SARS-COV-2 has been very good at mutating to keep infecting people – so good that most antibody treatments developed during the pandemic are no longer effective. Now a team led by Stanford University researchers may have found a way to pin down the constantly evolving virus and develop longer-lasting treatments.
The researchers discovered a method to use two antibodies, one to serve as a type of anchor by attaching to an area of the virus that does not change very much and another to inhibit the virus’s ability to infect cells. This pairing of antibodies was shown to be effective against the initial SARS-CoV-2 virus that caused the pandemic and all its variants through omicron in laboratory testing. The findings are detailed in the journal Science Translational Medicine.
“In the face of an ever-changing virus, we engineered a new generation of therapeutics that have the ability to be resistant to viral evolution, which could be useful many years down the road for the treatment of people infected with SARS-CoV-2,” said Christopher O. Barnes, the study’s senior author, an assistant professor of biology.
An overlooked option
The team led by Barnes and first author Adonis Rubio, a doctoral candidate in the Stanford School of Medicine, conducted this investigation using donated antibodies from patients who had recovered from COVID-19. Analysing how these antibodies interacted with the virus, they found one that attaches to a region of the virus that does not mutate often.
This area, within the Spike N-terminal domain, or NTD, had been overlooked because it was not directly useful for treatment. However, when a specific antibody attaches to this area, it remains stuck to the virus. This is useful when designing new therapies that enable another type of antibody to get a foothold and attach to the receptor-binding domain, or RBD, of the virus, essentially blocking the virus from binding to receptors in human cells.
An illustration of the bispecific antibodies the Stanford-led research team developed to neutralise the virus that causes COVID-19. Named “CoV2-biRN,” these two antibodies work together by attaching to different areas of the virus.The bispecific antibodies target two areas of the virus: One attaches to the “NTD,” or Spike N-terminal domain, an area on the virus that does not change very much. This allows the second antibody to attach to the “RBD,” or receptor-binding domain, essentially preventing the virus from infecting human cells. | Christopher O. Barnes and Adonis Rubio using Biorender stock images
The researchers designed a series of these dual or “bispecific” antibodies, called CoV2-biRN, and in laboratory tests they showed high neutralisation of all the variants of SARS-CoV-2 known to cause illness in humans. The antibodies also significantly reduced the viral load in the lungs of mice exposed to one version of the omicron variant.
More research, including clinical trials, would have to be done before this discovery could be used as a treatment in human patients, but the approach is promising – and not just for the virus that causes COVID-19.
Next, the researchers will work to design bispecific antibodies that would be effective against all coronaviruses, the virus family including the ones that cause the common cold, MERS, and COVID-19. This approach could potentially also be effective against influenza and HIV, the authors said.
“Viruses constantly evolve to maintain the ability to infect the population,” Barnes said. “To counter this, the antibodies we develop must continuously evolve as well to remain effective.”
The World Health Organization (WHO) announced that it has updated its tracking system and working definitions for variants of SARS-CoV-2, to better reflect the current global variant landscape, to independently evaluate Omicron sublineages in circulation, and classify new variants more clearly when required.
Omicron variants now accounts for 98% of circulating SARS-CoV-2, and new variants will likely emerge from this genetic background. Based on its latest risk assessment [PDF], South Africa has reported a strong increase in XBB.1.5 from 1% in December 2022, to 10% in January 2023, and 76% as of the latest report from February 2023.
Based on comparisons of antigenic cross reactivity using animal sera, replication studies in experimental models of the human respiratory tract, and evidence from clinical and epidemiological studies in humans, WHO experts conclude that, compared to previous variants, Omicron represents the most divergent variant of concern (VOC) seen so far. Since its emergence, Omicron viruses have continued to evolve genetically and antigenically with an expanding range of sublineages, which so far have had all been characterised by evasion of existing population immunity and a preference to infect the upper respiratory tract (versus lower respiratory tract), as compared to pre-Omicron VOCs.
The previous system classified all Omicron sublineages as part of the Omicron VOC and was not detailed enough to compare new descendent lineages with altered phenotypes to the Omicron parent lineages (BA.1, BA.2, BA.4/BA.5). So, WHO variant tracking system will consider the classification of Omicron sublineages independently as variants under monitoring (VUMs), variants of interest (VOIs), or VOCs.
WHO is also updating the working definitions for VOCs and VOIs. The main update consists in making the VOC definition more specific, to include major SARS-CoV-2 evolutionary steps that require major public health interventions.
In addition, going forward, WHO will assign Greek labels for VOCs, and will no longer do so for VOIs.
With these changes factored in, Alpha, Beta, Gamma, Delta as well as the Omicron parent lineage (B.1.1.529) are considered previously circulating VOCs. WHO has now classified XBB.1.5 as a VOI.
WHO emphasizes that these changes do not imply that the circulation of Omicron viruses no longer pose a threat to public health. Rather, the changes have been made in order to better identify additional or new threats over and above those posed by the current Omicron viruses in circulation.
Despite intensive public health efforts to grind the COVID-19 pandemic to a halt, the recent emergence of the highly transmissible, extensively drug-resistant and profoundly immune system-evading XBB.1.5 SARS-CoV-2 subvariant is putting the global community on edge.
XBB.1.5 has also been detected in municipal wastewater systems in the United States, Europe and other places.
How likely is XBB.1.5 to cause serious illness?
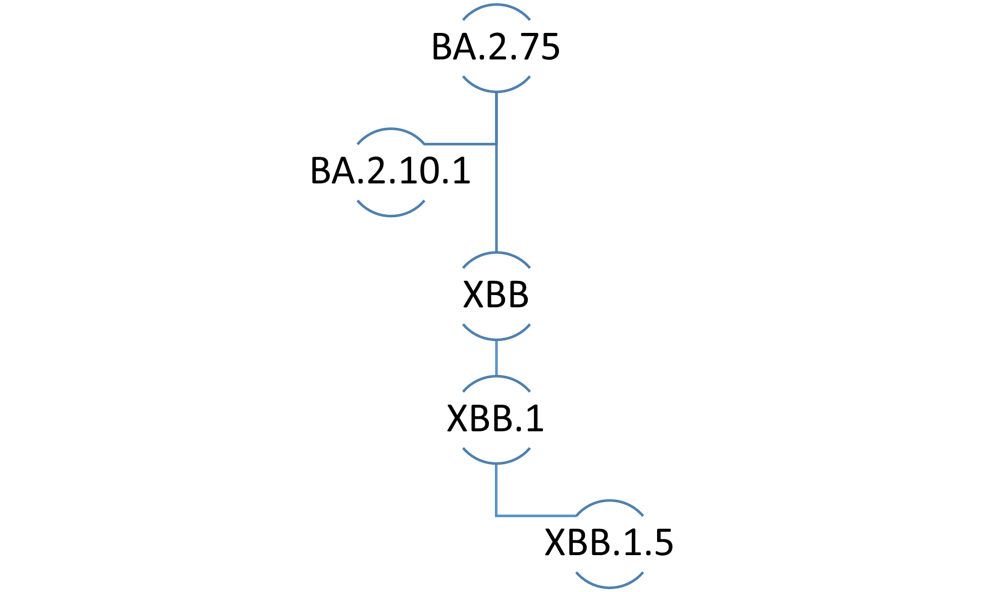
The XBB lineage emerged following natural co-infection of a human host with two Omicron subvariants, namely BA.2.10.1 and BA.2.75. (Shutterstock)
There is limited data about the ability of XBB.1.5 to cause serious illness. According to the World Health Organization, XBB.1.5 does not have any specific mutations that make it any more dangerous than its ancestral subvariants.
Nonetheless, XBB.1.5 is perceived as being equally capable of causing serious illness in elderly and immunocompromised persons compared to previous Omicron subvariants of concern.
Are current mRNA vaccines effective against XBB.1.5?
XBB.1.5 and XBB.1 are the Omicron subvariants with the greatest immune-evasive properties. Therefore, one of the most contentious issues surrounding XBB.1.5 relates to the degree of protection afforded by currently available mRNA vaccines, including the latest bivalent booster formulations.
Researchers from the University of Texas determined that first-generation and bivalent mRNA booster vaccines containing BA.5 result in lacklustre neutralizing antibody responses against XBB.1.5. A report (yet to be peer reviewed) from investigators at the Cleveland Clinic found that bivalent vaccines demonstrate only modest (30 per cent) effectiveness in otherwise healthy non-elderly people when the variants in the vaccine match those circulating in the community.
Furthermore, some experts believe the administration of bivalent boosters for the prevention of COVID-19 illness in otherwise healthy young individuals is not medically justified nor cost-effective.
In contrast, public health experts from Atlanta, Ga. and Stanford, Calif. reported that although the neutralizing antibody activity of bivalent booster vaccines against XBB.1.5 is 12 to 26 times less than antibody activity against the wild-type (original) SARS-CoV-2 virus, bivalent vaccines still perform better than monovalent vaccines against XBB.1.5.
However, investigators from Columbia University in New York found that neutralizing antibody levels following bivalent boosting were up to 155–fold lower against XBB.1.5 compared to levels against the wild-type virus following monovalent boosting.
This suggests that neither monovalent nor bivalent booster vaccines can be relied upon to provide adequate protection against XBB.1.5.
How can you protect yourself against XBB.1.5?
Standard infection control precautions including indoor masking, social distancing and frequent handwashing are effective measures against XBB.1.5 and other subvariants of concern. THE CANADIAN PRESS/Graham Hughes
The rapid evolution of SARS-CoV-2 continues to pose a challenge for the management of COVID-19 illness using available preventive and therapeutic agents. Of note, all currently available monoclonal antibodies targeting the spike protein of SARS-CoV-2 are deemed to be ineffective against XBB.1.5.
Antiviral medicines such as remdesivir and Paxlovid may be considered for the treatment of eligible infected patients at high risk of progressing to severe disease.
Standard infection control precautions including indoor masking, social distancing and frequent handwashing are effective measures that can be employed for personal and population protection against XBB.1.5 and other subvariants of concern.
Although bivalent boosters may be considered for elderly, immunocompromised and other risk-averse individuals, their effectiveness in preventing COVID-19 illness due to XBB.1.5 remains uncertain.
The ‘Kraken’ label for XBB.1.5 is currently in vogue on social media sites and news outlets, and the nicknames ‘Gryphon’ and ‘Hippogryph’ have been used to denote the ancestral subvariants XBB and XBB.1, respectively. Kraken refers to a mythological Scandinavian sea monster or giant squid, Gryphon (or Griffin) refers to a legendary creature that is a hybrid of an eagle and a lion, while Hippogryph (or Hippogriff) is a fictitious animal hybrid of a Gryphon and a horse.
Notwithstanding their potential utility as memory aids, the use of nicknames or acronyms in formal scientific discussions should be avoided.
Sameer Elsayed is Professor of Medicine, Pathology & Laboratory Medicine, and Epidemiology & Biostatistics at Western University.
On December 1, Charité — Universitätsmedizin Berlin reported new findings on the origins of the SARS-CoV-2 variant Omicron, one of which was a “stepwise” emergence of the variant across Africa rather than the accepted scenario of it emerging in a single area around South Africa.
In light of new findings of contaminated samples used in the research, the team led by Prof Jan Felix Drexler has now retracted the article, which was published in the journal Science.
The new findings mean that some of the article’s statements are no longer provable beyond reasonable doubt, and the authors retracted their article in line with sound scientific procedure.
In the article entitled “Gradual emergence followed by exponential spread of the SARS-CoV-2 Omicron variant in Africa”, researchers came to the conclusion that the Omicron variant of SARS-CoV-2 emerged in western Africa a few months prior its eventual discovery in South Africa in early November. Shortly after the article was published, other scientists, such as SA’s Dr Tulio de Oliveira, called into question the plausibility of the genome sequences analysed in the study. Subsequent analysis of residual samples found evidence of contamination, the source of which can no longer be traced.
One of the article’s messages — that viruses with Omicron sequence signatures existed across the continent before Omicron was officially detected in South Africa — is based on collective data from PCR analysis done independently by laboratories in several African countries. However, the conclusive reconstruction of the virus’s evolution, another of the article’s key messages, is likely to be affected by sequence contamination not detected before analysis.
The contamination also makes it impossible to correct the analyses retrospectively in due time, because this would require additional analyses of thousands of patient samples from Africa that may not be available in sufficient quantity and quality. Therefore, in agreement with all the authors, the entire article is being retracted. The research group that ran the project is currently carrying out an evaluation and review of the analyses.
Prof Drexler and his team expressed regret for the incident and gratitude to their international colleagues for flagging the potential problems following the article’s publication.
A widely reported study published in Science that presented evidence for a distributed, ‘stepwise’ origin for Omicron across the African continent has drawn criticism from a number of prominent scientists.
Dr Tulio Oliveira, the director of CERI (Centre for Epidemic Response & innovation) and KRISP (KZN Research Innovation & Sequencing Platform) was one of these scientists expressing their doubts over Twitter.
Dr Oliveira tweeted that, like many other scientists, he was sceptical of the Science paper’s narrative of a stepwise emergence of Omicron in Africa.
“First, the ‘fishing’ of intermediates in Africa should also have been performed in Europe and the USA, which were the regions of the world that introduced the majority of Omicron lineages to Africa -“
He also questioned the accuracy of their results due to possible contamination, and also the strength of their analyses, noting that phylogenetic analyses are weak.
For his fourth point, he says that “the Benin sequences could be recombinants of Delta and Omicron, real recombination, or recombination through contamination of the sequencing process.” He was unable to check for the prevalence of mutations.
He also makes a very simple observation regarding the timing of waves: if Omicron arose first in West Africa, why then did South Africa experience the Omicron wave before them?
The paper was also not presented as a preprint to allow for the research community to give feedback and improved the manuscript, a criticism echoed by biologist and physicist Richard Neher.
“Lastly, the results presented do not reject any of the three hypotheses of Omicron evolution (i.e. unsampled location, immune suppressed individual, animal reservoir).”
Nevertheless, he says that “I have many colleagues and collaborators in this paper and would like to recognize that the allele qPCR system to identify BA.1 is a great tool. Also that their mutation analyses are also good.”
Seemingly out of nowhere, the Omicron variant was first detected in South Africa and rapidly spread around the world. Now, a study published in the journal Science shows that Omicron’s predecessors existed on the African continent long before cases were first identified, suggesting that Omicron emerged gradually over several months in different countries across Africa.
Since the beginning of the pandemic, the coronavirus has been constantly changing. The biggest leap seen in the evolution of SARS-CoV-2 to date was observed by researchers a year ago, when a variant was discovered that differed from the genome of the original virus by more than 50 mutations. First detected in a patient in South Africa in mid-November 2021, the variant later named Omicron BA.1 spread to 87 countries around the world within just a few weeks. By the end of December, it had replaced the previously dominant Delta variant worldwide.
Since then, speculations about the origin of this highly transmissible variant have centred around two main theories: Either the coronavirus jumped from a human to an animal where it evolved before infecting a human again as Omicron, or the virus survived in a person with a compromised immune system for a longer period of time and that’s where the mutations occurred. A new analysis of COVID samples collected in Africa before the first detection of Omicron now casts doubt on both these hypotheses.
The analysis was carried out by an international research team led by Prof Jan Felix Drexler, a scientist at the Institute of Virology at Charité and the German Center for Infection Research (DZIF). Other key partners in the European-African network included Stellenbosch University in South Africa and the Laboratory of Viral Hemorrhagic Fever (LFHB) in Benin. The scientists started by developing a special PCR test to specifically detect the Omicron variant BA.1. They then tested more than 13 000 respiratory samples from COVID9 patients that had been taken in 22 African countries between mid-2021 and early 2022. In doing so, the research team found viruses with Omicron-specific mutations in 25 people from six different countries who contracted COVID in August and September 2021 – two months before the variant was first detected in South Africa.
To learn more about Omicron’s origins, the researchers also sequenced the viral genome of some 670 samples. Such sequencing makes it possible to detect new mutations and identify novel viral lineages. The team discovered several viruses that showed varying degrees of similarity to Omicron, but they were not identical.
“Our data show that Omicron had different ancestors that interacted with each other and circulated in Africa, sometimes concurrently, for months,” explains Prof Drexler. “This suggests that the BA.1 Omicron variant evolved gradually, during which time the virus increasingly adapted to existing human immunity.” In addition, the PCR data led the researchers to conclude that although Omicron did not originate solely in South Africa, it first dominated infection rates there before spreading from south to north across the African continent within only a few weeks.
“This means Omicron’s sudden rise cannot be attributed to a jump from the animal kingdom or the emergence in a single immunocompromised person, although these two scenarios may have also played a role in the evolution of the virus,” says Prof Drexler.
“The fact that Omicron caught us by surprise is instead due to the diagnostic blind spot that exists in large parts of Africa, where presumably only a small fraction of SARS-CoV-2 infections are even recorded. Omicron’s gradual evolution was therefore simply overlooked. So it is important that we now significantly strengthen diagnostic surveillance systems on the African continent and in comparable regions of the Global South, while also facilitating global data sharing. Only good data can prevent policymakers from implementing potentially effective containment measures, such as travel restrictions, at the wrong time, which can end up causing more economic and social harm than good.”
A study of COVID transmissions in a Taiwanese quarantine hotel revealed that SARS-CoV-2 can spread through cracks in walls and floors, according to findings published in Emerging Infectious Diseases.
The researchers investigated a cluster of SARS-CoV-2 infections in a quarantine hotel in Taiwan in December 2021. This happened amidst a succession of outbreaks in quarantine hotels involving the Omicron variant. The cluster involved three patients who lived in nonadjacent rooms on different floors, and who had no direct contact during their stay.
All three had tested negative by RT-PCR for SARS-CoV-2 within 72 hours before arrival to Taiwan and by deep-throat saliva RT-PCR upon arrival at the airport. None had left their rooms at any point during the stay in the hotel. No other guest or staff member at the hotel had tested positive since the month prior to the start of the investigation.
By directly exploring the space above the room ceilings, the researchers revealed residual tunnels, wall defects, and truncated pipes between their rooms. To see how the rooms were interconnected, they performed a simplified tracer-gas experiment, using ethanol. Aerosol transmission through structural defects in floors and walls in this poorly ventilated hotel was the most likely route of virus transmission.
This event demonstrated the high transmissibility of Omicron variants, even across rooms and floors, through structural defects. “Our findings emphasise the importance of ventilation and integrity of building structure in quarantine facilities,” the authors concluded.
The emerging Omicron variant BA.2.75.2 largely evades neutralising antibodies in the blood and resists several monoclonal antibody antiviral treatments, according to a study published in the journal The Lancet Infectious Diseases. The findings suggest a risk of increased COVID infections in the northern hemisphere’s winter, unless the new updated bivalent vaccines help to boost immunity in the population.
“While antibody immunity is not completely gone, BA.2.75.2 exhibited far more dramatic resistance than variants we’ve previously studied, largely driven by two mutations in the receptor binding domain of the spike protein,” said the study’s corresponding author Ben Murrell, assistant professor at the Department of Microbiology, Tumor and Cell Biology, Karolinska Institutet.
The study shows that antibodies in random serum samples from 75 blood donors in Stockholm were approximately only one-sixth as effective at neutralising BA.2.75.2 compared with the now-dominant variant BA.5. The serum samples were collected at three time points: in November 2021 before the emergence of Omicron, in April 2022 after a large wave of infections in the country, and at the end of August to early September after the BA.5 variant became dominant.
The researchers found that only one of the clinically available monoclonal antibody treatments that were tested, bebtelovimab, managed to effectively neutralise the new variant.
BA.2.75.2 is a mutated version of another Omicron variant, BA.2.75. Since it was first discovered earlier this fall, it has spread to several countries but so far represents only a minority of registered cases.
A possible increase in infections
“We now know that this is just one of a constellation of emerging variants with similar mutations that will likely come to dominate in the near future,” Ben Murrell says, adding “we should expect infections to increase this winter.”
Some questions remain. It is unclear whether these new variants will drive an increase in hospitalisation rates. Also, while current vaccines have, in general, had a protective effect against severe disease for Omicron infections, there is not yet data showing the degree to which the updated COVID vaccines provide protection from these new variants. “We expect them to be beneficial, but we don’t yet know by how much,” Ben Murrell says.
New research shows that the Omicron variants cause significantly lower levels of blood clotting, thereby providing further evidence for the link between the severity of the disease and the prevalence of persistent micro blood clots in individuals with acute and Long COVID.
Prof Resia Pretorius, a researcher in the Department of Physiological Sciences at Stellenbosch University (SU), South Africa, first made this connection late in 2020 when she detected small amyloid-like blood clots in the plasma of individuals suffering from COVID. Amyloids are a type of protein associated with various inflammatory diseases. As part of a long-term collaboration with Prof Douglas Kell from the University of Liverpool, they showed that these micro clots contained pro-inflammatory molecules. The results of both studies were published in the journal Cardiovascular Diabetology, in 2020 and 2021.
These insoluble micro clots inhibit or may temporarily block blood flow to capillaries and hence impair oxygen transfer to tissues. At present, they believe that this oxygen impairment in various parts of the body can account for most of the symptoms of Long COVID, such as constant fatigue, shortness of breath, brain fog, joint and muscle pain.
Prof Resia Pretorius
Prof Pretorius said the persistent prevalence of micro clots may have significant clinical value: “Our findings suggest that hypercoagulation and vascular damage are key role players causing the wide range of symptoms we see in patients with Long COVID. There is a golden thread running through pathologies noted in post-viral syndromes such as Long COVID.”
More recently, Prof Pretorius and Prof Kell worked with a team of clinicians in South Africa and the United States, to ascertain whether the difference in the degree of clotting between different viral strains of the SARS-CoV-2 virus provides a plausible explanation for the relatively low severity of the Omicron variants during acute COVID infection.
While the earlier variants caused severe disease and critically ill patients, the heavily mutated Omicron variants have been shown to have milder symptoms, most commonly a runny nose, rhinitis headaches, fatigue (from mild to severe), sneezing and a sore throat.
For the purposes of the study, they revisited data and blood samples from stored blood samples from ten patients with COVID due to the Beta and Delta variants between October 2020 and September 2021 before the patients received treatment.
The team also collected blood from patients infected with the Omicron variants. In all ten samples it was found that the Omicron samples presented with a significantly lower total amount of microclots compared to earlier Beta and Delta variants.
In a recent webinar on the topic, Dr Mark Walsh, an emergency medicine physician at the Saint Joseph Regional Medical Center in the United States of America, said the foundational work of Profs Pretorius and Kell has helped them to explain the clotting complications of COVID-induced coagulopathies (CAC) of patients with acute COVID. He is also one of the co-authors on the article.
“We could not understand why patients with CAC would clot and bleed at the same time. We now have the pathophysiological foundation for a point-of-care bedside medicine approach, based on the foundations of excellent research,” he said.
Early in the pandemic, Dr Walsh and his team of emergency physicians in the USA, developed a protocol to provide safe anticoagulation treatment to severely ill COVID patients. The team was guided by thromboelastography, a point-of-care protocol to monitor bleeding and clotting.
According to Prof Kell, more importantly, the findings are consistent with the view that these insoluble micro clots are not a side-effect of COVID-19, but a part of how the disease develops. However, he warned, we do not yet know how this will impact or relate to other post-viral syndromes such as Long-COVID, myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), post-Zika or post-Dengue diseases.
The paper, titled “Relative hypercoagulopathy of the SARS-CoV-2, Beta and Delta variants when compared with the less severe Omicron variants is related to TEG parameters, the extent of fibrin amyloid microclots, and the severity of clinical illness” is in press in the journal Seminars in Thrombosis and Hemostasis, and a preprint is available at https://www.researchsquare.com/article/rs-1970823/v1
The webinar, “COVID-induced Coagulopathy (CAC): The clot thickens…or not?” is presented by Dr Mark Walsh, Prof Resia Pretorius and Prof Douglas Kell, and moderated by Dr Asad Khan. It is available at https://youtu.be/yyf7xunWydM
South African researchers have found that, compared to Omicron BA.1 and earlier infections, those caused by Omicron BA.4 and BA.5 do not have an increased risk of hospitalisation for severe disease or death.
The study, which appears online in the medRxiv server, aimed to compare clinical severity of Omicron BA.4/BA.5 infection with BA.1 and earlier variant infections among laboratory-confirmed SARS-CoV-2 cases in the Western Cape, South Africa, using timing of infection to infer the lineage/variant causing infection.
In their study, the researchers included public sector patients aged 20 years or older with laboratory-confirmed COVID between 1 and 21 May 2022 (for the BA.4/BA.5 wave) and equivalent prior wave periods. They compared the risk for death and severe hospitalisation/death (all within 21 days of diagnosis), adjusting for for demographics, comorbidities, admission pressure, vaccination and prior infection.
Comparing 3793 patients from the BA.4/BA.5 wave and 190 836 patients from previous waves the risk of severe hospitalisation or death was similar in the BA.4/BA.5 and BA.1 waves (adjusted hazard ratio [aHR] 1.12). Both Omicron waves had a lower risk of severe outcomes than previous waves. They also found that both prior infection (aHR 0.29) and vaccination (aHR 0.17; 0.40 for boosted vs no vaccine) were protective.
Overall, the researchers found that COVID disease severity was similar for the BA.4/BA.5 and BA.1 periods in the context of growing immunity against SARS-CoV-2 due to prior infection and vaccination, which were both strongly protective.