The potential effect of induced abortion and miscarriage on the risk of breast cancer has remained debated and has been a persistent source of misinformation. Many previous studies have been small and based on self-reported data. Now, a study published in Acta Obstetricia et Gynecologica Scandinavica found that prior abortion or miscarriage was not linked with an increased risk of developing pre- or postmenopausal breast cancer.
In the nationwide Finnish registry-based study, investigators analysed data on 31 687 women with breast cancer diagnosed in 1972–2021 and 158 433 women without breast cancer.
The risk of breast cancer was found to be similar among women with a history of induced abortion and women with no history of abortion, both before and after 50 years of age. Risks were also similar among women with and without a past miscarriage.
In addition, breast cancer risks did not vary significantly by the number of abortions or miscarriages, nor by the time of first abortion or miscarriage.
“Miscarriage or induced abortion as potential risk factors for breast cancer has continued to raise concerns and has led to the spread of misinformation. In this study using high-quality Finnish registry data, we can reliably eliminate these concerns,” said corresponding author Oskari Heikinheimo, MD, PhD, of the University of Helsinki and Helsinki University Hospital. “Induced abortion or miscarriage are not risk factors for breast cancer, even if there are several of them. This information is important and reassuring for millions of women around the world.”
A drug mimicking the hormone progesterone has anti-cancer activity when used together with conventional anti-oestrogen treatment for women with breast cancer, a new Cambridge-led trial has found.
In the two-week window that we looked at, adding a progestin made the anti-oestrogen treatment more effective at slowing tumour growth. What was particularly pleasing to see was that even the lower dose had the desired effectRebecca Burrell
A low dose of megestrol acetate (a synthetic version of progesterone) has already been proven as a treatment to help patients manage hot flushes associated with anti-oestrogen breast cancer therapies, and so could help them continue taking their treatment. The PIONEER trial has now shown that the addition of low dose megestrol to such treatment may also have a direct anti-cancer effect.
Around three-quarters of all breast cancers are ER-positive. This means the tumours are abundant in a molecule known as an oestrogen receptor, ‘feeding’ on the oestrogen circulating in the body. These women are usually offered anti-oestrogens, medication that reduces level of oestrogen and hence deprives the cancer of oestrogen and inhibits its growth. However, reducing oestrogen levels can bring on menopause-like symptoms, including hot flushes, joint and muscle pain, and potential bone loss.
In the PIONEER trial, post-menopausal women with ER-positive cancers were treated with an anti-oestrogen with or without the progesterone mimic, megestrol. After two weeks of treatment, those that received the combination saw a greater decrease in tumour growth rates compared to those treated with an anti-oestrogen only.
Although further work is required in larger patient cohorts and over a longer period of time to confirm the findings, researchers at the University of Cambridge say the trial suggests that megestrol could help improve the lives of thousands of women for whom anti-oestrogen medication causes uncomfortable side-effects and can lead to some women stopping taking the medication.
PIONEER was led by Dr Richard Baird from the Department of Oncology at the University of Cambridge and Honorary Consultant Medical Oncologist at Cambridge University Hospitals NHS Foundation Trust (CUH). He said: “On the whole, anti-oestrogens are very good treatments compared to some chemotherapies. They’re gentler and are well tolerated, so patients often take them for many years. But some patients experience side effects that affect their quality of life. If you’re taking something long term, even seemingly relatively minor side effects can have a big impact.”
Some ER-positive breast cancer patients also have high levels of another molecule, known as progesterone receptor (PR). This group of patients also respond better to the anti-oestrogen hormone therapy.
To explain why, Professor Jason Carroll and colleagues at the Cancer Research UK Cambridge Institute used cell cultures and mouse models to show that the hormone progesterone stops ER-positive cancer cells from dividing by indirectly blocking ER. This results in slower growth of the tumour. When mice treated with anti-oestrogen hormone therapy were also given progesterone, the tumours grew even more slowly.
Professor Carroll, who co-leads the Precision Breast Cancer Institute and is a Fellow of Clare College, Cambridge, said: “These were very promising lab-based results, but we needed to show that this was also the case in patients. There’s been concern that taking hormone replacement therapy – which primarily consists of oestrogen and synthetic versions of progesterone (called progestins) – might encourage tumour growth. Although we no longer think this is the case, there’s still been residual concern around the use of progesterone and progestins in breast cancer.”
To see whether targeting the progesterone receptor in combination with an anti-oestrogen could slow tumour growth in patients, Dr Baird and Professor Carroll designed the PIONEER trial, which tested adding megestrol, a progestin, to the standard anti-oestrogen treatment letrozole.
A total of 198 patients were recruited at ten UK hospitals, including Addenbrooke’s Hospital in Cambridge, and randomised into one of three groups: one group received only letrozole; one group received letrozole alongside 40mg of megestrol daily; and the third group received letrozole plus a much higher daily dose of megestrol, 160mg. In this ‘window of opportunity’ trial, treatment was given for two weeks prior to surgery to remove the tumour. The percentage of actively growing tumour cells was assessed at the start of the trial and then again before surgery.
In findings published today in Nature Cancer, the team showed that adding megestrol boosted the ability of letrozole to block tumour growth, with comparable effects at both the 40mg and 160mg doses.
Joint first author Dr Rebecca Burrell from the Cancer Research UK Cambridge Institute and CUH said: “In the two-week window that we looked at, adding a progestin made the anti-oestrogen treatment more effective at slowing tumour growth. What was particularly pleasing to see was that even the lower dose had the desired effect.
“Although the higher dose of progesterone is licenced as an anti-cancer treatment, over the long term it can have side effects including weight gain and high blood pressure. But just a quarter of the dose was as effective, and this would come with fewer side effects. We know from previous trials that a low dose of progesterone is effective at treating hot flushes for patients on anti-oestrogen therapy. This could reduce the likelihood of patients stopping their medication, and so help improve breast cancer outcomes. Megestrol – the drug we used – is off-patent, making it a cost-effective option.”
Because women in the trial were only given megestrol for a short period of time, follow-up studies will be needed to confirm whether the drug would have the same beneficial effects with reduced side-effects over a longer period of time.
The research was funded by Anticancer Fund, with additional support from Cancer Research UK, Addenbrooke’s Charitable Trust and the National Institute for Health and Care Research Cambridge Biomedical Research Centre.
Personalised and precise cancer treatments underpin the focus of care at the future Cambridge Cancer Research Hospital. The specialist facility planned for the Cambridge Biomedical Campus will bring together world-leading researchers from the University of Cambridge and its Cancer Research UK Cambridge Centre and clinical excellence from Addenbrooke’s Hospital under one roof in a brand-new NHS hospital.
Adding breast magnetic resonance imaging (MRI) to a diagnostic mammogram did not reduce five-year cancer recurrence rates for patients with stage I/II hormone receptor (HR)-negative breast cancer, according to researchers at The University of Texas MD Anderson Cancer Center.
The Phase III Alliance A011104/ACRIN6694 trial found that five-year locoregional recurrence rates were 6.8% in patients who received an MRI as part of a diagnostic work-up and 4.3% in those who did not. These data were presented today at the San Antonio Breast Cancer Symposium (SABCS) by principal investigator Isabelle Bedrosian, MD, professor of Breast Surgical Oncology (Abstract GS2-07).
“We have long assumed that finding more breast cancer on an MRI and removing it with surgery would help lower the chance of a patient’s cancer coming back,” Bedrosian said. “When you look at our findings alongside earlier trials, the message is clear: adding MRI before surgery doesn’t improve results for patients – and may not have to be used as a standard part of the diagnostic process.”
No additional MRI benefit in this group
The trial enrolled 319 patients between 2014 and 2018 with newly diagnosed stage I or II HR-negative breast cancer. These patients were eligible for lumpectomy and did not have germline BRCA1/2 mutations, bilateral breast cancer or a history of prior breast cancer. All patients had undergone diagnostic mammography with or without ultrasound prior to trial enrolment. Patients were randomly assigned to undergo additional imaging by breast MRI (161 patients) or to receive no further imaging (158 patients).
Not only did breast MRI not impact five-year recurrence rates, but there were also not significant differences between groups for five-year distant recurrence-free survival nor overall survival.
A small subset of patients with tumour subtypes (HR- HER2+ and HR-HER2-) and those over the age of 50 at diagnosis also showed no benefit to MRI.
Pre-op MRI not finding anything important
Breast MRI is a common part of the diagnostic evaluation because it can reveal cancer that mammography might not detect. However, the evidence that it improves surgical outcomes for patients has been limited.
“We believe the reason MRI did not reduce recurrence rates may be twofold,” Bedrosian said. “It is possible that MRI didn’t uncover many lesions that mammography hadn’t already found, or perhaps identifying and surgically removing those additional lesions was not important to reducing risk of the cancer coming back. It’s possible that in the group that did not receive MRI, radiation and chemotherapy effectively treated the occult areas of disease”.
Experts are now analysing how often breast MRI identified additional lesions in the trial population to better understand why breast MRI did not impact oncologic outcomes.
Study limitations
Limitations included that most patients involved in the trial had breast cancer that hadn’t spread to their lymph nodes, which may partly explain why recurrence rates were low overall. Despite being open to women of all ages, the study enrolled mostly older women who may have been less likely to benefit from breast MRI.
These two magnetic resonance imaging (MRI) scans were taken 10 months apart. On the left, the blue arrow points to the edge of a breast tumour, and the red arrow locates a biopsy clip, which appears as a black dot. The MRI on the right, which includes the biopsy clip, shows the tumour is gone after a single, targeted dose of radiation and antihormone therapy.
A single, targeted high dose of radiation delivered before other treatments could completely eradicate tumours in most women with early-stage, operable hormone-positive breast cancer, according to a study led by UT Southwestern Medical Center researchers. The findings, published in JAMA Network Open, could shift the paradigm for patients with the most common form of breast cancer, who typically undergo surgery before a regimen of radiation therapy.
“This is a major advance in the field,” said study leader Asal Rahimi, MD, Professor of Radiation Oncology. “This treatment protocol provides patients a significant time savings, spares a lot of their tissue from irradiation, and allows them to still undergo any type of oncoplastic surgery they may choose, all while very effectively treating their disease.”
Like patients with other forms of cancer, those with breast cancer are typically treated with a combination of surgery to remove tumours, medications such as hormone blockers, chemotherapy, and radiation, often in that order. In addition, many patients choose to have breast reconstructive surgeries before radiation treatment.
Having targeted radiation prior to surgery has several benefits, including a more than 100-fold smaller volume of tissue being irradiated compared with whole breast radiation; one day of radiation compared with up to 6.5 weeks of radiation, creating a huge time savings for patients; and more options for patients seeking reconstructive surgery, explained Dr Rahimi.
Early-stage, hormone-positive breast cancer accounts for 60–75% of all breast cancers. Seeking a more time-efficient way to treat these patients, Dr Rahimi and her colleagues tested a strategy in which 44 patients started treatment with a single dose of targeted radiation. While typical radiation therapy protocols call for 1.8–2.67Gy per day for 16 to 33 days, the researchers divided the study participants into three groups and gave each patient a single dose of 30, 34, or 38Gy. The volunteers then went on hormone-blocking drugs and waited a median of 9.8 months until they underwent surgery to remove any residual tumour tissue.
In 72% of study participants, the surgeons found no residual tumor left, indicating that patients had a “pathological complete response.” An additional 21% of patients had a “near complete response,” meaning that their cancer was more than 90% eliminated.
Further analysis showed that time to surgery was the best predictor of response. The longer patients waited to undergo surgery, the more likely their tumours were to disappear, regardless of the radiation dose or tumour size. These results were probably due to the time it takes cells to die or be removed by the immune system after radiation therapy, Dr Rahimi explained.
This new treatment protocol could hold significant advantages over the current gold standard, said Marilyn Leitch, MD, Professor of Surgery. For example, being able to wait to schedule surgery will allow patients to plan for the disruption it brings to their lives. The radiation course lasts a single day rather than weeks. Plus, in the future, this new approach may eliminate the need for surgery in some patients.
“Much of the current research in breast cancer is looking at ways to reduce the extent of surgery, radiation, and/or medical therapy that is required to completely treat early-stage breast cancer. It is very exciting to be part of innovative research that can improve the quality of life of our cancer patients and minimize the extent of treatment they require,” Dr Leitch said.
The research team is currently enrolling patients in a phase two clinical trial. “If the results mirror the ones from this study, an initial targeted dose of radiation could become a new treatment option for patients with small, early-stage, hormone-positive breast cancer,” Dr Leitch said.
Radiotherapy can be safely omitted as a treatment for many breast cancer patients who have had a mastectomy and are taking anti-cancer drugs, as shown in a study published in the New England Journal of Medicine. An international trial found that patients with early-stage breast cancer who underwent a mastectomy had similar 10-year survival rates whether or not they received radiotherapy.
Experts say the findings should help guide treatment discussions, as many patients who currently qualify for radiotherapy after mastectomy under existing guidelines may not actually need it.
Outdated practice
For many patients with early-stage breast cancer treated by mastectomy and anti-cancer drugs, chest wall radiotherapy has long been standard to kill any remaining cancer cells and lower the risk of recurrence.
The practice is based on trials from the 1980s, now considered outdated, leaving uncertainty about its benefit and leading to variation in use worldwide.
The SUPREMO trial (Selective Use of Postoperative Radiotherapy after Mastectomy), led by the University of Edinburgh, studied the impact of chest wall radiotherapy in patients at intermediate risk of breast cancer returning.
International trial
The group included women from 17 countries with one to three affected lymph nodes, as well as those with none but who had other tumour features of aggressive behaviour that increase the chance of recurrence.
All 1607 patients in the study underwent mastectomy, axillary surgery – removing lymph nodes from the armpit – and modern anti-cancer therapy. They were randomly assigned to chest wall radiotherapy (808 women) or no radiotherapy (799).
Little benefit
There was no difference in overall survival of patients after ten years of follow up – 81.4% of those who received radiotherapy were still alive, compared with 81.9% of those who did not.
Radiotherapy also had no impact on disease-free survival – the length of time without any cancer returning – or on the cancer spreading from the breast around the body, the study found.
Radiotherapy had minimal impact on cancer recurring at the site of mastectomy. Nine patients who received the treatment saw their breast cancer return on the chest wall, compared with 20 who did not. Side effects from radiotherapy were mild with no excess deaths reported from cardiac causes.
Improved drugs
Experts attribute radiotherapy providing less benefit than previously thought to progressive improvements in treatment, particularly better drug treatments, which continue to reduce the chances of the cancer returning, and boost survival rates.
The research team caution that the study only looked at those with intermediate-risk breast cancer. Patients with a higher risk of their cancer returning could possibly benefit from chest wall radiotherapy, they add.
The SUPREMO trial provides no evidence to support the continued use of radiotherapy to the area of the chest wall in most patients with intermediate-risk breast cancer who have undergone a mastectomy if they are also treated with modern anti-cancer drug treatment.
Professor Ian Kunkler Institute of Genetics and Cancer, University of Edinburgh
Although reported toxicity in the trial was mild, we know that almost all patients experience some side effects of radiotherapy, that can even develop even some years after treatment. Avoiding unnecessary irradiation will reduce both treatment burden and, for example, the detrimental effects on breast reconstruction for these mastectomy patients.
Dr Nicola Russell Netherlands Cancer Institute and study coordinator on behalf of the EORTC
The international research team included scientists from the UK, Netherlands, Australia and China.
October is Breast Cancer Awareness Month, and what better way to celebrate than with floral elegance, an exquisite high tea, motivational speakers, and a live auction – all in the spirit of hope and healing.
On Saturday morning, 25th October 2025, at 11 am, PinkDrive will host their Hope Blooms High Tea at the Radisson Blu Hotel, Durban Umhlanga, a time of spring celebration and impactful fundraising. And you’re invited!
PinkDrive is a non-profit organisation (NPO) committed to prolonging lives through early detection of gender-related cancers. They operate mobile health units – those iconic pink trucks – that travel to rural and township areas to provide essential screenings to those who lack or have limited access to adequate healthcare.
Recent Rio Tinto outreach statistics highlight the urgent need for such interventions. In just one week in KwaZulu-Natal, 2251 health services were rendered, including 146 mammograms and 141 clinical breast examinations.
PinkDrive receives no government funding, relying entirely on donations, corporate partnerships, and community support to sustain its essential work. Among these partners is Lee-Chem Laboratories through their Mandy’s brand.
“This cause is deeply important to us – we’ve proudly supported PinkDrive for many years as a long-term corporate partner because of the difference they make in communities that need it most,” says Bhavna Sanker, Marketing Manager at Lee-Chem Laboratories. “It is a privilege to stand alongside them in their efforts to promote early detection and prolong lives. The Hope Blooms fundraiser perfectly reflects our shared commitment to raising awareness, providing crucial screening, and ultimately bringing hope where it’s needed most,” she explains. “We therefore want to encourage the public to also get involved by purchasing a ticket and enjoying an uplifting morning in support of PinkDrive’s vital work.
According to Janice Benecke from PinkDrive, corporate sponsors and partnerships, like that of Mandy’s, enable them to deliver this essential community service. “Mandy’s has been a proud supporter of PinkDrive for many years, generously providing branding, hampers, and product samples, along with an annual donation,” she says. “Through sponsored events like Hope Blooms, we hope to inspire further partnerships and support for our mission.”
Dr Marion Algar, Clinical Oncologist at Hopelands Cancer Centre specialising in breast cancer treatment, and Advocate Pria Hassan, founder of Women of Africa and champion of accessible healthcare through initiatives like iBreast, will share their insights as guest speakers. The elegant affair will be hosted by the lovely Delia Kroll, Mrs SA 2024 finalist, and attendees can also look forward to a welcome drink, networking opportunities, raffle prizes, gift bags, and an exciting live auction. Proceeds will go towards supporting PinkDrive’s free services, including clinical breast examinations, education, pap smears, and funding toward a new mammogram truck. Last year’s event raised R25 000; this year’s goal is to double that amount through your support.
“Hope Blooms reflects the courage, resilience, and renewal that come with a breast cancer journey,” notes Benecke. “Just like flowers that bloom after winter, it’s a reminder that through awareness, support, and love, hope always finds a way to grow.”
She concludes: “We want everyone to leave with this key message, and it’sa motto that I live by: ‘Only Believe, All Things Are Possible.’ Just look at me, I am a walking miracle.”
Tickets are R695 per person with a floral dress code. 10% of proceeds go directly to PinkDrive, and bookings can be made at info.durban.umhlanga@radissonblu.com. So why not consider purchasing a corporate table, inviting members from your sports or social club, or coming along with friends to enjoy a morning of elegance and purpose?
Study links blood levels of inflammatory markers with different aspects of cancer-related fatigue.
Photo by Karolina Grabowska on Pexels
New research reveals that inflammatory responses may play a role in different types of fatigue experienced by many people with cancer. The findings are published by Wiley online in CANCER, a peer-reviewed journal of the American Cancer Society.
Cancer-related fatigue can be a distressing and persistent burden that causes patients to feel physical, emotional, and/or cognitive tiredness or exhaustion. Activation of inflammatory responses by the tumour itself and/or by cancer treatment is thought to be a key biological driver of this symptom, but inflammatory activity across the cancer continuum has not been thoroughly examined.
To investigate, researchers at the University of California, Los Angeles (UCLA) analysed protein markers of inflammation in 192 women with early-stage breast cancer who were examined before radiation or chemotherapy and throughout the 18 months after treatment. At each assessment, women reported on different dimensions of fatigue (general, physical, mental, and emotional) and provided blood that was tested for protein markers of inflammation. These included two pro-inflammatory cytokines (TNF-α and IL-6) and two downstream markers of their activity (sTNF-RII and CRP).
Higher levels of TNF-α, sTNF-RII, and IL-6 were linked with greater general fatigue, which involves feelings of tiredness and exhaustion. These effects remained even after accounting for age, race, education, body mass index, and cancer stage. Similarly, there was a positive association between physical fatigue, which involves feelings of physical weakness and heaviness, and TNF-α, sTNF-RII, and CRP. Conversely, higher levels of TNF-α and sTNF-RII were associated with lower levels of emotional fatigue. No significant associations between mental (or cognitive) fatigue and inflammatory markers were found.
“Our findings indicate that inflammation plays a role in some aspects of cancer-related fatigue, but not others, and that these effects persist well after treatment,” said lead author Julienne E. Bower, PhD, of UCLA. “This is critical for developing targeted treatments for this common and disabling symptom.”
Rooibos, South Africa’s beloved herbal tisane, with proven benefits for the heart, diabetes management and brain health, is now revealing even more potential in preliminary breast cancer research led by Dr Nicky Verhoog, senior lecturer of biochemistry at Stellenbosch University.
Caption: Dr Nicky Verhoog, senior lecturer of biochemistry at Stellenbosch University.
Oestrogen’s role in breast cancer
While the research is still in its early stages, initial findings suggest that Rooibos extracts may counteract the activity of oestrogen in breast cancer cells – a discovery that has prompted the South African Rooibos Council (SARC) and the Department of Science, Technology and Innovation (DSTI) Sector Innovation Fund Programme to continue to support the work of Dr Verhoog with further studies in animal models scheduled to begin next year.
Oestrogen is often described as a kind of driver of breast cancer growth, because many breast cancer tumours carry receptors that respond to it. Although oestrogen doesn’t always start the cancer, it can speed up its growth once the disease has developed. Some newer studies also show that it may sometimes play a more direct role in triggering changes in cells that lead to cancer. Because so many breast cancers are sensitive to oestrogen, the possibility that Rooibos might help block its effect makes these findings especially significant.
Breast cancer in South Africa
Breast cancer remains a major health concern in the country. According to the latest statistics, between 11 000[1] and 15 000[2] women are diagnosed with breast cancer annually and the disease accounts for approximately 24% of all cancer cases in South African women. Early detection is critical – when identified at an early stage, breast cancer survival rates can exceed 90%, highlighting the importance of regular screening and self-examination.
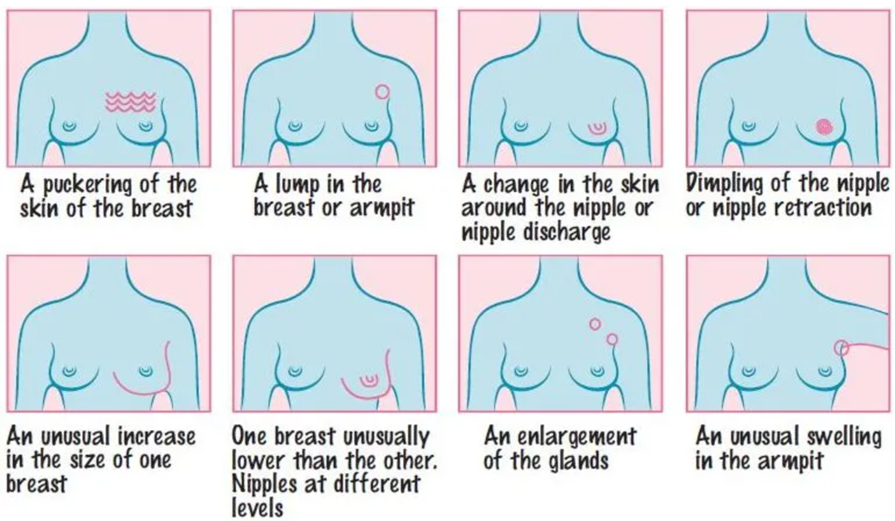
Caption: Warning signs of breast cancer. Source: CANSA (cansa.org.za)
Rooibos under the microscope
Against this backdrop, Dr Verhoog’s team conducted an in vitro (cell) study to examine whether Rooibos could influence oestrogen receptor-positive breast cancer cells. In the past, there has been some uncertainty about whether Rooibos might interact with oestrogen in ways that could affect women with hormone-sensitive breast cancer. This study set out to clarify its role – whether Rooibos could potentially act like estrogen or conversely, help block its activity – and to assess whether it influences cancer cell behaviour.
“To better understand how Rooibos interacts with natural hormones like estrogen, our team wanted to gather clearer scientific evidence,”
Dr Verhoog explains. “We also looked at whether Rooibos could influence the growth and spread of cancer cells, which is especially important for women with hormone-sensitive breast cancer.”
In the laboratory, the researchers worked with well-known breast cancer cell models that carry two types of estrogen receptors: one that can encourage tumour growth (ERα) and another that helps to suppress it (ERβ). They then added Rooibos extracts to see how the cells would respond – in terms of growth, movement and spread.”
The results were encouraging. The extracts acted against oestrogen, in a way similar to fulvestrant, a treatment commonly used to block oestrogen activity in breast cancer treatment. Rooibos slowed down oestrogen-induced cell growth and prevented the cells from spreading. Interestingly, the extracts showed a preference for activating ERβ, the receptor associated with tumour suppression.
“Rooibos appears to act in a protective way against oestrogen-driven breast cancer cells in the lab. It doesn’t mimic oestrogen, but rather inhibits its action. Importantly, we also found that it didn’t interfere with the effect of tamoxifen, a standard breast cancer therapy, which suggests Rooibos could be safely consumed by women undergoing treatment. Of course, this needs confirmation through in vivo (animal) studies.”
Next steps: pre-clinical trials in 2026
While the findings are promising, Dr Verhoog stresses the limitations of in vitro research.
“Lab studies involve single cell types and don’t replicate the complexity of the human body,” she says. “We need to see how Rooibos behaves when metabolised in the body, which is why our next step is pre-clinical trials planned for 2026.”
The next phase of research will move beyond cell studies to look at how Rooibos behaves in a pre-clinical model system. This step is important to confirm its safety for women with oestrogen-sensitive breast cancer and to better understand its effects in the body. The aim is not to test Rooibos as a treatment, but to ensure that it can be safely enjoyed alongside conventional therapies.
Rooibos’s broader health benefits
Rooibos is already celebrated for its wide range of health benefits. Rich in antioxidants and free from caffeine and added sugars, it is a popular alternative to sugary drinks, contributing to overall hydration and general wellness. Previous studies have also highlighted its potential protective effects against other cancer types, including prostate, liver and colon cancers, thanks to its potent antioxidant properties.
“While we are still in the early stages, our research adds to the growing evidence of Rooibos’ multifaceted biological actions. It’s a step toward understanding how this uniquely South African tisane may support health in a variety of ways,” emphasises Dr Verhoog.
Experts stress that these findings should not be interpreted as evidence that Rooibos can prevent or treat breast cancer. Rather, they reinforce its safety for consumption and provide a foundation for future research.
With October recognised as Breast Cancer Awareness Month, the study also underscores the urgent need for continued scientific investigation into the disease, while reminding women that regular screening, awareness of family history and early detection remain the most effective strategies for reducing breast cancer risk and improving outcomes.
[1]https://www.nicd.ac.za/wp-content/uploads/2025/04/NCR_ASR_tables_2023.pdf According to the National Cancer Registry (NCR), 10 980 cases of breast cancer were recorded in 2023. However, CANSA has highlighted significant underreporting, particularly in rural and under-serviced communities, suggesting that the actual number of cases is likely much higher. The available figures are based on pathological diagnoses.
The statistics provided by the International Agency for Research on Cancer (IACR) differ from those reported by the South African NCR, with the number of new breast cancer cases in 2020 being much higher in the IACR data than in the NCR data (15,491 versus 9259). These differences are due to the different strategies used to tally the statistics. The NCR is a collection of pathology-based cancer surveillance figures based on the curation of cancer diagnosis data from histology, cytology and bone marrow aspirate and trephine samples; these samples have been collected, analysed and then reported on annually [4]. The IACR data are based on the South African NCR and Eastern Cape Province Cancer Registries.
Women who miss their first mammogram run a higher risk of being diagnosed with advanced breast cancer and dying from the disease. This is shown in a new study from Karolinska Institutet published in The BMJ.
Since the early 1990s, women in Sweden have been offered regular mammograms, which has contributed to a decrease in breast cancer mortality. Despite this, a significant proportion choose not to attend their first examination. The researchers behind the new study wanted to investigate the long-term consequences of this.
The study is based on data from the Swedish mammography screening program and national health registries, and covers almost 433 000 women in Stockholm between 1991 and 2020, with follow-up for up to 25 years.
The results show that 32% of all women who were invited to their first screening declined. These women were also less likely to participate in future examinations, which often led to a later diagnosis and poorer prognosis.
“Skipping the first mammogram is a strong indicator of who is at risk of late detection and higher mortality. Our results show that missing the first mammogram is not just a one-time choice, but often marks the beginning of a long-term pattern of not attending check-ups,” says the study’s first author, Ziyan Ma, a doctoral student at the Department of Medical Epidemiology and Biostatistics, Karolinska Institutet.
Were detected at a more advanced stage
When women who skipped their first screening were later diagnosed with breast cancer, the disease was more often detected at a more advanced stage. The risk of developing stage III cancer was approximately 1.5 times higher, and for stage IV, the risk was as much as 3.6 times higher compared to those who participated in the first mammogram. Over a 25-year follow-up period, almost 1 percent of those who did not participate had died of breast cancer, compared with 0.7 percent among the participants – a difference that corresponds to a 40 percent higher risk of dying from the disease.
However, the total proportion of women who developed breast cancer was almost the same in both groups, approximately 7.7%. According to the researchers, this shows that the increased mortality is mainly due to delayed detection rather than more cases of the disease.
“Family history is a well-known, unchangeable risk factor for breast cancer. Our study shows that missing the very first screening examination carries a similar mortality risk – but unlike family history, this is a behaviour that we can change. Since over 30 percent of women skip their first screening, increased participation could save many lives. Since this group can be identified early, decades before deaths occur, healthcare providers have a chance to intervene with reminders or support to encourage participation, says the study’s last author, Kamila Czene, professor at the Department of Medical Epidemiology and Biostatistics, Karolinska Institutet
Immune cells (red) accumulating within a tumour (blue) and multiplying (green). When blood flow is blocked either in the heart or legs, these immune cells change in a way that enables tumour growth. Credit: NYU Langone
Cutting off blood flow can prematurely age the bone marrow, weakening the immune system’s ability to fight cancer, according to a new study from NYU Langone Health.
Published online August 19 in JACC: CardioOncology, the study showed that peripheral ischaemia, restricted blood flow in the arteries in the legs, caused breast tumours in mice to grow at double the rate seen in mice without restricted flow. These findings build on a 2020 study from the same team that found ischemia during a heart attack to have the same effect.
Ischaemia occurs when fatty deposits, such as cholesterol, accumulate in artery walls, leading to inflammation and clotting that restrict the flow of oxygen-rich blood. When this happens in the legs, it causes peripheral artery disease, which can increase the risk of heart attack or stroke.
“Our study shows that impaired blood flow drives cancer growth regardless of where it happens in the body,” says corresponding author Kathryn J. Moore, PhD, tProfessor of Cardiology at NYU Grossman School of Medicine. “This link between peripheral artery disease and breast cancer growth underscores the critical importance of addressing metabolic and vascular risk factors as part of a comprehensive cancer treatment strategy.”
Importantly, the research team found that restricted blood flow triggers a shift toward immune cell populations that cannot efficiently fight infections and cancer, mirroring changes seen with aging.
Systemic Skewing
To examine the mechanisms behind the link between cardiovascular disease and cancer growth, the study authors developed a mouse model with breast tumours and induced temporary ischaemia in one hind limb. The team then compared cancer growth in mice with and without impaired blood flow.
Their findings build on the nature of the immune system, which evolved to attack invading bacteria and viruses, and under normal conditions detects and eliminates cancer cells. These protective functions rely on stem cell reserves in the bone marrow, which can be activated as needed to produce key white blood cell populations throughout life.
Normally, the immune system responds to injury or infection by ramping up inflammation to eliminate threats, then scaling back to avoid harm to healthy tissue. This balance is maintained by a mix of immune cells that either activate or suppress inflammation. The researchers found that reduced blood flow disrupts this equilibrium. It reprograms stem cells in the bone marrow to favour the production of “myeloid” immune cells (monocytes, macrophages, neutrophils) that dampen immune responses, while reducing output of lymphocytes like T cells that help to mount strong antitumour responses.
The local environment within tumours showed a similar shift, accumulating more immune-suppressive cells, including Ly6Chi monocytes, M2-like F4/80+ MHCIIlo macrophages, and regulatory T cells, that shield cancer from immune attack.
Further experiments showed that these immune changes were long-lasting. Ischaemia not only altered the expression of hundreds of genes, shifting immune cells into a more cancer-tolerant state, but also reorganised the structure of chromatin, the protein scaffolding that controls access to DNA. This made it harder for immune cells to activate genes involved in fighting cancer.
“Our results reveal a direct mechanism by which ischemia drives cancer growth, reprogramming stem cells in ways that resemble aging and promote immune tolerance,” says first author Alexandra Newman, PhD, a postdoctoral scholar in Dr Moore’s lab. “These findings open the door to new strategies in cancer prevention and treatment, like earlier cancer screening for patients with peripheral artery disease and using inflammation-modulating therapies, to counter these effects.”
Moving forward, the research team hopes to help design clinical studies that evaluate whether existing inflammation-targeted therapies can counter post-ischaemic changes driving tumour growth.