drugs we should cut down on in terms of spending, because they were frequently expiring and being sent back”.
But particularly for rural hospitals like Benedictine, infrastructural problems can pose obstacles. Dludla says that since 2021, network problems caused by loadshedding have prevented the use of RxSolution throughout the hospital. Today, the software is only used in the pharmacy. Sibanda explains that “ideally RxSolutions should be [in each section of the hospital], but there have been challenges”. Aside from loadshedding “some hospitals can’t get a computer into each and every ward,” he says.
Monitoring suppliers
The National Health Department has also been monitoring drug suppliers. Jamaloodien says that companies that are awarded national tenders to provide medicines are “contractually bound to [provide] up-to-date production pipeline data for products that they supply. The mandatory six-month pipeline window allows for proactive prediction and management of looming supply challenges.”
Policies like this have good international precedent. Preliminary evidence found that Canada managed to reduce drug stockouts by forcing pharmaceutical companies to notify them of any supply interruptions. To work, they need to be implemented effectively however, and the National Health Department has previously complained that companies weren’t routinely notifying them of supply interruptions.
Yet if the health department has generally been making such positive strides toward reducing shortages, why are there still so many stockouts?
Global shortages
Part of the problem is international, says Andy Gray, a pharmacy expert at the University of KwaZulu-Natal: “globally, there is a problem with the security of supply in the pharmaceutical industry. For example there are a number of older cancer drugs that are out of stock in the US at the moment, and the UK has had persistent problems with antibiotics.”
Indeed, last week the European Union announced details of a “solidarity mechanism” in which member states who face drug shortages can now request donations from other European countries if they have exhausted all other options. This was after Europe faced repeated shortages of key medicines over its winter.
If a single factory runs into a problem, this can disrupt global supply, including in South Africa, where locally made drugs usually require active ingredients from abroad. Indeed, a 2020 paper found that pharmacists in Gauteng’s hospitals were often left waiting for medicine orders for months after the delivery deadline and many believed that this was due to contracted suppliers facing shortages of active pharmaceutical ingredients.
Local dynamics also play a role however. Problems have historically included the failure of provinces to pay contracted suppliers on time, staff shortages at clinics (which force overworked nurses to be in charge of stock management) and delays in the awarding of pharmaceutical tenders.
Split tenders to reduce vulnerability of supply
According to Gray, another issue is the overreliance on individual companies: “all too often the contract [to supply a particular drug] is awarded to a single supplier”. The conditions of pharmaceutical tenders often stipulate that if the company can’t meet its contractual obligations, the government can turn to alternative suppliers. But that’s easier said than done, says Gray: “If that single supplier is unable to meet demand…the alternative suppliers in the country simply don’t have the volumes to substitute…especially if there’s no prior warning that there is going to be a problem in supply”.
Jamaloodien argues that: “many contracts are currently awarded with…quantities split among suppliers”. However, doing so more frequently would present its own problems, as requiring several companies to produce small amounts of drugs “can invite higher prices because the price is largely related to economies of scale”. In other words, it’s cheaper for one company to supply all the drugs.
Gray acknowledges this but argues that the trade-off needs to be made more often in certain cases: “Vital medicines for which there are no alternatives are being given to maybe one or two suppliers”. The vulnerability this creates can come at enormous cost to patients.
He urges: “for vital medicines we need more split tenders”.
Disclosure: Spotlight editor Marcus Low was a member of the Stop Stockouts Project steering committee for several years in the mid-2010s. Also, Ritshidze is mentioned in this article. Spotlight is published by SECTION27 and the Treatment Action Campaign (TAC) and TAC is a Ritshidze member organisation. Spotlight is however editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council and subject to the Press Code.
The Government Employees Medical Scheme (GEMS) will, on November 2nd, 2023, host its 14th annual GEMS Symposium under the theme: “Advancing Health Equity by Addressing the Social Determinants of Health”. Experts, thought leaders and specialists in healthcare will engage in discussions towards a better understanding of the societal determinants of health in South Africa.
For this hybrid event, delegates will attend both in person at Sandton and virtually.
Dr Moloabi states that the “Symposium is an important event on the GEMS calendar, providing a platform for academic, clinical, government and business minds to discuss what social issues are at play in determining the nation’s health status and how to improvements in health equity can be realized”. Moreover, he also highlights the need to remove practical obstacles that make us an unequal society if we are to achieve collaborative and cohesive solutions to our healthcare challenges.”
Speakers will include:
Dr Ingrid Pooe – Chief Operations Officer, Government Employees Medical Scheme (GEMS),
Dr Sebayitseng Millicent Hlatshwayo – Chairperson, Government Employees Medical Scheme (GEMS),
Dr Chana Pilane-Majake – Deputy Minister of Public Service and Administration (DPSA),
Professor Mcebisi Ndletyana – Professor of Political Science, Department of Politics and International Relations, University of Johannesburg,
Dr Selaelo Mametja – Chief Research Officer, Government Employees Medical Scheme (GEMS),
Dr Vuyo Gqola – Chief Healthcare Officer, Government Employees Medical Scheme (GEMS),
Mr Louis Botha – Chief Executive Officer, Health Quality Assessment (HQA),
Ms Yoliswa Makhasi – Director General, Department of Public Service and Administration (DPSA),
Mr Frikkie de Bruin- General Secretary, Public Service Coordinating Bargaining Council (PSCBC),
Dr Pali Lehohla – Director of Economic Modelling Academy (EMA),
and
GEMS Principal Officer Dr Stanley Moloabi.
Dr Pilane-Majake, the Deputy Minister for the Department of Public Service and Administration (DPSA) will deliver the keynote address, elucidating, amongst other insights, the crucial relationship between the DPSA as employer and GEMS as an implementor of a mandate to ensure access to health and wellness by government employees and thus contributing towards the attainment of the ideals of Universal Healthcare Coverage.
Media personality Ms. Faith Mangope will facilitate conversations as the panel covers key discussion points, including:
Achieving the Sustainable Development Agenda 2030.
Beyond Healthcare: Addressing health equity and social determinants of health.
Policy Interventions for Addressing Social Determinants of Health: Lessons and best practices.
Value-Based Care and Social Determinants of Health: Integrating social context into healthcare delivery.
Advancing health equity by addressing social determinants of health; and
Exploring the interplay between healthcare quality and social determinants.
At GEMS, we are dedicated to fulfilling our responsibilities towards our members and the people of South Africa. The Symposium is a testament to our commitment to Universal Healthcare Coverage, and we are eagerly anticipating a productive outcome that will be memorable and provide an insightful experience for all involved, Dr. Moloabi” concludes.
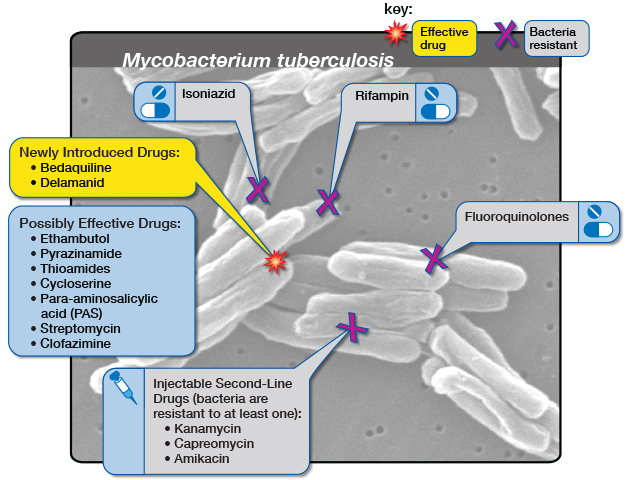
Diagram by the United States-based National Institute of Allergy and Infectious Diseases showing the medicine options for drug-resistant tuberculosis. (Via Flickr, CC BY 2.0 Deed)
The South African government and pharmaceutical company Johnson & Johnson (J&J) have agreed to a lower price for bedaquiline, a medicine used to treat drug-resistant tuberculosis (DR-TB) in South Africa.
This comes off the back of mounting pressure from activists and amid an ongoing investigation by the Competition Commission, looking into J&J’s pricing of the drug.
An estimated 14 000 people in South Africa fell ill with DR-TB in 2019. Bedaquiline is one of the main drugs used to treat DR-TB. Before bedaquiline became available, treatment for DR-TB would consist of up to two years of injections with serious side effects. The bedaquiline-containing regimen has no injectables, far fewer side effects and is typically six months.
Bedaquiline has been provided by the South African government since 2018.
In July, J&J agreed to sell bedaquiline to lower and middle-income countries through the Stop TB Partnership’s Global Drug Facility for $130 (R2470) per six-month regime, but South Africa does not make use of this facility due to national procurement policies.
Instead, about the same time that J&J made this announcement, the National Health Department agreed to pay J&J R5500 for the drug.
The Competition Commission announced in September that it will be investigating Johnson & Johnson’s pricing of the drug. The commission assisted the Department of Health in renegotiating the price, says department spokesperson Foster Mohale.
This week the department sent out a circular indicating that it will be paying R3,148 for bedaquiline.
Bedaquiline is prescribed to 7000 to 8000 people a year, Mohale told GroundUp. Mohale says the new price amounts to a 40% saving on bedaquiline for the next two years.
Candice Sehoma, Access Campaign Advocacy Advisor for Medicines Sans Frontiere (MSF), told GroundUp that the “momentous” cost saving is a “big achievement”. Sehoma says it is a sign that the global campaign to ensure accessible and affordable treatment for TB is yielding results.
MSF has estimated that bedaquiline could be manufactured and sold for profit for as little as $102 (R1940).
Fatima Hassan, director of the Health Justice Initiative, says that while the price drop is a victory, it is important to ensure that this does not happen again.
“The significant price reduction emphasises why price scrutiny is significant,” Hassan told GroundUp.
Alleged “evergreening”
J&J’s patent for bedaquiline expired in July 2023, but J&J had already applied for a new patent for a slightly different version of bedaquiline, which was granted. This meant their patent protection continued in South Africa after the original patent expired.
This amounts to “evergreening”, says Hassan. Evergreening, as explained in this article in The Conversation, “is achieved by seeking extra patents on variations of the original drug – new forms of release, new dosages, new combinations or variations, or new forms”.
The Competition Commission will be looking into J&J’s alleged “evergreening” as part of its investigation.
After making its agreement with the Global Drug Facility, J&J has announced it will not be enforcing the new patent – a move that will allow generic versions of the product to enter the market and further lower the price.
GroundUp sent questions to J&J but received no response.
In a nation where healthcare has been marred by disjointed systems and fragmented care, South Africa’s healthcare organisations are making strides to change this narrative.
South Africa’s health journey has faced challenges with siloed information, often paper-based systems, and a lack of information flow between health professionals, funders and health facilities. These barriers have significantly impacted the cost, quality, and access to healthcare for patients. In response, the Competition Commission’s Health Market Inquiry (HMI) panel spotlighted the urgent need for solutions that bolster transparency, coordination, and innovation.
South Africa’s first industry-wide health information exchange, CareConnect HIE, is a game-changing initiative and the brainchild of major hospital groups, including Life Healthcare, Mediclinic, and Netcare, coupled with leading medical scheme administrators like Discovery Health, Medscheme, and Momentum Health. Their shared vision? An interoperable health system that breaks historic barriers, promoting enhanced patient care, quality, and efficiency. This transformative approach to healthcare was showcased in action at an event in Sandton today, providing attendees a firsthand look at the potential of HIE in South Africa.
Since its launch in August 2022, CareConnect HIE has rapidly advanced, with over 5.2 million consented lives now integrated into the system. However, the true value – from population health benefits to progressive funding and health delivery models – exponentially increases as the amount of data on the exchange grows. Therefore, the aim of the HIE is to be the hub of exchange and the single integration point for ALL health data – from both the public sector and the private sector. Bearing testament to this, representatives from the South African Private Practitioners Forum, the Radiological Society of SA, Mediclinic, Discovery Health, Altron and Momentum Health will share their insights on how HIE will be used in their organisations. In addition, representatives from the Western Cape Department of Health will talk to the public-private collaboration with CareConnect.
CareConnect has adopted a set of international standards (FHIR and HL7) to transfer and share data between various healthcare systems regardless of how it is stored in those systems. These standards underpin interoperability because all participants are ‘speaking the same language’. An interoperable health system will be critical in achieving Universal Health Coverage (UHC) which will require the ability for patients to move seamlessly between the public and private health sectors, facilities, clinicians or other service providers, depending on the expertise and care they require. To this end, there is engagement with the National Department of Health, who were represented at the event.
Dr Rolan Christian, CEO of CareConnect HIE
Central to the CareConnect HIE is a Unified Care Record (UCR), an electronic medical record that holds a patient’s entire medical journey. This constantly updated and ever-evolving record gives clinicians on-demand access to consolidated patient data, promoting swift, well-informed treatment decisions when and where they are needed.
Privacy and security of data is critical to the success of HIE. The CareConnect HIE conforms to both local and international data privacy regulations to ensure that sensitive health information remains protected at all times and will only be accessible to healthcare providers when medically necessary and only with the patient’s consent. User-based access permissions are automatically regulated by the HIE, further safeguarding sensitive patient information.
Sharing health data saves lives. The more data the industry shares, the more value and benefit to the patient that will be extracted from the HIE.
Dr Rolan Christian, CEO of CareConnect HIE
CareConnect’s innovative new use cases, ranging from tracking acute and chronic patient conditions, listing allergies and adverse reactions, to standardising doctor clinical (discharge) summaries, were demonstrated at the event. These features will enable better coordination of care, minimise medical errors and pave the way to a more cohesive health system.
HIE in various forms has become common across many health systems in the world and has become a priority on many a government health policy agenda as a solution to achieving greater cohesion within health systems and as a mechanism to address cost and quality issues in health. Reflecting global best practices, the CareConnect HIE aligns with the world’s most mature HIEs and breathes life into the National Department of Health’s National Health Digital Strategy for South Africa. This important document outlines the country’s goals towards the development of electronic health records and building interoperability and linkages between existing patient-based information systems.
A strict code of ethics relating the use of information is governed by an internationally recognised and best practice multi-party trust agreement, called DURSA. The DURSA provides a framework that deals with sharing of data among HIE participants and defines the permitted purpose for which the data can only be used.
Dr Rolan Christian, CEO of CareConnect HIE shared: “Sharing health data saves lives. The more data the industry shares, the more value and benefit to the patient that will be extracted from the HIE. We envision that CareConnect HIE will become a ‘utility’ for the entire health sector – to enable improved quality of care, better health outcomes and a more responsive health system.”
The event today boasted a stellar lineup of speakers. Notably, Dr Stavros Nicolaou from B4SA and Aspen Pharmacare and Dominick Bizzarro, offering international perspectives from MVP Health Care, joined other industry luminaries. Their combined insights painted a promising future for healthcare – one that’s harmonised, transparent, and unequivocally cantered on the patient.
Dr Nicoline Potgieter at the Paediatric and Special Needs Dental Care Unit
The landscape of paediatric dental care in South Africa is poised for a significant transformation, marked by the launch of the nation’s first specialised Paediatric and Special Needs Dental Care Unit. This pioneering initiative, a result of the dedicated efforts of the Department of Paediatric Dentistry of the University of the Western Cape (UWC), The Provincial Government of the Western Cape (PGWC) and Rotary Club, is set to revolutionise Paediatric Dentistry in South Africa. It promises enhanced efficiency, a reduction in anxiety for young patients and a sharpened focus on providing dedicated oral health services to children and especially children with special health care needs.
Working towards the acknowledgment of Paediatric Dentistry as a specialty in South Africa, the need for a dedicated, specialised, child-friendly facility was identified – particularly in the Western Cape. This project stands as a steadfast response to establish such a paediatric dental unit, promising to positively impact service delivery to the children of the Western Cape.
Dalene Swart, President of the Rotary Club of Bellville, is passionate about this transformative initiative. She underscores the present scenario wherein young patients often undergo dental procedures under general anaesthesia.
“The establishment of a dedicated paediatric dentistry surgery unit, equipped with the latest materials and state-of-the-art equipment, not only enhances service quality but also serves as an invaluable training ground for postgraduate students,” she says.
However, the impact transcends mere smiles; it represents a pivotal advancement in South African healthcare, focused on the oral health of children. This project is expected to increase treatment capacity in the field of Paediatric Dentistry, thereby alleviating the workload of local healthcare professionals. It will also foster disease prevention and treatment programmes, bolster healthcare systems, and in time, significantly reduce the burden of disease and need for care under general anaesthesia.
Dr Nicoline Potgieter, president of the South African Association of Paediatric Dentistry and course coordinator for the Masters programme in Paediatric Dentistry at UWC, emphasises the enduring plight of the children in South Africa, who are in dire need of expert oral health care. “It is important to note, oral health directly impacts general health which directly impacts quality of life. It is our responsibility to provide the basic health care needs of our children. The technological advances incorporated into the unit, support minimally invasive techniques and preventative dentistry and the environment is focused on making the dental visit more pleasant for the child patient. Hopefully this is the first of many dedicated paediatric and special needs units across South Africa!”
This project, scheduled for full implementation by the end of October 2023, is the outcome of a collaboration between dedicated Rotary Club participants and the Tygerberg Oral Health Centre, which is a joint platform between UWC and PGWC. It seamlessly aligns with the UWC mission to train paediatric dentists as specialists in South Africa, reaffirming the institution’s commitment to community health and well-being. Similarly, it aligns with PGWC that is dedicated to high quality service rendering to all patients. Under this initiative, the first paediatric dentists will receive specialised training each year, while hundreds of children will benefit from disease prevention and interventions.
The project, funded with a capital expenditure of R1.2 million, draws support from various sources, including cash contributions from the Rotary Club of Bellville, Rotary Foundation and six other Rotary Clubs from the UK, USA and Canada. A significant portion of the funds raised was allocated to state-of-the-art essential dental equipment, consumables, and building materials.
Swart concludes by underlining that this project transcends immediate community needs for specialised paediatric dental care; it is about advancing medical care in South Africa and laying the groundwork for the long-term sustainability and transformation of dental care needs. This is why it enjoys unwavering support from local Rotarians.
Dr Bukiwe Spondo recently received the Rural Doctor of the Year award at the Rural Health Conference held in Chintsa in the Eastern Cape. PHOTO: Supplied
By Biénne Huisman for Spotlight
Describing the rutted gravel road between Butterworth and Tafalofefe District Hospital in the Eastern Cape, Dr Bukiwe Spondo uses the word “terrible” at least eighteen times. Dipping through the Amatole District, the 55-kilometre journey can take several hours. With heavy rain, tractors may be required to dislodge ambulances and often even staff have difficulty getting to work because of the mud.
Since 2007, Spondo and her colleagues have offered a multitude of services at Tafalofefe in the lush but impoverished Centane village. First off, she moved the hospital’s ARV clinic from an out-building to inside the premises – reducing stigma – “because if patients went into that building on the outside, automatically everyone knew,” she says.
In 2012, having observed how patients stopped taking treatment due to travel costs, she started driving up to 40 kilometres a day twice weekly to nine clinics in the area, where up to fifty patients would be queuing to see her. To make life easier for patients, she started pre-packing medication to take to them at the clinics. Later she opened a CHAMP (Clinical HIV /AIDS Management Programme) site at Tafalofefe to see complicated cases referred from the clinics, and a multi-drug-resistant TB (MDR-TB) review clinic in conjunction with Butterworth Provincial Hospital.
“As a rural doctor, you become a social worker, a pharmacist, a priest – you do everything,” she says, laughing.
Rural doctor of the year
Spondo’s efforts have not gone unnoticed. Last month at the Rural Doctor’s Association of South Africa (RuDASA’s) annual Rural Health Conference, she received the Rural Doctor of the Year award. RuDASA chairperson Dr Lungile Hobe conferred the award at the event hosted near Chintsa. Spondo is quick to point out that she also won an Amatole District leadership award last year.
Speaking to Spotlight over Zoom, she says, “So the roads here at Centane are terrible. It becomes a challenge to get ambulances through and the chopper cannot fly either when it’s raining. I mean, the other day a truck was stuck, crossing the road so the ambulance couldn’t pass. We had to take a private car from the hospital to go meet the ambulance halfway.”
She adds that the community hoped that roads would be improved after a devastating accident five kilometres from Tafalofefe in 2020 when an overloaded 65-seater bus plunged into a gorge, causing 25 deaths and 62 injuries. But, she says, the improvements never come.
At Tafalofefe, the two nearest referral hospitals are Cecilia Makiwane and Frere Provincial in East London, situated an additional 110 kilometres or 90-minute drive from Butterworth along the N2 highway. Housed in a pale building, Tafalofefe has 160 beds served by 41 professional nurses and seven doctors – including three community service doctors who joined last year. The additions have increased capacity, for example, emergency caesareans are now available around the clock.
Taking healthcare to the people
The hospital has three 4×4 bakkies [pick-ups] for visiting or transporting patients. It is in one of these that Spondo travels to see patients in remote corners between the Kobonqaba and Kei Rivers on Tuesdays and Thursdays.
“Clinics are part of decentralised primary healthcare goals,” she says. “But the problem was that if there were complicated cases – like if a patient is taking ARVs and then develop side effects, the sisters are not equipped to handle that. For example, if there is a kidney problem, they [cannot] do anything about that.
“And in time, I realised that for these people traveling to the hospital costs too much money. Let’s say, for example, the clinic at Qolora – for a person to travel from Qolora to Tafalofefe is R100. A return ticket is R200. And you know, most people here are unemployed. They can’t afford this. By the time they have saved up enough money to travel to the hospital, it’s too late. Like it would be the end stage of their kidney problem. You could not send this patient for dialysis, nothing could be done to help them. This is why I started my outreach trips.”
In motivating for Spondo to receive the RuDASA award, Tafalofefe’s CEO Masizakhe Madlebe pointed out how her work days start at 7am, only finishing once all patients had been seen, whether at the hospital or at one of the local clinics. In addition, he notes how, over the years, Spondo has mentored youth in the area, including children whose parents had succumbed to AIDS, and school girls on topics like life goals and contraceptives. He adds that Spondo even reached into her own pocket to pay school fees for children without parents.
Spondo relays how she noticed girls as young as twelve years old in their maternity ward, giving birth. “Myself and some nurses we went to two schools in the area to educate them, to discuss goals and contraceptives,” she says. “We started with grade 12 pupils. No teachers were present. It was just us and them. And I was surprised at how free they were talking. I said to them education is more important. I said to them – You see me? I am a doctor. One day you can be a doctor too, but you need to be educated. I told them they could come to Tafalofefe any time if they needed to talk, that I could help them apply for tertiary degrees, to college or to university.”
Spondo has kept a close eye on children orphaned by AIDS in the area. “I tell them to bring me their June, September, and December school reports, so I can see how they’re doing, so I can motivate them,” she says.
“These kids, I’ve seen them grow up. Some of them I saw angry – with everyone, with their own deceased parents. And I explained to them, don’t be angry. It’s not your mother’s fault. It’s not your father’s fault. It was the government’s fault for not giving your parents access to ARVs. But now, take your own ARVs and you will be fine. Some of them have passed high school with distinction, some even now have access to universities.”
Bringing her skills back home
Alongside two brothers whom she describes as “wonderful”, Spondo grew up in the village of Nqamakwe, on the opposite side of Butterworth. Her parents have passed away, but she still considers Nqamakwe her home. Here her family’s farming interests include cattle, goats, and sheep.
She attended Blythswood Secondary School in Nqamakwe – excelling at biology and physics, even though maths was hard work. “Becoming a doctor was just something I always wanted,” she says, relaying how in her formative years she had been a sickly child who often required medical care. This changed, she says, as she cannot remember ever being sick as an adult.
Spondo graduated from medical school at the University of KwaZulu-Natal in 2002, completing her internship at Cecilia Makiwane and her community service at Tafalofefe and Frere in 2004.
Speaking with rapid enthusiasm, she says how happy she is to bring her healthcare skills back home to serve the community that shaped her own humanity.
“I mean, I know these people inside out. I was born in front of them, raised in front of them,” she says. “These are our relatives, our aunts, our grannies. It’s giving back to them, to the community that raised you, that has done everything for you. Who supported you through all these years.”
She adds that Tafalofefe’s clinical manager, Sambona Ntamo, grew up near Butterworth too.
“Who would look after these people if we didn’t?” she asks.
Where does she find the resilience that drives her passion to care for sick people, often queuing at the end of long rutted roads?
“Lots of exercise,” she says, smiling.
At Tafalofefe there is a staff gym with a treadmill, a bicycle, weight lifts, and pilates balls.
“I tell the guys after work it’s gym time, it’s gym time, it’s gym time!” she says. “We’ve got a key and everyone knows that even if they want to go to the gym after midnight, they may get the key and go.”
Photographs capture an air of camaraderie at Tafalofefe. Staff sharing a meal of tripe and creamed spinach on heritage day, a farewell gathering for a retiring nurse with balloons and huge gifts in silver wrapping, [and] women knitting countless bright beanies for babies delivered in the maternity ward. A picture inside the hospital’s paediatric room shows youngsters on plastic motorbikes and mothers holding toddlers wrapped in blankets.
Spondo and her own eight-year-old son, Lutho desperately – which means the greatest one – live in a doctor’s house on the hospital’s premises. They travel to their family home in Nqamakwe over weekends.
For Spondo, being a doctor does not feel like a job. “When you do something you love, it doesn’t feel like a job,” she says. “Being a doctor is something I look forward to every morning. When patients return to me, saying they feel better with a smile on their faces, saying thank you for the treatment – that just makes my day.”











{kind=link}