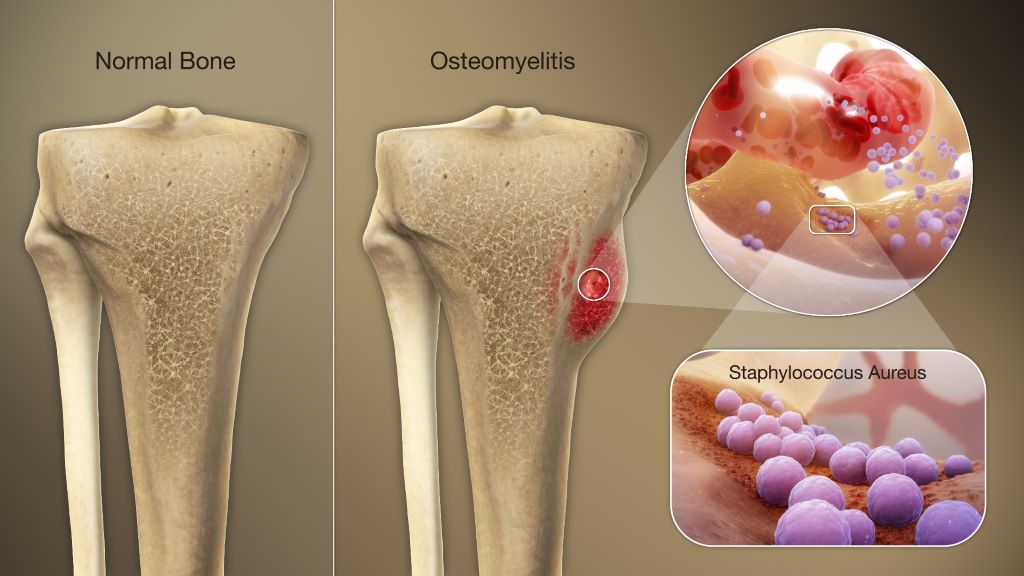
Osteomyelitis from Staphylococcus Aureus infection. Credit: Scientific Animations CC0
In patients who have undergone knee or hip replacement surgery, clinicians are noticing increasing numbers of chronic bone infections linked to a bacterial strain commonly found on the skin. A new study published in the Journal of Orthopaedic Research provides insights into the mechanisms involved, and how the bacteria lingers in bone reservoirs.
Utilising mouse models of bone infection and systematic electron microscopy studies, scientists found that the common skin bacteria Cutibacterium acnes can persist as layers of biofilms for weeks on contaminated titanium or stainless-steel implants. In mice, C. acnes could persist for 28 days in the tibia, and the researchers also observed C. acnes spreading to internal organs. compared to Staphylococcus aureus infections, C. acnes chronic osteomyelitis revealed markedly reduced bone osteolysis and abscess formation.
C. acnes can also invade deep pockets of the bone called osteocyte lacuno-canalicular networks and persist there.
“Our study highlights that osteocyte lacuno-canalicular networks can be a major reservoir for this bacterium and potentially provides a novel mechanism of why Cutibacterium acnes chronic bone infections are difficult to treat in the clinic,” said corresponding author Gowrishankar Muthukrishnan, PhD, of the University of Rochester Medical Center.
In APL Bioengineering, researchers report on an injectable hydrogel that treats infections around hip and knee replacement prosthetics without the problems caused by current treatments. Testing showed that the gel inhibits common bacteria and promotes tissue regrowth.
After hip and knee replacement surgeries, pathogenic bacteria can adhere to the surface of the joint prosthesis and form a dangerous biofilm. Gold standard clinical methods use potent antibiotics and further surgery, including removal of infected tissue and transplantation of new tissue, to treat these infections. However, these strategies run into problems with hyper-resistant bacteria caused by the abuse of antibiotics, persistent damage caused by tissue removal, difficulties in obtaining tissue donors, and toxicity and immune system complications.
A team from Shanghai Jiao Tong University School of Medicine created ablack phosphorus-enhanced antibacterial injectable hydrogel to re-establish biological barriers in soft tissue and suppress persistent infections. The gel has a porous structure, excellent injectability, and rapid self-healing properties.
“It is important to explore a new strategy for treatment of infected soft tissue wounds because it is directly related to prognosis,” said author Ruixin Lin. “We aspire to develop a simpler, safer method to help more patients avoid suffering and help more doctors make the right choices.”
In vitro tests showed the hydrogel had good stability and low toxicity to tissue cells. Irradiating the gel with near infrared light causes it to release silver ions. This process was highly efficient at inhibiting the common bacteria S. aureus.
“Furthermore, an in vivo infected wound model showed that the hydrogel could not only inhibit the persistent infection of the wound, but also accelerate the deposition of collagen fibres and angiogenesis, thereby realizing the repair of the natural barrier of soft tissue,” said Lin.
The novel hydrogel provides a safe and feasible synergistic antibacterial strategy for infected soft tissue healing. The team believes that it solves current clinical problems, such as stubborn infections caused by antibiotic resistance, and provides new ideas for minimally invasive treatment. They hope to see it used in the clinic after conducting sufficient studies on its underlying mechanisms.
A Monash University-led research team has developed a risk score based on individuals’ genetic data to predict their likelihood of needing hip or knee replacement surgery for osteoarthritis. The team validated the score’s predictive ability in a study published in Arthritis & Rheumatology.
The score incorporates 10 genetic sequence variants for predicting a person’s risk of needing knee replacement surgery and 37 genetic sequence variants for predicting the risk of needing hip replacement surgery.
Among 12093 individuals of European genetic descent aged 70 years or older, 1422 (11.8%) had knee replacements and 1,297 (10.7%) had hip replacements. Participants with high risk scores had a 1.44-times higher odds of knee replacement and a 1.88-times higher odds of hip replacement, compared with those with low risk scores.
“Genetic scores, such as the one we developed, do not change over a person’s life. They provide an individual with further information about their risk of severe osteoarthritis in later life and have the potential to improve prevention of severe knee and hip osteoarthritis by identifying those who may benefit from early intervention,” said senior author Flavia Cicuttini, PhD, of Monash University.
A study interviewing patients who received total knee replacement for osteoarthritis find that, despite the welcome pain relief, some also experience less pleasant psychological impacts.
For their study published in Arthritis Care & Research, UK researchers sought to bridge a knowledge gap of where people were dissatisfied with their total knee replacements even though they reported less pain and better function.
Using semi-structured interviews, researchers elicited comments from 34 patients, meant to explore patients’ thoughts about their knee implants. They received a lot of feedback about non-pain discomfort and feelings of dissonance.
“My leg feels like it’s made of lead,” one patient told researchers.
“It feels like someone is holding your knees, when you move, it’s like someone is … putting pressure there,” said another.
A third said: “I know it’s not my knee. It’s an alien knee in there. I don’t really feel connected to it.”
“Typically, the assessment of patient-reported outcomes after joint replacement focuses on functional outcome and pain relief as the main determinant of satisfaction,” the researchers explained. “This narrow perspective is compounded by poor definitions of satisfaction after surgery, and there is little research on how and why some patients express dissatisfaction with joint replacement and what they are dissatisfied about.”
Citing a study of hand surgery patients in which patients “spoke about their hand as if it were an object separate from their self,” the researchers argued that a psychological concept called embodiment could help explain the patients’ feelings of dissonance.
They wrote: “Embodiment refers to the experience of the body as both subject and object, such that this idea impacts the way in which a person sees and interacts with the world, and vice versa. Embodiment provides a way of understanding how one experiences limits of possible action, a sense of control, and empowerment over physical action.”
Initially, the researchers weren’t planning to focus on embodiment, but, they explained, “by the third interview we noted that some participants described sensations of discomfort such as heaviness or numbness when discussing pain and some described their knee as ‘alien,’ ‘foreign,’ or ‘not part of’ themselves. In response to these findings, the interviewer sought to elicit views about any such sensations in subsequent interviews, if this topic was not broached first by the participant.”
Their study emerged from an earlier one focusing on reasons for avoiding healthcare encounters post-surgery and involved the same participants, who had lingering pain and discomfort. The semi-structured interview covered pain as well as how patients managed it. After a third interview, patients who reported feelings of alienation from their implant were asked about it in more detail.
Participants reflected the general knee-replacement population – most in their 60 and 70s, and just over half were women. Of the 34 patients, 24 were between 2 and 4 years out from their surgery.
Physical types of non-pain discomfort were commonly reported, such as feelings of numbness and/or heaviness, as well as sensations of pressure applied externally. One man said it felt like the skin over his knee was stretched tight. Separate from these sensations were reports that the limb no longer felt like a part of them but something foreign, like an external prosthesis. Some patients complained of a lack of control. “That knee just wouldn’t do what it’s told to do,” one told the interviewer.
Others said they hadn’t regained trust in the knee, with one man still using a cane for fear of falling.
Overall, the researchers found that the patients’ experience were quite similar to those of amputees getting used to their prosthetic limbs. This could be partly explained by often experiencing years of pain and loss of function before the joint replacement.
“Presurgical chronic pain, instability, and untrustworthiness might continue to influence [mental] incorporation of the prosthesis afterwards,” the researchers suggested.
And there is a potential clinical implication for the findings: “Our study suggests that the interest for rehabilitation becomes not only strengthening the joint and promoting full recovery to tasks, but also modifying a person’s relationship with the new joint to achieve full incorporation or re-embodiment.”
The researchers proposed that other programmes developed for other conditions could be helpful, such as external prosthesis use as well as complex regional pain syndromes.
“Our focus should not be on the absence or loss of embodiment,” the researchers added, “but on employing a multidisciplinary approach to using the concept to guide the development of pre-rehabilitative strategies and appropriate outcome measures.”
Patients who have electroacupuncture during total knee replacement surgery report less pain and need far fewer opioids to manage their discomfort. In the study, 65% of patients who received acupuncture during surgery were able to have a low-dose or opioid-free postoperative experience, compared to 9% of patients outside of the study.
“Total knee replacements are one of the most common operative procedures in the United States and often very painful, so there’s a great need to explore non-opioid pain relief techniques for this type of surgery,” said lead author Stephanie Cheng, MD, DABMA, assistant attending anaesthesiologist at the Hospital for Special Surgery and assistant professor of clinical anaesthesiology at Weill Cornell Medicine. “Acupuncture is extremely safe and can help reduce pain with few unwanted side effects, but it has not been well researched as part of surgical anesthesia.”
The study enrolled 41 patients who had primary total knee replacement, all of whom received the institution’s standard opioid-sparing multimodal analgesic protocol, with the addition of electroacupuncture, which is a modified form of traditional acupuncture that applies a small electric current to thin needles that are inserted at known acupuncture points on the body. The acupuncture was administered during surgery by Dr Cheng, who is board-certified in medical acupuncture, to eight specific points in the ear to provide targeted pain relief in the knee.
With the addition of acupuncture, the majority of patients had reduced postoperative opioid use, compared to historical controls, while 65% of patients either maintained a low-dose opioid regimen of 15 oxycodone pills or less (57.5%) or remained completely opioid-free (7.5%) from induction of anaesthesia to 30 days post-surgery. Historically, only 9% of patients outside of the study were able to maintain a low-dose or opioid-free regimen post-surgery. Thirty days after surgery, all patients discontinued opioid use.
“Our study shows that if a trained medical acupuncturist is available to perform acupuncture in the operating room, it can help patients with postoperative pain recovery,” said Dr Cheng. “Most studies fail to incorporate nontraditional techniques, such as acupuncture, to help decrease the dependence on opioid medications for postoperative pain control.”
Low-dose perioperative opioid consumption is key to mitigating the opioid epidemic and opioid misuse by patients. Dr Cheng pointed out that with acupuncture being commonly used outside of the hospital as an effective therapy for pain management and treatment for a range of health issues and symptoms, it’s time to consider its benefits inside the hospital as well. “Additional research is needed to further define acupuncture’s effects and encourage its use in all aspects of disease treatment.”
A new study could help physicians better manage patients who experience debilitating stiffness after they undergo knee replacement surgery.
Researchers at Hospital for Special Surgery (HSS) in New York City presented their findings at the American Academy of Orthopaedic Surgeons (AAOS) 2021 annual meeting
Stiffness after knee replacement surgery, or total knee arthroplasty (TKA), is a rare but frustrating complication, affecting between 1% and 7% of patients who receive the artificial joints. “Why some people and not others experience limited range of motion after TKA is unknown,” said Ioannis Gkiatas, MD, PhD, an orthopedic surgeon at the University of Ioannina, in Greece, and the first author of the new study.
“The goal of the study was to see if we can help physicians predict how patients will do following the revision surgery, using information gathered before and after the procedure, to shape their postoperative treatment plans,” said Dr. Gkiatas. The work was conducted under the supervision of Peter K. Sculco, MD, hip and knee surgeon at HSS, who is leading a large, ongoing study of patient outcomes after revision TKA for reduced range of motion after index TKA.
The researchers followed 19 men and women who underwent revision TKA at HSS to try to improve stiffness in patients with prior TKA. Patients underwent range of motion testing before the procedure and at six weeks, six months and one year after the operation.
The range of motion of healthy knees ranges from full extension (0 degrees) through the sitting position (90 degrees) to kneeling (approximately 140 degrees). All patients gained an average of 28 degrees of motion after the revision surgery. The benefit mostly appeared in the first six weeks after the operation, then gradually tapered off over time.
Patients with the least restricted mobility had the greatest gains from the revision surgery. Patients who could able to bend their affected knee more than 82 degrees before TKA revision had an 80 percent chance of maintaining that level of mobility, or gaining flexibility in the joint, after the operation and throughout the follow-up period.
However, two-thirds of patients whose range of motion was less than 64 degrees prior to surgery experienced regression in that mobility during the study, never attaining the 82-degree threshold.
“Although 82 degrees doesn’t seem much more than 64 degrees, for the patient it’s a significant difference. With 82 degrees you can perform the basic activities of everyday life,” Dr Gkiatas said. “With these new data, if at six weeks a patient reaches 82 degrees of motion in their knee, we can say they have an 80 percent chance of at least maintaining this range of motion one year after surgery.”
The study results provide surgeons with the information needed to educate patients with stiff TKA on expected range of motion outcomes after revision surgery: Less than 60 degrees is a poor prognostic finding. Additionally, when patients return for their six-week appointment after revision TKA, and have less than 82 degrees of motion, additional pharmacologic or manual knee manipulation treatments should be done since this patient is at a high risk for range of motion regression and inferior clinical outcome at one-year post-revision.