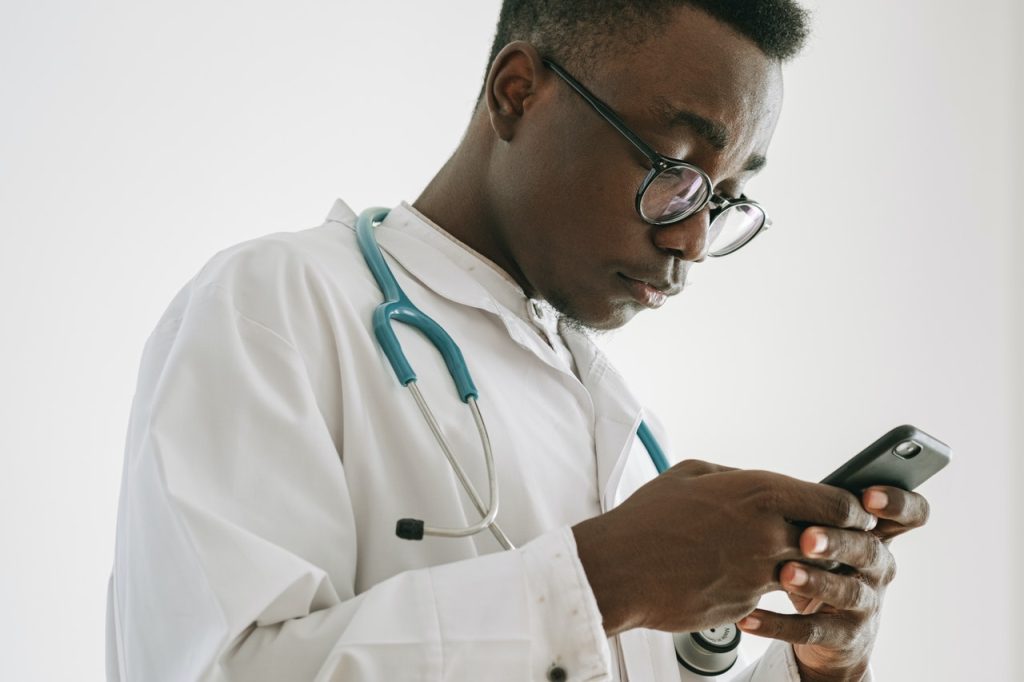
Engineers have designed a system that can remotely measure blood pressure from video of a person’s forehead and using artificial intelligence algorithms to extracting cardiac signals across a range of skin tones. They describe their new technology in a new paper published in Inventions.
Using the same remote-health technology they pioneered for non-contact monitoring of vital health signs, this new technology could replace the existing uncomfortable and cumbersome method of strapping an inflatable cuff to a patient’s arm or wrist, the researchers claim.
The researchers, from the University of South Australia and Baghdad’s Middle Technical University, describe the technique, which involves filming a person from a short distance for 10 seconds and then using AI to extract cardiac signals from two regions in the forehead.
Experiments were performed on 25 people with different skin tones and under changing light conditions, overcoming the limitations reported in previous studies. Compared to a digital sphygmomanometer (itself subject to errors), the systolic and diastolic readings were around 90% accurate.
“Monitoring blood pressure is essential to detect and manage cardiovascular diseases, the leading cause of global mortality, responsible for almost 18 million deaths in 2019,” says UniSA remote sensing engineer Professor Javaan Chahl. “Furthermore, in the past 30 years, the number of adults with hypertension has risen from 650 million to 1.28 billion worldwide.”
“The health sector needs a system that can accurately measure blood pressure and assess cardiovascular risks when physical contact with patients is unsafe or difficult, such as during the recent COVID outbreak,” Prof Chahl continues. “If we can perfect this technique, it will help manage one of the most serious health challenges facing the world today.”
The cutting-edge technology has come a long way since 2017, when the UniSA and Iraqi research team demonstrated image-processing algorithms that could extract a human’s heart rate from drone video.
In the past five years the researchers have developed algorithms to measure other vital signs, including breathing rates from 50 metres away, oxygen saturation, temperature, and jaundice in newborns.
Their non-contact technology was also deployed in the United States during the pandemic for non-contact monitoring of COVID signs.
Investigating the state of affairs in public clinics, Spotlight’s Daniel Steyn and Vusi Mokoena investigate whether the right technology could help them out of their predicament.
“I never look forward to clinic day,” says Nomtsato Tsietsi, 74, on a Monday morning while standing in the queue at Kayamandi Clinic in Stellenbosch, which she visits up to three times a month to collect pills, consult with a doctor, and have her blood tests taken.
Tsietsi has several diseases including diabetes and hypertension (high blood pressure). “We sit there for too long, sometimes all day,” she says.
Her experience is typical for people visiting state clinics. But for about 80% of South Africans, this is the only option: for most people private healthcare is unaffordable and public clinic services are free.
Some patients in the Kayamandi clinic queue said they sometimes pay people up to R80 to stand in the queue for them. One man, who had been paid by someone to stand in the queue, said that he had been there since 5am.
For employed people, a day at the clinic typically means taking a day off work, often without pay.
The pubIic health system is beset with problems: long waiting times, insufficient record keeping, poorly maintained infrastructure, and poor service delivery.
A 2018 study of nurses and doctors in Cape Town found that of 16 essential skills, ten were not performed in more than half of the consultations. In more than 60% of consultations, nurses and doctors in Cape Town did not greet patients, and in 90% of consultations, they did not attempt to understand the patient’s perspective. In nother study, 76% of Cape Town-based doctors in primary care reported that they are suffering from burnout.
During our visit to Kayamandi Clinic, we asked patients whether they would embrace technological solutions to make the experience more efficient. They all said they would. Almost all of them are smartphone users and some said they could not understand why appointments cannot be made and managed digitally, or why they cannot communicate with health workers online rather than in person.
Innovative technology solutions for primary care exist in South Africa.Phukulisa Health Solutions, for example, offers a platform that mimics a consultation with a healthcare practitioner. Equipped with Bluetooth sensors, the platform can screen patients for a range of health issues, focused specifically on HIV, TB, diabetes, and heart diseases.
Phukulisa’s CEO Raymond Campbell says that this testing and screening platform offers a more efficient screening service with a faster turnaround time. For example, the platform has been tested at an antenatal unit in Mamelodi, where the platform provided test results within 14 minutes, opposed to the usual 23 hours.
But Campbell says there is little interest from the public sector in his technology. Instead, he is finding more success licensing the platform to players in the private sector.
There have been some attempts to use innovative computer technology in public sector clinics. In Limpopo, the deputy director-general of the health department, Dr Muthei Dombo, has the vision to create a “clinic in the cloud”.
In 2018, Dombo partnered with theMint Group to conduct a trial funded by Microsoft at Rethabile clinic. Dombo provided the team at Mint Group with several problems to solve.
The team, led by Peter Reid, developed a technology to alleviate the high rate of fraud at medicine dispensing points, the difficulty of transferring medical records between different clinics, and the long waiting times.
When a patient entered the clinic, they would register at reception. Their identity document would be scanned and a picture would be taken of the patient. At every station in the clinic visited by the patient, a camera would identify the patient and the patient’s records would pop up on the screen. When the patient left the station, the profile would automatically lock.
This ensured that only patients due for specific medication would receive that medication, thereby eliminating fraud. Because the records were all kept in the cloud, the records could easily be transferred to another clinic. Without this technology, patients need to return to the same clinic every time they need to restock their medication.
The trial also assisted with queue management. Upon entering the clinic, patients would choose a “journey” based on their reason for visiting the clinic. The system would then guide the patient from one station to the next on big screens on the wall. This made the journey more seamless while also providing visual feedback to officials at the clinic helping them to manage the queues more effectively.
The trial ended shortly before the start of the Covid pandemic. The project has not yet been restarted.
One project that has been implemented widely in the public sector is Vula Mobile. Founded by Dr William Mapham in 2014, Vula aims to bridge the gap between health workers and specialists.
There is a shortage of specialist doctors in the public sector and health workers at the primary care level often lack the information to refer patients to a relevant specialist.
With the Vula app, a nurse seeing a patient can be linked with the closest specialist. Through the built-in chat function, the nurse can provide the specialist with all the necessary info and refer the patient.
The app is available in six provinces with an emphasis on the Eastern Cape. More than 24,000 health workers are registered on the system.
But other innovators in the health space, frustrated by the public sector, are focusing on providing affordable private healthcare. This follows a growing trend in South Africa, as medical aid providers increasingly offer more affordable packages targeted to lower-income earners.
At the Kayamandi clinic during GroundUp’s visit, Mcoleseli Mlenze, a 34-year-old father who often visits the clinic for hypertension medication or when his son is sick, said that while he uses the clinic to collect medication, he has started seeing a private doctor when he is sick.
He says he cannot really afford the private doctor, which costs upwards of R350 per consultation. If there was some middle-ground where he could pay R150-R200 for a consultation at a clinic that is faster and more efficient, he would happily do so.
Others in the queue said they would pay up to R50 for a better healthcare experience.
Saul Kornik, the founder of Healthforce and the Kena App, aims to lower the cost of quality primary health care so that millions of people have access to it.
Available in almost 500 pharmacies throughout the country, Healthforce’s technology enables nurses to conduct all necessary screenings and diagnostic procedures. If and when a doctor becomes necessary, the nurse presses a button to start a video call with one of the doctors in the Healthforce network.
The nurse and patient can both see the doctor and the doctor, with the help of the nurse, can consult the patient. This reduces the amount of time that the doctor is needed, thereby reducing the cost.
The patient ends up paying on average R70 to R90 for the nurse and R115 to R250 for the doctor. If needed, the doctor can prescribe medication that the patient can purchase at the pharmacy or pick up from a government dispensary.
There are Healthforce doctors available to speak any of the 11 official languages and they are available seven days a week.
In March, Healthforce launched the Kena Health app, through which patients can have consultations with nurses, doctors and mental health practitioners via chat, voice or video. The first three consultations per year are free.
After the consultation, if necessary, the doctor can provide a script for medication and a sick note.
At Kayamandi clinic, Gcobisa Malithafa, a 30-year-old mother of a toddler told GroundUp that although she would pay a small amount for a better experience, it should not have to come to that.
Malithafa suggests that instead, the clinic’s management should consult the community on a regular basis and make immediate improvements to the running of the clinic. “This thing of having one doctor at the clinic is not right,” she says.
She is struggling to get her child immunised, having visited the clinic many times without success.
Whether they use technology or not, she says, something has to change.
Popularly known as ‘dipsticks’, lateral flow assays (LFAs) have long been a standard point-of-care testing system, and continue to grow in popularity, especially in developing countries.
These disposable, paper-based diagnostic devices are inexpensive, readily available, have a long shelf life, and they’re fast, typically delivering results in under 20 minutes. They’re also easy to use at home, most commonly for pregnancy tests but also now for COVID.
“These tests have been extremely popular for years, mainly because they are so simple to use. You don’t send anything to the lab or clinic because these tests don’t require any external equipment to operate. This is an advantage,” said engineering researcher Fatih Sarioglu at the Georgia Institute of Technology. “But there also is a disadvantage. There are limitations to what they can do.”
Sarioglu and his team are overcoming the limitations of LFAs with development of a flow control technology, turning these simple tests into complex biomedical assays.
Their research is outlined in two papers in Science Advances and ACS Sensors. One explains the development of their technology and the other applies the technology in a toolkit to diagnose SARS-CoV-2, as well as influenza.
LFAs make use of capillary liquid flow to detect analytes. Sarioglu explained that conventional LFAs are not practical for performing multi-step assays – capillary flow precludes them from coordinating a complex process involving the application of multiple reagents in a specific sequence with specific delays in between.
The researchers describe a technique to control capillary flow by imprinting roadblocks on a laminated paper with water insoluble ink. The blocked liquid flow is thus manipulated into a void formed at the interface of the ink-infused paper and the polymer tape laminate. By modifying the roadblocks, the researchers can essentially set the time it takes for a void to form – creating timers that hold capillary flow for a desired period.
“By strategically imprinting these timers, we can program the assays to coordinate different capillary flows,” said Sarioglu, professor in the School of Electrical and Computer Engineering. “That enables multiple liquids to be introduced, and multistep chemical reactions, with optimal incubation times – so, we can perform complex, automated assays that otherwise would normally have to be performed in laboratories. This takes us beyond the conventional LFA.”
For the user, the new dipstick test works the same way as the reliable standard – a sample is added at one end and the results present themselves minutes later in living color(s) at the other end. Sarioglu and his colleagues simply enhanced and expanded the process in between.
Basically, they drew patterns on paper – a dipstick – and created immunoassays that rival other diagnostic tests requiring labs and extra equipment, in the effective detection of pathogenic targets like Zika virus, HIV, hepatitis B virus, or malaria, among others.
The paper in ACS Sensors describes a PCR-based point-of-care toolkit based on the lab’s flow technology. The assay is programmed to run a sequence of chemical reactions to detect SARS-CoV-2 and/or influenza A and influenza B. A traditionally labour-intensive genetic assay can now be done on a disposable platform which will enable frequent, on-demand self-testing, filling a critical need to track and contain outbreaks.
The lab is studying the technology’s application for other assays targeting other pathogens, with plans to publish in the coming months. Sarioglu is optimistic about the work’s potential.
“We believe this flow technology research will have widespread impact,” he said. “This kind of dipstick test is so commonly used by the public for biomedical testing, and now it can be translated into other applications that we do not traditionally consider to be cut out for these simple tests.”
Researchers have developed a way to quickly disinfect and electrostatically recharge used N95 respirators, restoring their effectiveness against COVID and other airborne diseases.
In their study published in Environment Science & Technology, the University of South Florida (USF) team showed their sterilisation technology could restore an N95 respirator’s original filtration efficiency of about 95 percent, even after 15 cycles of treatment. The technology fights coronavirus by using corona discharge, an electrical technique which simultaneously deactivating pathogens on a mask and restoring its electrostatic charges. It doesn’t require heat, or chemicals or contact, making it safe and convenient to use. It is safer than ultraviolet (UV) radiation and uses little electricity.
As well as restoring protection, the corona discharge treatment can reduce the impact of used masks on the environment. In a report by OceansAsia, a marine conservation organisation, 1.56 billion face masks polluted the oceans in 2020 and will likely take more than 450 years to fully decompose. The researchers say the technology will limit mask consumption to dozens each year instead of hundreds.
“It is a reduction of 90 percent for each user. If we assume that 10 percent of the population all over the world takes advantage of corona discharge mask reuse technology, there will be four- five billion fewer masks disposed to the environment,” said project lead Ying Zhong, assistant professor in the USF Department of Mechanical Engineering. “It will reduce at least 24 million tons of plastic pollution and reduce the amount of chemicals used for mask disinfection and avoid their environmental impact.”
“Despite the challenging conditions of the pandemic, this was the most thrilling project that I have ever worked on. We wish our research advances the understanding of how corona discharge disinfection can be turned into products on the market as soon as possible,” said co-project lead Libin Ye, assistant professor in the USF Department of Cell Biology, Molecular Biology and Microbiology.
The researchers are now working to develop this technology into products for hospitals and use by the general public, including handheld sterilisation devices.
At an annual meeting of the Heart Failure Society of America (HFSA), heart failure specialists agreed that recalling the HeartWare heart pump was good but debated whether its departure leaves the field of mechanical circulatory support (MCS) dead in the water.
In June, Medtronic stopped sales of its HeartWare Ventricular Assist Device (HVAD), citing excess neurological events and mortality with the device. As a result, Abbott’s HeartMate 3 became the only FDA-approved, durable left ventricular assist device (LVAD) on the market.
“Competition breeds innovation. When competition is absent or minimal, there is little incentive for corporations to innovate,” said Jennifer Cowger, MD, MS, of Henry Ford Hospital in Detroit, during the annual scientific meeting.
“While I believe the removal of the HVAD from the market was the ethical thing to do, unless we as a field start embracing MCS technology and change our messaging to the general cardiology community, our field is going to be viewed as niche to referring cardiologists and we’re going to face irrelevance and we’re going to have bad times ahead,” she added.
However Nancy Sweitzer MD, PhD, of the University of Arizona in Tucson, disagreed, pointing out that there are plenty of advances on the horizon.
Nine companies worldwide are developing heart pumps for this $3-4 billion market, Dr Sweitzer noted. Several devices under investigation — implantable ones with no external component — will probably proceed to first-in-man trials in the next year, she said. “There’s a lot of money if you do this well,” she added
Internal competition alone may be enough to advance the field, Sweitzer argued, citing Thoratec’s HeartMate II superseding their old HeartMate XVE.
“They put their own device up against their own device. So I would argue that corporate competition isn’t necessary when the stakeholders realize that we need to get better at this. I think the companies in this space realize there’s a huge unmet need here if we develop a really good MCS that was truly portable, gave people excellent quality of life, and had lower complications,” she said.
Yet given the pace of LVAD research, “in the next decade, we have cause for concern in the MCS field,” Dr Cowger countered.
Both debaters suggested that MCS technology shouldn’t stop at HeartMate 3, even with its relatively impressive performance.
“Outcomes on HeartMate 3 are not the outcomes we really want for these patients. There are still innumerable complications. Hospitalization rates are extraordinarily high in these patients post-implant even if they’re successful implants. They bleed, they get infected, they get strokes. That still happens,” noted Dr Sweitzer.
Innovation issues aside, Dr Cowger pointed out that HeartMate 3 is also much larger than the HVAD, and the smaller device’s loss leaves a gap for patients. She said negative media views had not helped the recent “sense of apathy and loss of enthusiasm for MCS”.
“Physicians don’t want to use technology that will harm or be perceived to harm patients,” she said, noting that sentiment has shifted from “VADs are sexy, cool” to “we would not choose LVADs over [heart] transplant.”
On Wednesday, the trial of Elizabeth Holmes, founder of medical technology company Theranos, began. Prosecutors alleged she “lied and cheated” for money and fame.
Ms Holmes faces 12 fraud charges over her role at the failed company which was once worth $9bn, facing up to 20 years in prison if found guilty.
She is accused of deceiving patients and investors about the company’s testing technology, which was claimed to diagnose basic illnesses from a few drops of blood. Her defence team argues that she was naive and her company simply failed.
“Failure is not a crime. Trying your hardest and coming up short is not a crime,” said defence lawyer Lance Wade in his opening statement on Wednesday.
Former Theranos executive Ramesh “Sunny” Balwani faces the same charges next year. He was romantically involved with Ms Holmes.
Ms Holmes, who founded Theranos in 2003 aged 19, was dubbed the world’s youngest self-made female billionaire and hailed as the “next Steve Jobs”.
In 2015 and 2016, investigations by the Wall Street Journal revealed Theranos’ blood-testing devices did not work and the company was doing most of its testing on commercially available machines made by other manufacturers. She initially denied these reports.
Prosecutor Robert Leach alleges that, after running out of funds, Ms Holmes and Mr Balwani turned to fraud in 2009, lying about the tests and exaggerating the firm’s performance. Mr Leach said this included falsely claiming the tests were vetted by Pfizer and being used by the US military.
The case will probably take months and Ms Holmes will likely take the stand — a necessary gamble in the face of overwhelming evidence that the technology did not work.
Ms Holmes “dazzled” Walgreens into using the company’s services, and the company brought her fame.
“She had become, as she sought, one of the most celebrated CEOs in Silicon Valley and the world. But under the facade of Theranos’ success there were significant problems brewing.”
The defence’s Mr Wade said Ms Holmes “naively underestimated” the business challenges but did not attempt to defraud investors. Ms Holmes has also alleged years of emotional and psychological abuse by Mr Balwani, who has denied the allegations. She is likely to testify as to how this affected her.
A prosthetic arm being fitted. Source: This is Engineering on Unsplash
Researchers have developed a bionic arm for patients with upper-limb amputations that allows wearers to think, behave and function like a person without an amputation.
The arm combines three important functions – intuitive motor control, touch and grip kinaesthesia, the intuitive feeling of opening and closing the hand. The developers, led by Clevelend Clinic, published their findings in Science Robotics.
“We modified a standard-of-care prosthetic with this complex bionic system which enables wearers to move their prosthetic arm more intuitively and feel sensations of touch and movement at the same time,” said lead researcher Paul Marasco, PhD, associate professor in Cleveland Clinic Lerner Research Institute’s Department of Biomedical Engineering. “These findings are an important step towards providing people with amputation with complete restoration of natural arm function.”
The system is the first to test all three sensory and motor functions in a neural-machine interface simultaneously in a prosthetic arm. The neural machine interface sends impulses from the brain to the arm and sensory information back to the brain.
“Perhaps what we were most excited to learn was that they made judgments, decisions and calculated and corrected for their mistakes like a person without an amputation,” said Dr Marasco. “With the new bionic limb, people behaved like they had a natural hand. Normally, these brain behaviors are very different between people with and without upper limb prosthetics. The researchers tested their new bionic limb on two study participants with upper limb amputations who had previously undergone targeted sensory and motor reinnervation -procedures that establish a neural-machine interface by redirecting amputated nerves to remaining skin and muscles.
In targeted sensory reinnervation, touching the skin with small robots activates sensory receptors that enable patients to perceive the sensation of touch. In targeted motor reinnervation, when patients think about moving their limbs, the reinnervated muscles communicate with a computerised prosthesis to move in the same way. Additionally, small, powerful robots vibrate kinesthetic sensory receptors in those same muscles which helps prosthesis wearers feel that their hand and arm are moving. The new prosthetic arm feels grip movement sensation, touch on the fingertips, and is controlled intuitively by thinking. Cameras lets the computer see the prosthetic’s position.
While wearing the advanced prosthetic, participants performed tasks reflective of basic, everyday behaviours that require hand and arm functionality, which were compared to people with traditional prosthetics and people without amputations.
According to Dr Marasco, because the limb lacks sensation, people with traditional prosthetics behave differently than people without an amputation when performing tasks. For example, traditional prosthesis wearers must constantly watch their prosthetic while using it, and have difficulty correcting for the correct amount of force needed.
The researchers could see that the study participants’ brain and behavioural strategies changed to match those of a person without an amputation. They no longer needed to watch their prosthesis, they could locate things without looking, and they could more effectively correct mistakes.
“Over the last decade or two, advancements in prosthetics have helped wearers to achieve better functionality and manage daily living on their own,” said Dr. Marasco. “For the first time, people with upper limb amputations are now able to again ‘think’ like an able-bodied person, which stands to offer prosthesis wearers new levels of seamless reintegration back into daily life.”
Researchers at Empa have developed a patch that stably seals two sutured pieces of intestine and thus prevents dangerous leaks.
A burst appendix or a life-threatening intestinal volvulus are emergencies that need to be treated by surgeons immediately. However, operations carry risks: highly acidic digestive juices and intestinal bacteria can leak out, causing peritonitis and sepsis.
Sealing sutured tissue with a plaster has already been tried, but the first were not well tolerated or were even toxic. Currently, these plasters are made of biodegradable proteins, which have variable clinical results. These is because they are mainly intended to support the healing process, and dissolve too quickly when in contact with digestive juices and don’t always hold tight. “Leaks after abdominal surgery are still one of the most feared complications today,” explained Empa researcher Inge Herrmann, who is also professor for nanoparticulate systems at ETH Zurich.
Searching for a material that could reliably seal intestinal injuries and surgical wounds, Hermann’s team found a synthetic composite material made up of four acrylic substances that, together, form a chemically stable hydrogel. Additionally, the patch actively cross-links with the intestinal tissue until it is fluid-tight. The quadriga of acrylic acid, methyl acylate, acrylamide and bis-acrylamide works in perfect synergy, as each component conveys a specific feature to the final product: a stable bond to the mucosa, the formation of networks, resistance to digestive juices and hydrophobicity. This new technology is detailed in Advanced Functional Materials.
In lab experiments, the researchers found the polymer system met their expectations. “Adhesion is up to ten times higher than with conventional adhesive materials,” said researcher Alexandre Anthis from Empa’s Particles-Biology Interactions lab in St. Gallen. “Further analysis also showed that our hydrogel can withstand five times the maximum pressure load in the intestine.” The material’s design uses its tailored effect: The rubbery composite selectively reacts with digestive juices that might leak through intestinal wounds, expands and closes all the more tightly. The inexpensive, biocompatible super glue, could thus shorten hospital stays and save healthcare costs, and Anthis is making plans to bring it to market.
A new electromedical device provides important data about possible cardiovascular and pulmonary risks before an operation.
Before any operation, it is important to properly assess the individual risk: Are there perhaps circulatory or pulmonary problems that need special consideration? To what extent can special risks be taken into account when planning the anaesthesia? Previously, clinicians have had to rely on rather subjective empirical values or carry out more elaborate examinations when in doubt. To address this, a novel device has been developed by TU Wien and MedUni Wien to objectively measure the cardiovascular and pulmonary system fitness of patients.
Pre-op interviews are important—but subjective Complications often occur after surgical interventions. In addition to blood loss and sepsis, perioperative cardiovascular and pulmonary problems are among the most common causes of death in the first 30 days after surgery.
To minimise this risk, anesthesiologists routinely talk to patients before surgery, in addition to measuring their blood pressure, performing an electrocardiogram, or conducting more laborious examinations. But assessing responses can be highly individualised. “There are also objectively measurable parameters by which one could easily identify possible risks,” said Prof Eugenijus Kaniusas (TU Wien, Faculty of Electrical Engineering and Information Technology). “So far, however, they have not been routinely measured.”
Just hold your breath This new device uses multiple sensors to determine key metrics in a completely non-invasive way. All the patient has to do is hold their breath for a short time to slightly outbalance their body, which responds reflexively with various biosignals. “Holding your breath is a mild stress for the body, but that is already enough to observe changes in the regulatory cardiovascular and pulmonary systems,” explained Eugenijus Kaniusas. “Oxygen saturation in the blood, heart rate variability, certain characteristics of the pulse waveform—these are dynamic parameters that we can measure in a simple way, and from them we could ideally infer individual fitness in general, especially before surgery.”
Since the device is non-invasive, medical training is not needed to operate it, and has no side effects. The result is easy to read: A rough assessment according to the three-color traffic light system or a score between 0 and 100 is displayed. The measurement can also be carried out at the bedside without any problems for people with limited mobility.
“Our laboratory prototype is being tested at MedUni Wien in cooperation with Prof. Klaus Klein from the University Department of Anesthesia, General Intensive Care Medicine and Pain Therapy. We hope to bring the device to market in the next 5 years with the help of research and transfer support,” said Eugenijus Kaniusas.
A rodent study has demonstrated the potential for transcranial focused ultrasound (tFUS) to relieve chronic pain and other symptoms.
Neuromodulation, or therapeutic stimulation of neurons with electrical energy. chemicals or potentially with acoustic waves, can amplify or dampen neuronal impulses in the brain or body to relieve symptoms such as pain or tremor.
Ultrasound is a promising non-invasive, non-surgical type of neuromodulation. It offers a temporary modulation that can be tuned for a desired effect. In this study, researchers have shown that it can be targeted at neurons with specific functions.
A team led by Bin He, PhD, professor of biomedical engineering at Carnegie Mellon University, and funded in part by the National Institute of Biomedical Imaging and Bioengineering (NIBIB), has demonstrated the potential of a neuromodulation approach that uses low-intensity ultrasound energy, called transcranial focused ultrasound-;or tFUS. In a paper published in Nature Communications, the authors describe the use of tFUS in rodent experiments, demonstrating the non-invasive neuromodulation alternative.
Moria Bittmann, PhD, Director of the Program in Biorobotic Systems, National Institute of Biomedical Imaging and Bioengineering, said: “Transcranial focused ultrasound is a promising approach that could be used to treat forms of chronic pain, among other applications. In conditions where symptoms include debilitating pain, externally generated impulses of ultrasound at controlled frequencies and intensity could inhibit pain signals.”
The researchers designed an assembly that included an ultrasound transducer and a multi-electrode array, which records neuronal data. During experiments with anaesthetised rodents, the researchers sent acoustic pulses into the brain cortex, targeting specific neurons, while recording change in electrophysiological signals from different neuron types.
When neurons transmit signals, whether engaging the senses or controlling movement, the firing of that signal across the synapse is termed a spike. The researchers observed two types of neurons: excitatory and inhibitory neurons.
When using tFUS to emit repeated bursts of ultrasound stimulation directly at excitatory neurons, the researchers saw an elevated impulse rate, or spike. Inhibitory neurons subjected to the same tFUS energy however did not display a significant spike rate disturbance. This showed that the ultrasound signal can be transmitted through the skull to selectively activate specific neuron sub-populations, in effect targeting neurons with different functions.
“Our research addresses an unmet need to develop non-toxic, non-addictive, non-pharmacologic therapies for human use,” said Prof He. “We hope to further develop the tFUS approach with variation in ultrasound frequencies and to pursue insights into neuronal activity so that this technology has the optimal chance for benefiting brain health.”
There are many broad applications for this research. Prof He believes non-invasive tFUS neuromodulation could be used to facilitate treatment for many people suffering from pain, depression and addiction. “If we can localise and target areas of the brain using acoustic, ultrasound energy, I believe we can potentially treat a myriad of neurological and psychiatric diseases and conditions,” Prof He said.