Facing high employee turnover and an aging population, nursing homes have increasingly turned to robots to complete a variety of care tasks, but few researchers have explored how these technologies impact workers and the quality of care.
A new study from a University of Notre Dame expert on the future of work finds that robot use is associated with increased employment and employee retention, improved productivity and a higher quality of care. The research has important implications for the workplace and the long-term care industry.
Yong Suk Lee, associate professor of technology, economy and global affairs at Notre Dame’s Keough School of Global Affairs, was the lead author for the study, published in Labour Economics. Most studies of robots in the workplace have focused on manufacturing and the industrial sector, but Lee’s research broke new ground by analysing long-term care – and by looking at the different types of robots used in this setting. Researchers drew on surveys of Japanese nursing homes taken in 2020 and 2022.
“Our research focused on Japan because it is a super-aging society that provides a good example of what the future could entail elsewhere – a declining population, a growing share of senior citizens and a declining share of working-age people,” Lee said. “We need to be ready for this new reality.”
In 2022, for instance, more than 57 million U.S. residents were 65 or older, according to the National Council on Aging. The Census Bureau forecasts that by 2050, this number will grow to 88.5 million.
The impact on workers
In a future where there are more senior citizens requiring care, using robots in a targeted fashion could benefit workers and patients alike, Lee said. The study analyzed three types of robots that are increasingly used in assisted living facilities:
Transfer robots, which nurses use to lift, move and rotate patients in beds and around rooms.
Mobility robots, which patients use to move around and to bathe.
Monitoring and communication robots, which include technologies such as computer vision and bed sensors that can monitor patient data such as movement and share it with care providers.
“We found that robot adoption complements care workers by reducing quit rates,” Lee said. “This is important because turnover is a big concern in nursing homes. Workers typically experience a great deal of physical pain, particularly in their knees and back. The work is hard and the pay is low. So robot use was associated with employee retention.”
While robot use was associated with an overall employment increase, Lee said, the trend seems to have helped some workers more than others: It was associated with an increased demand for part-time, less experienced employees and with less demand for more experienced workers.
Improving patient care
Patients benefited in facilities that have used robots, according to the study. The nursing homes that Lee’s team studied reported a decrease in the use of patient restraints and in the pressure ulcers or bedsores that nursing home residents commonly suffer, largely because of a lack of mobility. Both metrics are widely used in the long-term care industry to measure patient outcomes, Lee said.
By removing the physical strain associated with certain tasks, Lee said, robots may have made room for care workers to focus on tasks better suited for human beings.
“Robots can improve productivity by shifting the tasks performed by care workers to those involving human touch, empathy and dexterity,” Lee said. “Ultimately, robots can help workers provide a higher level of patient care.”
Dr Tim Forgan at the surgeon’s console of the da Vinci robotic system. (Photo: Biénne Huisman/Spotlight)
By Biénne Huisman
Within South Africa’s beleaguered public health sector – unsettled by budget cuts, understaffing, and divisive NHI legislation – cutting edge surgical robots that have been used to perform more than 600 surgeries at two Cape Town public hospitals are beacons of excellence that offer a glimmer of hope. Spotlight’s Biénne Huisman visited Dr Tim Forgan at Tygerberg Hospital to learn more.
Cutting edge robotic surgery might not immediately come to mind when one thinks of public hospitals, but in a first for public healthcare in South Africa, such systems are being used at two hospitals in the Western Cape.
The da Vinci Xi systems enable surgeons to control operations from a console – steering three arms with steel “hands” equipped with tiny surgical instruments; plus a fourth arm bearing a video camera (the laparoscope). The system translates a surgeon’s hand movements in real time, with enhanced precision, range and visuals, compared to manual surgery.
“It really is next level, it feels like you’re inside the patient,” says colorectal specialist Dr Tim Forgan, Tygerberg Hospital’s da Vinci robotics coordinator. “With this technology we can operate so much finer. You can see ten times better with this robot than with the naked eye; you can see tiny, tiny nerves you wouldn’t normally see. And you can manoeuvre surgical instruments so much better. Because of that, people have way better function after the procedure.”
He explains that the technology allows major surgery to be completed through small incisions – instead of larger cuts made by a doctor’s hand – leading to less bleeding and a faster recovery time.
Over 600 surgeries in two years
Lorraine Gys from Phillipstown in the Northern Cape can attest. On 22 February 2022, the 65-year-old pensioner became the first patient to undergo da Vinci robotic surgery in South Africa’s public sector. Forgan was behind the console, at Tygerberg Hospital.
Gys tells Spotlight: “The next day the sisters offered to wash me, I said to them ‘no, I’m not helpless.’ My recovery was very quick. I was up and about in no time, while the other patients had to be assisted. I was discharged on day four, and back at home I could even continue doing my own chores.”
Two years later, Gys is cancer free. The mother of three, who now lives in Eerste River, recalls how she made news headlines: “Before the operation, Dr Forgan explained everything to me. They asked my permission, saying that media will be there and the [provincial health] minister.”
Indeed, on the day Forgan operated on Gys, removing a cancerous rectal tumour, he was joined in theatre by several onlookers including former Western Cape MEC of Health and Wellness Nomafrench Mbombo.
“Yes it was a circus,” says Forgan, laughing. “A whole bunch of people watching me operate, quite bloody nerve-wracking. Fortunately I’m experienced at having lots of students around watching; plus performing surgery is just so immersive, everything else fades out.”
On that day, also in the operating room was colorectal surgeon Dr Roger Gerjy, keeping an eye. “He’s a very well-known robotic surgeon; a Swedish surgeon who works in Dubai,” says Forgan. “And if there was a problem, Roger would’ve taken over. He was also there to impart tips and tricks: move the instrument like this, shape it like a hockey stick; because with the robot it’s like having your whole arm inside [the body]. He’d give me advice on what to do with my extra floating arm – where to place it and how to manipulate it – because remember you’re controlling three arms at a time.”
Since 2022, the da Vinci robots installed at Cape Town’s two tertiary hospitals: Groote Schuur and Tygerberg, have enabled over 600 minimally invasive surgeries – including colorectal operations, prostatectomies, cystectomies (bladder removal surgery), and gynaecological procedures to treat endometriosis.
Groote Schuur Hospital has the other da Vinci Xi system run by Western Cape public healthcare
A spokesperson for the Western Cape Ministry of Health and Wellness, under former MEC Mbombo, Luke Albert explains: “We can see the immense impact it has for patients and the health system. For example, a traditional open cystectomy patient would require three days of ICU stay, as well as two weeks of hospital stay to recuperate. During this time, on average, 42% of patients require blood transfusions and almost 20% need total parenteral nutrition (when a patient is fed intravenously). A patient undergoing robotic surgery for a cystectomy requires no ICU stay and goes straight to a general ward for no more than six days on average, with no blood transfusions needed.”
Where the money came from
Asked how the department was able to afford R40 million per system for these machines in the context of severe budget cuts, Albert says: “The purchase was applicable to 2021/22 and not the current financial year; with all provincial health departments currently managing the effects of budget cuts.”
Asked the same question, Forgan explains the investment derived from surplus budget discovered within the throes of the COVID-19 pandemic: “There was a surplus because certain services just couldn’t be done. I mean, for us, we couldn’t do elective surgery. And how state funding works; if you don’t spend your [provincial] budget within the financial year, it goes back to central government.”
What it looks like
On a Friday afternoon at Tygerberg Hospital, Forgan is guiding Spotlight along corridors and up grey linoleum stairs, to the theatre where the da Vinci system is used. Dressed in black surgical scrubs bearing his name and a cap; on his feet Forgan is wearing bright pink crocs. In passing, he waves hello to fellow healthcare staff.
Inside the small blindingly white room, Forgan points out the three core components of the da Vinci system. There is a console with two control levers similar to refined joysticks – he demonstrates how to delicately hold them between forefingers and thumbs – a patient-side cart with four interactive metal arms (they are disposable; each arm can be used on twelve patients), and another trolley with a television screen. All connected by blue fibre optic cables.
As we speak, nurses arrive in the theatre, preparing it for upcoming gynaecology procedures scheduled for Monday. Forgan greets them, then continues to expand on his passion for colorectal surgery.
“With colorectal surgery, there’s a high rate of complications, but I really enjoy it, I really enjoy my job. When you have a successful outcome, saving a person from their cancer and prolonging their life through your intervention, that is the reward. Colorectal cancer is a very unpleasant disease, and operating like this can make one hell of a difference in a patient’s life.”
Colorectal cancer on the increase
Forgan adds that colorectal cancer is on the increase: “There aren’t many colorectal surgeons in South Africa, with a dire need for people to operate in this subspecialty. I mean, there are so few of us, we’re all on a WhatsApp group.”
Colorectal or colon cancer is the second most common cancer in South African men (following prostate cancer), and the third most common cancer in women (following breast and cervical cancer), according to the Cancer Association of South Africa.
Originally from Johannesburg, Forgan attended medical school at the University of the Witwatersrand. He qualified as a general surgeon at Stellenbosch University, sub-specialising in colorectal surgery at the University of Cape Town, before studying minimally invasive colorectal surgery at the Academic Medical Centre in Amsterdam.
He is also president of the South African Colorectal Society and runs a part-time private practise with his Tygerberg colleague, Dr Imraan Mia, at Cape Town’s Christiaan Barnard Hospital, where he has 32 all five-star Google reviews.
‘Early adopter’
Forgan considers himself an early adopter. But learning to use the da Vinci system did not happen overnight.
“We trained for ages,” he says. “On the surgical console there’s a simulator, so you spend hours and days and days doing procedures, over and over and over again. You have to get over 95% for each one of the procedures, before you can move on to the next skill.
“Then it’s how to use the machine, how to put it together, what to do if there’s an emergency; what if there’s a power failure and the machine stops working? How to safely remove it from the person. Then we went to the University of Lyon [in France] for two days of hands-on robotics training. And then a proctor – an international expert – comes to your theatre and does the procedures with you. So that was Dr Roger Gerjy, and that’s when we did Lorraine…”
First introduced by American biotechnology company Intuitive Surgical in 1999, the da Vinci Xi systems have sparked some liability lawsuits. An article from the Tampa Bay Times in February cites a lawsuit filed at the United States District Court in West Palm Beach, with a man claiming that a stray electrical arc from a surgical robot burned his wife’s small intestine during a colon cancer procedure, causing her death. The article quotes Intuitive Surgical’s 2023 financial report, which notes 8 606 da Vinci systems in use worldwide, having performed 2 286 000 procedures in 2023. The financial report mentions an undisclosed number of pending lawsuits, which the company disputes.
Nevertheless, Forgan remains an advocate.
Exiting via Tygerberg’s maze of corridors, he continues to reflect on his job. After our meeting, he is set to deliver a talk at the Cape Town International Convention Centre. His manner is earnest. Shrugging, he describes himself as a “glorified plumber”.
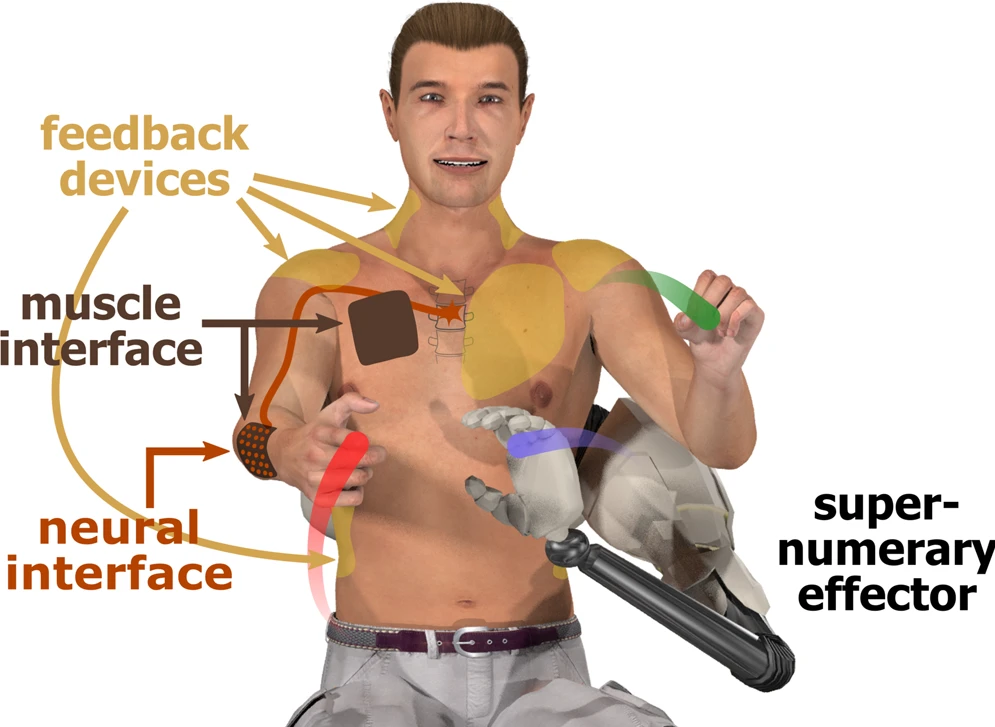
Interfaces for DoF augmentation (figure by Tobias Pistohl). From Eden at al., Nature Communications. 2022
Busy doctors and nurses may have often found themselves wishing they had an extra arm to help with a patient or help with a difficult suture. Researchers around the world are developing supernumerary robotic arms to help workers achieve certain tasks unaided, or with less strain – but how long would it take to master learning an additional limb? The answer is: not long at all. One hour’s worth of training is enough for people to carry out a task with their ‘third arm’ as effectively as with a partner, according to the results of a new study published in IEEE Open Journal of Engineering in Medicine and Biology.
A new study by researchers at Queen Mary University of London, Imperial College London and The University of Melbourne has found that people can learn to use supernumerary robotic arms as effectively as working with a partner in just one hour of training.
The study investigated the potential of supernumerary robotic arms to help people perform tasks that require more than two hands. The idea of human augmentation with additional artificial limbs has long been a staple of science fiction.
Demonstrating performing a suture with an assistant robotic arm.
“Many tasks in daily life, such as opening a door while carrying a big package, require more than two hands,” said Dr Ekaterina Ivanova, lead author of the study from Queen Mary University of London. “Supernumerary robotic arms have been proposed as a way to allow people to do these tasks more easily, but until now, it was not clear how easy they would be to use.”
The study involved 24 participants who were asked to perform a variety of tasks with a supernumerary robotic arm. The participants were either given one hour of training in how to use the arm, or they were asked to work with a partner.
The results showed that the participants who had received training on the supernumerary arm performed the tasks just as well as the participants who were working with a partner. This suggests that supernumerary robotic arms can be a viable alternative to working with a partner, and that they can be learned to use effectively in a relatively short amount of time.
“Our findings are promising for the development of supernumerary robotic arms,” said Dr Ivanova. “They suggest that these arms could be used to help people with a variety of tasks, such as surgery, industrial work, or rehabilitation.”
Advancements in AI have resulted in typically human characteristics like creativity, communication, critical thinking, and learning being replicated by machines for complex tasks like driving vehicles and creating art. With further development, these human-like attributes may develop enough to one day make it possible for robots and AI to be entrusted with nursing, a very ‘human’ practice. But… would it be ethical to entrust the care of humans to machines?
In a step toward answering this question, Japanese researchers recently explored the ethics of such a situation in the journal Nursing Ethics.
The study was conducted by Associate Professor Tomohide Ibuki from Tokyo University of Science, in collaboration with medical ethics researcher Dr Eisuke Nakazawa from The University of Tokyo and nursing researcher Dr Ai Ibuki from Kyoritsu Women’s University.
“This study in applied ethics examines whether robotics, human engineering, and human intelligence technologies can and should replace humans in nursing tasks,” says Dr Ibuki.
Nurses show empathy and establish meaningful connections with their patients, a human touch which is essential in fostering a sense of understanding, trust, and emotional support. The researchers examined whether the current advancements in robotics and AI can implement these human qualities by replicating the ethical concepts attributed to human nurses, including advocacy, accountability, cooperation, and caring.
Advocacy in nursing involves speaking on behalf of patients to ensure that they receive the best possible medical care. This encompasses safeguarding patients from medical errors, providing treatment information, acknowledging the preferences of a patient, and acting as mediators between the hospital and the patient. In this regard, the researchers noted that while AI can inform patients about medical errors and present treatment options, they questioned its ability to truly understand and empathise with patients’ values and to effectively navigate human relationships as mediators.
The researchers also expressed concerns about holding robots accountable for their actions. They suggested the development of explainable AI, which would provide insights into the decision-making process of AI systems, improving accountability.
The study further highlights that nurses are required to collaborate effectively with their colleagues and other healthcare professionals to ensure the best possible care for patients. As humans rely on visual cues to build trust and establish relationships, unfamiliarity with robots might lead to suboptimal interactions. Recognising this issue, the researchers emphasised the importance of conducting further investigations to determine the appropriate appearance of robots for facilitating efficient cooperation with human medical staff.
Lastly, while robots and AI have the potential to understand a patient’s emotions and provide appropriate care, the patient must also be willing to accept robots as care providers.
Having considered the above four ethical concepts in nursing, the researchers acknowledge that while robots may not fully replace human nurses anytime soon, they do not dismiss the possibility. While robots and AI can potentially reduce the shortage of nurses and improve treatment outcomes for patients, their deployment requires careful weighing of the ethical implications and impact on nursing practice.
“While the present analysis does not preclude the possibility of implementing the ethical concepts of nursing in robots and AI in the future, it points out that there are several ethical questions. Further research could not only help solve them but also lead to new discoveries in ethics,” concludes Dr Ibuki.
Having jobs be replaced by robots is a common fear for workers in all sectors of the economy. Working alongside robots may contribute to job burnout and workplace incivility, but self-affirmation techniques could help alleviate fears about being replaced by these machines, according to research published online in the Journal of Applied Psychology [PDF].
Researchers found that workers in the United States and parts of Asia feel job insecurity from robots, even in industries where robots aren’t being used, and those fears may not be justified, said lead researcher Kai Chi Yam, PhD, an associate professor of management at the National University of Singapore.
“Some economists theorise that robots are more likely to take over blue-collar jobs faster than white-collar jobs,” Dr Yam said. “However, it doesn’t look like robots are taking over that many jobs yet, at least not in the United States, so a lot of these fears are rather subjective.”
Researchers conducted experiments and analysed data from participants in the US, Singapore, India and Taiwan.
Working with industrial robots was linked to greater reports of burnout and workplace incivility in an experiment with 118 engineers employed by an Indian auto manufacturing company.
An online experiment with 400 participants found that self-affirmation exercises, where people are encouraged to think positively about themselves and their uniquely human characteristics, may help lessen workplace robot fears. Participants wrote about characteristics or values that were important to them, such as friends and family, a sense of humour or athletics.
“Most people are overestimating the capabilities of robots and underestimating their own capabilities,” Dr Yam said.
Fears about job insecurity from robots are common. The researchers analysed data about the prevalence of robots in 185 U.S. metropolitan areas along with the overall use of popular job recruiting sites in those areas (LinkedIn, Indeed, etc). Areas with the highest robot use also had the highest rates of job recruiting site searches, even though unemployment rates weren’t higher in those areas. The researchers theorised that people in these areas may have felt more job insecurity because of robots, but that there could be other reasons, such as people seeking new careers or feeling dissatisfied with their current jobs.
Another experiment comprised 343 parents of students at the National University of Singapore who were randomly assigned to three groups. One group read an article about the use of robots in businesses, the second group read a general article about robots, and the third read an unrelated article. Then the participants were surveyed about their job insecurity concerns, with the first group reporting significantly higher levels of job insecurity than the two other groups.
While some people may have legitimate concerns about losing their jobs to robots, some media coverage may be unnecessarily heightening fears among the general public, Dr Yam said.
“Media reports on new technologies like robots and algorithms tend to be apocalyptic in nature, so people may develop an irrational fear about them,” he said.
Recent advances in neural science, robotics, and software have enabled scientists to develop a robotic system that responds to muscle movement signals from a partially paralysed person relayed through a brain-machine interface. Human and robot act as a team to make performing some tasks a piece of cake.
Two robotic arms – a fork in one hand, a knife in the other – flank a seated man, who sits in front of a table, with a piece of cake on a plate. A computerised voice announces each action: “moving fork to food” and “retracting knife.” Partially paralysed, the man makes subtle motions with his right and left fists at certain prompts, such as “select cut location”, so that the machine slices off a bite-sized piece. Now: “moving food to mouth” and another subtle gesture to align the fork with his mouth.
In less than 90 seconds, a person with very limited upper body mobility who hasn’t been able to use his fingers in about 30 years, just fed himself dessert using his mind and some smart robotic hands.
A team led by researchers at the Johns Hopkins Applied Physics Laboratory (APL), in Laurel, Maryland, and the Department of Physical Medicine and Rehabilitation (PMR) in the Johns Hopkins School of Medicine, published a paper in the journal Frontiers in Neurorobotics that described this latest feat using a brain-machine interface (BMI) and a pair of modular prosthetic limbs.
Also sometimes referred to as a brain-computer interface, BMI systems provide a direct communication link between the brain and a computer, which decodes neural signals and ‘translates’ them to perform various external functions, from moving a cursor on a screen to now enjoying a bite of cake. In this particular experiment, muscle movement signals from the brain helped control the robotic prosthetics.
A new approach
The study built on more than 15 years of research in neural science, robotics, and software, led by APL in collaboration with the Department of PMR, as part of the Revolutionizing Prosthetics program, which was originally sponsored by the US Defense Advanced Research Project Agency (DARPA). The new paper outlines an innovative model for shared control that enables a human to manoeuvre a pair of robotic prostheses with minimal mental input.
“This shared control approach is intended to leverage the intrinsic capabilities of the brain machine interface and the robotic system, creating a ‘best of both worlds’ environment where the user can personalise the behaviour of a smart prosthesis,” said Dr Francesco Tenore, a senior project manager in APL’s Research and Exploratory Development Department. The paper’s senior author, Tenore focuses on neural interface and applied neuroscience research.
“Although our results are preliminary, we are excited about giving users with limited capability a true sense of control over increasingly intelligent assistive machines,” he added.
Helping people with disabilities
One of the most important advances in robotics demonstrated in the paper is combining robot autonomy with limited human input, with the machine doing most of the work while enabling the user to customize robot behavior to their liking, according to Dr David Handelman, the paper’s first author and a senior roboticist in the Intelligent Systems Branch of the Research and Exploratory Development Department at APL.
“In order for robots to perform human-like tasks for people with reduced functionality, they will require human-like dexterity. Human-like dexterity requires complex control of a complex robot skeleton,” he explained. “Our goal is to make it easy for the user to control the few things that matter most for specific tasks.”
Dr Pablo Celnik, project principal investigator in the department of PMR said: “The human-machine interaction demonstrated in this project denotes the potential capabilities that can be developed to help people with disabilities.”
Closing the loop
While the DARPA program officially ended in August 2020, the team at APL and at the Johns Hopkins School of Medicine continues to collaborate with colleagues at other institutions to demonstrate and explore the potential of the technology.
The next iteration of the system may integrate previous research that found providing sensory stimulation to amputees enabled them to not only perceive their phantom limb, but use muscle movement signals from the brain to control a prosthetic. The theory is that the addition of sensory feedback, delivered straight to a person’s brain, may help him or her perform some tasks without requiring the constant visual feedback in the current experiment.
“This research is a great example of this philosophy where we knew we had all the tools to demonstrate this complex bimanual activity of daily living that non-disabled people take for granted,” Tenore said. “Many challenges still lie ahead, including improved task execution, in terms of both accuracy and timing, and closed-loop control without the constant need for visual feedback.”
Celnik added: “Future research will explore the boundaries of these interactions, even beyond basic activities of daily living.”
Having to cope with the strain of COVID on an already fragile healthcare system, a few hospitals in the Western Cape have been introducing robotics for specialised tasks – but are they worth the hype?
Robotics was able to fill an unprecedented need during the COVID pandemic – the ability to remotely conduct ward rounds from remote locations. Tygerberg Hospital made use of ‘Quintin’, a robot that is essentially a tablet on a mobile stand that allows users to remotely communicate and inspect the area, but it can’t physically interact with its environment.
Robotics offers greater surgical precision, which may translate into reduced healthcare load. IOL reported that the provincial Department of Health plans to use a pair of new robotic surgery machines installed at the Groote Schuur and Tygerberg hospitals to fast-track surgeries and address the province’s surgical backlogs caused by COVID. These robotic surgery units will be used for procedures on colorectal, liver, prostate, kidney and bladder cancers, and women with severe endometriosis. In the province’s private sector, Netcare Christiaan Barnard Memorial Hospital also makes use of robotic-assisted surgery.
Robotic surgery has a number of advantages. The small robotic arms allow for smaller incisions and faster recovery times, reducing the strain on hospitals. A liver resection that would have a patient in hospital for a week can be reduced to one or two days with robotic surgery. More complex surgery becomes possible, eg in difficult to access areas or in patients with obesity. Robotic surgery allows surgeons to be off their feet, easing an extremely fatiguing job, and the software automatically compensates for any tremor in the surgeon’s hands.
However, robotic surgery still has drawbacks – chief among them is cost and the need to have trained personnel to operate them. There is also some latency between the surgeon’s hands movements and the corresponding movement of the robot, leading to possible errors. Shorting of the electrical current running through the robotic arms can also cause burns to the patient’s tissue, and there is also the possibility of nerve compression injuries due to the positioning of the patient. Furthermore, operator errors, especially when operators are inexperienced or robotic surgery is performed in lower volumes, is always a possibility.
Robotics have promising applications in sanitation – they can easily disinfect areas using UV light, for example – and can also assist nurses with certain tasks, such as making a 3D vein map prior to a venipuncture. Some robots can even assist the elderly, conversing with them and can perform simple tasks like calling a nurse. Other applications include the much simpler technology of exoskeletons, a wearable frame which amplify users’ strength (though nowhere near that of the fictional Iron Man) and are useful in rehabilitation and for enhancing mobility in the elderly. Other applications include increasing strength of care staff for assisting patients, freeing up other staff.
Some exoskeletons are even purely mechanical, merely readjusting loads without any sophisticated electronics or motors. Yet even these are prohibitively expensive: the Phoenix Medical Exoskeleton goes for about US$30 000 each.
While promising, robotic systems are at present still hugely expensive, limited in function and can only assist with a small fraction of the tasks that healthcare workers perform. Even if the cost could be reduced enough to help ease healthcare worker burden in South Africa to help, that still leaves the problem of enough experienced and motivated healthcare workers, beds and neglected rural areas.
Though it’s not quite as fantastic as Iron Man’s super-powered exoskeleton, a robotic exoskeleton designed by his father’s company helps 16 year old Oscar Constanza to walk. Oscar has a genetic neurological condition that means his nerves do not send enough signals to his legs.
Fastened to his shoulders, chest, waist, knees and feet, the exoskeleton enables Oscar to walk across the room and turn around. The exoskeleton is a voice-operated robot, responding to the user’s verbal commands, rather than other designs which respond to user movements or nerve signals.
“Before, I needed someone to help me walk … this makes me feel independent,” said Oscar.
His father Jean-Louis Constanza is one of the co-founders of the company that makes the exoskeleton, which is called Atalante.
“One day Oscar said to me: ‘dad, you’re a robotic engineer, why don’t you make a robot that would allow us to walk?’” his father recounted “Ten years from now, there will be no, or far fewer, wheelchairs,” he said.
Exoskeletons are being produced around the world, with a wide variety of applications including, the military, industrial work and in healthcare to help nurses move and position patients. During the COVID pandemic, they have even been evaluated for use in the physically taxing task of prone positioning of COVID patients in ICU wards. Some, like Wandercraft’s model, are designed to help people with mobility problems to walk.
Since most are still quite heavy, manufacturers are competing to make them as light and usable as possible.
Wandercraft’s Atalante exoskeleton, which is an outer frame that supports but also simulates the movement of the wearer’s body, has been sold to dozens of hospitals in France, Luxembourg and the United States, with a unit price of about $176 000, said Constanza. The Atalante exoskeleton is currently aimed at use in physical rehabilitation in stroke and spinal cord injury patients.
At the moment, it cannot be bought by private individuals for everyday use – but the Wandercraft engineers are working on this as the design would need to be much lighter.