Professor Luis Martinez-Sobrido, Ph.D., (left) and Staff Scientist Ahmed Mostafa Elsayed, PhD, (right) review test results for the presence of bird flu while wearing protective equipment required for biosafety level-3 laboratories.
One of the earliest strains of bird flu isolated from a human in Texas shows a unique constellation of mutations that enable it to more easily replicate in human cells and cause more severe disease in mice compared to a strain found in dairy cattle, researchers from Texas Biomedical Research Institute (Texas Biomed) report in Emerging Microbes & Infections.
The finding highlights a key concern about the H5N1 strains of bird flu currently circulating in the U.S.: the speed at which the virus can mutate when introduced to a new host.
Naturally found in wild birds and lethal in chickens, H5N1 has spread to a wide variety of mammals and began infecting dairy cows for the first time in spring 2024. As of early 2025, the outbreak had spread through herds across multiple states in the U.S. and infected dozens of people, mostly farm workers. So far, most people infected experience mild illness and eye inflammation and the virus is not spreading between people. The first H5N1 death in the U.S. was reported in January 2025 following exposure to infected chickens.
“The clock is ticking for the virus to evolve to more easily infect and potentially transmit from human to human, which would be a concern,” said Texas Biomed Professor Luis Martinez-Sobrido, PhD, whose lab specialises in influenza viruses and has been studying H5N1 since the outbreak began last year. The team has developed specialised tools and animal models to test prophylactic vaccines and therapeutic antivirals.
Human vs bovine
In the recent study, they compared H5N1 strains isolated from a human patient and from dairy cattle in Texas.
“There are nine mutations in the human strain that were not present in the bovine strain, which suggests they occurred after human infection,” Dr Martinez-Sobrido said.
In mouse studies, they found that compared to the bovine strain, the human strain replicated more efficiently, caused more severe disease and was found in much higher quantities in brain tissue. They also tested several FDA-approved antiviral medications to see if they were effective against both virus strains in cells.
“Fortunately, the mutations did not affect the susceptibility to FDA-approved antivirals,” said Staff Scientist Ahmed Mostafa Elsayed, PhD, first author of the study.
Antivirals will be a key line of defence should a pandemic occur before vaccines are widely available, Dr Martinez-Sobrido said. This is especially true since humans have no preexisting immunity against H5N1 and seasonal flu vaccines appear to offer very limited protection, according to a separate study conducted in collaboration with Aitor Nogales, PhD, at the Center for Animal Health Research in Spain.
Dr Elsayed shows the host species of the four types of influenza viruses: A, B, C and D. Avian influenza is part of the influenza A group and has infected a wide range of species. Influenza A and B are responsible for seasonal flu in humans.
Next steps and recommendations
Texas Biomed is now exploring the human H5N1 mutations individually to determine which are responsible for increased pathogenicity and virulence. The team wants to figure out what allows H5N1 to infect such a wide range of mammal species; why H5N1 causes mild disease in cows but is lethal in cats; and why infections via cows are less harmful to people than infections from chickens.
In a third paper, Dr Elsayed and collaborators analysed the history of H5N1 in dairy cattle for the journal mBio and called for a One Health approach to protect both animals and people.
“A key priority will be to eradicate bird flu from dairy cows to minimise risk of mutations and transmission to people and other species,” Dr Elsayed said. “Steps that can be taken now include thorough decontamination of milking equipment and more stringent quarantine requirements, which will help eliminate the virus more quickly in cows.”
McGill University scientists have discovered that pregnancy may trigger a natural immunity to boost protection against severe flu infection. Contrary to the common belief that pregnancy increases vulnerability to infections, researchers found that it strengthened an immune defence in mice, blocking the Influenza A virus from spreading to the lungs, where it can cause severe infection.
“Our results are surprising because of the current dogma, but it makes sense from an evolutionary perspective,” said co-lead author Dr Maziar Divangahi, Professor in McGill’s Faculty of Medicine and Health Sciences and Senior Scientist at the Research Institute of the McGill University Health Centre (The Institute).
“A mother needs to stay healthy to protect her developing baby, so the immune system adapts to provide stronger defenses. This fascinating response in the nasal cavity is the body’s way of adding an extra layer of protection, which turns on during pregnancy.”
Exploring benefits for pregnancy and beyond
The researchers used a mouse model to observe how a certain type of immune cell activates in the nasal cavity of mice during pregnancy, producing a powerful molecule that boosts the body’s antiviral defenses, especially in the nose and upper airways.
“Influenza A virus remains among the deadliest threats to humanity,” said first author Julia Chronopoulos, who carried out the research while completing her PhD at McGill. “This natural immunity in pregnancy could change the way we think about flu protection for expectant mothers.”
The Public Health Agency of Canada recommends pregnant women and pregnant individuals get the flu vaccine, as they are at high risk of severe illness and complications like preterm birth. The new insights offer promise for more targeted vaccines for influenza, which is among the top 10 leading causes of death in Canada.
“The broader population could also benefit, as our findings suggest the immune response we observed could be replicated beyond pregnancy,” said co-lead author Dr James Martin, Professor in McGill’s Faculty of Medicine and Health Sciences and Senior Scientist at the RI-MUHC. This could mean new nasal vaccines or treatments that increase protective molecules, known as Interleukin-17.
The team’s next focus is on finding ways to reduce lung damage during viral infections like the flu or COVID. Rather than targeting the virus, as previous research has done, they aim to prevent dysregulated immune systems from overreacting, an approach that could lower the risk of serious complications associated with flu infection.
A world-first study has found low-dose aspirin may treat flu-induced blood vessel inflammation, creating better blood flow to the placenta during pregnancy. Animal studies examined whether the treatment for preeclampsia could be applied to flu infections – and the results, published in Frontiers in Immunology, were very promising.
Lead researcher and RMIT Post-Doctoral Research Fellow, Dr Stella Liong, said that flu infections during pregnancy can resemble preeclampsia, a pregnancy complication that causes inflammation to the aorta and blood vessels. Low-dose aspirin is commonly taken to prevent preeclampsia, as it stops the body from creating chemicals that cause inflammation.
“When the vascular system is inflamed, it leads to poor blood flow and affects the aorta’s function,” she said. “This is especially a problem during pregnancy where good blood flow to the placenta is crucial to the development of the foetus.”
The research, led by RMIT University in collaboration with Trinity College Dublin, Ireland Professor John O’Leary and University of South Australia Professor Doug Brooks, found foetuses and placenta from mice with influenza A were smaller than those from uninfected mice.
Markers of low blood oxygenation and poor blood vessel development were also evident in the foetuses. The mice treated daily with low-dose aspirin had less inflammation and improved foetal development and offspring survival.
While the research was still awaiting human clinical trials, Liong said low-dose aspirin was already recognised as safe to take during pregnancy. The research team however recommended pregnant people seek medical advice before taking new medications.
Brooks said influenza A infections during pregnancy was a big concern as every pregnancy overlaps with part of a flu season.
“There are long term implications for both the mother and the foetus, and aspirin might provide a simple solution for preventing this influenza associated pathology,” Brooks said.
Why flu infection is dangerous during pregnancy
O’Leary said the research findings had huge implications for pregnancy and seasonal influenza virus infections for pregnant people.
“This study shines a light, for the first time, on the role of vascular inflammation associated with influenza virus and the potential dramatic effect of the disease-modifying drug aspirin, in low dosage, in pregnant women with co-morbid influenza,” O’Leary said.
While there weren’t many studies of the impacts of flu infections during pregnancy, project lead and RMIT Professor Stavros Selemidis said it was clear that pregnancy changed how the body responded to the virus.
Liong and Selemidis’ earlier breakthrough research found the flu virus during pregnancy could trigger a damaging hyperactive immune response, causing the virus to spread around the body from the lungs through the blood vessels.
“We used to think the flu virus just stayed in the lungs, but during pregnancy it escapes from the lungs to the rest of the body,” Selemidis said.
“This infection could set you up for cardiovascular disease later in life, but also set up cardiovascular disease in the offspring later in life.”
While vaccination was still the considered the best way to prevent flu infection during pregnancy, Selemidis pointed out vaccination rates were generally low in the pregnant population.
“Low vaccination rates aside, the flu shot may not generate the perfect immune response, especially if someone is pregnant or has an underlying medical condition,” he said.
“That’s why it’s useful to have a potential back up in low-dose aspirin to help prevent vascular dysfunction during pregnancy and improve foetal development.”
The new vaccine, tested in primates against the 1918 flu virus, would be a “one and done” shot
Photo by Mika Baumeister on Unsplash
New research led by Oregon Health & Science University reveals a promising approach to developing a universal influenza vaccine – one that also confers lifetime immunity against an evolving virus. The study, published in Nature Communications, tested an OHSU-developed vaccine platform against the virus considered most likely to trigger the next pandemic.
Researchers reported the vaccine generated a robust immune response in nonhuman primates that were exposed to the avian H5N1 influenza virus. But the vaccine wasn’t based on the contemporary H5N1 virus; instead, the primates were inoculated against the influenza virus of 1918 that killed millions of people worldwide.
“It’s exciting because in most cases, this kind of basic science research advances the science very gradually; in 20 years, it might become something,” said senior author Jonah Sacha, PhD, professor and chief of the Division of Pathobiology at OHSU’s Oregon National Primate Research Center. “This could actually become a vaccine in five years or less.”
Researchers reported that six of 11 nonhuman primates inoculated against the 1918 flu virus survived exposure to one of the deadliest viruses in the world today, H5N1. In contrast, a control group of six unvaccinated primates exposed to the H5N1 virus succumbed to the disease.
Sacha said he believes the platform “absolutely” could be useful against other mutating viruses, including SARS-CoV-2.
“It’s a very viable approach,” he said. “For viruses of pandemic potential, it’s critical to have something like this. We set out to test influenza, but we don’t know what’s going to come next.”
A senior co-author from the University of Pittsburgh concurred.
“Should a deadly virus such as H5N1 infect a human and ignite a pandemic, we need to quickly validate and deploy a new vaccine,” said co-corresponding author Douglas Reed, Ph.D., associate professor of immunology at the University of Pittsburgh Center for Vaccine Research.
Finding a stationary target
This approach harnesses a vaccine platform previously developed by scientists at OHSU to fight HIV and tuberculosis, and in fact is already being used in a clinical trial against HIV.
The method involves inserting small pieces of target pathogens into the common herpes virus cytomegalovirus, or CMV, which infects most people in their lifetimes and typically produces mild or no symptoms. The virus acts as a vector specifically designed to induce an immune response from the body’s own T cells.
This approach differs from common vaccines – including the existing flu vaccines – which are designed to induce an antibody response that targets the most recent evolution of the virus, distinguished by the arrangement of proteins covering the exterior surface.
“The problem with influenza is that it’s not just one virus,” Sacha said. “Like the SARS-CoV-2 virus, it’s always evolving the next variant and we’re always left to chase where the virus was, not where it’s going to be.”
The spike proteins on the virus exterior surface evolve to elude antibodies. In the case of flu, vaccines are updated regularly using a best estimate of the next evolution of the virus. Sometimes it’s accurate, sometimes less so.
In contrast, a specific type of T cell in the lungs, known as effector memory T cell, targets the internal structural proteins of the virus, rather than its continually mutating outer envelope. This internal structure doesn’t change much over time – presenting a stationary target for T cells to search out and destroy any cells infected by an old or newly evolved influenza virus.
Success with a century-old template
To test their T cell theory, researchers designed a CMV-based vaccine using the 1918 influenza virus as a template. In a highly secure biosafety level 3 laboratory at the University of Pittsburgh, they exposed the vaccinated nonhuman primates to small particle aerosols containing the avian H5N1 influenza virus – an especially severe virus that is currently circulating among dairy cows in the US.
Remarkably, six of the 11 vaccinated primates survived the exposure, despite the century-long period of virus evolution.
“It worked because the interior protein of the virus was so well preserved,” Sacha said. “So much so, that even after almost 100 years of evolution, the virus can’t change those critically important parts of itself.”
The study raises the potential for developing a protective vaccine against H5N1 in people.
“Inhalation of aerosolised H5N1 influenza virus causes a cascade of events that can trigger respiratory failure,” said co-senior author Simon Barratt-Boyes, PhD, professor of infectious diseases, microbiology and immunology at Pitt. “The immunity induced by the vaccine was sufficient to limit virus infection and lung damage, protecting the monkeys from this very serious infection.”
By synthesising more up-to-date virus templates, the new study suggests CMV vaccines may be able to generate an effective, long-lasting immune response against a wide suite of new variants.
“I think it means within five to 10 years, a one-and-done shot for influenza is realistic,” Sacha said.
Creative artwork featuring colourised 3D prints of influenza virus (surface glycoprotein hemagglutinin is blue and neuraminidase is orange; the viral membrane is a darker orange). Note: Not to scale. Credit: NIAID
Researchers at Vanderbilt University Medical Center have isolated human monoclonal antibodies against influenza B, a significant public health threat that disproportionately affects children, the elderly and other immunocompromised individuals, as they report in the journal Immunity.
Seasonal flu vaccines cover influenza B and the more common influenza A but do not stimulate the broadest possible range of immune responses against both viruses.
In addition, people whose immune systems have been weakened by age or illness may not respond effectively to the flu shot.
Small-molecule drugs that block neuraminidase, a major surface glycoprotein of the influenza virus, can help treat early infection, but they provide limited benefit when the infection is more severe, and they are generally less effective in treating influenza B infections. Thus, another way to combat this virus is needed.
The VUMC researchers describe how, from the bone marrow of an individual previously vaccinated against influenza, they isolated two groups of monoclonal antibodies that bound to distinct parts of the neuraminidase glycoprotein on the surface of influenza B.
One of the antibodies, FluB-400, broadly inhibited virus replication in laboratory cultures of human respiratory epithelial cells. It also protected against influenza B in animal models when given by injection or through the nostrils.
Intranasal antibody administration may be more effective and have fewer systemic side effects than more typical routes – intravenous infusion or intramuscular injection – partly because intranasal antibodies may “trap” the virus in the nasal mucus, thereby preventing infection of the underlying epithelial surface, the researchers suggested.
These findings support the development of FluB-400 for the prevention and treatment of influenza B and will help guide efforts to develop a universal influenza vaccine, they said.
“Antibodies increasingly have become an interesting medical tool to prevent or treat viral infections,” said the paper’s corresponding author, James Crowe Jr, MD. “We set out to find antibodies for the type B influenza virus, which continues to be a medical problem, and we were happy to find such especially powerful molecules in our search.”
Creative artwork featuring colourised 3D prints of influenza virus (surface glycoprotein hemagglutinin is blue and neuraminidase is orange; the viral membrane is a darker orange). Note: Not to scale. Credit: NIAID
By Elri Voigt for Spotlight
COVID-19-related factors resulted in several years of lower-than-normal rates of the flu, but experts say that is now something of the past. As this year’s flu season gets under way, Elri Voigt asks several local experts what their expectations are, which flu vaccines are available this year, and whether we should be concerned about new strains of bird flu.
While most people who get the flu experience only mild to moderate symptoms, some can get severe symptoms and even die, especially the very young and the old. As Spotlight previously reported, the influenza virus causes around 11 000 deaths per year in South Africa, with around 40 000 people hospitalised.
Dr Sibongile Walaza, a medical epidemiologist and the Head of Epidemiology at the Centre for Respiratory Disease and Meningitis at the National Institute for Communicable Diseases (NICD), says that it is difficult to predict what a flu season will look like beforehand.
Nicole Jennings, spokesperson for the South African Pharmaceutical company Pharma Dynamics, agrees. “Influenza is a global disease and the spread of the virus in other parts of the world can influence the trajectory of flu seasons in different regions. For now, it’s too early to make any predictions,” she says.
It is difficult to predict the trajectory of flu seasons ahead of time, Jennings says, because of a “complex interplay” of factors, including the fact that influenza viruses are constantly mutating. This makes it difficult to accurately predict which strains of the influenza virus will dominate and how they will behave.
“The level of immunity in the population can also vary from year to year due to factors, such as vaccination rates, previous exposure to similar strains and so forth,” she adds. “However, surveillance efforts, modelling and ongoing research conducted by the NICD can help the public to prepare for the cold and flu season as best possible.”
NICD guidelines published in April 2023 already stated that since the COVID-19 pandemic, there have been some changes in the timing of flu transmission.
The transmission reduction strategies – like masking and social distancing – during the pandemic had an impact on the rates of flu transmission and the duration of the flu season between 2020 to 2022, according to Dr Jocelyn Moyes, a medical epidemiologist at the Centre for Respiratory Disease and Meningitis at the NICD.
Back to normal?
Although the numbers were still much lower, it appears that the winter flu season’s peak had started to return to levels seen pre-COVID-19 in 2022 and 2023, Walaza confirms.
“In 2023, the flu season was a little bit longer than we’d seen before [COVID-19], but it started on time. So, in terms of the timing, it was similar to what we would see before COVID-19,” she says.
When exactly the winter flu season starts each year varies, Walaza says, but on average it can start anytime from the third week of April and can circulate until August. It has been known to go on longer though.
At the time of the interview, the NICD had only detected sporadic cases of flu but had not yet seen the sustained uptick in transmission which usually signals the start of the flu season. The latest surveillance data published by the NICD indicate that 108 cases of influenza had been detected so far this year. The real number of flu cases will be much higher since most cases of flu are not diagnosed.
This year’s vaccines
Walaza explains that the flu vaccine is updated each year based on the World Health Organization’s (WHO) recommendations. This is to ensure it provides protection against evolving influenza viruses seen in global surveillance programmes.
Photo by National Cancer Institute
Flu shots used in South Africa are inactivated influenza vaccines. This means they do not contain live virus and cannot cause flu.
In the public healthcare sector, the government this year procured the trivalent vaccine which protects against three strains of the influenza virus – two influenza A strains (H1N1pdm 2009 and H3N2) and one influenza B strain (known as the B/Victoria), Walaza says. These jabs should be in public health clinics by the first week of May.
In the private healthcare sector, she says a trivalent and a quadrivalent vaccine are available. The quadrivalent shot includes protection against a second influenza B strain (B/Yamagata), but that strain has not been seen circulating in a few years. These flu shots are already available in the private healthcare sector.
The level of protection provided by the flu shot varies and generally it ranges in effectiveness against infection from about 30% to 60%, according to Walaza, but importantly it protects against severe illness.
How effective this year’s flu shot will be depends on which influenza strain or strains circulate in the country. “The hope is that if an individual gets infected by any of those strains [in the vaccine], then that individual is protected or has some level of protection [against these strains] and will have some protection against severe illness” she says.
However, she adds, it’s difficult to predict how effective this year’s flu shot will be against preventing someone from getting the flu or experiencing symptoms of the flu. This is because there is always the chance that the strains which do circulate this season are different from the ones in the vaccine or have mutated so the shot becomes less effective.
Should we worry about bird flu?
At the start of April, the WHO reported that one case of avian influenza A (H5N1), one of the avian/bird flu viruses, had been detected in a person in the United States after they had come into contact with a cow who was presumed to be infected. This was the second human case of influenza A (H5N1) detected in that country, and the first case of a person being infected with this strain after coming into contact with a non-avian species.
So far, the risk to the general public is low, according to the WHO.
“Since the virus [avian influenza A (H5N1)] has not acquired mutations that facilitate transmission among humans and based on available information the WHO assesses the public health risk to the general population posed by this virus to be low and for occupationally exposed persons, the risk of infection is considered low-to-moderate,” the WHO statement said.
There are many subtypes of influenza A viruses, Moyes tells Spotlight, and avian influenzas are similar to human influenza A viruses. And so, she explains, there is always a possibility that these viruses mutate, enabling them to infect humans, or more importantly develop the ability to transmit effectively from one person to another. This could potentially cause a pandemic.
She tells Spotlight that over the last decade sporadic cases of human avian influenza have been described related to global outbreaks in birds. These cases have all been in people who have had very close contact – usually during the culling process – with sick birds. She advises that people involved in the management of avian influenza outbreaks take precautions, such as using appropriate personal protective equipment to prevent infection.
When asked whether people in South Africa need to be concerned about a potential bird flu outbreak, Walaza says so far, no cases of bird flu infection in humans – even during the recent widespread outbreaks in birds – have been identified in the country. But it is something that the NICD is aware of and surveillance for human cases during outbreaks of bird flu in the country is being conducted.
“What’s important though to note is that even when cases have been detected [in other countries] the risk of person-to-person transmission is extremely low,” she adds.
Launch of Cough Watch SA
Walaza tells Spotlight that most of the data gathered by the NICD on influenza is from surveillance in healthcare facilities, which means that not all cases of influenza are necessarily identified.
To gather additional data, the NICD is in the process of rolling out an additional digital surveillance system to detect influenza cases, called Cough Watch SA. This online web application allows the public to report influenza symptoms.
People who sign up are asked to provide basic demographic data like age and postal code. Participants will then be sent a weekly prompt asking if they’ve had any flu symptoms. If they have had symptoms, according to Walaza, then they will be asked to provide more information. This data will then be linked to the NICD database where it will be compared to other surveillance data to see if the platform could serve as an early warning system for a flu outbreak.
Cough Watch SA will be launched in the week of 7 May, says Moyes, who urged the public to help keep an eye on flu by signing up.
It has long been known that people with diabetes are at a substantially increased risk of developing severe lung disease if they become infected with viruses such as influenza, as well as other pathogens. When the COVID-19 pandemic started in early 2020, it became even more important to understand this mysterious phenomenon. It became clear that people with diabetes were at a significantly higher risk of coming down with severe, even fatal, lung disease after developing severe COVID, but no one understood why. In fact, some 35% of the pandemic’s COVID mortalities had diabetes.
Now, research conducted at the Weizmann Institute of Science and published in Nature has revealed how, in diabetics, high levels of blood sugar disrupt the function of key cell subsets in the lungs that regulate the immune response. It also identifies a potential strategy for reversing this susceptibility and saving lives.
Prof. Eran Elinav‘s team in his lab at Weizmann, headed by Drs. Samuel Nobs, Aleksandra Kolodziejczyk and Suhaib K. Abdeen, subjected multiple mouse models of types 1 and 2 diabetes to a variety of viral lung infections. Just as in diabetic humans, in all these models the diabetic mice developed a severe, fatal lung infection following exposure to lung pathogens such as influenza. The immune reaction, which in nondiabetics eliminates the infection and drives tissue healing, was severely impaired in the diabetic mice, leading to uncontrolled infection, lung damage and eventual death.
Next, to decode the basis of this heightened risk, the team performed an evaluation of gene expression on the level of individual cells, in more than 150 000 single lung cells of infected diabetic and nondiabetic mice. The researchers also performed an extensive array of experiments involving immune and metabolic mechanisms, as well as an in-depth assessment of immune cell gene expression in infected diabetic mice. In the diabetic mice they identified a dysfunction of certain lung dendritic cells, the immune cells that orchestrate a targeted immune response against pathogenic infection. “High blood sugar levels severely disrupt certain subsets of dendritic cells in the lung, preventing these gatekeepers from sending the molecular messages that activate the critically important immune response,” says Nobs, postdoctoral fellow and study first author. “As a result, the infection rages on, uncontrolled.”
Next, they explored ways to prevent the harmful effects of hyperglycaemia in lung dendritic cells, as a means of lowering the infection’s risk in diabetic animals. Indeed, tight control of glycaemic levels by insulin supplementation prompted the dendritic cells to regain their capacity to generate a protective immune response that could prevent the cascade of events leading to a severe, life-threatening viral lung infection. Alternatively, administration of small molecules reversing the sugar-induced regulatory impairment corrected the dendritic cells’ dysfunction and enabled them to generate a protective immune response despite the presence of hyperglycaemia.
“Correcting blood sugar levels, or using drugs to reverse the gene regulatory impairment induced by high sugar, enabled our team to get the dendritic cells’ function back to normal,” says Abdeen, a senior intern who co-supervised the study. “This was very exciting because it means that it might be possible to block diabetes-induced susceptibility to viral lung infections and their devastating consequences.”
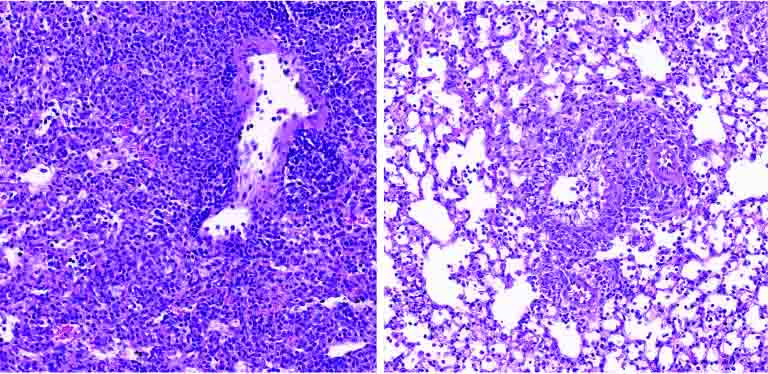
Lung tissue of a diabetic mouse (right) contains fewer immune cells (small purple dots) than that of a non-diabetic animal (left)
With over 500 million people around the world affected by diabetes, and with diabetes incidence expected to rise over the next decades, the new research has significant, promising clinical implications.
“Our findings provide, for the first time, an explanation as to why diabetics are more susceptible to respiratory infection,” Elinav says. “Controlling sugar levels may make it possible to reduce this pronounced diabetes-associated risk. In diabetic patients whose sugar levels are not easily normalized, small molecule drugs may correct the gene alterations caused by high sugar levels, potentially alleviating or even preventing severe lung infection. Local administration of such treatments by inhalation may minimize adverse effects while enhancing effectiveness, and merits future human clinical testing.”
Researchers from The University of Tokyo have helped unravel the connection between high body temperature and increased viral resistance. Older adults are at a higher risk of contracting viral infections, research shows. Quite notably, they also have lower mean body temperatures – yet the effects of increased body temperature on fighting viral infections remain largely unexplored. The researchers found that higher temperature increased bile acids along with the infection-fighting capability of the gut microbiota. Their study was published in Nature Communications.
To conduct their experiments, the team used mice which were heat- or cold-exposed at 4°C, 22°C, or 36°C a week before influenza virus infection. After the viral infection was induced, the cold-exposed mice mostly died due to severe hypothermia, whereas the heat-exposed mice were highly resistant to the infection even at increasing doses of the virus. “High-heat-exposed mice raise their basal body temperature above 38°C, allowing them to produce more bile acids in a gut microbiota-dependent manner,” remarks Dr Takeshi Ichinohe from the Division of Viral Infection, The University of Tokyo, Japan.
The authors speculated that signalling of deoxycholic acid (DCA) from the gut microbiota and its plasma membrane-bound receptor “Takeda G-protein-coupled receptor 5” (TGR5) increased host resistance to influenza virus infection by suppressing virus replication and neutrophil-dependent tissue damage.
While working on these experiments, the team noticed that mice infected with the influenza virus showed decreased body temperatures nearly four days after the onset of the infection, and they snuggled together to stay warm!
The team noticed similar results after switching the influenza virus with SARS-CoV-2 and the study results were also validated using a Syrian hamster model. Their experiments revealed that body temperature over 38°C could increase host resistance to influenza virus and SARS-CoV-2 infections. Moreover, they also found that such increase in body temperature catalyzed key gut microbial reactions, which in turn, led to the production of secondary bile acids. These acids can modulate immune responses and safeguard the host against viral infections.
Dr. Ichinohe explains, “The DCA and its nuclear farnesoid X receptor (FXR) agonist protect Syrian hamsters from lethal SARS-CoV-2 infection. Moreover, certain bile acids are reduced in the plasma of COVID-19 patients who develop moderate I/II disease compared with the minor severity of illness group.”
The team then performed extensive analysis to gain insight into the precise mechanisms underlying the gut-metabolite-mediated host resistance to viral infections in heat-exposed rodents. Besides, they also established the role of secondary bile acids and bile acid receptors in mitigating viral infections.
“Our finding that reduction of certain bile acids in the plasma of patients with moderate I/II COVID-19 may provide insight into the variability in clinical disease manifestation in humans and enable approaches for mitigating COVID-19 outcomes,” concludes Dr. Ichinohe.
To briefly summarize, the published study reveals that the high-body-temperature-dependent activation of gut microbiota boosts the serum and intestinal levels of bile acids. This suppresses virus replication and inflammatory responses that follow influenza and SARS-CoV-2 infections.
A heartfelt appreciation to the Japanese researchers for placing their trust in their intuition and gut instincts!
Influenza epidemics, caused by influenza A or B viruses, result in acute respiratory infection. New research published in published in the journal PNAS has identified how the influenza A virus manages to penetrate cells to infect them. By attaching itself to a receptor on the cell surface, it hijacks the iron transport mechanism to start its infection cycle. By blocking the receptor involved, the researchers were also able to significantly reduce its ability to invade cells. These results highlight a vulnerability that could be exploited to combat the virus.
Influenza viruses represent a major risk to human and animal health. Their potential for mutation makes them particularly elusive. ”We already knew that the influenza A virus binds to sugar structures on the cell surface, then rolls along the cell surface until it finds a suitable entry point into the host cell. However, we did not know which proteins on the host cell surface marked this entry point, and how they favoured the entry of the virus,” explains study leader Mirco Schmolke, Associate Professor at University of Geneva (UNIGE).
A receptor as a key to infection
The scientists first identified cell surface proteins present in the vicinity of the viral haemagglutinin, the protein used by the influenza A virus to enter the cell. One of these proteins stood out: transferrin receptor 1. This acts as a revolving door transporting iron molecules into the cell, which are essential for many physiological functions.
“The influenza virus takes advantage of the continuous recycling of the transferrin receptor 1 to enter the cell and infect it,” explains first author Béryl Mazel-Sanchez, a former post-doctoral researcher in Mirco Schmolke’s lab. “To confirm our discovery, we genetically engineered human lung cells to remove the transferrin receptor 1, or on the contrary to overexpress it. By deleting it in cells normally susceptible to infection, we prevented influenza A from entering. Conversely, by overexpressing it in cells normally resistant to infection, we made them easier to infect.”
Inhibiting this mechanism
The research team then succeeded in reproducing this mechanism by inhibiting the transferrinreceptor 1 using a chemical molecule. ”We tested it successfully on human lung cells, on human lung tissue samples and on mice with several viral strains,” says Béryl Mazel-Sanchez. ”In the presence of this inhibitor, the virus replicated much less. However, in view of its potentially oncogenic characteristics, this product cannot be used to treat humans.” On the other hand, anti-cancer therapies based on the inhibition of the transferrin receptor are under development and could also be interesting in this context.
”Our discovery was made possible thanks to the excellent collaboration within the Faculty of Medicine as well as with the University Hospitals of Geneva (HUG) and the Swiss Institute of Bioinformatics (SIB),” the authors add. In addition to the transferrin receptor 1, scientists have identified some 30 other proteins whose role in the influenza A entry process remains to be deciphered. It is indeed likely that the virus uses a combination involving other receptors. ”Although we are still far from a clinical application, blocking the transferrin receptor 1 could become a promising strategy for treating influenza virus infections in humans and potentially in animals.”
The cooler months bring with them a surge in cases of influenza or ‘flu’. Flu infection causes up to 650 000 deaths globally each year, and the highest numbers occur in sub-Saharan Africa.1
Seasonal flu is characterised by a sudden onset of fever, cough (usually dry), headache, muscle and joint pain, severe malaise, sore throat and a runny nose. The cough can be severe and can last two or more weeks.2
South Africa’s seasonal flu usually has its highest number of recorded cases between May and September each year, with over 11 000 flu-related deaths occurring in the country annually.1 It is therefore important that healthcare professionals (HCPs) and high-risk population groups such as those living with chronic illnesses do not delay getting their flu shot this winter season.
Who is at risk of contracting severe flu, and of experiencing complications?
According to the National Institute for Communicable Diseases (NICD), the people most at risk for severe/complicated influenza include:1
Pregnant women and women up to 2 weeks postpartum
Young children (particularly those under 2 years of age)
Persons over the age of 65 years
Individuals who are morbidly obese (body mass index ≥40)
immunosuppression (e.g. those on immunosuppressive medication, or who have cancer)
heart disease (e.g. congestive cardiac failure), except for hypertension
metabolic disorders (e.g. diabetes mellitus)
kidney or liver disease
neurological and neurodevelopmental conditions
abnormal production or structure of haemoglobin (e.g. sickle cell disease)
Those under 18 years receiving chronic aspirin therapy
HCPs are particularly vulnerable for contracting flu: a systematic review comparing the incidence of flu in healthy adults and HCPs found a significantly higher incidence in HCPs, since they are exposed to the virus via their patients.3 The World Health Organization (WHO) adds that “Because healthcare workers are dedicated individuals, they often come to work when they are sick, increasing the risk of transmission,” and therefore recommends that all HCPs are vaccinated against seasonal flu every autumn.3
The NICD indicates that it is particularly important to protect HCPs and ensure that they are able to continue to work and to reduce any additional burden on the health system.1
Most people recover from fever and other symptoms within a week of contracting the flu, without requiring medical attention. However, among high-risk groups, and those with serious medical conditions, flu can cause severe illness or death.2
Complicated influenza includes cases requiring hospital admission and/or with symptoms and signs of lower respiratory tract infection (hypoxaemia, dyspnoea, tachypnoea, lower chest wall indrawing and inability to feed), central nervous system involvement and/or a significant exacerbation of an underlying medical condition.1
When is the best time to get vaccinated?
Dr Lourens Terblanche, Medical Head: South Africa, Sanofi Vaccines, says: “People should ideally get vaccinated against flu before the flu season begins for the most effective coverage, although vaccination at any time during the flu season can still help protect against flu infections.”
“Influenza viruses evolve constantly, so twice a year the WHO makes recommendations to update vaccine compositions. HCPs and patients who are known to be at high risk for developing severe or complicated illness as a result of contracting the flu, should prioritise immunisation against flu every year, as recommended by the NICD,” says Dr Terblanche. “The vaccine is however available to any individual from the age of 6 months to help prevent influenza infection.”
How vaccination could protect beyond flu
Flu can impact many systems in the body, so flu vaccination can provide protection where these systems would have been affected. For example, complications of flu include a 10x higher risk of having a heart attack,4 an 8x higher risk of stroke,4 and an 8x greater risk of pneumonia in children under the age of 14,5 while persons with diabetes experience a 75% increase in glycaemic events.6
According to the US Centers for Disease Control (CDC), during the 2019-2020 season, flu vaccination averted 7.5 million cases of flu, 3.7 million medical visits, 105 000 flu-associated hospitalisations, and 6 300 deaths.7
A 2021 study by the CDC also showed that among adults hospitalised with flu, vaccinated patients had a 26% lower risk of having to go into the ICU and a 31% lower risk of death from flu, compared with those who were unvaccinated.7
“Flu vaccination is also essential considering the possible co-circulation of both the flu and SARS-Cov-2 or other respiratory pathogens. However, it is important to remember that the flu vaccine will not prevent COVID-19 and vice versa; therefore, it is important to ensure that HCPs and their patients are vaccinated against both. Simultaneous infection with flu and COVID-19 canresult in severe disease,8” says Dr Terblanche.
Current guidance from the Department of Health regarding administering flu and COVID-19 vaccinations at the same time is that this may be done, if they are given in different arms.9
The WHO reports that there are still a number of myths about the flu vaccine10 – myths to which HCPs are not immune – including that ‘Flu is not serious, so I don’t need the vaccine’. The WHO responds as follows: “As many as 650 000 people a year can die of the flu. This only represents respiratory deaths, so the likely impact is even higher. Even healthy people can get the flu, but especially people whose immune systems are vulnerable. Most people will recover within a few weeks, but some can develop complications including sinus and ear infections, pneumonia, heart or brain inflammation.”
“It is good to be aware of the myths surrounding flu vaccination in order to encourage high-risk individuals to have their flu vaccine timeously,” says Dr Terblanche.
The quadrivalent Vaxigrip Tetra vaccine produced by Sanofi Pasteur complies with the WHO’s Southern Hemisphere recommendations for the 2023 season11 and protects against the following strains:
∙ an A/Sydney/5/2021 (H1N1)pdm09-like virus;
∙ an A/Darwin/9/2021 (H3N2)-like virus;
∙ a B/Austria/1359417/2021 (B/Victoria lineage)-like virus; and
∙ a B/Phuket/3073/2013 (B/Yamagata lineage)-like virus.
4. Warren-Gash C, et al. Laboratory-confirmed respiratory infections as triggers for acute myocardial infarction and stroke: a self-controlled case series analysis of national linked datasets from Scotland. Eur Respir J. 2018; DOI: 10.1183/13993003.01794-2017
5. Kubale J, et al. Individual-level Association of Influenza Infection With Subsequent Pneumonia: A Case-control and Prospective Cohort Study. Clin Inf Dis. 2021; 73(11): e4288–e4295.
6. Samson SI, et al. Quantifying the Impact of Influenza Among Persons With Type 2 Diabetes Mellitus: A New Approach to Determine Medical and Physical Activity Impact. J Diabetes Sci Technol. 2019; 15(1):44-52.
8. Stowe J, et al. Interactions between SARS-CoV-2 and influenza, and the impact of coinfection on disease severity: a test-negative design. International Journal of Epidemiology 2021;1-10. doi: 10.1093/ije/dyab081.