In an analysis of information on adults with colorectal cancer, patients who also had diabetes, particularly those with diabetic complications, faced a higher risk of early death. The results are published in CANCER, a peer-reviewed journal of the American Cancer Society.
For the study, Kuo‐Liong Chien, MD, PhD, of National Taiwan University, and his colleagues examined data registered between 2007 and 2015 in the Taiwan Cancer Registry Database, which is linked to health insurance and death records. Their analysis included 59 202 individuals with stage I–III colorectal cancer who underwent potentially curative surgery to remove their tumours. Among these patients, 9448 experienced a cancer recurrence and 21 031 died from any cause during the study period.
Compared with individuals without diabetes, those with uncomplicated diabetes were at a minimally or insignificantly higher risk of all‐cause and cancer‐specific death, whereas those with complicated diabetes had 85% higher odds of death from any cause and 41% higher odds of death from cancer. These associations were more pronounced in women and in patients with early‐stage colorectal cancer.
Also, compared to patients without diabetes, patients with uncomplicated or complicated diabetes had a 10–11% higher risk of colorectal cancer recurrence.
The mechanisms behind the relationship between diabetic severity and poor colorectal cancer prognosis could involve various pathways and responses triggered by high insulin and glucose levels in the blood, as well as elevated inflammatory states, which are characteristic of type 2 diabetes.
“While a higher diabetes prevalence was noted in patients with colorectal cancer, the study suggests that coordinated medical care involving multiple specialists can help prevent diabetes complications, potentially improving long-term colorectal cancer oncological outcomes, particularly in women and patients with early-stage cancer,” said Dr Chien.
A new study appearing in Cell Medicine Reports suggests that an existing drug could be repurposed to treat type 1 diabetes, potentially reducing dependence on insulin as the sole treatment.
Type 1 diabetes, an autoimmune disease which attacks insulin-producing beta cells in the pancreas, is traditionally managed by replacing the missing insulin with injections which, though effective, can be expensive and burdensome.
The research, led by researchers at the University of Chicago Medicine and Indiana University, focuses on α-difluoromethylornithine (DFMO), which inhibits an enzyme that plays a key role in cellular metabolism. The latest translational results are a culmination of years of research: In 2010, while corresponding author Raghu Mirmira, MD, PhD, was at Indiana University, he and his lab performed fundamental biochemistry experiments on beta cells in culture. They found that suppressing the metabolic pathway altered by DFMO helped protect the beta cells from environmental factors, hinting at the possibility of preserving and even restoring these vital cells in patients diagnosed with type 1 diabetes.
The researchers confirmed their observations preclinically in zebrafish and then in mice before senior author Linda DiMeglio, MD, MPH, Edwin Letzter Professor of Pediatrics at Indiana University School of Medicine and a pediatric endocrinologist at Riley Children’s Health, launched a clinical trial to evaluate the safety and tolerability of the drug in type 1 diabetes patients. The results of the trial, which was funded by the Juvenile Diabetes Research Foundation (JDRF) and used DMFO provided by Panbela Therapeutics, indicated that the drug is safe for type 1 diabetes patients and can help keep insulin levels stable by protecting beta cells.
“As a physician-scientist, this is the kind of thing we’ve always strived for – to discover something at a very basic, fundamental level in cells and find a way to bring it into the clinic,” said Mirmira, who is now Professor of Medicine and an endocrinologist at UChicago Medicine. “It definitely underscores the importance of supporting basic science research.”
“It’s been truly thrilling to witness the promising results in the pilot trial after this long journey, and we’re excited to continue our meaningful collaboration,” said DiMeglio.
Importantly, DFMO has already been FDA-approved as a high dose injection since 1990 for treating African Sleeping Sickness and received breakthrough therapy designation for neuroblastoma maintenance therapy after remission in 2020. Pre-existing regulatory approval could potentially facilitate its use in type 1 diabetes, saving effort and expense and getting the treatment to patients sooner.
“For a drug that’s already approved for other indications, the approval timeline can be a matter of years instead of decades once you have solid clinical evidence for safety and efficacy,” said Mirmira. “Using a new formulation of DFMO as a pill allows patients to take it by mouth instead of needing to undergo regular injections, and it has a very favorable side effect profile. It’s exciting to say we have a drug that works differently from every other treatment we have for this disease.”
To follow up on the recently published results, a multi-centre clinical trial was launched to gather even stronger data regarding the efficacy of DFMO as a type 1 diabetes treatment.
“With our promising early findings, we hold hope that DFMO, possibly as part of a combination therapy, could offer potential benefits to preserve insulin secretion in individuals with recent-onset type 1 diabetes and ultimately also be tested in those who are at risk of developing the condition,” said Sims.
“A new era is dawning where we’re thinking of novel ways to modify the disease using different types of drugs and targets that we didn’t classically think of in type 1 diabetes treatment,” said Mirmira.
The synthetic melanin is being applied to inflamed skin. Just under the surface of the skin are green free radicals, also known as reactive oxygen species (ROS). Credit: Yu Chen, Northwestern University
Imagine a skin cream that heals damage occurring throughout the day when your skin is exposed to sunlight or environmental toxins. That’s the potential of a synthetic, biomimetic melanin developed by scientists at Northwestern University.
In a new study, published in Nature npj Regenerative Medicine, the scientists show that their synthetic melanin, mimicking the natural melanin in human skin, can be applied topically to injured skin, where it accelerates wound healing. These effects occur both in the skin itself and systemically in the body.
When applied in a cream, the synthetic melanin can protect skin from sun exposure and heals skin injured by sun damage or chemical burns, the scientists said. The technology works by scavenging free radicals, which are produced by injured skin such as a sunburn. Left unchecked, free radical activity damages cells and ultimately may result in skin aging and skin cancer.
Melanin in humans and animals provides pigmentation, protecting cells from sun damage with increased pigmentation in response to sunlight. That same pigment in skin also naturally scavenges free radicals in response to damaging environmental pollution from industrial sources and automobile exhaust fumes.
Everyday skin injury
“People don’t think of their everyday life as an injury to their skin,” said co-corresponding author Dr. Kurt Lu, the Eugene and Gloria Bauer Professor of Dermatology at Northwestern University Feinberg School of Medicine and a Northwestern Medicine dermatologist. “If you walk barefaced every day in the sun, you suffer a low-grade, constant bombardment of ultraviolet light. This is worsened during peak mid-day hours and the summer season. We know sun-exposed skin ages versus skin protected by clothing, which doesn’t show age nearly as much.”
The skin also ages due to chronological aging and external environmental factors, including environmental pollution.
“All those insults to the skin lead to free radicals which cause inflammation and break down the collagen,” Lu said. “That’s one of the reasons older skin looks very different from younger skin.”
When the scientists created the synthetic melanin engineered nanoparticles, they modified the melanin structure to have higher free radical scavenging capacity.
“The synthetic melanin is capable of scavenging more radicals per gram compared to human melanin,” said co-corresponding author Nathan Gianneschi, the Jacob and Rosaline Cohn Professor of Chemistry, Materials Science & Engineering, Biomedical Engineering and Pharmacology at Northwestern. “It’s like super melanin. It’s biocompatible, degradable,nontoxic and clear when rubbed onto the skin. In our studies, it acts as an efficient sponge, removing damaging factors and protecting the skin.”
Once applied to the skin, the melanin sits on the surface and is not absorbed into the layers below.
“The synthetic melanin stabilises and sets the skin on a healing pathway, which we see in both the top layers and throughout the body,” Gianneschi said.
The scientists, who have been studying melanin for nearly 10 years, first tested their synthetic melanin as a sunscreen.
“It protected the skin and skin cells from damage,” Gianneschi said. “Next, we wondered if the synthetic melanin, which functions primarily to soak up radicals, could be applied topically after a skin injury and have a healing effect on the skin? It turns out to work exactly that way.”
Lu envisions the synthetic melanin cream being used as a sunscreen booster for added protection and as an enhancer in moisturiser to promote skin repair.
“You could put it on before you go out in the sun and after you have been in the sun,” Lu said. “In both cases, we showed reduction in skin damage and inflammation. You are protecting the skin and repairing it simultaneously. It’s continuous repair.”
The cream could also potentially be used for blisters and open sores, Lu said.
Gianneschi and Lu discovered that the synthetic melanin cream, by soaking up the free radicals after an injury, quieted the immune system. The stratum corneum, the outer layer of mature skin cells, communicates with the epidermis below. It is the surface layer, receiving signals from the body and from the outside world. By calming the destructive inflammation at that surface, the body can begin healing instead of becoming even more inflamed.
“The epidermis and the upper layers are in communication with the entire body,” Lu said. “This means that stabilising those upper layers can lead to a process of active healing.”
The scientists used a chemical to create a blistering reaction to a human skin tissue sample in a dish. The blistering appeared as a separation of the upper layers of the skin from each other.
“It was very inflamed, like a poison ivy reaction,” Lu said.
They waited a few hours, then applied their topical melanin cream to the injured skin. Within the first few days, the cream facilitated an immune response by initially helping the skin’s own radical scavenging enzymes to recover, then by halting the production of inflammatory proteins. This initiated a cascade of responses in which they observed greatly increased rates of healing. This included the preservation of healthy skin layers underneath. In samples that did not have the melanin cream treatment, the blistering persisted.
“The treatment has the effect of setting the skin on a cycle of healing and repair, orchestrated by the immune system,” Lu said.
Melanin could protect from toxins including nerve gas
Gianneschi and Lu are studying melanin as part of US government-funded research, which has included looking at melanin as a dye for clothing that would also act as an absorbent for toxins in the environment, particularly nerve gas. They showed they could dye a military uniform black with the melanin, and that it would absorb the nerve gas.
Melanin also absorbs heavy metals and toxins. “Although it can act this way naturally, we have engineered it to optimise absorption of these toxic molecules with our synthetic version,” Gianneschi said.
The scientists are pursuing clinical translation and trials testing for efficacy of the synthetic melanin cream. In an initial step, the scientists recently completed a trial showing that the synthetic melanins are non-irritating to human skin.
Given their observation that melanin protects biologic tissue from high energy radiation, they surmise that this could be an effective treatment for skin burns from radiation exposure.
The promising work may well provide treatment options for cancer patients in the future, undergoing radiation therapy.
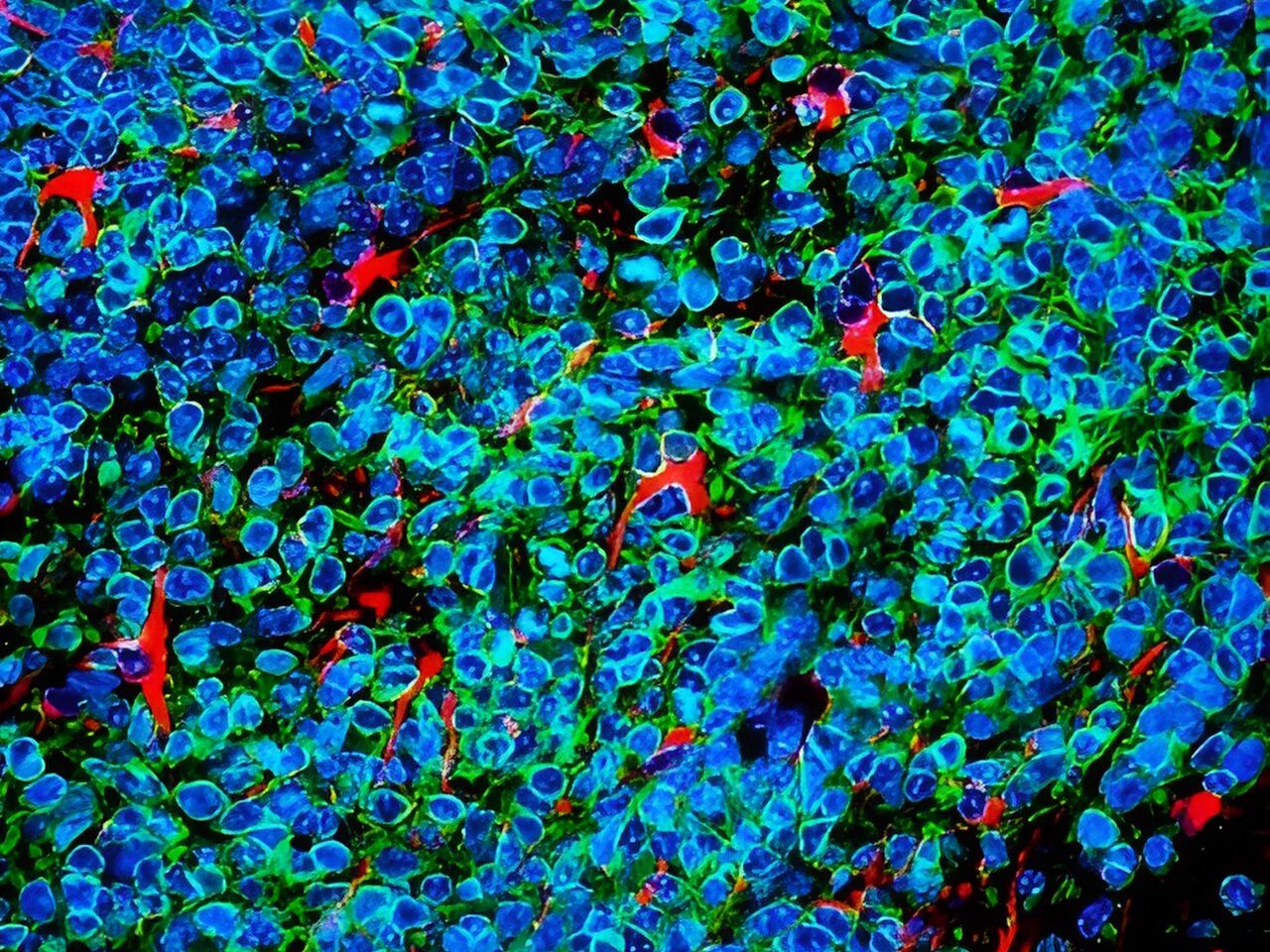
Small cell lung cancer cells (green and blue) that metastasised to the brain in a laboratory mouse recruit brain cells called astrocytes (red) for their protection. Credit: Fangfei Qu
Lung cancer cells that metastasise to the brain survive by convincing brain cells called astrocytes that they are baby neurons in need of protection, according to a study by researchers at Stanford Medicinepublished in Nature Cell Biology.
The cancer cells carry out their subterfuge by secreting a chemical signal prevalent in the developing human brain, the researchers found. This signal draws astrocytes to the tumour, encouraging them to secrete other factors that promote the cancer cells’ survival. Blocking that signal may be one way to slow or stop the growth of brain metastases of small cell lung cancer, which account for about 10% to 15% of all lung cancers, the researchers believe.
In the adult brain, astrocytes play a critical role in maintaining nerve function and connectivity. They are also important during brain development, when they facilitate connections between developing neurons.
The researchers studied laboratory mice, human tissue samples and human mini-brains, or organoids, grown in a lab dish to dissect the unique relationship between the cancer cells and their ‘big sister’ astrocytes, which hover nearby and shower them with protective factors.
“Small cell lung cancers are known for their ability to metastasise to the brain and thrive in an environment that is not normally conducive to tumour growth,” said professor of paediatrics and of genetics Julien Sage, PhD. “Our study suggests that these cancer cells reprogram the brain microenvironment by recruiting astrocytes for their protection.”
Professor Sage is the senior author of the study, while postdoctoral scholar Fangfei Qu, PhD, is the lead author.
Invasion of the brain
Small cell lung cancer excels at metastasising to the brain – about 15% to 20% of people already have clusters of cancer cells in their brains when their lung tumours are first diagnosed. As the cancer progresses, about 40% to 50% of patients will develop brain metastases. The problem is so prevalent, and the clinical outcome so dire, that clinicians recommend cranial radiation even before brain metastases have been found.
How and why small cell lung cancer has such an affinity for the brain has been something of a mystery. Brain metastases are rarely biopsied or removed because doing so has not been shown to affect a patient’s survival, and brain surgery is so invasive. Using laboratory mice is also of little help since small cell lung cancers in those animals rarely develop metastases in the brain, perhaps due to subtle biological differences between species.
Small cell lung cancers have another distinguishing feature – they are neuroendocrine cancers, meaning they arise from cells with similarities to both neurons and hormone-producing cells. Neuroendocrine cells link the nervous system with the endocrine system throughout the body, including in the lung.
Sage and his colleagues wondered whether neuronal-associated proteins on the surface of small cell lung cancer cells give them a leg up when the cells first begin to infiltrate the brain.
“We know the brain is full of neurons,” Sage said. “Maybe that’s why these cancer cells with some neuronal traits are happy in the brain and are accepted into that environment.”
Qu and Sage developed a way to inject mouse small cell lung cancer cells grown in the laboratory into the brains of mice to spark the development of brain tumours. They saw that astrocytes, a subtype of glial cell, flocked to the infant tumours and began to churn out proteins critical during brain development, including factors that stimulate nerve growth.
A plethora of astrocytes
A similar call happens in human brains, they noted: Brain tissue samples from people who had died of metastatic small cell lung cancer, shared by professor of pathology and paper co-author Christina Kong, MD, had many more protective astrocytes in the interior of the tumours than did metastases of melanoma, breast cancer and another type of lung cancer called adenocarcinoma.
Qu worked with assistant professor of paediatrics and co-author Anca Pasca, MD, to fuse aggregates of small cell lung cancer, lung adenocarcinoma or breast cancer cells with what are called cortical organoids – in vitro-grown clumps of brain cells including neurons and astrocytes that begin to mimic the organisation and connectivity of a human cortex. Within 10 days, many more protective astrocytes had infiltrated the small cell lung cancer pseudo-tumours than the adenocarcinoma or breast cancer.
“This showed us that the astrocytes actively move toward the small cell lung cancer cells, rather than simply being engulfed by the growing tumour,” Sage said. “What’s more exciting, though, is that these organoids, or mini-brains, realistically model the developing human brain. So, we’re no longer relying on a mouse model. It’s a perfect system to study brain metastases.”
Further research showed that the small cell lung cancer cells summon protective astrocytes by secreting a protein called Reelin that mediates the migration of neuronal and glial cells during brain development. Triggering Reelin expression in mouse breast cancer cells injected into the brain significantly increased the number of astrocytes in the resulting tumours in the mice, and the tumours were larger than in control animals injected with cells with low Reelin expression.
The apparent reliance of the cancer cells on chemical signals and responses specific to the developing brain may give clues for the development of future therapies, Sage believes.
“Some of these signals may not be as relevant or as highly expressed in the adult brain,” Sage said. “As a result, perhaps they could still be targeted to slow or prevent brain metastases without harming a normal brain. This might be an important window of opportunity for therapy.”
Newly announced results of a pivotal phase 3 trial have demonstrated the effectiveness of a new one-dose treatment for gonorrhoea. The medicine, called zoliflodacin, is the first new drug developed to treat gonorrhoea in over 30 years. More than half of the 930 patients included in the trial were from South Africa, including women, adolescents, and people living with HIV.
Zoliflodacin, which was shown to be non-inferior to (as good as) the currently used treatment in treating uncomplicated gonorrhoea, provides an important new tool to combat rising rates of drug resistant gonorrhoea. It was found to be generally well tolerated and there were no serious adverse events or deaths recorded in the trial. So far, only top line results have been shared in a media release and the findings have not yet been published in a medical journal. (You can see some technical details of the study design on ClinicalTrials.gov)
The World Health Organization raised the alarm about increasing rates of drug resistant gonorrhoea in 2017, noting the emergence of cases of untreatable gonorrhoea resistant to all available antibiotics. According to the United States Centers for Disease Control and Prevention “medication to treat gonorrhoea has been around for decades, but the bacteria has grown resistant to nearly every drug ever used to treat it”. They say: “only one class of antibiotics known as cephalosporins remains to treat the infection”.
As a drug from a new class of antibiotics, zoliflodacin, offers a new potential treatment for patients whose gonorrhoea was previously untreatable, as well as a new tool for safeguarding the ongoing effectiveness of currently available antibiotics.
How zoliflodacin may change gonorrhoea treatment
Professor Sinead Delany-Moretlwe, Director of Research for Wits RHI and the National Principal Investigator for the trial in South Africa, told Spotlight that while zoliflodacin may be used to treat drug resistant gonorrhoea, it also provides an attractive new treatment option for first-line treatment of gonorrhoea in some countries (in other words, gonorrhoea that is not resistant to other treatments).
Zoliflodacin, which is taken as a single oral dose, is simpler to administer than the current standard of care, which involves a combination of injectable ceftriaxone and oral azithromycin. Removing the need for an injection could simplify the administration of gonorrhoea treatment and improve its uptake.
Using zoliflodacin as first-line gonorrhoea treatment can also help safeguard the ongoing effectiveness of cephalosporins (including ceftriaxone), according to Delany-Moretlwe, which she adds are needed not just for treatment of gonorrhoea, but also other infections.
According to Delany-Moretlwe, because zoliflodacin is the first of a new class of antibiotics with novel mechanisms of action and without existing cross resistance, the hope is that widespread use of zoliflodacin as first-line gonorrhoea treatment will slow the emergence of resistance compared with the medicines currently being used.
The Global Antibiotic Research and Development Partnership (GARDP), a non-profit that sponsored the trial, points out that: “Antimicrobial resistance [AMR] has been around for millions of years, long before the first man-made antibiotics. So, drug-resistant bacteria are inevitable and will eventually affect all antibiotics”. They state: “to beat AMR we need a steady supply of new antibiotics to be developed that are effective against drug-resistant bacteria, particularly for priority pathogens that have the greatest public health impact.”
Gonorrhoea in South Africa
South Africa has incredibly high rates of gonorrhoea, with an estimated 2 million new cases annually. While data on rates of drug resistance in the country is limited, the data that is available indicates that ceftriaxone resistance in the country is low, but azithromycin resistance is concerningly high in some parts of the country.
As there is no routine screening for gonorrhoea in South Africa, linkage to treatment remains a challenge. Currently, diagnosis is largely done through symptomatic reporting by patients. But this approach misses many cases as some patients do not self-report symptoms and some cases of gonorrhoea are asymptomatic.
In 2022, the Southern African HIV Clinicians Society released new guidelines for the management of sexually transmitted infections which called for provider-initiated symptomatic screening and provider-initiated diagnostic screening in high-risk populations.
The country’s new National Strategic Plan on HIV, TB and STIs has set a target to increase the number of pregnant women tested for gonorrhoea from 10% in 2023 to 80% by 2028 and has committed to implementing diagnostic testing in other priority populations, including adolescent girls and young women.
How will new gonorrhoea treatments be commercialised?
Zoliflodacin was developed by GARDP in collaboration with the company Innoviva Specialty Therapeutics. According to GARDP, it holds the rights to register and commercialise zoliflodacin in more than three-quarters of the world’s countries, including all low-income countries, most middle-income countries, and several high-income countries. While, Entasis Therapeutics Limited, an affiliate of Innoviva Specialty Therapeutics, “retains the commercial rights for zoliflodacin in the major markets in North America, Europe, Asia-Pacific, and Latin America”.
South Africa is one of the countries in which GARDP holds the rights to register and commercialise zoliflodacin. It is anticipated that this will be done through selection and licensing of companies to manufacture and supply zoliflodacin in South Africa and other countries where GARDP holds commercialisation rights.
GARDP recently launched a request for proposals from partners that are interested in commercialising zoliflodacin. GARDP has also signed a memorandum of understanding with two generic producers to explore opportunities to commercialise the medicine in low-and-middle-income countries.
While the price that will be offered by commercial partners for the product remains to be seen, it is anticipated that products will be made available at affordable prices in line with GARDP’s goal to ensure that “all GARDP products are available, affordable, and appropriately used across populations that need them”.
“This is the first study to address a World Health Organization priority pathogen that has been sponsored and led by a non-profit organization,” says GARDP.
“This demonstrates that GARDP’s model can play a crucial role in helping to fix the public health failure at the heart of the global AMR crisis,” says Professor Glenda Gray, GARDP board member and President of the South African Medical Research Council.
SA involvement
According to GARDP, South Africa had the highest number of participants in the global trial, across six sites in four provinces: Wits RHI in Hillbrow, Johannesburg; the Desmond Tutu HIV Foundation in Masiphumelele, Cape Town; Setshaba Research Centre in Soshanguve, Gauteng; the SAMRC’s clinical research sites in Botha’s Hill and Tongaat in KwaZulu-Natal; and Ndlovu Research Centre in Groblersdal, Limpopo.
“We have also been able to leverage our HIV experience to build capacity for trials of novel STI technologies, a previously neglected area. Undertaking this vital work on a new treatment for gonorrhoea has also given us the opportunity to focus sharply on the local situation in South Africa,” says Delany-Moretlwe.
Atherosclerosis, caused by arterial wall plaque build-up, is a leading cause of death globally, particularly in the developed countries. Although the mortality rates for this condition fell dramatically during the 20th century, the incidence is now ever increasing. Unfortunately, despite the widespread impact of atherosclerosis – and efforts to curb it – data on the global and national trends of the disease is quite limited.
In a recent effort to address this knowledge gap, a research team from China led by Professor Rongchong Huang decided to conduct a detailed statistical analysis on the impact of atherosclerosis at the global and national levels by using GBD data. The study was published in the Chinese Medical Journal.
“It is unknown how global changes in pertinent controllable variables in recent years have affected the burden of atherosclerosis,” remarks Prof Huang.
The researchers analysed publicly available data from the Global Burden of Disease Study 2019 related to the three main clinical presentations of atherosclerosis, ischaemic heart disease (IHD), ischaemic stroke (IS), and peripheral arterial disease (PAD). The data collected, which spanned the period from 1990 to 2019, included participants of all ages with similar epidemiologic characteristics and in relative proximity, from 21 countries.
Overall, the study had four main goals. The first was to determine the global trends in terms of prevalence, mortality, and disability of the three conditions. The second goal was to identify the years that had the biggest shift in the trends of these indicators. Finally, the third and fourth goals were to analyze global trends based on age, gender, and socioeconomic factors and report global and national patterns, respectively.
According to the results, there was an overall increasing trend in the global incidence of the three clinical manifestations of atherosclerosis from 1990 to 2019. Notably, the main drivers for this rising incidence were adults aged 20–54. The researchers found this very concerning, given that atherosclerosis with such an early onset is usually caused by preventable factors, such as lack of exercise, dietary habits, and environmental pollution. However, the mortality rates and disability-adjusted life years for IHD and IS declined during this period across all age groups. This could indicate greater awareness regarding these conditions and their early symptoms, as well as advancements in clinical management.
Nonetheless, the global rise in the incidence of atherosclerosis over the past three decades is a serious problem that warrants special attention towards its root causes. In this regard, Prof Huang explains: “This rise can be attributed to a variety of factors. Firstly, global aging trends have led to a higher prevalence of the disease, given that age is a significant risk factor for atherosclerosis. Secondly, modern lifestyle habits, including high-fat diets, lack of exercise, smoking, and excessive alcohol consumption, have increased atherosclerosis risk. Lastly, there has been a rise in chronic diseases such as diabetes and hypertension, which are significant risk factors for atherosclerosis.”
The researchers also pointed out that the burden posed by atherosclerosis is increasing significantly in low- or middle-income countries, summarising key social and economic development indicators. China, which has the world’s greatest number of deaths due to cardiovascular diseases, is a prime example of this issue.
Taken together, the study paints a grim picture of global cardiovascular health, which is very concerning. “Overall, the burden of atherosclerosis-related disease is still not significantly decreasing and is even trending upward, especially in low- and middle-income countries and in younger populations,” says Prof Huang, “There is an urgent need for more targeted treatment and management in younger populations and in low-middle and middle-income countries.”
Hopefully, the results of these analyses will prompt decision makers, scientists, and medical professionals alike to increase their efforts towards fighting against atherosclerosis and its devastating consequences.