The South African Health Products Regulatory Authority (SAHPRA) confirms that it has granted Section 21 authorisation for the importation of the Dollvet Foot and Mouth Disease (FMD) vaccine with conditions and is currently assessing an additional application for the same vaccine.
Foot and Mouth Disease is a highly contagious viral disease affecting cloven-hoofed animals such as cattle, pigs, sheep, and goats. It causes fever and painful blister-like sores in the mouth, on the teats, and between the hooves. While many animals recover, outbreaks can result in severe production losses, high mortality in young animals, and significant economic consequences for the agricultural sector.
Speaking on the authorisation, Dr Boitumelo Semete-Makokotlela, Chief Executive Officer of SAHPRA, said:
“The health of our livestock is critical to South Africa’s food security, economic stability, and the livelihoods of our farmers. By granting Section 21 authorisation for the importation of FMD vaccines, SAHPRA is ensuring that veterinarians and farmers have timely access to safe, effective, and scientifically approved tools to protect animals against this highly contagious and devastating disease”.
Section 21 of the Medicines and Related Substances Act provides a mechanism for the controlled importation of medicines and vaccines not yet registered in South Africa, under strict regulatory oversight. This pathway enables SAHPRA to respond rapidly to urgent public and animal health outbreaks while maintaining rigorous standards of quality, safety, and efficacy. Authorisations granted under this provision are temporary and subject to ongoing review.
All imported vaccines undergo strict regulatory controls and quality assurance processes. Distribution will be coordinated by the Department of Agriculture: Animal Health, which is responsible for implementing national disease control measures.
FMD spreads rapidly through direct contact with infected animals, contaminated equipment, vehicles, clothing, feed, and even via wildlife carriers. Outbreaks can lead to movement restrictions, quarantines, trade limitations, and increased compliance costs for farmers. Loss of South Africa’s FMD-free status can trigger immediate export bans on livestock and related products, affecting foreign revenue losses and market stability.
The Department of Agriculture has emphasised that FMD is a controlled disease and that vaccination must take place only within officially approved programmes. Unregulated vaccination may mask infections, weaken surveillance systems, and delay the country’s ability to regain its FMD-free status under international standards set by the World Organisation for Animal Health (WOAH).
“Our collaboration with SAHPRA reflects the importance of partnerships in safeguarding animal health. The South Africans farming community can be assured that every vaccine authorised for use in the country undergoes careful evaluation for safety, efficacy, especially against locally circulating strains and quality and we are optimistic that the disease will be contained” said Dr Bothle Modisane, Chief Director for Animal Health at the National Department of Agriculture.
SAHPRA remains committed to transparency and will continue to update stakeholders on developments related to veterinary vaccine import authorisations for FMD control.
Pretoria, 8 January 2026 – The South African Health Products Regulatory Authority (SAHPRA) has been made aware of products in the market containing Zinc picolinate (as a source material for zinc) and/or Selenium intended for use in children.
The safety concerns related to children are as follows:
Zinc picolinate, at any supplemental dose, can cause side effects which include indigestion, diarrhoea, headache, nausea, and vomiting. As the bio-availability of Zn from Zn-picolinate is variable due to multiple factors, the risk of side effects may be higher and unpredictable, and it is unsuitable as a source of elemental zinc supplementation in children; and
Selenium, when supplemented to children, represents a safety concern considering the potential differences in selenium daily intake between different population groups. While selenium intake is a viable requirement for children in areas of famine or dietary restriction, the potential adverse effects of selenium overdose are of concern when provided in general supplements/medicines intended for children.
The products currently on the market are marketed and sold, among others, as “Immune boosters” for children, with the main active ingredients being Zinc (when derived from Zinc picolinate) and/or Selenium intended for use in children. These products are indicated for supporting the treatment of colds, flu, diarrhoea, and skin-related conditions, rendering the products in question medicines that require registration by SAHPRA.
Any medicine sold that contains Zinc picolinate or Selenium intended for use in children does not qualify as a Category D (complementary) medicine. As such, their sale as a Category D medicine is illegal. Therefore, with effect from the date of publication of this notice, all selenium and zinc picolinate-containing products intended for use in children shall be subject to registration as a medicine falling into Category A, as defined in Section 14(2) of the Medicines and Related Substances Act, 101 of 1965, and need to be submitted to SAHPRA for registration. The sale of Category D (complementary) medicines containing Zinc picolinate or Selenium and intended for use in children must be withdrawn from the market within six (6) months of the date of this publication.
Advice for health professionals and distributors:
SAHPRA requests that Health professionals cease all distribution, selling, and/or dispensing and remove all selenium and zinc picolinate-containing products intended for use in children from stores, storage facilities, and shelves.
Members of the public are urged to return products containing Zinc Picolinate and Selenium when intended for use in children, to their pharmacist, supplying warehouse, or distributor.
Reporting side effects
Public and healthcare professionals are encouraged to report any side effects after using a health product by using the Med Safety App. Your report will contribute to our monitoring of these health products.
The South African Health Products Regulatory Authority (SAHPRA) has officially been accepted as a member of the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH), following an ICH assessment of compliance with requirements for membership, including a formal presentation outlining SAHPRA’s interest, progress, and milestones in implementing ICH principles.
The ICH is a unique global body that brings together regulatory authorities and the pharmaceutical industry to align scientific and technical standards for the registration of medicines. Since its establishment in 1990, it has evolved to support an increasingly globalised pharmaceutical environment. Its mission is to promote worldwide harmonisation to ensure that safe, effective, and high-quality medicines are developed and registered efficiently. This harmonisation is achieved through the development of ICH Guidelines, which are formulated through scientific consensus between regulators and industry experts. Successful adoption relies heavily on regulators’ commitment to implement these final Guidelines within their national systems.
The ICH Assembly met in person on 18-19 November 2025 in Singapore, in parallel with meetings of 12 Working Groups and preceded by meetings of the ICH Management Committee (MC) and the MedDRA Steering Committee (SC).
“ICH is delighted to welcome NAFDAC, Nigeria, and SAHPRA, South Africa, as new ICH Members, in addition to two new Observers: DIGEMAPS, Dominican Republic, and Philippine FDA, Philippines, bringing ICH to a total of 25 Members and 41 Observers.”
Welcoming SAHPRA’s membership, CEO Dr Boitumelo Semete-Makokotlela said: “This is a significant milestone for the South African Health Products Regulatory Authority. Membership of the ICH strengthens our commitment to the three pillars of safety, quality, and efficacy, while ensuring that our processes remain resource-efficient. This development allows SAHPRA to benchmark its regulatory practices against global best practice for the benefit of all people living in South Africa.”
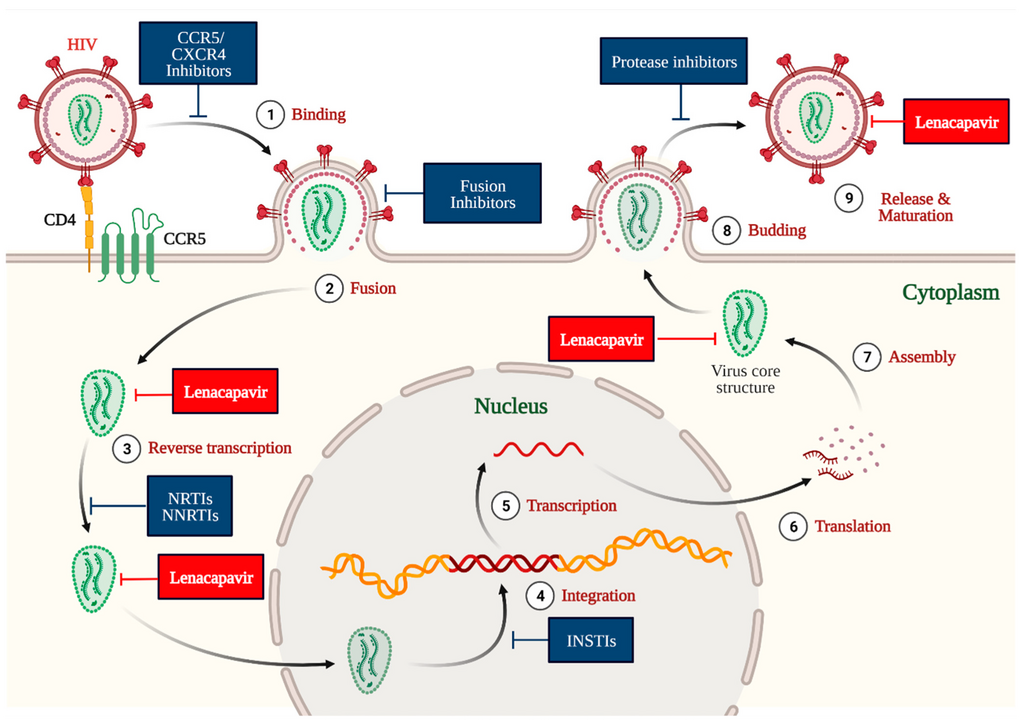
Pretoria, 27 October 2025 – The South African Health Products Regulatory Authority (SAHPRA) is pleased to announce the registration of Lenacapavir. Lenacapavir is an antiviral medicine that is recommended, in combination with safer sex practices, for pre-exposure prophylaxis (PrEP) to prevent HIV-1 infection in adults and adolescents weighing at least 35kg.
An application by Gilead was submitted to SAHPRA in March 2025. The SAHPRA review process was done in collaboration with the European Medicines for All Procedure (EU-M4all). This procedure enables the European Medicines Agency (EMA), together with the participating regulatory authorities, to provide scientific opinions on high-priority medicines, such as Lenacapavir, intended for markets outside the European Union. The benefits of this pathway are to strengthen regulatory systems and accelerate access to essential medicines.
This product, developed to prevent new HIV infections, is a six-monthly injection. There is an initiation dose of a subcutaneous injection (administered just under the skin) with tablets (taken on days 1 and 2). It is used to reduce the risk of HIV in adults and adolescents who weigh at least 35kg, are HIV negative, and are at risk of getting HIV. Lenacapavir for PrEP should always be used in combination with safer sex practices, such as using condoms, to reduce the risk of getting other sexually transmitted infections.
“The registration of Lenacapavir is a game-changer, given the high prevalence rate of HIV in South Africa. This product is the most effective HIV prevention measure thus far,” indicated Dr Boitumelo Semete-Makokotlela, CEO: SAHPRA.
Pretoria, 28 September 2025 – The South African Health Products Regulatory Authority (SAHPRA) wishes to reassure the public that paracetamol remains a safe and recommended option for the relief of pain and fever during pregnancy, when used short-term at recommended doses.
Paracetamol is one of the most widely used medicines globally and has been extensively studied for decades. There is currently no scientific evidence that using paracetamol in pregnancy causes attention-deficit hyperactivity disorder (ADHD) and autism.
SAHPRA will continue to monitor emerging evidence on the safety of paracetamol.
Advice for healthcare professionals
Paracetamol remains a recommended safe treatment for pain or fever in pregnant women. Pregnant women should be reassured that there is no evidence that taking paracetamol during pregnancy causes autism or ADHD in children. Healthcare professionals are encouraged to provide counselling to patients about the side effects of paracetamol, as detailed in the product’s professional information and patient information leaflet (https://pi-pil-repository.sahpra.org.za/).
Advice for healthcare professionals to provide to patients
Pregnant women and those planning a pregnancy should be advised to use paracetamol only when needed and at the lowest effective dose for the shortest possible time. Untreated fever and pain may pose risks to the unborn baby, and it is therefore important to seek treatment if recommended by a healthcare professional. Pregnant women should consult a healthcare professional if pain or fever persists or if they have any concerns about medicine use during pregnancy. Pregnant women should also be advised to avoid combining paracetamol with other medicines without first seeking medical advice.
Report any suspected adverse drug reactions
Healthcare professionals and members of the public are urged to report any suspected adverse drug reactions (ADRs) related to the use of paracetamol and other health products to SAHPRA via the eReporting link available on the SAHPRA website (www.sahpra.org.za) or complete an ADR reporting form accessible via the SAHPRA website and email it to adr@sahpa.org.za. Alternatively, reporting can be done via the Med Safety App, downloadable through Google Play or the Apple App Store.
SAHPRA remains committed to ensuring the safety of medicines available in South Africa and will update the public if new scientific evidence changes current recommendations.
Most medical devices are used in healthcare settings but some like bandages, thermometers, condoms, and blood pressure monitors are used at home. Photo by Mockup Graphics on Unsplash
By Catherine Tomlinson
Unlike with medicines, and with a few exceptions, South Africa’s regulator does not assess whether diagnostic tests and other medical devices on the market are safe and work as they are supposed to. The regulator has however started down a road that should eventually lead to the regulation of all medical devices in the country.
From scalpels to surgical robots, finger-prick diagnostic tests to MRIs, thermometers to wearable AI-powered health monitoring devices, bandages to prosthetics: the range of products classified as medical devices is vast.
Some medical devices are used briefly and then disposed of after a single use, while others are designed to stay in our bodies for long periods of time, such as implants to prevent pregnancy and pacemakers to help the heart beat regularly.
While most medical devices are used in medical settings, some, like bandages, thermometers, condoms, and blood pressure monitoring devices, are used at home.
The World Health Organization estimates that there are more than two million different types of medical devices used around the world. Given the enormous diversity of medical devices, it can be tricky to see what links all these products together.
One answer, and essentially the one used in South African law, is that it is the intended use of the device. A medical device is thus simply any device that is intended to be used to prevent, diagnose, monitor, or treat a disease, injury, or other medical condition.
Because medical devices are sold for medical purposes, they require regulatory oversight to ensure that they are safe to use and work as intended. But in South Africa, this regulatory oversight is not yet fully in place, and you can’t always trust that devices do what they claim to do, or that tests are accurate.
‘Inaccurate readings’
On a recent webinar hosted by FIND, an international non-profit engaged in the development of diagnostics for low resource settings, the chairperson of NGO SA Diabetes Advocacy, Kirsten de Klerk, told participants that “a lot of people assume that if a medical device is available for purchase, it has been correctly tested and approved for use” but “unfortunately, that’s not the case”.
De Klerk added: “I have unfortunately had community members sharing stories of life-threatening situations because of inaccurate readings” from continuous glucose monitors (CGMs). These are medical devices used by people with diabetes to monitor their blood sugar level.
To address the challenge of poor-quality CGMs on the market, South African diabetes advocates and FIND launched a tool to assist people with diabetes and healthcare providers to identify and use monitors that have been properly assessed for safety and functioning.
But what role does the South African Health Products Regulatory Authority (SAHPRA) play in ensuring the safety and effectiveness of medical devices used in the country, and what steps is it taking to better protect the public?
A mandate to regulate
Though medical devices aren’t yet registered, SAHPRA does have a legal mandate to regulate medical devices. The relevant legal requirements were introduced in the 2015 Medicines and Related Substances Amendment Act 14. Before the 2015 Amendment Act came into force in 2017, only electromagnetic or radiation-emitting medical devices were regulated in South Africa.
The 2015 amendments provided for the establishment of SAHPRA to replace the Medicines Control Council as the country’s health products regulator and expanded SAHPRA’s regulatory scope to cover all medical devices.
SAHPRA’s first big move towards regulating the medical device industry was to introduce requirements for medical device companies to be licensed as medical device establishments. Medical device companies were informed that they would need a medical device establishment license to operate in the country in a government gazette notice issued in 2017. (Manufacturers of the lowest risk products – Class A medical devices that don’t have a measuring function and/or are not required to be sterile – are currently exempt from the licensing requirements.)
Today, over 2 500 companies hold active medical devices establishment licenses from SAHPRA. In their applications for these licenses, companies must list the medical devices that they will manufacture, import, or wholesale in South Africa and the establishment licenses that they are granted are specific to the class of products that they are manufacturing or handling.
Medical devices are classed in four groups from lowest to highest risk products, based on the risk posed by the product to patients and the broader public health. Bandages for example are classed as low risk, while heart valves are classed as high risk. Using a risk-based approach allows SAHPRA to harmonise how medical devices are regulated in South Africa with international norms and will allow the regulator to prioritise review of high-risk products as it phases in requirements for registration of medical devices used in the country.
In addition to listing the devices that they manufacture, distribute, or wholesale, companies seeking medical device establishment licenses from SAHPRA are also required to provide a declaration regarding the quality management systems that they have in place.
Critically, however, the devices themselves are not yet being assessed by SAHPRA.
Dr Dimakatso Mathibe, senior manager of SAHPRA’s medical device unit, told Spotlight that more than 200 000 different medical devices are used in South Africa. While over two thousand companies hold active medical device establishment licenses, she explained that a single company may be importing over a hundred products. She noted that as SAHPRA has increased the regulatory requirements for operating in South Africa, some medical device companies have voluntarily withdrawn from the market.
ISO 13485 certification
SAHPRA’s second big move, which is now being rolled out, is the introduction of requirements for medical device companies to gain ISO 13485 certification verifying that they meet international quality management standards.
Medical device companies operating in South Africa can receive certification that they meet ISO 13485 standards from an international or local conformity assessment body that has been accredited to provide this certification.
When SAHPRA first introduced medical device establishment licenses, it did not require companies to have ISO 13485 certification, as it was concerned that enforcing this too quickly could disrupt access to medical devices in the country. This was in part due to the lack of local conformity assessment bodies accredited by the South African National Accreditation System (SANAS) to grant this certification at the time.
John Ndalamo, accreditation manager for SANAS’ certification programme, told Spotlight that six local conformity assessment bodies have now been accredited to provide ISO 13485 certification.
SAHPRA now requires that companies renewing their five-year medical device establishment licenses provide either proof of ISO 13485 certification or evidence that the company has begun the process of seeking this certification.
What about regulation of the actual devices?
While important strides have been made by SAHPRA toward regulating the medical device industry, medical devices themselves still remain mostly unregulated in South Africa.
What this means is that, as pointed out by SA Diabetes Advocacy, medical devices may currently be marketed in the country without an independent regulator confirming that they are safe to use and perform as advertised.
The registration of the over 200 000 medical devices in use in the country is a mammoth job. Mathibe said that when SAHPRA introduces requirements for the registration of medical devices, it will do so in a phased and transitional manner. She explained that the call-up of medical devices for registration will likely be phased by product risk classes and conditions. Presumably, SAHPRA will start with the highest risk products and work down from there.
Assessing feasibility
SAHPRA is conducting a feasibility study of its intended approach to register medical devices. Companies holding medical device establishment licenses have been asked to voluntarily participate in the study.
In documentation published for the feasibility study, SAHPRA indicated it plans to include 32 medical devices used for HIV and TB in the study. These will cover in vitro diagnostic tests, condoms, and X-ray devices used for TB screening.
SAHPRA also aims for half of the products included in the study to be manufactured locally and the other half to be imported. In doing so, SAHPRA can use the study to test its approach for registering products that are evaluated locally, as well as products assessed in other countries with which it has a regulatory reliance mechanism in place (meaning it can rely on regulatory evaluations performed in these countries).
How will safety and performance be assessed in the feasibility study?
Mathibe said that SAHPRA will not directly assess the safety and performance of medical devices in the feasibility study. Instead, this will be done by accredited conformity assessment bodies, which is the same approach used by regulators in Europe. The assessment made by the conformity assessment bodies will then be used by SAHPRA in determining whether a product should be approved for use in the country.
For medical devices already registered in jurisdictions with which SAHPRA has a reliance mechanism in place, like the European Union, Australia, and Japan, companies can submit evidence of such conformity assessments and marketing approval. SAHPRA can then use this information to help make its own registration decisions.
Devices that are not approved by a regulatory authority recognised by SAHPRA, must undergo a safety and performance assessment by a locally accredited conformity assessment body.
Mathibile said insights from the study will be shared with stakeholders next year, and the lessons will help inform how SAHPRA introduces medical device registration in South Africa.
Emergency authorisation of COVID-19 and Mpox medical devices
While SAHPRA has not yet registered medical devices, it introduced rules in 2020 for emergency authorisation listings for certain medical devices used for COVID-19 in South Africa, and it announced in 2024 that diagnostic tests for Mpox required approval from SAHPRA before they could be used in the country.
SAHPRA has thus “listed” multiple COVID-19 tests and two Mpox diagnostic tests as approved for use in South Africa. Khanyisile Nkuku of SAHPRA’s medical devices unit told Spotlight that the diagnostic products for COVID-19 and Mpox received interim Section 21 authorisation.
Section 21 authorisation allows for the use of unregistered products under certain conditions, including public health emergencies. This mechanism has been used by SAHPRA both to respond to the public health needs posed by COVID-19 and Mpox and to prevent the use of substandard products, which was a challenge faced in the early days of COVID-19.
Nkuku added while South Africa has had a relatively low number of Mpox cases, South Africa is a leading supplier of in vitro diagnostics to the rest of the continent, including countries facing large Mpox crises, and so SAHPRA shares the responsibility of ensuring that Mpox diagnostics used on the continent work properly and is working with the African Medicines Regulatory Harmonisation programme to review Mpox diagnostics.
By Matimba Ngobeni, Country Head: Value & Access, Novartis South Africa
28 July 2025, Johannesburg South Africa – South Africa’s healthcare system stands at a crossroads. Despite the promise of progress outlined in the Budget Speech and the Presidential Health Compact, the reality on the ground reveals persistent and growing barriers to accessing innovative medicines.
Economic pressures, funding constraints, and infrastructure gaps continue to undermine equitable healthcare delivery, particularly for vulnerable communities. What’s more, recent international developments—such as U.S. President Donald Trump’s cuts to funding that supported healthcare initiatives in South Africa—threaten to exacerbate these challenges, potentially limiting access to life-saving advanced therapies.[1]
Economic pressures
The cost of advanced therapies remains out of reach, and the structural inequalities in our healthcare system persist. While top-tier medical plans still provide access to advanced medicines, we are seeing a shift. Patients are moving to lower-tier plans or into the public system, simply because they cannot afford more. And with that shift, their access to advanced therapies disappears. [2]This is not a uniquely South African problem.
Globally, we see the same story repeat: private healthcare becomes a fortress that only those who can pay the toll may enter. Everyone else is left to rely on an overburdened public system, strained by funding shortfalls, infrastructure gaps, and critical workforce shortages. The public healthcare system, already overburdened, struggles to absorb this increased demand. Rising healthcare costs combined with limited household budgets create a perfect storm where affordability becomes the biggest barrier to accessing cutting-edge treatments.
Funding constraints and infrastructure challenges
Both private and public sectors face severe funding constraints. Innovative medicines, especially advanced therapies, come with high price tags that strain budgets and limit availability. At the same time, infrastructure and skills gaps hinder the effective delivery of these treatments. Investments in healthcare infrastructure, workforce training, and data management are urgently needed to support the growing demand for advanced therapies.
While it may seem like all hope is lost, the Presidential Health Compact offers a promising framework aimed at transforming South Africa’s healthcare landscape through infrastructure development and improved data surveillance[3]. However, it stops short of directly addressing access to innovative medicines. This gap underscores the need for stronger collaboration between public and private stakeholders to ensure that patients do not bear the financial burden alone.
Towards equitable access: Collaboration is imperative
Another way forward is through a robust, transparent Health Technology Assessment (HTA) process, where medicines are evaluated not only on their cost but on their ability to save lives, improve quality of life, and reduce the long-term burden on the health system.
Inclusive HTAs, where payers and pharmaceutical companies work together, are essential for reimagining access to advanced therapies. If we only look at the upfront cost of innovation, we miss the bigger picture of societal value.
Globally, risk-sharing models and outcome-based pricing agreements are helping bridge the affordability gap[4]. South Africa could benefit from more flexible legislation to enable these models, ensuring that innovation doesn’t remain locked behind prohibitive price tags.
South Africa’s healthcare future depends on what we choose to prioritise: short-term financial gains or long-term societal wellbeing. Too often, systems have been designed around protecting profits rather than protecting lives. Healthcare should never be a luxury. Yet in South Africa, and across much of the world, the reality is stark: exclusion is the norm, not the exception.
If we want a future where access to life-saving medicines is a reality for all, we need to break down the barriers of affordability, infrastructure, and policy inertia. And we need to do it together — governments, healthcare companies, funders, and civil society — because lives are at stake.
All hope is not lost. But we cannot wait for crisis to be our catalyst. The time for bold, collaborative action is now.
**About Novartis:**
Novartis is an innovative medicines company. Every day, we work to reimagine medicine to improve and extend people’s lives so that patients, healthcare professionals and societies are empowered in the face of serious disease. Our medicines reach more than 250 million people worldwide.
Novartis South Africa (Pty) Ltd, Magwa Crescent West, Waterfall City, Jukskei View, 2090. Co. Reg. No. 1946/020671/07. Tel. No. +27 (0) 11 347 6600.
Disclaimer: The presentation may include data on formulations, products, indications, and dosages not yet approved by the South African Health Products Regulatory Authority. This information is not intended to be promoting nor recommending any formulation, indication, dosage, or other claim not covered in the approved Professional Information. Novartis South Africa (Pty) Ltd recommends the use of their products in accordance with the locally approved Professional Information. Views and opinions of speakers do not necessarily reflect those of Novartis.
Pretoria, 15 July 2025 – The South African Health Products Regulatory Authority (SAHPRA) was notified of the Lancet Global Health 2025; 13: e1250, an investigational study and its findings on substandard anti-cancer medications in Sub-Saharan African countries, including Ethiopia, Kenya, Malawi, and Cameroon. This study did not include South Africa. The seven (7) medicines/dosage forms mentioned in the study are cisplatin, oxaliplatin, methotrexate, doxorubicin, cyclophosphamide, ifosfamide, and leucovorin. The specific brands mentioned/shown in the article are neither registered nor marketed in South Africa.
SAHPRA, in terms of the Medicines and Related Substances Act 101 of 1965, as amended, and its General Regulations, requires medicines marketed in the country to meet prescribed requirements and adhere to set standards. Every batch of medicine produced must undergo testing to ensure that the integrity of the product is consistent with approved specifications before the release for sale, and imported medicines must additionally comply with the Guideline for Post-Importation Testing.
SAHPRA commenced internal processes to verify whether any of the South African-registered cancer medicines with the mentioned Active Pharmaceutical Ingredients (API) might have been affected or implicated. The cancer products registered and marketed in South Africa were not implicated/affected by the investigational study and its findings on substandard anti-cancer medicines. SAHPRA conducts risk-based post-market surveillance (PMS), sampling, and testing on high-risk medical products.
SAHPRA is satisfied that the marketed and registered cancer medicines meet the appropriate specifications; therefore, no substandard cancer medicines were detected.
“SAHPRA is committed to the three pillars of quality, safety, and efficacy. I am satisfied that our rigorous regulatory processes have borne fruit and that all patients, especially cancer patients, can rest assured that their health and well-being are not compromised,” indicated SAHPRA CEO, Dr Boitumelo Semete-Makokotlela.
The South African Health Products Regulatory Authority (SAHPRA) has joined the Medical Device Single Audit Programme (MDSAP), an international audit programme of medicines and medical device regulators aimed at improving efficiencies in the regulation of medical device manufacturers by engaging in work sharing and collaboration. SAHPRA joins MDSAP as an affiliate member, which expands its ability to monitor the manufacturing of medical devices beyond South Africa’s borders.
The MDSAP membership will result in the improved regulation of medical devices and in-vitro diagnostics (IVDs) as it increases SAHPRA regulatory reach and ensures that SAHPRA can leverage the resources of other regulators that participate in the MDSAP to both audit and monitor adherence to quality standards by medical device manufacturers in several countries globally.
“SAHPRA’s admission into MDSAP signals progress in our strategy to ensure the efficient application of our own resources and those of our peers globally in safeguarding the quality, efficacy and safety of medical devices and in-vitro diagnostics (IVDs) used by the South African public,” says Dr Boitumelo Semete-Makokotlela, SAHPRA Chief Executive Officer.
Dr Semete-Makokotlela says that the admission to MDSAP adds to individual agreements for both monitoring and regulatory reliance that SAHPRA already has in place with several regulators the world over, and would thus improve SAHPRA’s quality assurance abilities and has the potential to increase turnaround times in reviewing and approving key medical devices manufactured elsewhere in the world.
The South African Health Products Regulatory Authority (SAHPRA) encourages members of the public to always report any suspected side effects they may experience from taking medicines, vaccines and/or using medical devices, to help make medicines safer for everyone. While humanity benefits greatly from medicines in the treatment of illness and management of certain conditions, medicines may at times cause side effects. However, the risk of side effects and severe harm can be drastically reduced by taking medicines correctly and following the advice of a healthcare practitioner.
SAHPRA, together with over 90 other medicines and health products regulators as well as healthcare organisations globally, is participating in the annual #MedSafetyWeek awareness initiative, which takes place between 4 and 10 November 2024, under the theme “the importance of using medicines in the right way to prevent side effects, and to report side effects when they do occur”.
The awareness initiative is spearheaded by the Uppsala Monitoring Centre under the auspices of the World Health Organisation (WHO) Programme for International Drug Monitoring, a programme whose member organisations work nationally and collaborate internationally to monitor and identify adverse effects of medicines and vaccines, to reduce risks to patients, and to establish worldwide pharmacovigilance standards and systems.
During this #MedSafetyWeek and beyond, SAHPRA is calling upon patients, caregivers and healthcare professionals to utilise its reporting tools to report all suspected side effects and adverse reactions.
SAHPRA Chief Executive Officer, Dr Boitumelo Semete-Makokotlela, indicates that handling and storing as well as taking medicines as directed by a healthcare professional is key in reducing the incidence of adverse reactions. “Research shows that about half of all side effects are preventable. Patient safety is our top priority and during #MedSafetyWeek, we wish to remind patients to take their medicines as instructed and healthcare professionals to review therapies as well as each patient’s unique health conditions before prescribing or dispensing medicines,” says Dr Semete-Makokotlela.
SAHPRA calls upon the South African public and healthcare professionals to use either the MedSafety App or the eReporting portal both accessible on the SAHPRA website to report suspected side effects from health products. All reports are assessed and examined by SAHPRA to determine the correct steps to protect medicine users in South Africa from harm. The purpose is to gain better knowledge about known side effects and to discover new ones. This can result in warnings and changes to how a medicine is used. SAHPRA’s MedSafety App and eReporting portal can be used for reporting suspected adverse drug reactions from medicines, vaccines, herbal products, biological medicines and any quality issues relating to health products.