To mark Men’s Health Awareness Month, International SOS, the world’s leading health and security risk services company, emphasises the importance of creating supportive workplace environment that foster men’s health and mental wellbeing.
Men’s health remains a significant concern and poorer health profiles for men than for women have been reported, with discrepancies found in metrics including life expectancy, mortality rates, disability-adjusted life years, and non-sex-specific disease death rates.1 The World Health Organization (WHO) reports that non-communicable diseases (NCDs), are claiming around 74% of all lives lost each year2, and in 2018, NCDs and injuries accounted for 86% of all male fatalities.3
The WHO data shows that men across all socioeconomic groups demonstrate unhealthier smoking practices, unhealthier dietary patterns, higher alcohol consumption levels and higher rates of injuries than women.3 In fact, among the global population that used tobacco in 2020, a significantly higher percentage were men (36.7%), compared to women (7.8%).4 These statistics highlight the need to focus on improving men’s health and organisations can play a vital role in enhancing men’s health within their workplaces.
Men are significantly less likely than women to seek preventive care services, which can often lead to undiagnosed conditions.1 Men are also found to be less likely to have received mental health treatment than women. The stigma attached to illness and men perceiving illness as a weakness are often found to be the reasons why men are not as vocal about their health and mental wellbeing concerns.5
Dr Anthony Renshaw, Regional Medical Director at International SOS, said “Men’s Health Awareness Month provides a crucial opportunity for organisations to re-evaluate their approach to supporting the health and wellbeing of male employees. In addition to physical health, we must also prioritise mental health, as it has a direct impact on overall productivity and workplace satisfaction. Employers can play a pivotal role in fostering open discussions, reducing stigma, and promoting a supportive environment for men to seek the help they may need.”
International SOS offers guidelines for organisations to provide workplace support specific for men’s health and wellbeing with the ‘H-O-P-E’ approach:
Hold workplace men’s forum that can act as a safe space. Having a supportive work environment where everyone, particularly men, know that they are allowed the time to address any health concerns is extremely enabling.
Offer male-specific confidential support from mental health professionals.
Provide your team leads with appropriate training to enable them to spot early signs of poor physical and mental health and know where they can signpost their employees to.
Encourage employees to have regular health check-ups, particularly screening for early detection and treatment of NCDs, as well as a mental health assessment if needed.
Only concerted multi-disciplinary collaboration and research will stem the tide of diabetes and diabetes-linked cardiovascular disease (CVD), the latter currently the leading cause of death locally and worldwide, claiming 17.9 million lives annually1.
This was the consensus among some of the world’s leading cardiologists and researchers gathered at the SA Heart Association’s annual congress aptly themed: ‘The Cardiac Collaboration,’ which took place at the Sandton Convention Centre in Johannesburg from 26-29 October this year.
Globally, CVD takes more lives than TB, HIV and malaria combined, while 215 South Africans are killed by CVD every day – with 80% of CVD and strokes being preventable.1,2 The prevalence of diabetes has also increased in South Africa, from 4.5% in 2010 to 12.7% in 2019. Of the 4.58 million people aged 20-79 years who were estimated to have diabetes in 2019, 52.4% were undiagnosed.3
With diabetes being a key driver of CVD – especially in Africa (with limited access to novel drugs and the prevalence of sugar-rich, poverty-driven lifestyles), the mutual consensus at this year’s congress was that collaboration is key.
Dr Zaheer Bayat, Chairperson of the Society for Endocrinology, Metabolism and Diabetes of South Africa (SEMDSA), told delegates that endocrinologists and cardiologists would have to work together to improve outcomes for diabetic patients, 30% of whom suffered cardiovascular events. He warned that a 134% increase of people living with diabetes was predicted over the next two decades, translating into a dramatic surge in chronic kidney disease, cardiovascular disease, blindness, and amputations.
Dr Bayat said he intends appealing for mass diabetes screening to find the 52% of people whom researchers estimate are undiagnosed. Ideally, this should be followed by access to cheaply acquired, effective new glucose-lowering drugs.
“The reality is that this country cannot afford all the new treatments for everyone – not private funders, not government. So, drugs are not really a solution – the best solution is to change lifestyle and prevent disease in the first place,” said Dr Bayat.
“We’re here to fight for our patients, not our pockets. Can we afford to have 52% of our patients not knowing they’re diabetic? People who should be contributing to our economy are living with diabetes and eventually dying,” he asserted.
Dr Bayat also said that globally, First World countries such as the USA and Sweden are reducing myocardial infarctions, strokes, and amputations, because they’re doing all the right things together. This included adopting a healthy lifestyle, effective management of sugar, blood pressure and cholesterol and smoking cessation.
“However, here in South Africa with private healthcare representing 15% of healthcare delivery but consuming 50% of the spend and the public sector representing 85% of the population and consuming the other half – we’re not doing nearly as well. With only 200 cardiologists in the country (one per 190 000 population), and even less nephrologists, we need to join together and change the trajectory of diabetes. We must work together to reduce morbidity and mortality,” said Dr Bayat.
According to the SA Heart Association, this graphically illustrates the importance of a multi-disciplinary approach, the very reason why the conference was called ‘The Cardiac Collaboration.’
The SA Heart Association has already begun forging formal ties with other academic societies and next year, it hopes to join and host joint sessions with collaborative meetings to connect a multidisciplinary team in order to achieve a well-rounded balance of care.
Already long surgical waiting lists in the Northern Cape appear to have ballooned in recent months. In May, the province’s MEC for Health Maruping Lekwene told the province’s legislature that surgical waiting lists in the province stood at just under 4000. According to more recent figures from the Northern Cape Department of Health’s 2023/24 First Quarterly report, the surgical backlog stands at 6373 – an increase of more than 50% on the figure given in May.
Lulu Mxekezo, Northern Cape Department of Health Spokesperson, confirmed to Spotlight last week that the surgical backlogs had indeed increased from around 4000 to around 6000. She said that the numbers fluctuate as the need continues to increase on a daily basis.
“The shortage of specialised theatre staff makes it impossible for us to utilise all theatres daily to perform the procedures,” said Mxekezo, adding that the department will not compromise the safety and lives of patients and operate in theatres with no specialised theatre staff.
The increase in the backlog came despite the outsourcing of some surgical services in the province. Lekwene told the legislature that the Northern Cape Department of Health pays Gauteng-based Medicomed (captured as Medicore-Mets in the legislature minutes) R400 000 per month to assist with orthopaedic surgeries at Robert Mangaliso Sobukwe (RMS) Hospital in Kimberly on a month-to-month basis. He said the company supplies the department with specialised theatre nurses which is a scarce skill in the province. In May, Lekwene told legislators that the company had assisted with 57 surgeries over a two-week period.
Lack of theatre staff
The quarterly report stated that the backlog is fuelled by the lack of theatre staff at RMS hospital, and that the private sector was called in to fill this gap.
When asked by Izak Fritz, Democratic Alliance member of the Provincial Legislature, why the department does not appoint specialist nurses instead of outsourcing these services, Lekwene answered that there are unfortunately not enough theatre specialist nurses in the province.
“For us to take this route, it means that we need to have internal capacity. For instance we will have a neurosurgeon but we will not have an anaesthetist. We have nurses, but we do not have theatre specialist nurses,” he said.
He said they do not enjoy outsourcing, but that because of the urgency and the growing backlog the department has to act swiftly. “However as soon as the backlog has been reduced, we will then try to use our internal staff,” he said.
Lekwene also told the legislature that the backlog was mostly caused by the Covid-19 pandemic. “Remember that for two years during Covid-19, hospitals were closed,” he said.
Left stranded
Some workers at RMS said the long waiting list has left many patients frustrated and stranded. One doctor described the situation to Spotlight as “dire”. “The hospital has four fully equipped theatres but patients do not get help,” he said. He asked not to be named for fear of losing his job.
“Yes, we do have a shortage of nurses, but it is not as bad as they say. We are available as doctors, but without the help from nurses we are unable to perform surgeries at all,” he said.
The doctor said that currently the list of patients that need to receive emergency surgery is longer than 30. He said that for ordinary surgeries such as hip replacements there are patients who have been in hospital for more than 18 months, while some have been waiting for cataract surgery for five years.
A strain on staff and patients
Dennis Segano, provincial chairperson of Health and Other Services Personnel Trade Union in South Africa (HOSPERSA) said the surgery backlog is putting a strain on both nurses and patients.
He said the main problems that they see at RMS is the shortage of specialised theatre nurses and a lack of equipment. “When you enter the theatres there are enough doctors but not enough nurses,” he said. “We have a problem with our theatre nurses who are often outsourced by the service provider to work during their surgery marathons at the RMS hospital but have to wait three months or sometimes even six months before they can get paid.”
Spotlight asked Mxekezo about the late payment allegations but had not received a response by the time of publication.
“We don’t know why the government is not appointing the nurses instead of paying a service provider,” Segano said. “The system is burdened, the nurses in orthopaedic wards are burdened and we feel sad for the patients who have to spend months in hospital. “As a patient when you have a fracture, you must be able to go to theatre immediately, but in this province, you have to wait months before you receive help.”
“Stakeholders are also assisting us in performing theatre marathons to deal with the backlog,” Mxekezo said.
For example, in October last year, disaster relief organisation Gift of the Givers sent a team of theatre nurses and anaesthetists to assist with the backlog at RMS. According to Ali Sablay, the organisations project manager, they performed 72 operations on 72 patients during the catch-up drive.
Long-term solution
When asked what the department’s long-term plans are to reduce the pressure, Mxekezo explained that the operationalisation of theatres in district hospitals with specialised theatre staff will assist in minimising the backlog at RMS as many patients are transferred from districts.
Segano agreed that a long-term solution is to equip district hospitals with decent theatres and specialised theatre nurses.
“Minor fractures must be dealt with at district hospitals. RMS Hospital must only perform serious surgeries,” he said. “If the department can prioritise Harry Surtie Hospital and De Aar Hospital with theatre staff and equipment, RMS Hospital will operate much better and the patients will be helped. It is incorrect to send all patients of the Northern Cape to one hospital in Kimberly. They will not succeed.”
“Permanent employment of theatre staff will also assist in stabilising the surgical backlogs,” Mxekezo said.
Sceptical opposition
Fritz told Spotlight the DA is very concerned about the growing backlog in the Northern Cape and that they have repeatedly highlighted surgery backlogs at the provinces only tertiary facility (RMS).
“When one looks at nursing appointments at the RMS hospital, we see a trend whereby more nurses’ contracts are terminated each year than the amount of nurses who actually get appointed,” he said. “In effect, the hospital only operationalises four of its nine theatres.”
“Despite agreements with private agencies for surgery marathons to help tackle the backlogs, this only has a limited impact because of the inability to operationalise more theatres and to ensure there is an availability of more beds for recovery,” he said.
Fritz said the reality is that the people who require elective surgery often have to wait years to be attended to while their condition progresses. “Only when their case becomes an emergency can they be bumped up the list, and by that time their disease has become worse and their hopes of a full recovery is minimised,” he said.
Wynand Boshoff, the Freedom Front Plus’s (FF+) Northern Cape Provincial Leader, said in an interview with Spotlight last week that the problem with the department is that it is an entity that is riddled with mismanagement and a culture which aims for anything but service delivery.
He said the FF+ is not only approached by patients, but also by doctors on a regular basis who want to leave the health department because of management that he said has completely abandoned services.
“It is clear that more is needed than the appointment of a new minister or a new Head of Department, as the legacy of mismanagement overwhelms individual role players. A comprehensive investigation and steadfast disciplinary action is needed,” he said. “Repeat offenders should not be tolerated in the department, not even in the most humble of positions.”
As Spotlight previously reported, the Northern Cape Department of Health has had several acting heads in the last three years and several senior officials have and are facing charges in court. The current Head of Department is Dr Alastair Kantani, who has been acting in the position since 8 September following the arrests of seven officials, including former head Dr Dion Theys who now occupies the post of Medical Director in the department. In a statement issued by the department on 13 September Lekwene said this action is informed by the constitutional responsibility to ensure relative stability in the delivery of healthcare services in the province.
The National Health Insurance (NHI) will further widen the inequality gap, put even more pressure on the already overburdened taxpayer and lead to an outflow of medical expertise should it be implemented. AfriForum has detailed these and other consequences of the NHI in a new research report.
In its report, the organisation details, among other things, the ideological basis of the NHI, the place it occupies in the ANC’s National Democratic Revolution (NDR), the economic consequences of the centralisation of health financing and the vagueness in the bill itself. Furthermore, the report provides an overview of centralised health systems in a number of other countries and how they compare or contrast with the economic and policy environment in South Africa.
One of the biggest issues with the NHI Bill is its funding. According to the report, four possible sources of income are currently being investigated that will have a negative impact on taxpayers – including payroll tax. This option entails that the government will require employers to recover a portion of their employees’ salaries which will then be remitted to the government – this on top of the deductions that are already recovered from employees’ salaries. South Africa’s marginal income tax is already higher than that of most other countries such as Canada, the USA and Namibia. Although this is the same as Australia, Switzerland and South Korea’s marginal income tax, South Africa has little in terms of service delivery to show for it.
The research finds in almost all the areas of investigation that NHI will be harmful to the economy and negative for the well-being of most South Africans and concludes that the bill should be rejected by parliament and opposed by the health sector.
According to Louis Boshoff, Campaign Officer at AfriForum, this report appears at a critical time where the parliamentary battle over the NHI Bill rages on and many misconceptions about it are circulating. “NHI is easily summarized incorrectly with slogans such as ‘free health care for all’, but the report takes a step back to obtain a more sober and objective picture, namely that the policy is expensive, unmotivated and unworkable,” says Boshoff.
The full report is available at www.jougesondheid.co.za, where the latest information on NHI is posted.
Atherosclerosis, caused by arterial wall plaque build-up, is a leading cause of death globally, particularly in the developed countries. Although the mortality rates for this condition fell dramatically during the 20th century, the incidence is now ever increasing. Unfortunately, despite the widespread impact of atherosclerosis – and efforts to curb it – data on the global and national trends of the disease is quite limited.
In a recent effort to address this knowledge gap, a research team from China led by Professor Rongchong Huang decided to conduct a detailed statistical analysis on the impact of atherosclerosis at the global and national levels by using GBD data. The study was published in the Chinese Medical Journal.
“It is unknown how global changes in pertinent controllable variables in recent years have affected the burden of atherosclerosis,” remarks Prof Huang.
The researchers analysed publicly available data from the Global Burden of Disease Study 2019 related to the three main clinical presentations of atherosclerosis, ischaemic heart disease (IHD), ischaemic stroke (IS), and peripheral arterial disease (PAD). The data collected, which spanned the period from 1990 to 2019, included participants of all ages with similar epidemiologic characteristics and in relative proximity, from 21 countries.
Overall, the study had four main goals. The first was to determine the global trends in terms of prevalence, mortality, and disability of the three conditions. The second goal was to identify the years that had the biggest shift in the trends of these indicators. Finally, the third and fourth goals were to analyze global trends based on age, gender, and socioeconomic factors and report global and national patterns, respectively.
According to the results, there was an overall increasing trend in the global incidence of the three clinical manifestations of atherosclerosis from 1990 to 2019. Notably, the main drivers for this rising incidence were adults aged 20–54. The researchers found this very concerning, given that atherosclerosis with such an early onset is usually caused by preventable factors, such as lack of exercise, dietary habits, and environmental pollution. However, the mortality rates and disability-adjusted life years for IHD and IS declined during this period across all age groups. This could indicate greater awareness regarding these conditions and their early symptoms, as well as advancements in clinical management.
Nonetheless, the global rise in the incidence of atherosclerosis over the past three decades is a serious problem that warrants special attention towards its root causes. In this regard, Prof Huang explains: “This rise can be attributed to a variety of factors. Firstly, global aging trends have led to a higher prevalence of the disease, given that age is a significant risk factor for atherosclerosis. Secondly, modern lifestyle habits, including high-fat diets, lack of exercise, smoking, and excessive alcohol consumption, have increased atherosclerosis risk. Lastly, there has been a rise in chronic diseases such as diabetes and hypertension, which are significant risk factors for atherosclerosis.”
The researchers also pointed out that the burden posed by atherosclerosis is increasing significantly in low- or middle-income countries, summarising key social and economic development indicators. China, which has the world’s greatest number of deaths due to cardiovascular diseases, is a prime example of this issue.
Taken together, the study paints a grim picture of global cardiovascular health, which is very concerning. “Overall, the burden of atherosclerosis-related disease is still not significantly decreasing and is even trending upward, especially in low- and middle-income countries and in younger populations,” says Prof Huang, “There is an urgent need for more targeted treatment and management in younger populations and in low-middle and middle-income countries.”
Hopefully, the results of these analyses will prompt decision makers, scientists, and medical professionals alike to increase their efforts towards fighting against atherosclerosis and its devastating consequences.
By Matshidiso Lencoasa and Dominic Brown for Spotlight
In the context of weak economic growth, lower-than-expected tax revenues, and the implementation of measures to reduce public spending, there is “rising panic” ahead of this year’s Medium Term Budget Policy Statement (MTBPS). The concern for health care provision is palpable as anticipated budget cuts threaten the country’s already fragile and understaffed public healthcare system. There is only one nurse for every 224 patients in the public health system, and over 5 000 nursing posts remain unfilled (something primarily attributed to funding constraints).
In times of poor economic performance, difficult policy choices and trade-offs arise, and it may be tempting for fiscal policymakers to slash public health spending. However, without meaningful consideration of the impact of these decisions on our people and our constitutional right to access healthcare, the MTBPS risks exacerbating the hardships faced in our country.
Austerity context
South Africa’s economic outlook has been riddled with challenges permeating our healthcare system. Over the past decade, the country’s economic growth has underperformed, falling in real terms from 2.3% in 2013 to 0.1% in 2023. National Treasury has responded to this with cuts to social spending, including healthcare. Public health is receiving fewer resources in real terms, and our government spends more on debt-servicing (R340.5 billion in the 2023/24 Budget) than on healthcare (R259.2 billion in the 2023/24 Budget). Moreover, healthcare’s allocation of R259 billion in 2023/24 was the same as last year’s allocation, meaning that the value of resources allocated to healthcare this year is eroded by Consumer Price Index (CPI) inflation, which was projected to be 4.9% at the time of the Budget Speech in February this year.
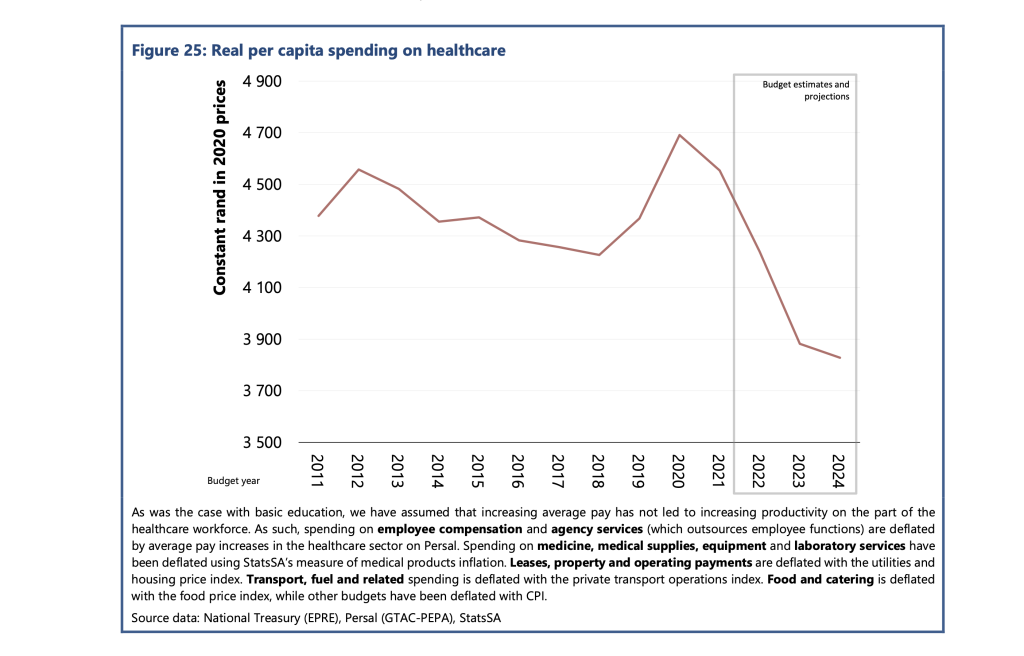
According to the Public Economy Project, the spending per healthcare user fell from approximately R4 600 in 2012 to R4 300 in 2018. PHOTO: Sourced from the Public Economy Project (PEP) Public services, government employment and the budget
Worse, this allocation needed to account for the rising demand projected for public healthcare services. Currently, about 84% of the population relies on the public health care system. This figure is projected to increase in response to population growth and rising unemployment making medical aid inaccessible for many in the country.
According to the Public Economy Project, after accounting for inflation and population growth, the spending per healthcare user fell from approximately R4600 in 2012 to R4300 in 2018. Based on current budget estimates, it is projected that real per capita public health spending will fall below R3 900 by 2024/25.
Implications for health care staffing
Although the 2023/24 budget proposed a measly 1.5% nominal increase to the public sector wage bill, President Cyril Ramaphosa approved a 3.8% increase for this year. However, Treasury’s cost containment measures have stipulated a hiring freeze for the rest of the 2023/24 financial year and no further allocations towards personnel expenditure. This is despite the Department of Health’s 2030 Human Resources for Health Strategy quantifying that 96 586 additional health workers are required to bolster the healthcare of all provinces to the same standard as the third-ranked province by 2025. This requires an additional cost of nearly R40 billion in total.
The real-life implications for South Africans are dire. Chris Hani Baragwanath Hospital – the largest hospital in Africa and the third largest hospital globally – faces significant staff shortages, cancelling almost 900 surgeries in 2022. The underpaid and overworked Chris Hani Baragwanath Hospital nurses have reported “pooling funds to buy patients bread.” Doctors at Nelson Mandela Bay’s Livingstone Tertiary Hospital have attributed “suboptimal, undignified patient care” to budget shortages and forecast higher medico-legal claims, which National Treasury described as a “sub-national risk”. However, budget measures that impede public health care’s ability to address staff shortages exacerbate the likelihood of errors by overstretched staff, worsening the medico-legal claims bill for health departments.
Gender and budget cuts
Health budget cuts disproportionately burden women. This burden is evident in the inordinate risk and prevalence of HIV that women face in the country. It is exacerbated by women’s higher and differentiated health needs (including those for reproductive and maternal health). Women-led households are 40% poorer, and unemployment is most prevalent among women. These socioeconomic factors make women more dependent on the public health system.
Budget cuts and underspending clearly have implications for gender equity in the country.
Furthermore, the Department of Health has recognised the healthcare workforce as a critical driver of inclusive economic growth and a means to create decent work for women, especially in rural and underserved communities. Over 90% of nurses in our public health system are women, and in our society of unequal gendered norms, it is also women who carry the care work burden in the home. Many will likely interpret any proposed MTBPS cuts without factoring gender equity implications as an under-appreciation of women’s labour in making a fragile healthcare system and society work.
A case for human rights budgeting
Although improving the country’s economic outlook is imperative, without consideration of the power that fiscal policy has in advancing human rights in the country, there is a likelihood of tabling an MTBPS that impedes the realisation of constitutionally guaranteed human rights in the country.
More than ever, our health system requires inculcation of human rights impact assessments as recommended by the UN Committee on Economic, Social and Cultural Rights, to which South Africa is a party. These assessments could compel policymakers to outline how the resources allocated will protect the right to access healthcare for all in the country, especially when budget cuts are considered. Including these considerations in budget policy may further advance meaningful public participation processes in fiscal policy.
Furthermore, a gender-responsive MTBPS is long overdue and a powerful means to protect the most vulnerable people in the country from reduced social investment. The health budget could be tagged to identify programmes with gender as a principal or significant objective and areas which would need to be protected and consideration of the gendered experience of healthcare to prevent fiscal policy from worsening gender inequities in the country. Budget policymakers should further promote the collection of gender-disaggregated data and establish indicators and benchmarks on gender and other socio-economic factors to advance a more equitable funding allocation.
Lastly, authentic public engagement will allow National Treasury and budget policymakers to solicit and table more equitable fiscal expansion alternatives. Increased public consultation could include extending the pre-budget consultations with the public.
Moreover, civil society organisations like the Institute of Economic Justice and the Alternative Information and Development Centre (AIDC) have proposed alternative approaches to fiscal constraints that could ensure sufficient resources to protect our frail public health system from threats to resource availability. These alternatives should be explored.
One strategy proposed is strengthening the country’s capacity to halt the significant revenue losses owing to to corporate tax abuses, including illicit financial flows (IFF) and base erosion and profit shifting (BEPS). IFF refers to the cross-border movement of illegally sourced funds while BEPS refers to when multinational companies shift the profits generated in South Africa to another jurisdiction that has lower or zero tax rates in order to minimise their tax burden.
The Financial Intelligence Centre estimates that between $15 billion and $25 billion is shifted out of our country to tax havens yearly. We call for greater urgency towards implementing publicly disclosed beneficial ownership registries based on country-by-country reporting and the automatic exchange of information, strengthening capital and exchange controls, and increasing South African Revenues Services (SARS) capacity to investigate corporations suspected to be involved in IFF and BEPS. These essential measures can contribute to curbing profit shifting, resulting in more than R100 billion in revenue each year.
The upcoming MTBPS will find National Treasury in a challenging position where various trade-offs will likely be made. In this harsh economic climate, if something has to give, it cannot be the constitutional right to health care for all in this country.
*Lencoasa is a Budget Researcher at SECTION27 and Steering Committee Member of the Budget Justice Coalition. Brown is Director of the Alternative Information and Development Centre and member of the Budget Justice Coalition.
By Robert Appelbaum & Prelisha Singh, Partners at Webber Wentzel
In Africa, dysfunctional governments are often unable to allocate sufficient funds for essential aspects of healthcare. This results in a shortage of new primary and specialised hospitals, little local pharmaceutical and medical device manufacture and the inability to train doctors beyond undergraduate level, creating a shortage of medical specialists.
In a recent seminar hosted by Invest Africa and moderated by Webber Wentzel, panelists Silven Chikengezha, Liza Eustace, Jen Pedersen, Jasen Smallbone and Dr Sue Tager, shared their insights on how to tackle the problems of financing healthcare in Africa, and building a pipeline of medical professionals who remain in Africa.
Funding
From the perspective of the IFC, the obvious need for greenfield hospitals in Africa is not sufficient to attract funding. To be attractive, projects need to meet certain criteria.
The first is that it must have a sponsor with experience in construction and operations. The second is that it has to have the potential to grow. It takes at least three years for a hospital to start making returns. Primary care is an identified area of potential growth on the continent, but it offers low margins so it needs to build up volumes. If the hospital is a primary healthcare facility that addresses an identified need in the local community, it is more likely to attract reliable footfall. But there is very little revenue in basic services like treating TB, AIDS and giving vaccination, so the facility should offer a range of affordable treatments.
The third criterion for any hospital project seeking funding is that it should have, or will be able to attract suitably qualified staff. Doctors like to work in complementary practice groups, so the hospital should be able to offer an attractive environment for medical professionals.
The next important issue is the certainty of cash flow. Although government-sourced revenue for the hospital can provide a steady income stream, governments can be slow payers. It is important to look at each government’s history of making timely payments. Commercial banks will also consider the affordability of the hospital’s services, given that a very small proportion of Africa’s population has medical insurance. In some countries, governments require employers to pay their employees’ medical bills, which provides a level of comfort to the banks. Technology can help to improve affordability, for example, innovations such as monitors that track the temperature of heat-sensitive medicines in transit, which reduces wastage.
A fifth critical issue for funders is the way the funding is structured. If a large hospital project is structured with 60-70% debt from its initial stages, it is likely to struggle to meet interest payments. It is better to start with a smaller facility that is scaleable, and structure the funding so that there is more equity than debt in the early years.
ABSA noted that they would seek strong equity holders before considering debt, and they will look carefully at who the main equity funders are. This is an area where the IFC and other Development Finance Institutions (DFIs) can play a role because they are usually willing to take the “first loss” risk, which encourages commercial banks to extend debt. Commercial banks take comfort from developers with strong balance sheets.
An emerging source of funding for healthcare projects in Africa (as well as other projects, such as in energy, water and education) are social impact bonds, in which an institutional funder will lend money to an implementer that can correctly manage a project that meets a need – often a need identified by the government. Corporates should be pooling their available funds to create scaleable projects that will make an impact.
If healthcare financing is intended to support existing service providers in Africa, it has to adapt to the capacity of what are often very small- to medium-sized businesses. These businesses, which may be anything from manufacturers of medical devices to providers of digi-health services, need far less than USD 20 million, so they tend to be ignored. But funding is essential to help established businesses build scale. This is another area where DFIs and commercial banks working together can help, as the DFI can provide the first loss facility which allows commercial banks to take risk on smaller clients.
Public-private partnerships
The pandemic made it clear that perceived obstacles between public and private entities in providing healthcare together could be overcome if there was the right will and people in the room.
Speakers discussed the Wits Donald Gordon Medical Centre as an example of a successful PPP, which could be replicated elsewhere. The Donald Gordon offers treatment to the private sector, and the derived profits are used to train medical students from Wits University, which is the public partner. The centre also performs liver transplants for all patients, both public and private. Mediclinic has a share in Donald Gordon but does not receive dividends. All profits are recycled back into the hospital.
A PPP model for the provision of healthcare needs partners who have similar levels of sophistication and can work together. Governments have to appreciate that the role of the private sector is not merely to bring money so that the government can continue running things the way they have always done. Private sector partners should be allowed to introduce the levels of efficiency in delivery that are typically found in the private sector.
Polygenic risk scores, which estimate a person’s disease risk based on thousands or millions of common genetic variants, perform poorly in screening and prediction of common diseases such as heart disease, according to a new study led by UCL (University College London) researchers. An extremely high number of individuals would need to be screened for each potential intervention, creating a significant burden on healthcare, while producing numerous false positive results.
It has been claimed that polygenic risk scores are set to transform the prediction and prevention of common diseases, with companies already set up to sell polygenic risk score testing services.
The new study, published in BMJ Medicine, examined 926 polygenic risk scores for 310 diseases. It found that, on average, only 11% of individuals who develop disease are identified, while at the same time 5% of people who do not develop the disease test positive. Unaffected people usually outnumber those affected which results in far more false than true positive predictions.
Lead author Professor Aroon Hingorani said: “Strong claims have been made about the potential of polygenic risk scores in medicine, but our study shows that this is not justified.
“We found that, when held to the same standards as employed for other tests in medicine, polygenic risk scores performed poorly for prediction and screening across a range of common diseases.”
For the new study, researchers looked at data available in an open-access database, the Polygenic Score Catalog, to determine what the detection rate and false positive rate of the scores would be if used in screening.
For breast cancer and coronary artery disease, the risk scores identified only 10% and 12% of eventual cases respectively, using a cut-off that resulted in 5% of unaffected individuals testing positive.
The researchers also investigated how polygenic risk scores would perform if used alongside conventional screening methods.
They found that, if used alongside conventional risk factors, several thousand people would need to have a polygenic risk score done to guide statin prescriptions to prevent one additional heart attack or stroke. The researchers noted that using age alone as a guide to statin prescription would be simpler and more effective at preventing heart attacks and strokes without the need for genetic testing.
They also found that adding polygenic risk scores as first stage screening to determine who should be prioritised for mammography would miss most women who later develop breast cancer and generate many false positives, adding to the burden on healthcare systems.
Co-author Professor Sir Nicholas Wald said: “It has been suggested that polygenic risk scores could be introduced early on to help prevent breast cancer and heart disease but, in the examples we looked at, we found that the scores contributed little, if any, health benefit while adding cost and complexity.”
In the paper, the researchers suggest regulation of commercial genetic tests based on polygenic risk scores to “protect the public from unrealistic expectations and already stretched public health systems from becoming overburdened by the management of false positive results”.
The researchers said consumers of commercial polygenic risk score tests should be informed of the detection rate and false positive rate of the polygenic risk scores as well as the absolute risk with and without a polygenic score result so they can better judge whether the test is useful.
Co-author Dr Jasmine Gratton said: “Polygenic risk scores seem attractive because genotyping is now inexpensive, the same for all diseases and is performed only once because a person’s genotype does not change. However, these features are irrelevant if the test is not useful.”
Professor Sir Nick Wald said: “Our results build on evidence that indicates that polygenic risk scores do not have a role in public health screening programmes.”
The researchers said the performance of polygenic risk scores was unlikely to change much as the variants with the strongest effect had already been identified.
Polygenic risk scores should not be confused with genetic testing for certain single gene mutations such as BRCA1 and BRCA2 which have an important role in screening for breast and ovarian cancer.
Discovering variants that are associated with a higher risk of disease is still crucial for drug development, the team emphasised, as the variants encode proteins that can be targeted with drugs that would be useful for everyone regardless of their genetic makeup.
Polygenic risk score testing is also one of the aims of the UK’s nationwide Our Future Health project.
For National Health Insurance to succeed in South Africa, a meaningful collaboration needs to take place between private and public health care so as to speed up the implementation of the initiative and overcome major obstacles.
This was the opinion of the five panellists who on the first day of the Hospital Association of South Africa conference in Cape Town spoke of how best the NHI could be rolled out by calling on private health care for assistance.
“’It’s fundamental to the economic growth that we so desperately need in South Africa, and a productive nation needs access to health care. So we do need to address the inequalities, we need to address the gap and do not need to preserve the status quo,” said Professor Roseanne Harris, of Discovery Health.
But a concern she raised is the risk of the introduction of a single funding model reliant on taxes, and the introduction of a monopoly market.
“And one of the implications of the bill is centralisation (of health care). There is a need for planning to ensure that it won’t have an unintended consequence of impacting service delivery and impacting on the rights of the healthcare personnel,” she added.
Harris said that both the private sector and public sector needed to go through a consultative process and that sustainable critical milestones needed to be put in place to hold the process to account.
Another panellist at the event Dr Simon Strachan of the South African Private Practitioners Forum (SAPPF), pointed out that the COVID pandemic showed how public and private health care could collaborate successfully. Here service agreements between the two entities were met and were focused solely on fighting the pandemic.
“So to create the way forward, what we need to be able to do is to have a very clear understanding of what it is we’re trying to achieve, that there is robust trust, and that there is a groundwork for sustainable collaboration,” he explained.
An urgent need for this collaboration he said was the recent introduction of Section 33 of the NHI bill, which in its present form would have health care professionals working for the state at a fee the state sets, with benefits not included.
A second issue he said was the need for a successful funding model that will be acceptable to all South Africans.
Economist Nicola Theron of FTI consulting told the audience that structures already in place and used in the private sector could make for a smoother transition for the NHI. In particular when it comes to issues like the pricing of medicines.
“We are now at a point with the current NHI that there are talks about the lowest possible price at a reasonable return for healthcare providers. There is no indication of what return means,” she said.
“But what we have is an existing system of pricing which has been developed over time, and which should form the basis of pricing going forward,” said Theron.
By not getting the pricing right could lead to investment leaving South Africa, she warned. She suggested in turn that it would be a better model to have multiple buyers that will stimulate competition.
Dr Ali Hamdulay, CEO, Metropolitan Health, said that a way forward would be to implement the suggestions that came out of the Health Marketing Inquiry that took a hard look at both the public and private health care systems, outlining the problems with both.
“So effectively by addressing the recommendations of the Health Market Inquiry you’re actually foster an environment of culture and direction to work towards universal health care,” said Hamdulay.
Barry Childs, of Insight Actuaries, said that while fundraising mechanisms in the public sector needed to be improved, the introduction of the NHI offers a great opportunity to reform the healthcare system.
“As much as we talk about the need for reform of the private sector side, there’s been no meaningful reform of the public sector for many decades. And the NHI is a wonderful opportunity for them to introduce some better, more responsive financing mechanisms.” he said.
But for NHI to ultimately provide the services it promises, Childs said South Africa’s economy needed to improve, and more jobs to be created.
South Africa’s sewage crisis has dire consequences for public health, waterways, and ecosystems. Outdated and poorly maintained wastewater infrastructure due to insufficient investment is one factor that results in poor waste management. The strain of rapid urbanisation with inadequate sanitation facilities in informal settlements and the exacerbating impact of climate change through increased rainfall events are also factors that contribute to poor waste management. Despite these challenges, there is room for optimism. Collaborative efforts between government and the private sector have the potential to address this dire situation, bringing forward practical, affordable solutions that hold the promise of a cleaner, healthier future for all communities.
A public health crisis: deadly waterborne diseases
South Africa’s persistent sewage crisis recently sparked a new cholera outbreak, primarily stemming from dysfunctional municipal sewage systems. Over 90% of the nation’s 824 treatment plants discharge untreated or partially treated sewage into our limited water resources. As of June 2023, the Department of Health had documented 1,045 suspected cholera cases across five provinces, with 197 cases confirmed by laboratory testing, directly linked to compromised water supply.
This crisis disproportionately impacts both urban and rural regions, where access to clean water and sanitation remains a pressing concern. Impoverished communities often rely on highly polluted water sources contaminated by sewage from overwhelmed treatment plants, further straining water purification efforts to meet safety standards. Recognising the intrinsic connection between drinking water quality and wastewater treatment is crucial, necessitating immediate attention and resolution.
However, a significant challenge faced by South African communities is the prohibitive cost of implementing waterborne sanitation solutions everywhere. With over four million latrines and roughly 50 million people lacking adequate sanitation, conventional waterborne systems are neither viable nor cost-effective comprehensive solutions.
South Africa’s water quality reports: red flags aplenty
The Blue Drop Report 2023, released in June 2023, paints a concerning picture of South Africa’s drinking water quality. While major cities maintain safe water, outlying areas face contamination and infrastructure challenges. Key statistics from the report reveal that the average Technical Site Assessment (TSA) score for water treatment systems is 69%, indicating partial functionality. About 15% of water supply systems are in poor or critical condition, with only 33% having Water Safety Plans, posing significant risks to water quality. Additionally, 50% of municipalities struggle with bad or poor microbiological water quality.
Wastewater and water wasting: two major risks
The 2023 Green Drop Report assesses wastewater treatment systems, showing a decline with an average score of 50%. Regional disparities persist, with Eastern Cape and Limpopo scoring lowest, while the Western Cape and Gauteng lead. The No Drop Report examines water losses, revealing a decline in overall performance in 2023, with an average score of 65%, which means that one-third of supplied water is wasted before it reaches consumers.
These reports collectively underline the urgent need to enhance drinking water quality in South Africa. Municipalities must focus on prioritising infrastructure maintenance and upgrades, implement risk-based water quality management, and strengthen compliance with standards. The Department of Water and Sanitation must offer more support to municipalities. Failing wastewater treatment facilities exacerbate drinking water purification, risking tap water safety and triggering further potential health and environmental crises. Therefore, they must take steps to safeguard water quality and address sewage infrastructure issues.
Rapid crisis intervention required
South Africa’s sewage crisis is a dire challenge that requires immediate action and innovative solutions. In recognising the inextricable link between sewage waste management and water quality, we must also acknowledge that this crisis cannot only be addressed by government without support from private sector industry leaders and experts. Portable water treatment package plants are available, along with small filtration and sterilisation systems for communities. Wastewater packaged treatment plants and solutions can help both alleviate immediate concerns and contribute to long-term sewage management strategies. Further neglecting the sewage problem and the critical maintenance of existing infrastructure will only deepen our water crisis. For this reason, the government needs to prioritise investment in sewage treatment infrastructure and implement practical, affordable solutions across all communities.
Mitigating South Africa’s sewage crisis
If municipal water supplies deteriorate further, sanitation specialists will be required to step in with a range of interventions. These extend from portable water treatment packaged plants to improve water quality at its source, to small-scale filtration and sterilisation systems designed for household use to ensure safe drinking water directly from the tap. From a contamination perspective, it is critical to reduce sewage entry into water courses, particularly in rural areas and informal settlements. This can be achieved through enhanced sanitation solutions, such as dry sanitation toilets, which are waste-contained alternatives to pit latrines.
From immediate relief to sustainable futures
Interventions will need to consider both immediate and long-term strategies. For short-term relief, containerised package plants can bolster sewage treatment facilities without the need for extensive infrastructure development, alleviating the strain on existing systems. Simultaneously, sanitation providers in the private sector can aid municipalities in implementing long-term solutions, including megalitre plans that feature efficiently packaged treatment plants. By adopting these smaller, cost-effective alternatives, it is possible to achieve the same capacity traditionally associated with larger concrete plants, in a fraction of the time to avert total system collapse and the impending health and economic catastrophes that would surely follow.