
#InTheSpotlight | Where are We in the Search for an HIV Cure?
By Elri Voigt

Highly effective treatments for HIV have existed since the mid-1990s. But while these treatments keep people healthy, we do not yet have a safe and scalable way to completely rid the body of the virus. In this Spotlight special briefing, Elri Voigt takes stock of where we are in the decades-long search for an HIV cure.
As the science stands, the vast majority of the roughly eight million people in South Africa living with HIV will have to take treatment for the rest of their lives. This is because the antiretrovirals used to treat HIV prevents the virus from replicating but cannot eliminate it from the body. As soon as treatment is stopped, the virus rebounds, resulting in illness and eventually an early death.
A handful of people have been cured of HIV, but these “cures” involve very risky bone marrow transplants given as part of cancer treatment. The harsh reality is that 40 years into the HIV epidemic, and despite major scientific advances, we don’t yet have a viable cure for the roughly 40 million people on the planet who are living with the virus.
The good news, as one will see at any major AIDS conference these days, is that researchers around the world are working very hard to find a cure. In this #InTheSpotlight special briefing, we take a closer look at what progress has been made on this fascinating scientific journey and ask what the possible routes are toward an HIV cure.
What do we actually mean by a cure?
Dr Sharon Lewin, a leading figure in the world of HIV cure research and the inaugural director of the Peter Doherty Institute for Infection and Immunity in Melbourne, explains that a true “cure” for HIV would mean that there is not a single HIV infected cell left in a person’s body.
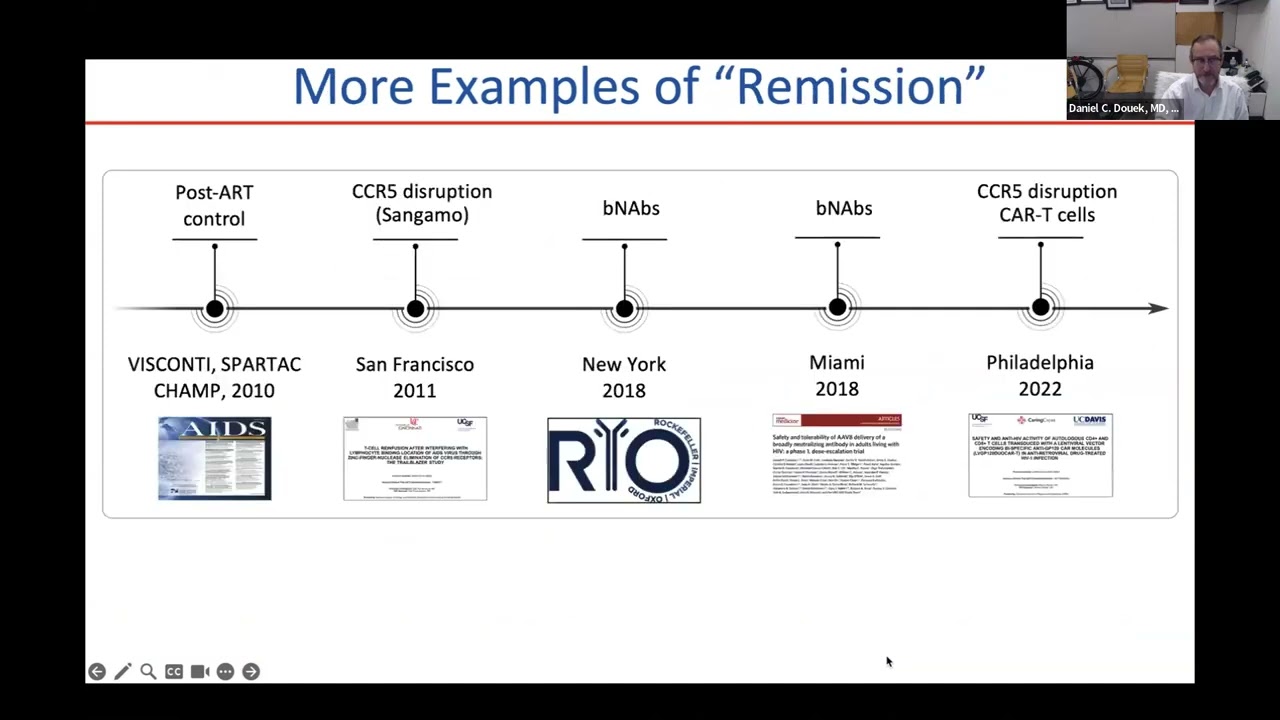
By contrast, “remission” would mean that the virus is still in the body, but it is being kept under control by the immune system. This could theoretically happen if the amount of HIV infected cells in a person’s body has been reduced to very low levels and the immune system’s ability to control those remaining cells has been enhanced. Basically, Lewin says, it is when the immune system does what antiretroviral therapy (ART) does without needing to take medication. Another term for this is ART-free viral load control.
There are some people living with HIV called “elite controllers” whose immune systems can naturally, without ART, control HIV. There are also extraordinary elite controllers, says Lewin, who through their immune response have been able to get rid of every single piece of the virus that they had in their bodies. Studying what is special about these rare people has been a key area of research in recent years.
Along with concepts like cure, remission, and control, it also helps to understand where vaccines fit in. As Jessica Salzwedel, the senior programme manager for research engagement at New York-based NGO AVAC, explains, a potential HIV vaccine might be therapeutic and not necessarily preventative. A therapeutic vaccine would be given to someone who is already living with HIV, in the hope that the vaccine would prime their immune system to better fight HIV or potentially clear it.
Why don’t we have a viable cure yet?
Finding cures for viral infections is not unheard of. In fact, one of the most consequential medical breakthroughs of the last decade or so was the development of a highly effective cure for hepatitis C. Unfortunately, it seems HIV is a much tougher nut to crack.
HIV works largely by invading a type of immune cell called a CD4 cell. Once inside, HIV writes its own genetic information into the cell’s DNA and then uses the cell’s machinery to produce more HIV. Eventually, the infected CD4 cell bursts and dies. Different types of antiretrovirals work by gumming up different stages of this process by which HIV invades and exploits CD4 cells. Most antiretroviral treatment regimens used today contain two drugs that target two different stages of this process. These medicines can drive HIV replication in the body down to near zero – which is why people who are stable on ART can live essentially normal, healthy lives.
Unfortunately, that is not the full story. As Lewin explains, the virus has a range of “tricks” that allows it to stay in someone’s body for much longer. One of those tricks is that HIV uses one of the immune system’s greatest assets against it. A person’s immune system contains cells that function as an immunological memory – essentially memory cells – which are designed to survive for a very long time. These memory cells, which include special CD4+ (CD4 positive) T-cells, contain information about which antigens it has encountered during a person’s lifetime. This helps the immune system recognise and kill those antigens faster the next time they enter the body.
HIV writes its own genetic code into some of these memory cells, which helps it stay in the body for as long as that person is alive. Lewin explains that once someone is on treatment, these immune system cells infected with HIV go silent and the virus stops replicating. These silent cells that contain infectious virus are rare, about one in every million, and can’t be found easily by the immune system, allowing the virus to hide in an inactive state but still able to release virus should the cell one day be activated.
These memory cells are found mainly in the lymph nodes, although they can also hide away in the gut, the spleen, and even the brain. Collectively, these HIV-infected cells in hiding are known as the latent reservoir. Should someone stop taking antiretroviral treatment, some of the cells in this latent reservoir could reactivate and start replicating again.
Lewin says researchers are getting better at finding these latent HIV-infected cells, but there still isn’t a way to easily tag these cells and destroy them.
Three lines of investigation
According to Lewin, researchers are exploring three broad strategies in search of an HIV cure.
Firstly, with a strategy called “shock and kill”, researchers try to reactivate (shock) the virus in the cells where it is hiding and then destroy (kill) it once it is flushed out. Such an approach will likely require at least two medicines – one to shock and one to kill. Unfortunately, attempts to find treatments that reliably shock HIV-infected cells out of their slumber has not borne much fruit so far.
Secondly, with “block and lock”, researchers hope to permanently silence the HIV that is hiding away in a person’s body. The aim here is to keep HIV latent for good, so that we never need to worry about killing it. This approach might involve using ART together with a latency promoting agent, of which several are currently being researched. “Block and lock” approaches have been picking up momentum in recent years.
Thirdly, with gene editing, researchers aim to “edit” cells to make them resistant to HIV or remove HIV from them. For example, CD4 cells can be modified to not have the specific receptor called CCR5 that HIV requires to gain entry into the cell. Essentially, if you remove the CCR5 receptor from a cell, HIV has no way in and the cell becomes immune to HIV. In this area, there have been some tantalising developments, but nothing yet that amounts to a workable cure. For example, in one study, people had their blood drawn, the CCR5 receptors removed from the CD4 cells in the blood, and then had the blood reinfused. It worked somewhat, but not nearly well enough to call it a cure.
These three categories are not the only way to think about potential cures.
Broadly, we can think about there being two big “buckets” of approaches for an HIV cure, says Salzwedel. The first “bucket” of approaches targets the virus, and those approaches are trying to remove HIV from the cell or “silencing” it so even if it is still present there is no replication. The other “bucket” of approaches looks at the host – or the person living with HIV – and improving their immune system so it can adequately kill HIV or make the cells that have HIV in them easier to spot so these cells can’t hide from the immune system. She says a combination of approaches from both “buckets” will probably need to be used for a cure.
A resource of HIV cure trials maintained by Treatment Action Group, a New York-based advocacy organisation, lists hundreds of clinical trials currently underway that are trying these different approaches or combinations of approaches.
What about the people who have been cured?
As mentioned earlier, one area of research has involved trying to understand “elite controllers”. Another critically important group of people in the search for a cure are the seven or so people who were living with HIV, but who have been cured. Some of these people, like Timothy Ray Brown and Adam Castillejo, have become minor celebrities in the HIV world.
Lewin explains that people like Brown and Castallejo, both of whom have essentially no HIV left in their bodies, had to go through interventions that can’t be replicated in everyone. Both had a type of blood cancer and were living with HIV. They had to undergo chemotherapy which wiped out their bone marrow, including the cells that had HIV in them. They were then given a whole new bone marrow system through a donation from someone who was naturally resistant to HIV since their CD4 cells do not have CCR5 receptors. This allowed the latently infected cells to be “flushed out” of their bodies. One of the other people cured of HIV received a bone marrow transplant from umbilical cord blood.
Such transplants are not things you can do for everyone who is living with HIV, its expensive and the severe risks of the procedure can only be taken in people living with both HIV and certain cancers. Even so, these cases, says Salzwedel, has shown us that it is possible to cure HIV and made us aware of some of the challenges.
Lewin says that cases like those of Brown and Castallejo helped advance gene editing approaches because they showed that not having CCR5 receptors makes CD4 cells essentially immune to HIV. This led to studies using special gene scissors – a technique called CRISPR – to find the gene for the CCR5 receptor in cells and remove it. CRISPR has also been used experimentally to remove HIV from cells.
So far only a small number of studies have been conducted using CRISPR-based gene editing approaches in an attempt to cure HIV – and these were mostly in the lab or in mice and monkeys. The first human gene editing study for CCR5 was done ex vivo – meaning cells were taken out of the body, edited, and then reinfused into the body. The first clinical trial of CRISPR for HIV in vivo – meaning it is done inside the body – is currently underway and early results were presented in July at the AIDS 2024 conference. While initial results in monkeys were promising, the early findings in humans were disappointing. EBT-101, the specific type of CRISPR treatment, did not prevent HIV from returning once treatment was stopped – although one study participant’s HIV only started replicating again after 16 weeks. A longer follow-up study is currently open in the United States for enrolment.
Gene editing could also potentially be used to strengthen the immune system. This could work, Lewin explains, by inserting a new gene that produces an antibody against HIV into cells and then putting those cells back into the body. “So instead of giving an infusion of an antibody, your own body makes the antibody. And that’s been done successfully in people with HIV on ART in two separate clinical trials and more recently in infant monkeys where ART was stopped,” she says. “The investigators injected CRISPR that delivered two different antibodies to infant monkeys who are infected with a monkey adapted form of HIV virus and on ART. The infant monkey’s muscle cells then start making the antibodies, and when they stopped ART, the antibodies kicked in and kept the virus under control, so that’s the most successful type of gene therapy,” Lewin says.
Boosting the immune response
Another promising avenue is broadly neutralising antibodies (bNAbs) – the broadly refers to the ability of these antibodies to neutralise a range of different HIV viral strains. Broadly neutralising antibodies can work as an antiviral while present in the body, but they can also trigger the immune system to control the virus and, according to Lewin, figuring out how bNAbs do this is a very important part of current cure research. Broadly neutralising antibodies that are HIV specific, work by binding with the virus and eliminating it while also enhancing a person’s immune system so it can control the virus that remains in the body by hiding in the immune system’s memory cells. Broadly neutralising antibodies potentially have this beneficial effect on immune control by activating CD4 and CD8 responses – part of the immune system’s defence – to kill HIV cells. There have been several clinical trials where a subset of participants who have been given bNAbs have been able to control the HIV virus for six months after stopping ART and when the bNAbs are no longer detected in blood. The scientific challenge is that this beneficial effect was only seen in a subset of participants and the duration of control is not fully understood as most clinical trials only assess participants up to 24 weeks off of ART.
Lewin says a small study has also looked at using anti-PD1, an antibody that reverses immune system exhaustion and essentially “revs” up the immune system to keep fighting HIV. Early study findings were presented at the Conference on Retroviruses and Opportunistic Infections (CROI) this year. Participants stopped ART and were given four doses of the antibody, called Budigalimab, or placebo over 29 weeks. Six out of the nine people who received the antibody had delayed viral rebound and/or ART free control, and two people had viral control off ART for over 29 weeks. The antibody will now be evaluated in a larger study.
Additional approaches, according to Dr Daniel Douek, an expert in immunology and the Chief of the Human Immunology Section at the National Institute of Allergy and Infectious Diseases in the United States, include HIV vaccines, which so far have not generated a strong enough immune response to be considered successful. Douek was speaking on an IAS webinar on HIV cure research. Another promising approach is to start someone on ART as quickly as possible after infection in the hope of preventing the establishment of the latent reservoir.
Suppressing the immune system with a drug has also been tried, says Douek, and research so far in this area warrants further investigation. While it seems counterintuitive, the researchers wanted to see if suppressing immune system cells might stop or reduce HIV replication because the virus likes to replicate in activated immune cells. People living with HIV, even when on treatment have a lot of activated immune cells. The drug Ruxolitnib, which is used to treat graft-versus-host disease in transplant patients, was given to 60 people living with HIV alongside their HIV treatment. After five weeks, there was a decrease in markers of immune activation and cell survival. And between five and 12 weeks of using this combination, those with large viral reservoirs displayed signs that their reservoirs were reducing in size. However, Douek cautioned that much more work needs to be done before we can draw firm conclusions about the value of this approach .
What comes next?
Though we don’t yet have a viable cure for HIV, Lewin says a lot of progress has been made, especially over the decade and a half since Brown was cured. We now know a lot more than we did about the virus and how it hides away in cells. Today, she says, we have cure interventions that work well in monkeys and some interventions being investigated in human clinical trials have induced ART-free viral control in some participants. But she is also clear that it will probably be “a very long time” before you can go to your doctor and get an HIV cure.
In this #InTheSpotlight special briefing, we have focused on the science, but as we have learnt from the new hepatitis C cures and from HIV prevention injections, the journey from the lab to your local clinic can be a very long one and involves far more than just the science.
According to Lewin, a successful HIV cure will have to tick several boxes. She says one needs an intervention that is durable, so that it leads to ART-free viral load control over a prolonged period of time. At this point, an intervention that allows for control over two, three or five years, is seen as worthwhile. Although the ideal would be to give something once and have ART-free viral load control over a lifetime. The intervention also needs to be scalable, so it can be given to a lot of people. It also needs to be cheap.
And if there is one insight we’ve gained over our many years covering HIV, it is that affordability and sufficient supply are not things we can take for granted. Given that many of the potential cures involve treatments that are substantially more complicated to produce and administer than antiretrovirals, the challenges here might be more acute than what we’ve seen before.
That we will eventually get a cure is also by no means inevitable. This is why it is critically important that governments and philanthropies continue to invest in cure research and support programmes such as the International AIDS Society’s Toward an HIV Cure initiative. Among others, this initiative is helping to build the capacity needed to conduct cure research in low-and-middle income countries.
Right now, even under a best-case scenario, a world without a cure will mean that many millions of people will still be living with HIV until late in the 21st century. A successful cure could change this trajectory. Ultimately, Salzwedel is right when she says: “We can’t really end an epidemic without a cure”.
Republished from Spotlight under a Creative Commons licence.






