New research in patients undergoing neurosurgery reveals the unique human ability to conceptualise numbers may be rooted deep within the brain. In good news for those who are stumped by maths, the results of the study by Oregon Health & Science University involving neurosurgery patients suggests new possibilities for tapping into those areas to improve learning.
“This work lays the foundation to deeper understanding of number, math and symbol cognition – something that is uniquely human,” said senior author Ahmed Raslan, MD, professor and chair of neurological surgery in the OHSU School of Medicine. “The implications are far-reaching.”
Raslan and co-authors recruited 13 people with epilepsy who were undergoing a commonly used surgical intervention to map the exact location within their brains where seizures originate, a procedure known as stereotactic electroencephalography. During the procedure, researchers asked the patients a series of questions that prompted them to think about numbers as symbols (for example, 3), as words (“three”) and as concepts (a series of three dots).
As the patients responded, researchers found activity in a surprising place: the putamen.
Located deep within the basal ganglia above the brain stem, the putamen is an area of the brain primarily associated with elemental functions, such as movement, and some cognitive function, but rarely with higher-order aspects of human intelligence like solving calculus. Neuroscientists typically ascribe consciousness and abstract thought to the cerebral cortex, which evolved later in human evolution and wraps around the brain’s outer layer in folded grey matter.
“That likely means the human ability to process numbers is something that we acquired early during evolution,” Raslan said. “There is something deeper in the brain that gives us this capacity to leap to where we are today.”
Researchers also found activity as expected in regions of the brain that encode visual and auditory inputs, as well as the parietal lobe, which is known to be involved in numerical and calculation-related functions.
From a practical standpoint, the findings could prove useful in avoiding important areas during surgeries to remove tumors or epilepsy focal points, or in placing neurostimulators designed to stop seizures.
“Brain areas involved in processing numbers can be delineated and extra care taken to avoid damaging these areas during neurosurgical interventions,” said lead author Alexander Rockhill, PhD, a postdoc in Raslan’s lab.
Researchers credited the patients involved in the study.
“We are extremely grateful to our epilepsy patients for their willingness to participate in this research,” said co-author Christian Lopez Ramos, MD, neurosurgical resident at OHSU. “Their involvement in answering our questions during surgery turned out to be the key to advancing scientific understanding about how our brain evolved in the deep past and how it works today.”
Indeed, the study follows previous lines of research involving mapping of the human brain during surgery.
“I have access to the most valuable human data in nature,” Raslan said. “It would be a shame to miss an opportunity to understand how the brain and mind function. All we have to do is ask the right questions.”
In the next stage of this line of research, Raslan anticipates discerning areas of the brain capable of performing other higher-level functions.
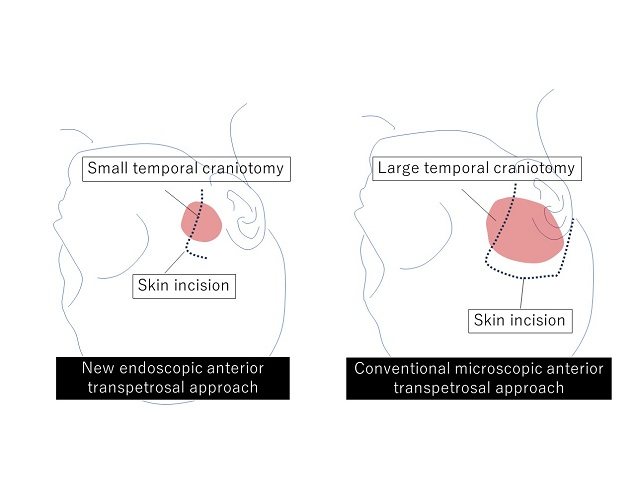
Tumours arising in the base of the skull are among the most difficult to remove in neurosurgery. The current treatment method is to perform surgical removal by what is known as the microscopic anterior transpetrosal approach (ATPA). Seeking to lessen the risk of damage and postoperative complications, as the skull base is densely packed with nerves, blood vessels, and other tissues, not to mention the brain stem, an Osaka Metropolitan University medical research team is taking a new approach.
Led by Dr Hiroki Morisako, a lecturer in the Graduate School of Medicine’s Department of Neurosurgery, and its department head Professor Takeo Goto, the team has developed a minimally invasive surgical technique called a purely endoscopic subtemporal keyhole ATPA. The team members write in The Journal of Neurosurgery that this is, to their knowledge, the first time this procedure to remove lesions in the skull base region known as the petrous apex has been described in an article.
Diagram of skin incision and extent of craniotomy. New endoscopic neurosurgery approach does not require a large craniotomy, so the result is a smaller scar. Credit: Osaka Metropolitan University
The endoscopic technique means a smaller area of the skull needs to be surgically opened compared to the microscopic approach, an average of only 11.2 cm² versus 33.9 cm². The risk of damage to the brain is also reduced.
The team performed 10 neurosurgeries using their method from 2022 to 2023 at Osaka Metropolitan University Hospital and compared the results to 13 surgeries using the microscopic ATPA from 2014 to 2021. In terms of operative time, the endoscopic approach reduced it noticeably, from an average of 410.9 minutes to 252.9 minutes. Similarly, blood loss lessened from a mean of 193 ml to 90 ml. The degree of tumour resection (surgical removal) was just as high as the microscopic method, while neurological functions were preserved at a rate equal to or higher than with the conventional approach.
“Comparison of the new endoscopic method and the conventional microscopic method showed no significant difference in tumour resection rate or in the ability to perform daily activities before and after surgery, with the new endoscopic approach resulting in shorter operative times and less blood loss,” Professor Goto stated. “The widespread use of this surgical procedure is expected to improve the treatment results of brain tumours in the base of the skull, not only in Japan but also worldwide.”
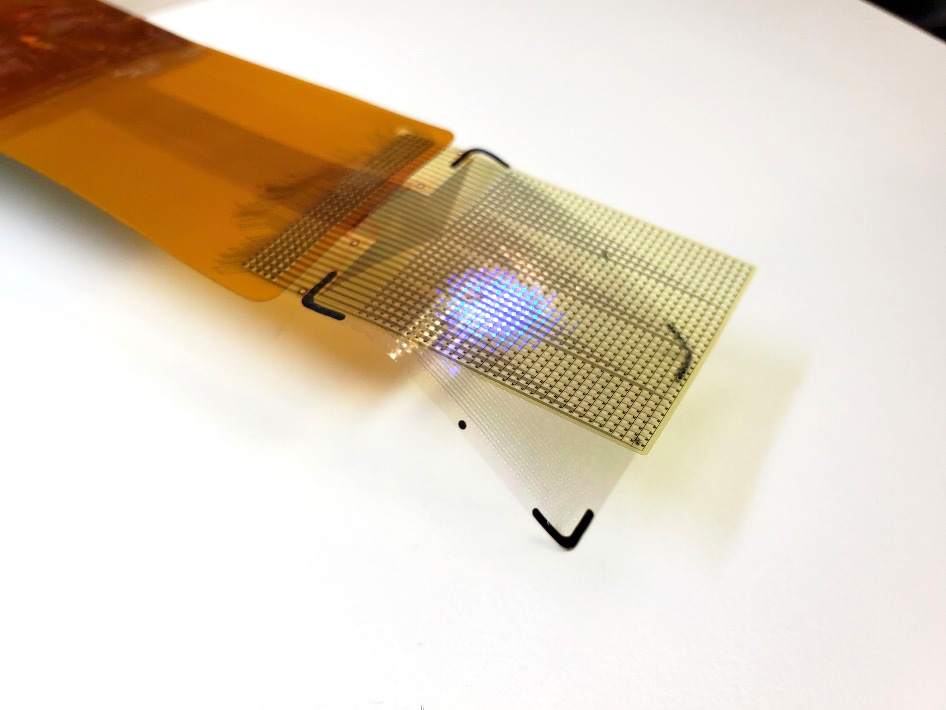
The device represents a huge leap ahead guide neurosurgeonswith visualised brain activity
The device’s LEDs can light up in several colors. This allows surgeons to see which areas they need to operate on. It allows them to track brain states during surgery, including the onset of epileptic seizures. Credit: UCSF
A thin film that combines an electrode grid and LEDs can both track and produce a visual representation of the brain’s activity in real-time during surgery-a huge improvement over the current state of the art. The device is designed to provide neurosurgeons visual information about a patient’s brain to monitor brain states during surgical interventions to remove brain lesions including tumours and epileptic tissue.
Each LED in the device represents the activity of a few thousand neurons. In a series of proof-of-concept experiments in rodents and large non-primate mammals, researchers showed that the device can effectively track and display neural activity in the brain corresponding to different areas of the body. In this case, the LEDs developed by the team light up red in the areas that need to be removed by the surgeon. Surrounding areas that control critical functions and should be avoided show up in green.
The study also showed that the device can visualise the onset and map the propagation of an epileptic seizure on the surface of the brain. This would allow physicians to isolate the ‘nodes’ of the brain that are involved in epilepsy. It also would allow physicians to deliver necessary treatment by removing tissue or by using electrical pulses to stimulate the brain.
“Neurosurgeons could see and stop a seizure before it spreads, view what brain areas are involved in different cognitive processes, and visualise the functional extent of tumour spread. This work will provide a powerful tool for the difficult task of removing a tumour from the most sensitive brain areas,” said Daniel Cleary, one of the study’s coauthors, a neurosurgeon and assistant professor at Oregon Health and Science University.
The device was conceived and developed by a team of engineers and physicians from University of California San Diego and Massachusetts General Hospital (MGH) and was led by Shadi Dayeh, the paper’s corresponding author and a professor in the Department of Electrical and Computer Engineering at UC San Diego.
Protecting critical brain functions
During brain surgery, physicians need to map brain function to define which areas of the organ control critical functions and can’t be removed. Currently, neurosurgeons work with a team of electrophysiologists during the procedure. But that team and their monitoring equipment are located in a different part of the operating room.
Brain areas that need to be protected and those that need to be operated on are either marked by electrophysiologists on a paper that is brought to the surgeon or communicated verbally to the surgeon, who then places sterile papers on the brain surface to mark these regions.
“Both are inefficient ways of communicating critical information during a procedure, and could impact its outcomes,” said Dr Angelique Paulk of MGH, who is a co-author and co-inventor of the technology.
In addition, the electrodes currently used to monitor brain activity during surgery do not produce detailed fine grained data. So surgeons need to keep a buffer zone, known as resection margin, of 5 to 7mm around the area they are removing inside the brain.
This means that they might leave some harmful tissue in. The new device provides a level of detail that would shrink this buffer zone to less than 1mm.
“We invented the brain microdisplay to display with precision critical cortical boundaries and to guide neurosurgery in a cost-effective device that simplifies and reduces the time of brain mapping procedures,” said Shadi Dayeh, the paper’s corresponding author and a professor in the Department of Electrical and Computer Engineering at the UC San Diego Jacobs School of Engineering.
Researchers installed the LEDs on top of another innovation from the Dayeh lab, the platinum nanorod electrode grid (PtNRGrid). Using the PtNRGrids since 2019, Dayeh’s team pioneered human brain and spinal cord mapping with thousands of channels to monitor brain neural activity.
They reported early safety and effectiveness results in a series of articles in Science Translational Medicine in 2022 in tens of human subjects.
(New sensor grids record human brain signals with record breaking resolution and Microelectrode array can enable safer spinal cord surgery) — ahead of Neuralink and other companies in this space.
The PtNRGrid also includes perforations, which enable physicians to insert probes to stimulate the brain with electrical signals, both for mapping and for therapy.
How it’s made
The display uses gallium nitride-based micro-LEDs, bright enough to be seen under surgical lights. The two models built measures 5mm or 32mm on a side, with 1024 or 2048 LEDs. They capture brain activity at 20 000 samples a second, enabling .
“This enables precise and real-time displays of cortical dynamics during critical surgical interventions,” said Youngbin Tchoe, the first author and co-inventor, formerly a postdoc in the Dayeh group at UC San Diego and now an assistant professor at Ulsan National Institute of Science and Technology.
In addition to the LEDs, the device includes acquisition and control electronics as well as software drivers to analyse and project cortical activity directly from the surface of the brain.
“The brain iEEG-microdisplay can impressively both record the activity of the brain to a very fine degree and display this activity for a neurosurgeon to use in the course of surgery. We hope that this device will ultimately lead to better clinical outcomes for patients with its ability to both reveal and communicate the detailed activity of the underlying brain during surgery,” said study coauthor Jimmy Yang, a neurosurgeon and assistant professor at The Ohio State University.
Next steps
Dayeh’s team is working to build a microdisplay that will include 100 000 LEDs, with a resolution equivalent to that of a smartphone screen – for a fraction of the cost of a high-end smartphone. Each LED in those displays would reflect the activity of a few hundred neurons.
These brain microdisplays would also include a foldable portion. This would allow surgeons to operate within the foldable portion and monitor the impact of the procedure as the other, unfolded portion of the microdisplay shows the status of the brain in real time.
Researchers are also working on one limitation of the study – the close proximity of the LED sensors and the PtNRGrids led to a slight interference and noise in the data.
The team plans to build customised hardware to change the frequency of the pulses that turn on the LEDs to make it easier to screen out that signal, which is not relevant to the brain’s electrical activity.