The cancellation of PEPFAR funding to South Africa could cause between 150 000 and 295 000 additional HIV infections by the end of 2028. This is unless the South African government covers some of the defunded services.
These are the preliminary findings of a new modelling study commissioned by the National Health Department to look into the impact of PEPFAR funding cuts in South Africa. It was authored by researchers at the University of Cape Town (UCT) and University of the Witwatersrand (WITS). PEPFAR is a multi-billion dollar US initiative that supports HIV-related services globally, but which has been significantly slashed by the Trump administration since February.
The research on South Africa comes at the same time that a separate modelling study was published in The Lancet which found that the discontinuation of PEPFAR could cause an additional 1-million HIV infections among children in sub-Saharan Africa by 2030. This would lead to the deaths of about 500 000 children according to the study, while over 2-million others would be left orphaned.
On 20 January, newly-elected US president Donald Trump issued an executive order which suspended virtually all US foreign development assistance for 90 days pending a review. As a result, US-backed aid programmes were brought to a standstill across the world, including in South Africa. While a waiver was published which supposedly allowed some PEPFAR-related activities to continue, this had a limited effect in practice.
Since then, some US grants have resumed, while others have been cancelled. The value of all terminated grants comes to tens of billions of dollars globally. In South Africa, numerous awards have been cancelled from PEPFAR, which had provided roughly R7.5-billion to non-profit organisations in the country in 2024. These organisations primarily used the money to hire and deploy health workers in government clinics, or to operate independent health facilities. Many of these have now been forced to close.
While there are still some active PEPFAR grants in South Africa, it’s unclear how much longer these will be retained, as many are only approved until September. The new study focusing on South Africa models what would happen if all PEPFAR funding was eliminated.
Up to 65 000 additional deaths expected by 2028
In 2024 roughly 78% of all people who had HIV in South Africa were on antiretroviral (ARV) treatment. This figure has been steadily rising over time. By 2026, it was expected to climb to 81%, according to Dr Lise Jamieson, lead author of the local modelling study.
But this trend will be reversed if the entire PEPFAR programme is cancelled and the government fails to step in. ARV coverage among people with HIV would drop to 70% by 2026, according to the study. Under the model’s more pessimistic scenario, the figure would drop even lower – to 59% by 2026.
This is partly because some people living with HIV in South Africa get their ARVs directly from PEPFAR-funded drop-in centres. If these centres close down, some patients may stop taking their ARVs. Indeed, this is precisely what happened after one centre in Pretoria stopped providing services.
The loss of PEPFAR funds could also hinder the health system’s capacity to get newly-infected people on HIV treatment. For instance, PEPFAR-funded organisations had employed nearly 2000 lay counsellors across South Africa who tested people for HIV. Without these staff, fewer people will be diagnosed and get started on treatment.
Not only will ARV coverage drop due to the cuts, but HIV prevention services will also be affected, according to the study. For instance, PEPFAR-funded drop-in sites had been providing people with pills that prevent HIV, called pre-exposure prophylaxis (PrEP). These services were targeted at groups most likely to contract and transmit HIV, like sex workers. According to the new modelling study, the full termination of PEPFAR would lead to as much as a 55% reduction in PrEP coverage for female sex workers by 2026.
Because of factors like these, the researchers estimate that the PEPFAR cuts would cause between 56 000 and 65 000 additional HIV-related deaths in South Africa by 2028. By 2045, this would increase to between 500 000 and 700 000 deaths.
Nearly 90% of USAID contracts terminated in South Africa
All of these results only hold if the South African government fails to step in, according to Jamieson. The modelling study finds that to cover all PEPFAR services from 2025 to 2028, the government would need to spend an extra R13 to 30-billion in total.
It’s unlikely that the government will cough up this amount, but according to Jamieson the National Health Department is taking steps to identify and support certain key services that were defunded by PEPFAR. She is hopeful that the results may not be as drastic as what the study suggests.
Another caveat is that the modelling study estimated what would happen if South Africa lost all of its PEPFAR funding. But at least for now, there are still some grants reaching beneficiaries in the country.
PEPFAR funds are primarily distributed by two US agencies – the US Agency for International Development (USAID) and the US Centres for Disease Control and Prevention (CDC). While both agencies paused funding after the initial suspension order in late-January, the CDC resumed its funding roughly two weeks later. This was after a US federal court ruled that the Trump administration could not freeze congressionally appropriated funds.
CDC grants only appear to be active until September (at least for South African beneficiaries), though uncertainty remains about this.
USAID has taken a much harder line – funding was suspended from late January. By late-February, the agency moved from pausing funds to issuing termination notices to most of its beneficiaries.
In South Africa, roughly 89% of all USAID funding has been cancelled. The value of all cancelled funds comes to about US$261-million (R5.2-billion). Only five other countries have faced larger cuts in absolute terms (see all country-level estimates here). Spotlight and GroundUp have confirmed that at least some of the remaining 11% of USAID funding has once again begun flowing to beneficiaries in the country.
Thus, a small amount of USAID funding is trickling into South Africa, while CDC funds have largely been retained in full. Though it’s unclear for how much longer.
Finance Minister Enoch Godongwana holding a copy of the 2025 Budget Speech. (Photo: Parliament of RSA via X)
By Charles Parry, Funeka Bango, Tamara Kredo, Wanga Zembe, Michelle Galloway, Renee Street and Caradee Wright
While the 2025 national budget boosts health spending, researchers from the South African Medical Research Council stress the need for strong accountability measures. They also raise concerns about rising VAT and omissions related to US funding cuts and climate change.
The 2025 budget speech by Finance Minister Enoch Godongwana saw a welcome boost to the health budget with an increased allocation from R277 billion in 2024/2025 to R329 billion in 2027/2028. This signals a government that is responding to the dire health needs of the public sector, that serves more than 80% of the South African population.
As researchers at the South African Medical Research Council (SAMRC), we listened with interest and share our reflections on some of the critical areas of spend relevant for health and wellbeing.
We note the increase in investment in human resources for health and allocations for early childhood development and social grants. At the same time, we also raise concern about increasing VAT, with knock-on effects for the most vulnerable in our country. There were also worrying omissions in the speech, such as addressing the impact of the United States federal-funding freeze on healthcare services nationally, and a noticeable absence of comment on government’s climate-change plans.
Health and the link with social development: Recognising the importance of early childhood development
Education and specifically early childhood development (ECD) is known to have critical impacts on children’s health and wellbeing, with longstanding effects into youth and adulthood. In South Africa, eight million children go hungry every day, and more than a third of children are reported to live in households below the food poverty line, that is below the income level to meet basic food requirements, not even covering other basic essentials such as clothes.
While the increase in the number of registered ECDs is laudable, many more ECD centres in low-income areas remain unregistered, which means they do not get support from the government in terms of subsidies and oversight.
Social grants
The increase in social grants is welcomed. However, the marginal increase of the Child Support Grant (CSG) by only R30, from R530 to R560, is too little to impact on the high levels of child hunger and malnutrition. The release of the Child Poverty Review in 2023, which highlighted the eight million children going hungry every day, including CSG recipients, proposed the immediate increase of the CSG to at least the Food Poverty Line (R796 in 2024).
Social relief of distress still too small
The Social Relief of Distress (SRD) Grant is an important source of income for low-income, working-age, unemployed adults. Its continuance in 2025 is welcomed. However, it remains too small at R370 per person per month, and the stringent means-test criteria which disrupt continuous receipt from month-to-month, makes it an unreliable, unpredictable source of income for low-income individuals.
Strengthening the healthcare workforce
The Minister stated that “R28.9 billion is added to the health budget, mainly to keep about 9 300 healthcare workers in our hospitals and clinics”. It will also be used to employ 800 post-community service doctors, and to ensure that our pharmacies do not run out of medicines. The speech highlighted the necessary commitment to strengthening the healthcare system, specifically human resources for health.
Considering the pressures on resources, primarily due to the escalating disease burden and challenges within the health workforce, the proposed budget increase from R179 billion to R194 billion – an increase of 8.2% – to maintain the current workforce and employ additional healthcare workers signifies a positive step forward that will aid in addressing staff shortages.
Despite the gains in health spending, the proposed increase in VAT raises substantial concerns to partially negate the potential benefits to the health sector. As the World Bank reports that approximately 60% of people living in South Africa live below the poverty line, increases to VAT will likely drive poverty levels higher.
A focus on other forms of taxation may be better, more evidence-based, and less likely to disproportionately affect those at the highest levels of poverty.
On the issue of alcohol taxes, often mischaracterised as “sin taxes” rather than “health taxes”, the Minister has proposed excise duties of 6.75% on most products for 2025/26. This is 2% above consumer inflation, which stands at 4.75%.
Raising alcohol prices through higher excise taxes is globally recognised as an effective way to address alcohol-related harms. National Treasury is to be commended for adjusting alcohol excise tax rates above CPI in the 2025/26 Budget. This is a move in the right direction, but it does not address the current anomalies in tax rates across different products. This failure to address shortcomings in the excise tax regime is expected, given the release of a discussion document on alcohol excise taxes in December 2024 with a February 2025 response date. The earliest we can expect substantial changes in excise tax rates is in February 2026.
From a public-health perspective, it makes sense to link alcohol excise taxes to the absolute alcohol content of the product to standardise across products. Ethanol is ethanol. The current differential in excise tax rates on different alcohol products is indefensible. Specifically, it makes no sense to tax wine and beer so much less than spirits in terms of absolute alcohol content. Wine, especially bag-in-box wine, is the cheapest product on the market in South Africa, and its affordability increases consumption, leading to more societal harm.
Beer is the most consumed product in the country and is increasingly sold in larger, non-resealable containers. A 2015 SAMRC study in Gauteng found the highest level of heavy episodic drinking with beer products, largely due to their affordability, especially in larger, non-resealable containers. Heavy episodic drinking is a major public-health concern in South Africa, with 43.0% of current drinkers engaging in heavy episodic drinking at least monthly, 50.9% of male and 30.3% of female drinkers. Increasing the excise tax on beer is a powerful tool that the state can use to reduce the level of such behaviour.
Additionally, it makes sense to have lower taxes on alcohol products with lower alcohol content, as this could shift consumption to less harmful products. The current excise tax regimen does not account for this within a single product type like beer or wine, as all products are taxed at the same rate regardless of their alcohol content.
During the COVID-19 pandemic, we saw the benefits of decreased access to alcohol: fewer injuries, fewer unnatural deaths, and communities less disrupted by patrons visiting liquor outlets. While no one advocates for total liquor sales bans, increasing excise taxes on wine and beer would decrease alcohol consumption and reduce harms on drinkers, on others around them, and on society more broadly.
Acute risk to lives with knock on effects due to US federal funding cuts
We believe the South African government has a responsibility to step into the gap left by the sudden US federal funding freeze on HIV and TB services. The US President’s Emergency Plan for AIDS Relief (PEPFAR) funds 17% of HIV and TB services in South Africa and covers salaries for thousands of health workers, including the vital services of community health workers.
The implications for people living with HIV and TB and affected by the externally funded services will be devastating. It will also have ripple effects on the health system as we see inevitable increases in demand for health services to address advancing illness, effects on families caring for ill relatives or losing income.
This area needs to be addressed and clear communication from the National Department of Health is urgently awaited. The US funding cuts clearly impact on essential research funding available to institutions like the SAMRC and no indication has been given in the budget of any plans to augment or replace such funding.
National Health Insurance for South Africa’s public sector
The Minister addressed budget allocations for NHI implementation, specifically, the mid-term indirect and direct conditional grants for NHI were R8.5 billion and R1.4 billion respectively. Although these amounts in themselves are minor compared to other health-budget allocations, allocations for infrastructure (R37.4 billion over the mid-term economic framework period) and additionally allocations for digital patient health information systems, chronic medicine dispensing and distribution systems, and medicine stock surveillance systems are vital for healthcare efficiency and improved outcomes.
Least said not soonest mended: climate change – ‘no comment’?
From a climate-crisis perspective, although the budget speech did not explicitly mention climate change or its related health challenges, there seems to be positive steps being taken to address these issues. Initiatives such as clean energy projects and efforts to improve water management have the potential to benefit all sectors of society, while helping to mitigate the health risks associated with climate change.
Promising spend on health, but who will measure the impact?
Ultimately, increasing health spend is a promising step to increase access to quality health services for South Africa’s population. However, this is not enough, government must seize the opportunity to translate the budget increase into improved health outcomes. The effectiveness of the additional funds must be maximised through efficiency, transparency, and sound governance. The government can reinforce the integrity of public-health services by aligning these increases with robust accountability measures.
Government-academic partnerships represent an opportunity to share knowledge, technical skills and resources to support evidence-informed decision-making for national health decision-making and strengthen monitoring and evaluation mechanisms. There are many examples of this working well, and we trust that the SAMRC, along with the network of higher education institutions are well placed to provide the necessary support.
*Parry, Bango, Kredo, Zembe, Galloway, Street and Wright are researchers with the SAMRC.
Note: Spotlight aims to deepen public understanding of important health issues by publishing a variety of views on its opinion pages. The views expressed in this article are not necessarily shared by the Spotlight editors.
After the US slashed global aid, the South African government stated that only 17% of its HIV spending relied on US funding. But some experts argue that US health initiatives had more bang for buck than the government’s programmes. Jesse Copelyn looks past the 17% figure, and considers how the health system is being affected by the loss of US money.
In the wake of US funding cuts for global aid, numerous donor-funded health facilities in South Africa have shut down and government clinics have lost thousands of staff members paid for by US-funded organisations. This includes nurses, social workers, clinical associates and HIV counsellors.
Spotlight and GroundUp have obtained documents from a presentation by the National Health Department during a private meeting with PEPFAR in September. The documents show that in 2024, the US funded nearly half of all HIV counsellors working in South Africa’s public primary healthcare system. The data excludes the Northern Cape.
Counsellors test people for HIV and provide information and support to those who test positive. They also follow up with patients who have stopped taking their antiretrovirals (ARVs), so that they can get them back on treatment.
Overall, the US funded 1,931 counselors across the country, the documents show. Now that many of them have been laid off, researchers say the country will test fewer people, meaning that we’ll miss new HIV infections. It also means we’ll see more treatment interruptions, and thus more deaths.
PEPFAR also funded nearly half of all data capturers, according to the documents. This amounted to 2,669 people. Data capturers play an essential role managing and recording patient files. With many of these staff retrenched, researchers say our ability to monitor the national HIV response has been compromised.
These staff members had all been funded by the US President’s Emergency Plan for AIDS Relief (PEPFAR). The funds were distributed to large South African non-government organisations (NGOs), who then hired and deployed the staff in government clinics where there is a high HIV burden. Some NGOs received PEPFAR funds to operate independent health facilities that served high-risk populations, like sex workers and LGBTQ people.
But in late January, the US paused almost all international aid funding pending a review. PEPFAR funds administered by the US Centres for Disease Control (CDC) have since resumed, but those managed by the US Agency for International Development (USAID) have largely been terminated. As a result, many of these staff have lost their jobs.
The national health department has tried to reassure the public that the country’s HIV response is mostly funded by the government, with 17% funded by PEPFAR – currently about R7.5 billion a year. But this statistic glosses over several details and obscures the full impact of the USAID cuts.
Issue 1: Some districts were heavily dependent on US funds
The first issue is that US support isn’t evenly distributed across the country. Instead, PEPFAR funding is targeted at 27 ‘high-burden districts’ – in these areas, the programme almost certainly accounted for much more than 17% of HIV spending. Some of these districts get their PEPFAR funds from the CDC, and have been less affected, but others got them exclusively from USAID. In these areas, the HIV response was heavily dependent on USAID-funded staff, all of whom disappeared overnight.
Johannesburg is one such district. A doctor at a large public hospital in this city told Spotlight and GroundUp that USAID covered a substantial proportion of the doctors, counsellors, clerks, and other administrative personnel in the hospital’s HIV clinic. “All have either had their contracts terminated or are in the process of doing so.”
The hospital’s HIV clinic lost eight counselors, eight data capturers, a clinical manager, and a medical officer (a non-specialised doctor). He said that this represented half of the clinic’s doctors and counselors, and about 80% of the data capturers.
This had been particularly devastating because it was so abrupt, he said. An instruction by the US government in late-January required all grantees to stop their work immediately.
“There was no warning about this, had we had time, we could have made contingency plans and things wouldn’t be so bad,” he explained. “But if it happens literally overnight, it’s extremely unfair on the patients and remaining staff. The loss of capacity is significant.”
He said that nurses have started to take on some of the tasks that were previously performed by counselors, such as HIV testing. But these services haven’t recovered fully and things were still “chaotic”.
He added, “It’s not as if the department has any excess capacity, so [when] nurses are diverted to do the testing and counselling, then other parts of care suffer.”
Issue 2: PEPFAR programmes got bang for buck
Secondly, while PEPFAR may only have contributed 17% of the country’s total HIV spend, some researchers believe that it achieved more per dollar than many of the health department’s programmes.
Professor Francois Venter, who runs the Ezintsha research centre at WITS university, argued that PEPFAR programmes were comparatively efficient because they were run by NGOs that needed to compete for US funding.
“PEPFAR is a monster to work for,” said Venter, who has previously worked for PEPFAR-funded groups. “They put targets in front of these organisations and say: ‘if you don’t meet them in the next month, we’ll just give the money to your competitors’ and you’ll be out on the streets … So there’s no messing around.”
US funding agencies, he said, would closely monitor progress to see if organisations were meeting these targets.
“You don’t see that with the rest of the health system, which just bumbles along with no real metrics,” said Venter.
“The health system in South Africa, like most health systems, is not terribly well monitored or well directed. When you look at what you get with every single health dollar spent on the PEPFAR program, it’s incredibly good value for money,” he said.
Not only were the programmes arguably well managed, but PEPFAR funds were also strategically targeted. Public health specialist Lynne Wilkinson provided the example of the differentiated service delivery programme. This is run by the health department, but supported by PEPFAR in one key way.
Wilkinson explained that once patients are clinically stable and virally suppressed they don’t need to pick up their ARVs from a health facility each month as it’s too time-consuming both for them and the facility. As a result, the health department created a system of “differentiated service delivery”, in which patients instead pick up their medication from external sites (like pharmacies) without going through a clinical evaluation each time. But Wilkinson noted that before someone can be enrolled in that service delivery model, clinicians need to check that patients are eligible.
“Because [the enrollment process] was going very slowly … this was supplemented by PEPFAR-funded clinicians who would go into a clinic and review a lot of clients, and get them into that system”. By doing this, PEPFAR-funded staff successfully resolved a major bottleneck in the system, she said, reducing the number of people in clinics, and thus cutting down on waiting times.
Not everyone is as confident about the overall PEPFAR model. The former deputy director of the national health department, Dr Yogan Pillay, told Spotlight and GroundUp that we don’t have data on how efficient PEPFAR programmes are at the national level. This needs to be investigated before the health department spends its limited resources on trying to revive or replicate the programmes, argued Pillay who is now the director for HIV and TB delivery at the Gates Foundation.
While he said that many PEPFAR-funded initiatives were providing crucial services, Pillay also argued that “the management structure of the [recipient] NGOs is too top-heavy and too expensive” for the government to fund. Ultimately, we need to consider and evaluate a variety of HIV delivery models instead of rushing to replicate the PEPFAR ones, he said.
Issue 3: PEPFAR supported groups that the government doesn’t reach
An additional issue obscured by the 17% figure is that PEPFAR specifically targeted groups of people that are most likely to contract and transmit HIV, like people who inject drugs, sex workers, and the LGBTQ community. These groups, called key populations, require specialised services that the government struggles to provide.
Historically, PEPFAR has given NGOs money so that they could help key populations from drop-in centres and mobile clinics, or via outreach services. All of this operated outside of government clinics, because key populations often face stigma in these settings and are thus unwilling to go there.
For instance, while about 90% of surveyed sex workers say that staff at key populations centres are always friendly and professional, only a quarter feel the same way about staff at government clinics. This is according to a 2024 report, which also found that many key populations are mistreated and discriminated against at public health facilities. (Ironically, health system monitoring organisation Ritshidze, which conducted the survey, has been gutted by US funding cuts.)
While the key populations centres funded by the CDC are still operational, those funded by USAID have closed. The health department has urged patients that were relying on these services to go to government health facilities, but researchers argue that many simply won’t do this.
Venter explained: “For years, I ran the sex worker program [at WITS RHI, which was funded by PEPFAR] … Because sex workers don’t come to [health facilities], you had to provide outreach services at the brothels. This meant … we had to deal with violence issues, we had to deal with the brothel owners, and work out which days of the week, and hours of the day we could provide the care. Logistically, it’s much more complex than sitting on your bum and waiting for them to come and visit you at the clinic.
“So you can put up your hand and say: ‘Oh they can just come to the clinics’ – like the minister said. Well, then you won’t be treating any sex workers.” Venter said this would result in a public health disaster.
He argued that one of the most crucial services that key populations may lose access to is pre-exposure prophylaxis (PrEP), a daily pill that prevents HIV.
While the vast majority of government clinics have PrEP on hand, they often fail to inform people about it. For instance, a survey of people who are at high-risk of contracting HIV in KwaZulu-Natal found that only 15% were even aware that their clinic stocked PrEP.
Another large survey found that at government facilities, only 19% of sex workers had been offered PrEP. By contrast, at the drop-in centres for key populations, the figure was more than double this, at 40%. Without these centres, the health system may lose its ability to create demand for the drug among the most high-risk groups.
One health department official told Spotlight and GroundUp that the bulk of the PrEP rollout would continue despite the US funding cuts. “The majority of the PrEP is offered through the [government] clinics,” she said, 96% of which have the drug.
However, she conceded that specific high-risk groups like sex workers have primarily gotten PrEP from the key populations centres, rather than the clinics. “This is the biggest area where we are going to see a major decline in uptake for [PrEP] services,” she said.
600 000 dead without PEPFAR?
Overall, the USAID funding cuts have severely hindered the HIV testing programmes, data capturing services, PrEP roll-out, and follow-up services for people who interrupt ARV treatment. And the patients who are most affected by this are those that are most likely to further transmit the virus.
So what will the impacts be? According to one modelling study, recently published in the Annals of Medicine, the complete loss of all PEPFAR funds could lead to over 600 000 deaths in South Africa over the next decade.
While South Africa still retains some PEPFAR funding that comes from the CDC, beneficiaries are bracing for this to end. According to Wilkinson, the PEPFAR grants of most CDC-funded organisations end in September and future grants are uncertain. For some organisations, the money stops at the end of this month.
Meanwhile, if the government has any clear plan for how to manage the crisis, it’s certainly not making this public.
In response to our questions about whether the health department would be supporting key populations centres, the department’s spokesperson, Foster Mohale, said: “For now we urge all people living with HIV/AIDS and TB to continue with treatment at public health facilities.”
When pressed for details about the department’s plans for dealing with the US cuts, Mohale simply said that they could not reveal specifics at this stage and that “this is a work in progress”.
In his budget speech in Parliament on Wednesday, Finance Minister Enoch Godongwana did not announce any funding to cover the gap left by the abrupt end of US support for the country’s HIV response. Prior to the speech, Godongwana told reporters in a briefing that the Department of Health would assist with some of the shortfall, but no further information could be provided.
Photo by Miguel Á. Padriñán: https://www.pexels.com/photo/syringe-and-pills-on-blue-background-3936368/
By Ufrieda Ho
Amid major disruptions caused by aid cuts from the United States government, the health department aims to enrol a record number – an additional 1.1 million – of people living with HIV on life-saving antiretroviral medicine this year. Experts tell Spotlight it can’t be business as usual if this ambitious programme is to have a chance of succeeding.
Government’s new “Close the Gap” campaign launched at the end of February has set a bold target of putting an additional 1.1 million people living with HIV on antiretroviral treatment by the end of 2025.
Around 7.8 million people are living with HIV in the country and of these, 5.9 million are on treatment, according to the National Department of Health. The target is therefore to have a total of seven million people on treatment by the end of the year. Specific targets have also been set for each of the nine provinces.
The initiative is aimed at meeting the UNAIDS 95–95–95 HIV testing, treatment and viral suppression targets that have been endorsed in South Africa’s National Strategic Plan for HIV, TB, and STIs 2023 – 2028. The targets are that by 2030, 95% of people living with HIV should know their HIV status, 95% of people who know their status should be on treatment, and 95% of people on treatment should be virally suppressed (meaning there is so little HIV in their bodily fluids that they are non-infectious).
Currently, South Africa stands at 96–79–94 against these targets, according to the South African National Aids Council (SANAC). This indicates that the biggest gap in the country’s HIV response lies with those who have tested positive but are not on treatment – the second 95 target.
But adding 1.1 million people to South Africa’s HIV treatment programme in just ten months would be unprecedented. The highest number of people who started antiretroviral treatment in a year was the roughly 730 000 in 2011. In each of the last five years, the number has been under 300 000, according to figures from Thembisa, the leading mathematical model of HIV in South Africa. According to our calculations, if South Africa successfully adds 1.1 million people to the HIV treatment programme by the end of 2025, the score on the second target would rise to just above 90%.
The record for the most people starting antiretroviral treatment in a single year was approximately 730 000 in 2011. (Graph by Spotlight, based on Tembisa data.)
The ambitious new campaign launches at a moment of crisis in South Africa’s HIV response. Abrupt funding cuts from the United States government – the PEPFAR funding – has meant that the work of several service-delivery NGOs have ground to a halt in recent weeks.
These NGOs played an important role in getting people tested and in helping find people and supporting them to start and restart treatment. The focus of many of these NGOs was on people in marginalised but high-risk groups, including sex workers, people who use drugs and those in the LGBTQI community. As yet, government has not presented a clear plan for how these specialised services might continue.
“We will need bridging finance for many of these NGOs to contain and preserve the essential work that they were doing till we can confer these roles and responsibilities to others,” says Professor Francois Venter, of the Ezintsha Research Centre at the University of the Witwatersrand.
He says good investment in targeted funding for NGOs is a necessary buffer to minimise “risks to the entire South African HIV programme” and the looming consequences of rising numbers of new HIV cases, more hospitalisations, and inevitably deaths.
Disengaging from care
South Africa’s underperformance on the second 95 target is partly due to people stopping their treatment. The reasons for such disengagement from HIV care can be complex. Research has shown it is linked to factors like frequent relocations, which means people have to restart treatment at different clinics over and over. They also have to navigate an inflexible healthcare system. A systematic review identified factors including mental health challenges, lack of family or social support, long waiting times at clinics, work commitments, and transportation costs.
Venter adds that while people are disengaged from care, they are likely transmitting the virus. The addition of new infections for an already pressured HIV response contributes to South Africa’s sluggish creep forward in meeting the UNAIDS targets.
The health department has not been strong on locating people who have been “lost” to care, says Venter. This role was largely carried out by PEPFAR-supported NGOs that are now unable to continue their work due to the withdrawal of crucial US foreign aid.
Inexpensive interventions
Other experts working in the HIV sector, say the success of the Close the Gap campaign will come down to scrapping programmes and approaches that have not yielded success, using resources more efficiently, strategic investment, and introducing creative interventions to meet the service delivery demands of HIV patients.
Key among these interventions, is to improve levels of professionalism in clinics so patients can trust the clinics enough to restart treatment.
Professor Graeme Meintjes of the Department of Medicine at the University of Cape Town says issues like improving staff attitudes and updating public messaging and communications are inexpensive interventions that can boost “welcome back” programmes.
“The Close the Gap campaign must utilise media platforms and social media platforms to send out a clear message, so people know the risks of disengagement and the importance of returning to care. The longer someone interrupts their treatment and the more times this happens, the more they are at risk of opportunistic infections, severe complications, getting very sick and needing costly hospitalisations,” he says.
Clinics need to provide friendly, professional services that encourage people to return to and stay on treatment, Meintjes says, and services need to be flexible. These could include more external medicine pick-up points, scripts filled for longer periods, later clinic operating hours, and mobile clinic services.
“We need to make services as flexible as possible. People can’t be scolded for missing an appointment – life happens. Putting these interventions in place are not particularly costly, in fact it is good clinical practice and make sense in terms of health economics by avoiding hospitalisations that result from prolonged treatment interruptions,” he says.
The Close the Gap campaign, Meintjes adds, should reassure people that HIV treatment has advanced substantially over the decades. The drugs work well and now have far fewer side effects, with less risk of developing resistance. More patients are stable on the treatment for longer and most adults manage their single tablet once-a-day regime easily.
Insights from our experiences
Professor Linda-Gail Bekker, Chief Executive Officer at the Desmond Tutu Health Foundation, says to get closer to the target of 1.1 million people on treatment by year-end will mean using resources better.
“Additional funding is always welcome, so are new campaigns that catalyse and energise. But we also need to stop doing the things we know don’t have good returns. For instance, testing populations of people who have been tested multiple times and aren’t showing evidence of new infections occurring in those populations,” she says.
There is also a need for better data collection and more strategic use of data, Bekker says. Additionally, she suggests a status-neutral approach, meaning that if someone tests positive, they are referred for treatment, while those who test negative are directed to effective prevention programmes, including access to pre-exposure prophylaxis (PrEP) for people at high risk of exposure through sex or injection drug use.
But Bekker adds: “We need to be absolutely clear; these people aren’t going to come to us in our health facilities, or we would have found them already. We have to do the work that many of the PEPFAR-funded NGOs were doing and that is going to the last mile to find the last patient and to bring them to care.”
She says the impact of the PEPFAR funding cuts can therefore not be downplayed. “The job is going to get harder with fewer resources that were specifically directed at solving this problem.”
Venter names another approach that has not worked. This, he says, is the persistence of treating HIV within an integrated health system. Overburdened clinics have simply not coped, he adds, with being able to fulfil the ideal of a “one-stop-shop” model of healthcare.
Citing an example, he says: “Someone might come into a clinic with a stomach ache and be vomiting, they might be treated for that but there’s no investigation or follow-up to find out if it might be HIV-related, for instance. And once that person is out of the door, they’re gone.”
Campaign specifics still lacking
The Department of Health did not answer Spotlight’s questions about funding for the Close the Gap campaign; what specific projects in the campaign will look like; or how clinics and clinic staff will be equipped or supported in order to find the 1.1 million people. There is also scant details of the specifics of the campaign online.
Speaking to the public broadcaster after the 25 February campaign launch, Health Minister Dr Aaron Motsoaledi said South Africa is still seeing 150 000 new infections every year. He said they will reach their 1.1 million target through a province-by-province approach. He used the Eastern Cape as an example.
“When you look at the 1.1 million, it can be scary – it’s quite big. But if you go to the provinces – the Eastern Cape needs to look for 140 000 people. Then you come to their seven districts, that number becomes much less. So, one clinic could be looking for just three people,” he said.
Nelson Dlamini, SANAC’s communications manager, says the focus will be to bring into care 650 000 men, as men are known to have poor health-seeking habits. Added to this will be a focus on adolescents and children who are living with HIV.
He says funding for the Close the Gap campaign will not be shouldered by the health department alone.
“This is a multisectoral campaign. Other departments have a role to play, these include social development, basic education, higher education and training, etc, and civil society themselves,” Dlamini says.
The province-by-province approach to reach the target of finding 1.1 million additional people is guided by new data sources.
“Last year, SANAC launched the SANAC Situation Room, a data hub which pulls data from multiple sources in order for us to have the most accurate picture on the status of the epidemic,” says Dlamini.
These include the Thembisa and Naomi model outputs and data from the District Health Information System and Human Sciences Research Council, he says adding that SANAC is working to secure data sharing agreements with other sectors too.
Dlamini however says the health department, rather than SANAC, will provide progress reports on the 10-month project.
South Africa faces its worst health crisis in 20 years. Worse than COVID, and one that will overshadow diabetes as a major killer, while pouring petrol on a dwindling TB fire. But it is preventable if our government steps up urgently.
Nearly eight-million people have HIV in South Africa; they need life-long antiretroviral medicines to stay healthy.
The near-total removal of US government funding last week, a programme called PEPFAR, will see every important measure of the HIV programme worsen, including hospitalisations, new infections in adults and children, and death. Unless government meaningfully steps in to continue funding the network of highly efficient organisations that currently fill key gaps in national care, an epidemic that was tantalisingly close to coming under control will again be out of our reach. Millions of people in South Africa will become infected with HIV and hundreds of thousands more will die in the next ten years. 2025 will end much more like 2004, when we started our HIV treatment programme.
Many fail to recognize the danger. Commentators, public health officials, and government spokespeople have downplayed the US financial contributions to the HIV response, suggesting services can be absorbed within current services. The funding cuts amount to approximately 17% of the entire budget for HIV and largely go to salaries for health staff. On the face of it, this indeed seems replaceable. So why are the consequences so deadly?
To understand the impact, one must recognize how US funding has supported HIV care. The money is largely allocated to a network of non-government organisations through a competitive, focused, and rigorously monitored program in four key areas:
Active case finding: The best way to prevent new cases of HIV is find everyone with the disease early on, and get them on treatment. These organisations deploy people in high-risk areas, to test for HIV and screen for TB, and shepherd people who test positive to treatment programmes. People are almost always healthy when they start treatment, and remain healthy, with greatly reduced time to transmit the virus, and much less chance of ever “burdening” the health sector with an opportunistic infection. They are hugely cost-effective.
Tracing people who disappear from care: Patients on antiretrovirals fall out of care for many reasons, ranging from changing their address, to life chaos such as losing their job or mental illness. Or they are simply mixed up in the filing dysfunction within clinics. The US supported programmes helped finding people ‘lost from care’, maintaining systems able to track who has not come back, and how to contact them, often spending considerable time cleaning redundant records as people move between facilities.
Vulnerable population programmes: Services include those for sex workers, LGBTQ+ people, adolescents, people who use drugs, and victims of gender violence. These programs are for people who need tailored services beyond the straightforward HIV care offered in state clinics. They are often discriminated against in routine services and also at significant risk of contracting HIV.
Supporting parts of the health system: This includes technical positions supporting medicine supply lines, laboratories and large information systems, as well as organisations doing advocacy or monitoring the quality of services. All of this keeps the health system ticking over.
In central Johannesburg, where I work, HIV testing services have collapsed. The people who fell out of programmes are not coming back. HIV prevention and TB screening have largely stopped.
Reassurances that state clinics will pick up testing are empty – the staff do not exist, and testing has not resumed. State clinics do not trace people who fall out of care for any illness, let alone for HIV. The data systems maintained by PEPFAR-supported organisations are now gone.
What happens now? The first hard sign that things are failing will be a large drop in the number of people starting treatment, versus what happened in the same month one year ago. The next metric to watch will be hospitalisations for tuberculosis and other infections associated with untreated HIV infection. This will happen towards the end of the year, as immune systems fail. Not long after, death rates will rise. We will see that in death certificates among younger people – the parents and younger adults.
Unfortunately, much of this information will not be available to the health department for at least a year or two, because among the staff laid off in this crisis are the data collectors for the programmes that tracked vital metrics.
The above should come as no surprise, especially to the public health commentators and health department, which is why it is so surprising to hear how certain they are that the PEPFAR programme can easily be absorbed into the state services. The timing of this crisis could not be worse, with huge budget holes in provincial health departments.
Why should this be a priority? After starting the HIV programme in 2004, we spent the next few years muddling through how to deliver antiretrovirals to millions of people in primary care, before we realised we also needed to diagnose them earlier. In 2004, the average CD4 count (a measure of immune strength) at initiation of treatment was about 80 cells/ul, devastatingly low – normal is > 500 cells/ul. A quarter were ill with TB.
This CD4 count average took years to go up, but only by pushing testing into clinic queues, communities, and special services for key populations, not waiting till they were sick. Recently, the average initiation CD4 count was about 400 cells/ul, stopping years of transmission, with most people healthy, and only a small number with TB.
There are many reasons to criticise the relationship between PEPFAR and the health department. It suited both parties to have a symbiotic relationship that meant each got on with their job and ticked their respective output boxes, but neither had to tussle with the messiness of trying to move the PEPFAR deliverables into the health department. As we move forward, learning from these fragilities to plan for the future of the HIV care programme, and for other diseases, will be critical.
Since the suspension of funding, many people have said, “We don’t hear much about HIV anymore”. That is because when the system works well, you don’t hear about it. Some things are far better compared to 2004:
We have a government not in denial about HIV being a problem nor encouraging pseudoscience or crackpots.
Our frontline health workers, in over 3000 clinics, have vast experience initiating and maintaining antiretrovirals.
Antiretrovirals are cheaper, more potent, more durable, and safer.
Treatment protocols are simpler.
New infection rates are way down.
Government delivery systems have improved.
Data systems suggest that the majority of ‘lost’ patients are in care, often simply in another clinic.
A sensible emergency plan would do this:
Fund existing programmes for a limited time, understanding that the level of reach and expertise is impossible for the health department to replicate at short notice.
Couple this with a plan to make posts more sustainable over the next year or two.
Learn from the PEPFAR programme that rigorously held organisations accountable, so that provinces can similarly be answerable for their HIV metrics.
Ask hard questions why single patient identifiers, and government information systems, that could easily be linked to laboratory, pharmacy and radiology databases, are still not integrated within the public systems, as they are throughout the private health system.
Accept that certain key functions and clinics may best be sited outside of the health department.
This will not save the large and valuable research programmes, which need other help. Much of the rest of Africa needs a Marshall Plan to rescue their entire HIV service, as they are almost totally dependent on US government funding.
But ideas like the above will preserve the current South African HIV response and allow us to imagine interventions that could end the disease as a threat for future generations.
No one disputes we need a move away from donor-assisted health programmes. But the scale and immense urgency of this oncoming emergency needs to be understood. We need a plan and a budget, and fast. Or we will have an overwhelmed hospital system and busy funeral services again.
Professor Francois Venter works for Ezintsha, a policy and research unit at Wits. He has been involved in the HIV programme since 2001, and ran several large PEPFAR programmes till 2012. Venter and his unit do not receive funding from PEPFAR, USAID or CDC. Thank you to several experts for supplying analysis and ideas for the initial draft of the article.
Cuts to United States spending on aid and medical research have caused widespread havoc and anxiety in the last month. Professor Tulio de Oliveira sat down with Spotlight’s Biénne Huisman to talk through what it might mean for health research in South Africa.
As the Trump administration moves to freeze foreign aid, halting vital humanitarian health programmes and medical research trials worldwide – leaving patients cut off from lifesaving medicines and scientists in a bind – Professor Tulio de Oliveira argues that the United States stand to lose far more from this move than its 1% government investment in foreign aid.
The non-partisan Pew Research Center recently released figures showing that of the American government’s total 2023 budget, 1.2% or about $71.9 billion was spent on foreign aid. Of this foreign aid budget, 14.7% or about $10.6 billion was earmarked for the “ongoing battle against HIV/AIDS” and 2% or about $1.5 billion for “combatting pandemic influenza and other emerging public health threats”.
Speaking to Spotlight in a boardroom at the Centre for Epidemic Response and Innovation (CERI) at Stellenbosch University, De Oliveira says: “Spending on biosecurity is an investment in the future – I think the United States benefits much more from our research and our work than what we cost them.” Biosecurity refers to measures designed to protect populations against harmful biological or biochemical substances.
During the height of the COVID-19 pandemic, De Oliveira, a professor in bioinformatics, shot to global attention for leading the South African team credited with discovering the Beta and Omicron variants of SARS-CoV-2. Now, in the face of a new global health upheaval, he insists that cross-border scientific collaboration is critical for combating the global spread of disease.
“Pathogens don’t need passports, they don’t care about nationality,” he says, referencing former World Health Organisation Director-General, Dr Margaret Chan, who first used the phrase at the 2007 World Health Assembly.
Professor Tulio de Oliveira. (Photo: Supplied)
De Oliveira is a native Brazilian who speaks accented English. During his interview with Spotlight, his demeanour is calm and his speech unrushed as he expands: “It’s of great interest to America to keep investing – not as a kind of donation, or because we’re entitled to it – but because of how it helps them. We just came out of a pandemic and America actually had much bigger waves of infection than many of the poor countries.”
He lists recent global population health threats: “Like with Covid, now we have influenza; and the virus is mutating, transmitting through multiple animals. We just had an outbreak of Marburg in Rwanda and another one in Kenya. We had an emergence of mpox in central Africa. We had an emergence in Sudan of a strain of Ebola. In Uganda, a growing rate of malaria drug resistance.
“And in the last year, the US saw the biggest number of TB cases ever. So it’s of critical interest that these pathogens get quickly identified, are quickly controlled, that you treat people so that it doesn’t spread to other countries. In the end, it’s the health of the global population, it doesn’t matter which country we live in or how wealthy people are.”
Major funding cuts
Scores of South African research groups (many who provide affiliated public healthcare services) have in the past received funding from United States government entities – including the National Institutes of Health (NIH), the Centers for Disease Control and Prevention (CDC), USAID, and the President’s Emergency Plan for Aids Relief (PEPFAR).
Many of these funding flows have been paused in recent weeks by the Trump administration. As a result, several important clinical trials have been stopped. The impacts are far-reaching – around 28% of the South African Medical Research Council’s (SAMRC) 2025/2026 budget was set to be funded by US government entities. Professor Ntobeko Ntusi, President of the SAMRC, told Spotlight that it would be catastrophic if the funding is cut.
Adding further uncertainty, prominent vaccine sceptic Robert F. Kennedy has been confirmed as the US’s health secretary under the Trump administration. Kennedy has argued that the NIH should reduce its focus on infectious diseases and dedicate more resources to non-communicable diseases like diabetes. The US government has until now been by far the biggest funder of both HIV and TB research.
De Oliveira appears unflustered. At CERI, of which he is the founding director, he says only 7% of funding is from the NIH – “and we have reason to believe that the current NIH grants that we have will not be discontinued”. One such grant was for R40 million over five years awarded in 2023 to CERI’s Professor Frank Tanser for designing HIV prevention strategies.
In fact, De Oliveira says CERI and the KwaZulu-Natal Research Innovation and Sequencing Platform (KRISP) which he also heads, are expanding. Both centres use state-of-the-art genomics – the study of the DNA of organisms – to identify new variants of pathogens and to prevent disease.
“Yes, the opposite, we’re in an expansion phase,” says De Oliveira.
“Just last week, we advertised five post-doctoral fellowship positions. We hope that we can even absorb some of the great talent that may be lost from groups that were unfortunately more reliant on American funding.”
He stresses the importance of having a diversified funding portfolio, saying the work of CERI and KRISP is funded through 46 active grants with another 9 in the offing. “We have multiple grants from multiple funders from multiple countries. So again, I know it’s easily said, but I think it’s something that we should learn going forward, not to grow too reliant on one funder.”
Filling the gap
If the United States pulls back permanently from its leadership role in providing global aid – and medical research funding in particular – who might fill the gap?
The New Yorker quotes Clemence Landers, vice-president of the think tank Centre for Global Development, suggesting that China might come forward.
In response, De Oliveira says: “China could fill the gap. But people don’t realise the biggest foundation in the world at the moment is called the Novo Nordisk Foundation in Denmark which is linked to the company that had the massive breakthrough with Ozempic. They could easily fill the gap if they wanted. There are others as well. I would not be surprised if a completely unexpected foundation came forward to fill the gap.”
Reflecting further, he expresses hope that “people with noble causes step up”.
In 2022, TIME Magazine named De Oliveira one of the world’s 100 most influential people, and in 2024 he cracked the magazine’s top 100 health list. Has this public recognition made it easier for him to attract funding? He shrugs this off.
“We’re really committed to having a global impact that saves lives. And that commitment is not centralised in the director, but in our vision shared across principal investigators. And this is really important for the sustainability of organisations. I get offered good jobs every couple of weeks, and I mean even though I don’t intend on going anywhere, anything could happen. For example, two weeks ago I was skateboarding and cracked my ribs.”
In a moment of levity, he elaborates: “And this is the fifth time I cracked my ribs. Once was while skateboarding, another while snowboarding, surfing, once while mountain biking and another time falling from a children’s tractor.”
De Oliveira moved to South Africa in 1997, as the AIDS crisis was heading toward its peak. He says he feels “eternally grateful” for the boost PEPFAR brought to South Africa’s HIV-programme, adding that today the country might be in a “better position to absorb the loss of the funding than say five, ten years ago”.
He notes that 17% of South Africa’s HIV/AIDS spending was from PEPFAR, but that this does not include the procurement of antiretrovirals. “So yes, I think as South Africans we might be in a position to come up with solutions, as the programme is very well run.”
De Oliveira’s concern is for more vulnerable African countries – he singles out Mozambique – which are reliant on foreign aid for the procurement of medicines like antiretrovirals.
Needless to say, these recent events are a setback in the quest to develop an HIV vaccine. “When you decrease investment in research and science, you keep further away from developing the solutions,” he says. “But in terms of HIV/AIDS, luckily there are antiretroviral therapies that are very efficient.”
As we wrap up the interview, De Oliveira zooms out to the bigger picture: “Unfortunately, we are destroying the environment, there’s increased globalisation and crazy urbanisation, and this is making it easier for infectious diseases to spread.
“This is a challenging time for scientific and medical research. A time to develop solutions.”
Numerous South African health projects funded by the US President’s Emergency Plan for AIDS Relief (PEPFAR) remain closed. This is despite a federal court judgment which ordered President Donald Trump’s administration to lift the blanket freeze on global aid.
A waiver on life-saving humanitarian services appears to have had little effect. Funding remains frozen for many projects that provided services explicitly covered by the waiver, such as antiretroviral (ARV) medicines for people with HIV.
A spokesperson for one of these projects said that the United States Agency for International Development Aid (USAID) had not provided any communication regarding the waiver, despite requests for information.
A second organisation said USAID instructed it to provide an adapted budget that only covers services included in the waiver. The organisation submitted it, but it has not yet been approved. The organisation supports orphaned children living with HIV.
CDC funding
PEPFAR is a US initiative that provides billions of dollars a year toward combating HIV in different parts of the world. These funds are primarily distributed through two agencies: USAID and the Centers for Disease Control and Prevention (CDC).
In late January USAID issued stop-work orders to the organisations which it funds. A few days later, the CDC did the same. This was after an executive order by Trump which paused foreign development funding for 90 days pending a review. As a result, US-funded health organisations across South Africa were forced to close their doors. In some cases, HIV patients were left without ARVs.
Last week the CDC issued notifications to its recipient organisations rescinding the stop-work orders. The CDC stated that this was because of a temporary restraining order issued by a federal judge in Rhode Island that halted the Trump administration’s ability to freeze congressional funds. Since then, many South African organisations that get money from the CDC have reopened.
But USAID did not send out similar notifications. PEPFAR funds from this agency largely remain frozen.
In a separate judgment on 13 February, a federal judge in Washington DC blocked the implementation of Trump’s executive order to freeze foreign aid. The administration’s lawyers have argued that the US government can continue to freeze aid via other channels unrelated to the executive order.
Dangerous disruption
GroundUp and Spotlight visited three health centres in South Africa funded by USAID, and found all three remained closed. Representatives from a fourth USAID-funded organisation confirmed that its funding has not been restored, and that its partner organisation was in the same boat.
The first centre that we visited is a clinic in Rosebank, Johannesburg, run by OUT LGBT Wellbeing. It provided free HIV testing, ARVs, and the daily HIV-prevention pill (this is referred to as Pre-exposure Prophylaxis or PrEP). It’s one of several US-funded clinics that OUT operates around the country.
Its services are geared toward men who have sex with men. The reason is that rates of HIV are high among this group, and stigma may prevent some from seeking help in general healthcare settings.
When we visited the centre in Rosebank, a note was tied to the gate, stating: “Regrettably our clinic is temporarily closed and consequently no health services are available”. It encouraged patients to go to their nearest health facility.
According to OUT spokesperson Luiz De Barros, the clinics were forced to halt immediately after stop-work orders were issued. This prevented them from making alternative plans, leaving many people without ARVs or PrEP.
He said the centres had a total of 84 staff, who are now “at home without pay”, and about 5000 clients. Without their ARVs, De Barros worries that many clients are at risk of falling ill or developing drug-resistant HIV. Stopping HIV prevention services like PrEP will also “heighten the spread of HIV within communities,” he noted.
De Barros said they had not yet received any communication from USAID about the limited waiver, despite asking for information.
A clause in the waiver says it does not apply to “gender or DEI [diversity, equality and inclusion] ideology programs”. The Trump administration has not spelled out exactly what these terms mean, but it appears that DEI includes any health project which targets particular groups, like LGBTQ people.
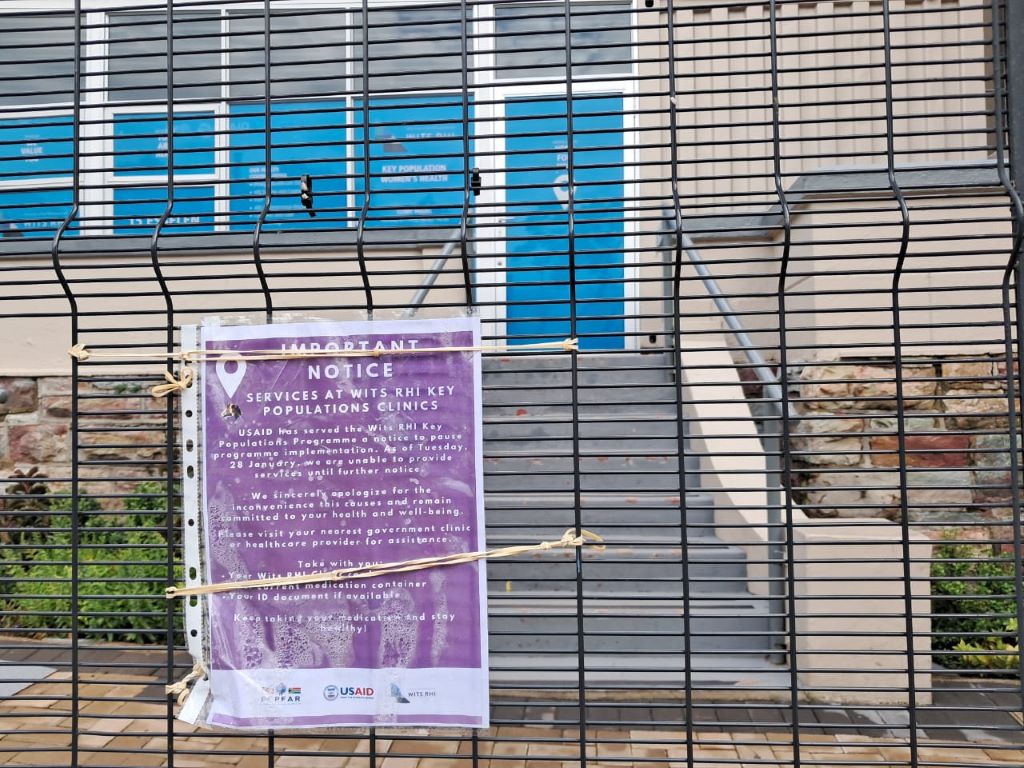
GroundUp and Spotlight visited a second health centre in Hillbrow run by the WITS Reproductive Health Institute (RHI). A sign on the gate stated: “USAID has served the WITS RHI Key Populations Programme a notice to pause programme implementation. As of Tuesday, 28 January, we are unable to provide services until further notice.”
WITS RHI’s annual reports suggest that USAID has previously sponsored its projects to treat and prevent HIV, including among high-risk groups like sex workers and transgender people.
The third health facility that we visited is the Ivan Toms Centre for Health, based in Green Point, Cape Town. A temporary closure notification hung from the door. The centre provided HIV and TB testing, ARVs, PrEP, and counselling services – all focused on men who have sex with men.
Representatives from a fourth organisation, NACOSA, told GroundUp and Spotlight that it had been forced to halt all of its USAID-funded services. Subsequently, USAID instructed the organisation to provide a revised budget which only includes activities listed under the waiver. As part of this limited budget, NACOSA proposed retaining a project which helps orphaned and vulnerable children living with HIV in the Western Cape.
Dr Ntlotleng Mabena, a technical specialist at NACOSA, said the project provides these children with psychological support and connects them to health providers. Clinical workers linked to the ANOVA health institute (which is also US-funded) provide the children with ARV treatment, she said.
NACOSA submitted the revised budget with the hope of restarting this service, but they are still awaiting approval. Mabena stated that ANOVA was also waiting for permission to continue. In the meantime, the service remains closed.
The US embassy in South Africa maintains that Trump’s funding cuts do not affect PEPFAR initiatives that provide life-saving services as defined in the limited waiver.
Yet all of the life-saving PEPFAR services that we investigated on Thursday are closed. The only services which have reopened are those funded by the CDC, which is unrelated to the waiver.
Sign outside a Wits RHI clinic in Johannesburg. Photo: Ihsaan Haffejee
South Africa’s National Department of Health is still to outline a clear contingency plan as a United States (US) funding freeze puts lives at risk, spells job losses, and presents threats to keeping HIV and TB under control.
The ripple effects of US President Donald Trump’s 90-day freeze of funding on foreign aid programmes have hit South Africa hard. The damage is being counted at multiple levels – even as some limited funding flows are being restored.
For the country, the fallout has heightened civil society’s calls for a prompt, implementable plan to fill the gaps in care and services. Also needed, they say, is clarity on longer-term strategies for greater self-sufficiency in the country’s HIV responses as donor-funded models look increasingly precarious. Such an argument for increased independence in Africa and the global south was made by president of the South African Medical Research Council (SAMRC), Professor Ntobeko Ntusi, writing in the journal Nature.
South Africa should have been better prepared and not caught off guard to be left in the position it now finds itself in, some beneficiaries of US-funded projects told Spotlight. They were speaking on condition of anonymity, given the risk of public comments jeopardising their prospects of having their funding restored.
The immediate need is to ensure that the country’s overburdened and under-resourced public clinic system is able to absorb the tens of thousands of people living with HIV who will have to use public facilities. This is partly because the NGOs they have relied on have been forced to close shop – virtually overnight. Clinics catering to specific groups, such as men who have sex with men, have been particularly hard hit.
South Africa is the largest global recipient of President’s Emergency Plan for Aids Relief (PEPFAR) funds. These funds make its way to South Africa through the United States Agency for International Development (USAID) and the Centers for Disease Control and Prevention (CDC). Through PEPFAR, USAID has been funding and supporting local NGOs and our Department of Health for around two decades. According to USAID’s website, it invested $5.6 billion (roughly R100 billion at the current rand/dollar exchange rate) between 2004 and 2020 towards prevention and treatment of HIV and TB in South Africa.
Trump’s initial executive order, signed on 20 January, halted funding received via USAID. USAID is an agency of the US government that now falls under the State Department under the leadership of Secretary of State Marco Rubio. Since taking office, Trump has slated USAID as “corrupt” and run by “radical left lunatics”.
The Washington head offices of USAID were closed on Friday 7 February as per Trump’s orders and even as the 90-day review period had just got underway, signage on the building was being removed or taped over. Trump’s actions have now been challenged in courts with successful temporary blocks to his orders to place 2 200 USAID workers in the US on paid leave and to reinstate 500 US-based staff who were already placed on administrative leave from when the order was first signed. The situation is highly fluid and several court actions remain in progress.
Some limited relief
In South Africa, NGOs that received USAID funding remain largely in limbo. Although the United States mission in South Africa confirmed that some PEPFAR-funded services could continue in the country, it is subject to some relatively strict limitations and with no assurances of longer term support. As is clear from reporting by Bhekisisa, the process to get at least some funding to flow again to PEPFAR-supported projects is not straight forward.
There was some good news this week linked to PEPFAR-funding channelled through the CDC – a US federal agency under the Department of Health and Human Services. Following a court order, organisations getting these funds should for now be able to continue their work. However, the court process is far from over and the future prospects of NGOs that depend on CDC funds remains precarious.
Given these ongoing uncertainties and severe disruptions to cash flows, Spotlight understands that some large NGOs may have to close down, while others may have to drastically reduce their services. As reported by Spotlight and GroundUp, several NGOs have appealed to the private sector for assistance. As it stands, thousands of people employed or contracted by local NGOs face the loss of their jobs, cut-backs and deepening anxiety over income security. These people include community health workers, peer counsellors, patient navigators, community activists and advocates, support and administrative staff members, and contract workers who keep these organisations functioning.
At stake too are specialised services for so-called key populations such as sex workers, men who have sex with men, the LGBTQI+ community, and people who use drugs. Until recently, a focus on improving services for key populations was generally accepted, including by PEPFAR, to be the right strategy given the disproportionate risk of HIV infection in these groups. But under the Trump administration’s “anti-woke” agenda, it seems likely that many services aimed at key populations are set to be defunded.
A White House media note on 29 January made clear the US’s stance: “The previously announced 90-day pause and review of U.S. foreign aid is already paying dividends to our country and our people. We are rooting out waste. We are blocking woke programs. And we are exposing activities that run contrary to our national interests. None of this would be possible if these programs remained on autopilot.”
A timeline of the US aid cuts
20 January
90-day pause
In an executive order, US President Donald Trump orders a 90-day pause in US foreign development for “assessment of programmatic efficiencies and consistency with United States foreign policy”.
26 January
USAID funding paused
US Secretary of State Marco Rubio pauses all US foreign assistance funded by or through the State Department and US Agency for International Development (USAID) for review.
28 January
Waiver issued
Subject to certain conditions, Rubio issues a waiver stating: “Implementers of existing life-saving humanitarian assistance programs should continue or resume work if they have stopped.”
1 February
Waiver clarified
The extent of the January 28 waiver is clarified in a memo from the US Department of State.
5 February
Health portfolio committee briefing
South Africa’s Health Minister Dr Aaron Motsoaledi briefs Parliament on the US funding cuts and their impact on healthcare services.
7 February
South Africa singled out
In an executive order applying only to South Africa, Trump orders that “the United States shall not provide aid or assistance to South Africa”.
10 February
Waiver still applies
The US mission in South Africa releases an FAQ in which they state that PEPFAR activities that fall under the limited waiver will resume despite the February 7 executive order.
12 February
CDC grants reinstated
The grants of NGOs receiving support through the CDC are reinstated following a court order issued in a US court.
Crisis of fear, silence, and uncertainty
Spotlight understands that staff of affected NGOs have essentially been forbidden from speaking publicly about the 90-day funding freeze. Many declined to speak on the record to Spotlight, even anonymously – too afraid it might affect the decision on their funding after the 90-day review period.
According to an FAQ by the US mission in South Africa that was published on February 10, they have been communicating with the South African government, though it is not clear when this happened. Five days earlier on 5 February, Health Minister Dr Aaron Motsoaledi told Parliament’s Portfolio Committee that he had not had any official communication from the US government on the matter.
Figures from Motsoaledi’s presentation showed that in 2023/2024, PEPFAR funding to South Africa’s health department amounted to 17% of its spending on HIV. Funding totals R4.6 billion for staffing and R2.9 billion for running costs for NGOs. These NGOs include organisations working directly with people living with HIV, mobile units and youth organisations and programmes. PEPFAR focuses on the 27 districts in South Africa with the highest disease burden.
The health department did not respond to Spotlight’s questions on contingencies, or details of next steps to fill the funding gaps or how capacity and resources will be redirected to avert catastrophe. Motsoaledi did not give any of these details in his presentation to Parliament either.
What he did say was that since Trump’s executive order came into place, the health department had hosted a meeting with the provincial leads on HIV and TB; conducted assessments on the immediate impacts of the executive order; met with people living with HIV and engaged with SANAC to finalise a sustainability framework.
A collective of activist organisations, including the Health Justice Initiative, SECTION27, the Cancer Alliance, Treatment Action Campaign, Sweat, PSAM and the African Alliance, have pressed the Department of Health to create an “urgent co-ordinated emergency plan” along with an increased budget to avert a looming disaster.
The activists highlighted that despite the announcement by the Trump administration that some NGOs could apply for a waiver, many have had no practical way to do so without ways to communicate with their USAID contacts. This as USAID employees were placed under a work stop order and were shut out of their offices and denied access to their work emails.
The appeal from the collective also extends to protecting the work of academic and clinical research in the fields of HIV, TB, and cervical cancer that will also be affected by the funding freeze. As Spotlight reported, around 28% of the South African Medical Research Council’s budget for 2025/2026 was set to come from the United States government.
An ‘unreal world’
Professor Linda-Gail Bekker, chief executive officer at the Desmond Tutu Health Foundation, said Trump’s actions put in jeopardy the goal to finally have epidemic control of HIV – and right at the final hurdles.
“We have made amazing progress. And thank you to PEPFAR that helped us to get this far, but the work is not over. For the US to pull out at this point is a massive loss of investment; it’s also regression. It’s like getting to the end of a book but having the last chapters torn out before you can read it,” said Bekker.
She said PEPFAR funding has made it possible to build a formidable cohort of lay and professional people trained and dedicated to their roles that supported public healthcare in the most critical ways.
“These are individuals who distribute antiretrovirals, distribute pre-exposure prophylaxis, find and trace individuals who’ve been lost to care. They take services into communities, to outside of the health facilities, and made the effort to go the last mile to find those individuals – that is how you close down the epidemic,” Bekker said.
Her caution too is that loosening a grip on HIV control means potential surges in tuberculosis. “HIV and TB track together all the time, and an HIV epidemic that is once again out of control, almost certainly means what will follow is a TB epidemic that is out of control,” Bekker said.
Trump has created an “unreal world”, said Dr Andy Gray of the University of KwaZulu-Natal, who has also worked with the World Health Organization (WHO) in various capacities over two decades. “People are being held to ransom; and people are scared.”
“We have always been used to the oscillation between the United States’ Republican and Democratic administrations; things may be a little uncomfortable or there may be some disruption, but not this ‘let’s burn down the house’ approach taken by the Trump administration,” he said.
“There is no consideration of human rights or for human beings anywhere in the world, including America,” he added, pointing out too that the CDC has for the first time in 60 years been instructed to cease publishing weekly mortality and morbidity data, despite a breakout of avian flu (H5) in the country.
For Gray, South Africa’s strategic health response in the wake of this crisis should be to shift from a donor-funded model. His concern, however, is that with a stretched South African purse and with competing priorities, the HIV response will slip down the list.
Gray said that better self-sufficiency comes from eliminating waste, investing in employing the right people in the right jobs as well as investing in efficient systems.
He added that National Treasury will have to redirect money for the interim shortfall left by the US funding freeze, and provinces will have to step up by getting their houses in order.
South Africa, he warned, should ready itself for the “worst case scenario” once the 90-day review period is up.
SANAC response
The South African National AIDS Council (SANAC) role is meant to bring together government, civil society and the private sector to create a collective response to HIV, TB and STIs in South Africa. But if there is a crisis strategy from the council, it has not yet been announced.
SANAC head of communications, Nelson Dlamini, said that they have been left in a position of not being able to engage publicly because they haven’t had any direct communication with PEPFAR’s and USAID representatives based in Pretoria.
“PEPFAR is a government-to-government agreement and there ought to be official communication with the government of South Africa so we know what this means for our working relationship, but nothing has been forthcoming,” said Dlamini. “SANAC is a co-ordinator so we have to still coordinate. We are engaging in the background with relevant structures but we can’t say we are doing X, Y, Z till we have a sit down with PEPFAR,” he said.