Gut Microbiome. Credit Darryl Leja National Human Genome Research Institute National Institutes Of Health
A study conducted by researcher Juan Du’s research group at the Karolinska Institutet sheds light on the capabilities of our gut microbes and their metabolites. The findings reveal potent inhibitory effects on the growth of antibiotic-resistant bacteria and suggest interactions and signaling between gut microbes and pathogens.
The study,published in the journal Gut Microbes, focuses on identifying key microbes within the gut microbiome that inhibit the growth of pathogens, particularly antibiotic-resistant strains.
Strains from Clostridium perfringens, Clostridium butyricum, and Enterobacter maltosivorans and their metabolites were found to directly inhibit the growth of pathogens, including multi-drug-resistant ones. The study also reveals novel dipeptide features, suggesting interactions and signaling between gut microbes and pathogens.
“Multidrug-resistant microorganisms pose a global threat, and understanding the role of gut microbiota is crucial. Metabolites derived from these microbial communities play a significant role in regulating biochemical processes in the human body. Despite this, only a limited number of gut microbes and their bioactive metabolites have been explored so far”, explains author Juan Du. She continues:
“We plan to expand our screening to include a broader collection of commensal bacteria from various body sites. We’ll conduct mechanism studies to understand how these compounds function on pathogens, especially antibiotic-resistant strains”, says Juan Du.
Dr Kenneth Jacobs entered Parliament as an ANC MP in 2019, and two years later was elected chairperson of the Portfolio Committee on Health. (Photo: Parliament)
By Biénne Huisman
The chairperson of the National Assembly’s Portfolio Committee on Health Dr Kenneth Jacobs played a pivotal role in deliberations on the National Health Insurance Bill. Spotlight’s Biénne Huisman asked Jacobs about some criticisms of NHI and about his plans for life after Parliament.
Back in Cape Town, Jacobs tells Spotlight the NHI signing was the culmination of his own work dating back fifteen years. He says he started working on public health projects relating to universal health coverage and the NHI in 2009, as a consultant to the National Department of Health.
For him, at the heart of the bill lies fairness.
“We should be able to provide all of the people of South Africa the opportunity to access quality healthcare,” he says.
Jacobs entered Parliament as an ANC MP in 2019, and two years later was elected chairperson of the Portfolio Committee on Health after his predecessor, Dr Sibongiseni Dhlomo, became the Deputy Minister of Health. Committee chairpersons are elected by and from among the members of each committee, meaning the majority party in Parliament has the most influence in selecting chairpersons.
As chairperson, a large part of Jacobs’ job was to hold the country’s executive and the National Department of Health to account on behalf of South Africa’s citizens.
Amongst other tasks, he played a pivotal role in overseeing public deliberations around the NHI Bill, which included 338 891 written submission and presentations by 133 organisations. These included political parties, trade unions, medical aid schemes, health technology organisations, the South African Medical Association, and university departments.
“It is never in the history that the committee had such an engagement by the public,” says Jacobs. “So I’ve been very blessed and fortunate to go to Parliament in the final process of the NHI Bill.”
‘Disheartening’ criticism
Both before and after its signing into law, NHI has been deeply divisive, with several political parties and other role players threatening litigation. One line of criticism is that, while many people and organisations made submissions to the committee chaired by Jacobs, the final bill did not changed substantially from what it was prior to the public hearings.
Interviewed on the topic, Business Leadership South Africa CEO Busi Mavuso, said government rushed populist policy through Parliament – an electioneering ploy – as the significant public input into the Bill and its socioeconomic ramifications had not been considered.
Jacobs voices his frustration at such criticism of the NHI public participation process, saying it is “disheartening”, adding that criticism are doled out by South Africans who are “in better financial positions”.
He explains the process of collating so much information: “Well, firstly it’s driven by the chairperson [him]… We appointed a team through Parliamentary processes, who looked at the submissions, and interpreted the submissions using computerised systems. It’s thematic – what are the themes, really? These are developed into reports; the reports on all the public hearings, those reports are all available.”
He adds: “So people who want to write and say all these negative things, they really should go and access these documents and see what the submissions were.”
‘It’s attractive to make people insecure’
Another aspect of NHI over which many have expressed concern is the potential for corruption, particularly in light of massive healthcare corruption during the height of the COVID-19 pandemic and more recent alleged corruption at Tembisa Hospital in Gauteng. Here criticism ranges from a simple distrust in government to run such funds, to more nuanced criticisms of aspects of the bill that critics say increases the risk of corruption – such as the Minister of Health’s expansive powers and accountability to cabinet rather than to Parliament.
In an interview following the signing of the bill, DA Chief Whip who was also a health portfolio committee member, Siviwe Gwarube, said: “The NHI will not address the underlying issues in our healthcare system; it is financially unfeasible, an election gimmick, and will burden South Africans with increased taxes.” She added: “The potential for corruption is staggering, and the flawed parliamentary process further erodes public trust…”
When asked about fears that money might disappear from centralised NHI coffers – to be governed by a board appointed by the minister of health – and accountability to prevent such, Jacobs says: “I think that people are putting the cart before the horse. You must remember this will be an entity [with tender procedures], and then who is supposed to appoint them [board members] in any case? Somebody has to have the responsibility. Why can that not be the minister, for example. But remember that it will be a transparent process, the same as the appointment, I think, as what we do with the appointment of judges.”
The NHI fund will be a schedule 3A entity, similar to, among others, the Road Accident Fund, the National Lotteries Commission, the National Laboratory Service, the Office of Health Standards Compliance, the Competition Commission, and the Council for Medical Schemes.
Jacobs says checks will be provided by the country’s forensic investigation agency, the Special Investigating Unit (SIU). “And there are many ways to put checks and balances into place,” he says, “we talk [in the bill] about the interventions which can be made, or the investigations which can be made by the SIU and other law enforcement agencies”.
Shortly after taking over as health committee chairperson, Jacobs told Spotlight that rooting out corruption in the health sector was a priority. At the time, he stressed the importance of safety nets for whistle-blowers, and of establishing systems to enforce accountability. Around the time of his appointment in 2021, whistle-blower Babita Deokaran was murdered for exposing R1 billion worth of allegedly irregular tenders issued at the Tembisa Hospital in Gauteng.
Asked about these particular earlier priorities, Jacobs responds: “I have no answer on that, I don’t think I want to talk about corruption now…” Upon reflection, he adds: “Of course corruption is important. Losses to the fiscal is important; people doing wrong is important. People need to be brought to book, be held accountable for doing wrong…”
Later on in the interview, when the issue of corruption comes up again, he says that corruption has decreased in South Africa: “I think we’ve advanced quite a bit from the time when corruption was more rife. I think nowadays you hardly hear about these things and it’s because unprecedented intensive programmes were put in place to address these issues of corruption and fraud. I really think what they [critics] are doing is fear-mongering, telling people that you need to be frightened, and I’m going to say again, those who are telling others to feel frightened, are in a better financial position. So it’s attractive to make people insecure.”
Money for NHI?
Another common argument against implementing NHI is that it is not affordable. Government’s spending on health has declined in real terms for much of the last decade and the South African economy is struggling by most measures.
Asked about crippling budget cuts in the health sector as it stands, and questions around the NHI’s affordability, Jacobs says South Africa has insufficient central funds because of unemployment, and that South Africa needs more jobs and more workers to increase its tax-base.
“My personal view is that we need to understand why there’s a budget problem,” he says. “So where is government supposed to get money? Who are supposed to contribute? Those who are employed. And look at our employment rate – is it government’s responsibility? No, the emphasis is wrong. It is businesses’ responsibility.
“When people have employment they can contribute to the coffer… and I’m going to keep on saying, the narrative is in the wrong place. We need to say to South Africans: ‘don’t all of us have a responsibility?’ Those who have the economy in their hands and those who don’t have the economy in their hands, all of the responsibility to drive our country forward.”
How to drive South African healthcare forward, remains contested. Several organisations representing healthcare workers, such as the South African Medical Association, do not support the NHI Act in its current form. Others, including the South African Medical Association Trade Union, welcome it.
Meanwhile, Jacobs expresses empathy for his clinician colleagues: “As a medical doctor, I have absolute respect for all of my colleagues. I would like you to write it; I understand the conditions under which our medical and or health personnel have to function. And I don’t think that National Health Insurance be a negative thing for healthcare professionals.”
‘Why should there be people who profit from the ill health of other people?’
Another concern in some quarters is that NHI will over time squeeze out medical aid schemes and leave people with no alternative to health services provided through NHI. This because, according to Section 33 of the NHI Act, medical schemes will not be allowed to cover services that are already covered by the NHI fund.
Asked about the future of medical aid schemes in South Africa, Jacobs says: “What is the medical aid system? It’s a profit driven system by people who are in business. Is it correct that there are people who make profit off the lives of people, and the health of people? I don’t think that is correct.” (Note: Medical schemes are non-profit entities while medical scheme administrators are for-profit.)
He adds: “What is wrong with having one single system, in which everybody has access to the same healthcare? Why do we need to keep exclusionary rights for some people, based on them having a better income than others? I think that’s the bottom-line on the answer of the medical aid. Whether medical aid will stop functioning or not. I think that’s not the question to ask. The question is why should there be people who profit from the ill health of other people?”
‘From policy to practice’
Going forward, given that he won’t be returning to Parliament, Jacobs hopes to resume doing public health consulting work for the National Department of Health.
“I have a project which is very dear to me,” he says. “I want to start an institute for health governance, and it’s called, ‘from policy to practice’. It’s on health governance, universal health coverage… and will be instrumental in influencing dialogue. So, I can’t wait to stay active in the health sector, but not being restricted in that I’m no longer a member of Parliament, not feeling that there’s some sort of conflict.”
Jacobs will now move from the Acacia Park Parliamentary Village on Cape Town’s northern fringes back to his family home in Wellington.
Jacobs says that they will soon have seven public health doctors in his family – that is, when his son completes medical school at Stellenbosch University. His daughter recently finished medical school and is contracted as a doctor at a clinic in Khayelitsha.
Originally from Gqeberha, Jacobs holds a Bachelor of Medicine and Bachelor of Surgery degree from Stellenbosch University where he also obtained a Master of Medicine degree in family medicine. He went on to get a Master of Science degree in sports medicine from the University of Pretoria. In earlier years, he served as a physician to the Stormers and Springbok rugby teams.
In the previous interview with Spotlight, Jacobs relayed how his formative years were tough. His family were forcibly evicted from sea-facing South End, in what was then Port Elizabeth, and moved to Gelvandale, in the city’s northern suburbs. His father worked in a shoe factory, but lost his job when Jacobs was in grade 10.
“South End was like Port Elizabeth’s District Six,” said Jacobs, in the earlier interview. “So yes, honestly, that was something that had a huge impact on me. I decided then that I would not allow somebody to suppress or oppress me and I think it is probably why I just kept on studying and improving.”
At 65 years old, Jacobs exudes ambition and enthusiasm. Wrapping up, he quotes an Afrikaans aphorism: “Die mens wik maar God beskik” (Humanity proposes, God disposes).
Lung cancer metastasis. Credit: National Cancer Institute
A new study led by investigators from Mass General Cancer Center, a founding member of the Mass General Brigham healthcare system, reveals that statins may block a particular pathway involved in the development of cancer that results from chronic inflammation. The findings are published in Nature Communications.
“Chronic inflammation is a major cause of cancer worldwide,” said senior author Shawn Demehri, MD, PhD. “We investigated the mechanism by which environmental toxins drive the initiation of cancer-prone chronic inflammation in the skin and pancreas. Furthermore, we examined safe and effective therapies to block this pathway in order to suppress chronic inflammation and its cancer aftermath.”
Demehri and his colleagues’ study relied on cell lines, animal models, human tissue samples and epidemiological data. The group’s cell-based experiments demonstrated that environmental toxins (such as exposure to allergens and chemical irritants) activate two connected signaling pathways called the TLR3/4 and TBK1-IRF3 pathways. This activation leads to the production of the interleukin-33 (IL-33) protein, which stimulates inflammation in the skin and pancreas that can contribute to the development of cancer.
When they screened a library of U.S. Food and Drug Administration–approved drugs, the researchers found that a statin, pitavastatin, effectively suppresses IL-33 expression by blocking the activation of the TBK1-IRF3 signalling pathway. In mice, pitavastatin suppressed environmentally-induced inflammation in the skin and the pancreas and prevented the development of inflammation-related pancreatic cancers.
In human pancreas tissue samples, IL-33 was over-expressed in samples from patients with chronic pancreatitis and pancreatic cancer compared with normal pancreatic tissue. Also, in analyses of electronic health records data on more than 200 million people across North America and Europe, use of pitavastatin was linked to a significantly reduced risk of chronic pancreatitis and pancreatic cancer.
The findings demonstrate that blocking IL-33 production with pitavastatin may be a safe and effective preventive strategy to suppress chronic inflammation and the subsequent development of certain cancers.
“Next, we aim to further examine the impact of statins in preventing cancer development in chronic inflammation in liver and gastrointestinal tract and to identify other novel, therapeutic approaches to suppress cancer-prone chronic inflammation” said Demehri.
Sanitech, a leader in integrated hygiene and sanitation solutions, recently celebrated its 50th anniversary. Reflecting on the company’s journey from a small plumbing business to a comprehensive sanitation provider, Sanitech’s Managing Director, Robert Erasmus, shares insights into the company’s history, recent initiatives, and future aspirations.
The Sanitech name was registered in 1974 by Grant Murray in KwaZulu-Natal. Initially, it was a small plumbing business, but Murray quickly identified a market for portable sanitation services. Over the years, Sanitech expanded, albeit on a limited scale, by partnering with various agents. The significant transformation began in the 1990s and early 2000s when private equity ownership enabled national growth. In 2007, the business continued to expand following the acquisition of Sanitech, which marked the beginning of global support for WACO International.
Erasmus joined Sanitech in 2008, marking a pivotal moment. “My role was to transform Sanitech into a corporate entity aligned with WACO International’s standards in health, safety, policies, and procedures,” Erasmus explains. Under his leadership, Sanitech expanded from eight locations to 24 and diversified its services beyond portable toilets to include integrated hygiene services, water and waste treatment, and pest control. Today, Sanitech employs over 3,000 people, a substantial increase from 350 in 2008.
Instead of a traditional celebration event for its 50th anniversary, Sanitech chose to invest in Corporate Social Investment (CSI) projects. Sanitech sponsored 50 Khusela sanitation units across various regions in South Africa. These units were installed in disadvantaged schools in areas such as Witbank, Johannesburg, Durban, Port Elizabeth, and Cape Town, providing proper sanitation facilities and meals for the day. “It was a school-focused initiative, ensuring that learners have access to clean and safe sanitation, which is crucial for their health and education.”
Looking ahead, Erasmus envisions Sanitech continuing its trajectory of growth and innovation. “We aim to expand our product and service offerings in the hygiene and sanitation sector, especially as we face new challenges like the potential water crisis. Sub-Saharan Africa presents significant opportunities, and we’ve already established a presence in Mozambique,” he notes. Sanitech plans to enhance its contributions to clients’ Environmental, Social, and Governance (ESG) requirements by expanding its hygiene, cleaning, and pest control services.
Reflecting on the impact of their CSI projects, Erasmus shares a poignant experience: “Visiting the school in Palm Ridge where we installed new sanitation units was eye-opening. The conditions these young learners face are challenging, yet their discipline and resilience are incredible. It was a humbling reminder of the importance of our work.”
Since 2007, Vodacom Foundation has proudly partnered with the Smile Foundation to support Smile Week, an initiative that provides life-changing reconstructive surgery to children with treatable facial anomalies. Smile Week not only addresses the physical challenges faced by these young people but also alleviates the emotional distress associated with feeling different, enabling them to embrace their lives to the fullest.
“As we mark Vodacom’s 30th anniversary this year, it’s a good time to reflect on the dramatic change in the countries in which we operate, in terms of bringing connectivity to people. What we are also particularly proud of is how we have brought purpose to society and how we have made a meaningful difference in people’s lives,” says Shameel Joosub, Vodacom Group CEO.
Orofacial cleft lip/palate (CLP) remains in the top five of South Africa’s most common congenital disorders. Smile Week sees surgeons, their surgical teams, and other medical professionals around the country dedicate their time and expertise to perform reconstructive surgery on children whose families would not otherwise have been able to afford it.
“Families invariably find their way to state hospital facilities, where there are very capable and competent surgeons and medical professionals, but budget constraints have often meant elective surgery has to wait before more critical cases are addressed,” says Marc Lubner, founder and executive chairman of the Smile Foundation.
To date, the partnership between Vodacom and the Smile Foundation has benefited 600 children, with the shared goal of enhancing their overall quality of life and well-being.
“I want to thank all the medical professionals for being partners with us since 2007, and for giving their time and commitment to make this a reality. Vodacom’s support of Smile Week reaffirms our commitment as a company to use our capabilities collaboratively for a brighter, more inclusive future,” says Joosub.
In this video, parents and Smile Week recipients share their experiences and the importance of this initiative in transforming lives.
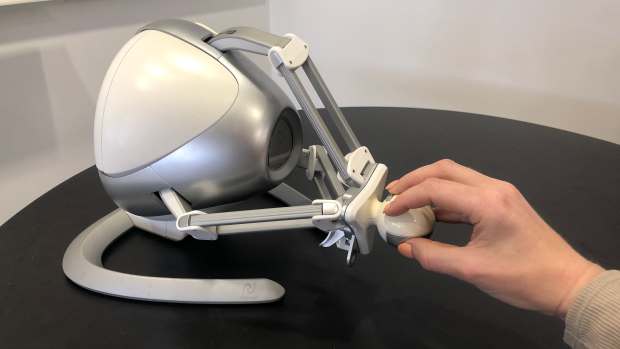
The Novint Falcon, a desktop robot typically used for video games, can guide users through specific arm motions and track the trajectory of its controller.
For recovering stroke survivors, getting intensive, frequent rehabilitation therapy to help restore fine motor skills can be challenging and expensive.
Now, researchers at NYU Tandon School of Engineering are developing a new technology that could allow stroke patients to undergo rehabilitation exercises at home by tracking their wrist movements through a simple setup: a smartphone strapped to the forearm and a low-cost gaming controller called the Novint Falcon.
The Novint Falcon, a desktop robot typically used for video games, can guide users through specific arm motions and track the trajectory of its controller. But it cannot directly measure the angle of the user’s wrist, which is essential data for therapists providing remote rehabilitation.
“Patients would strap their phone to their forearm and manipulate this robot,” said Maurizio Porfiri, NYU Tandon Institute Professor and director of its Center for Urban Science + Progress (CUSP), who is the paper’s senior author. “Data from the phone’s inertial sensors can then be combined with the robot’s measurements through machine learning to infer the patient’s wrist angle.”
The researchers collected data from a healthy subject performing tasks with the Falcon while wearing motion sensors on the forearm and hand to capture the true wrist angle. They then trained an algorithm to predict the wrist angles based on the sensor data and Falcon controller movements.
The resulting algorithm could predict wrist angles with over 90% accuracy, a promising initial step toward enabling remote therapy with real-time feedback in the absence of an in-person therapist.
“This technology could allow patients to undergo rehabilitation exercises at home while providing detailed data to therapists remotely assessing their progress,” Roni Barak Ventura, the paper’s lead author who was an NYU Tandon postdoctoral fellow at the time of the study. “It’s a low-cost, user-friendly approach to increasing access to crucial post-stroke care.”
The researchers plan to further refine the algorithm using data from more subjects. Ultimately, they hope the system could help stroke survivors stick to intensive rehab regimens from the comfort of their homes.
This study adds to NYU Tandon’s body of work that aims to improve stroke recovery. In 2022, Researchers from NYU Tandon began collaborating with the FDA to design a regulatory science tool based on biomarkers to objectively assess the efficacy of rehabilitation devices for post-stroke motor recovery and guide their optimal usage. A study from earlier this year unveiled advances in technology that uses implanted brain electrodes to recreate the speaking voice of someone who has lost speech ability, which can be an outcome from stroke.