A new analysis involving over 13 000 people has found changes to blood vessels in the brain that can increase the risk of stroke and dementia are common in people with a range of heart conditions, regardless of whether they have experienced a stroke.
The new research, published in Neurology®, the medical journal of the American Academy of Neurology, is the most comprehensive systematic review of ‘hidden’ brain changes in people with a range of heart conditions to date.
Lead author Dr Zien Zhou from The George Institute for Global Health said that identifying these changes could play an important role in choosing treatments for these patients.
“Although people with heart disease are two to three times more likely than the general population to have changes in their brain’s vascular system, they’re often overlooked, because these patients don’t routinely undergo brain imaging unless they have suffered a stroke,” he said.
“But it can make them more susceptible to the risk of brain bleeds from medications commonly used to treat or prevent blood clots – intracranial haemorrhage is a life-threatening complication with no proven treatment and a survival rate of less than 50 percent.”
Changes to blood vessels in the brain that can only be detected by brain imaging such as silent brain infarction (SBI) and cerebral small vessel disease (CSVD) are known to occur more commonly in older people or those who have hypertension.
While not sufficient to cause obvious neurological symptoms, they can result in subtle neurological deficits and increase the longer-term risk of stroke or dementia.
To determine the prevalence of these hidden or covert cerebrovascular changes in adults with atrial fibrillation, coronary artery disease, heart failure or cardiomyopathy, heart valve disease, and patent foramen ovale (a hole in the heart), George Institute researchers conducted a meta-analysis of 221 observational studies published between 1988 and 2022.
The findings showed that in people with heart disease:
approximately one third had any form of SBI
a quarter had lacune (small cavities where neural tissue has died after a previous blockage or leakage from small arteries)
two-thirds had white matter lesions (damage to the protective coating around nerve fibres)
a quarter had evidence of asymptomatic microbleeds in the brain tissue, and
over one half had brain atrophy (a shrinking of the brain due to loss of neurons or connections between neurons).
The prevalence of these brain changes was generally the same between those with and without a recent stroke and there were no apparent sex differences in the results.
Dr Zhou said the study also confirmed that heart disease is one of the main causes of these changes that reflect brain ‘frailty’.
“While several potential mechanisms of the association between heart disease and hidden cerebrovascular injury have been proposed, the two conditions share common risk factors such as ageing, hypertension, type 2 diabetes, hyperlipidaemia, and smoking,” said Dr Zhou.
“It’s possible that a gradual decline in cardiac output in some patients with heart disease might affect how much blood is reaching the brain tissue, contributing to vascular changes and cognitive dysfunction in these patients,” he added.
“It’s also possible that hidden brain changes and cognitive dysfunction are a consequence of tiny blood clots traveling to the brain through the arterial circulation after forming in the heart.”
Dr Zhou said that more research was needed to look at the exact causes of these brain changes and the implications for managing these patients.
“We need to know whether performing an additional MRI in those considered for anticoagulation therapy – which is required for most people with heart disease – would be cost-effective in terms of preventing unwanted side effects,” he said.
“But refining the risks of brain clots and bleeds from anticoagulants and using this information to make the best treatment choice could improve treatment safety for people with heart disease.”
The device represents a huge leap ahead guide neurosurgeonswith visualised brain activity
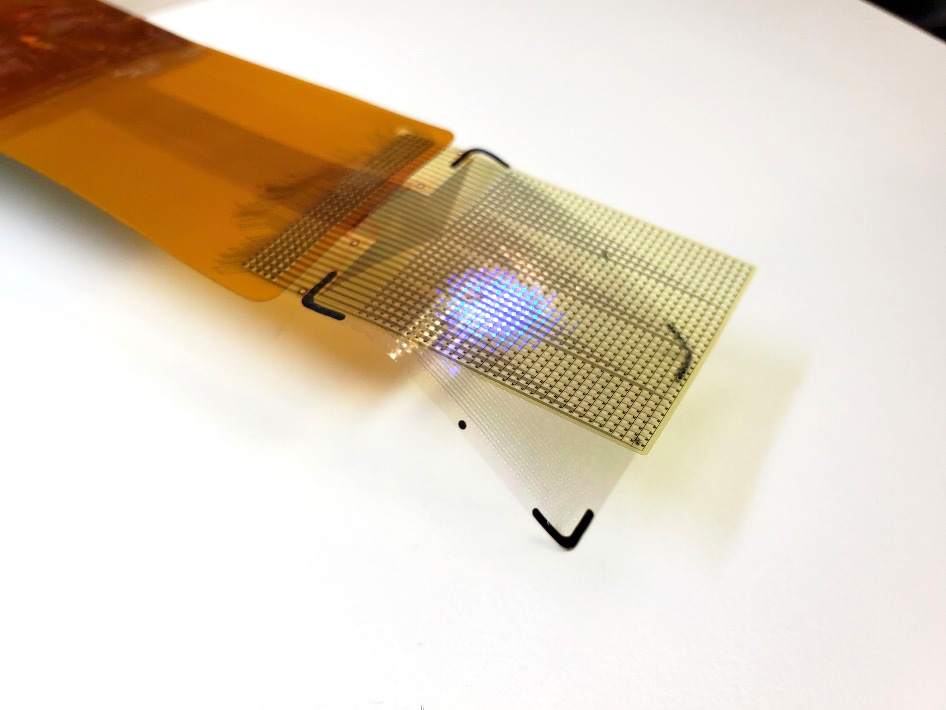
The device’s LEDs can light up in several colors. This allows surgeons to see which areas they need to operate on. It allows them to track brain states during surgery, including the onset of epileptic seizures. Credit: UCSF
A thin film that combines an electrode grid and LEDs can both track and produce a visual representation of the brain’s activity in real-time during surgery-a huge improvement over the current state of the art. The device is designed to provide neurosurgeons visual information about a patient’s brain to monitor brain states during surgical interventions to remove brain lesions including tumours and epileptic tissue.
Each LED in the device represents the activity of a few thousand neurons. In a series of proof-of-concept experiments in rodents and large non-primate mammals, researchers showed that the device can effectively track and display neural activity in the brain corresponding to different areas of the body. In this case, the LEDs developed by the team light up red in the areas that need to be removed by the surgeon. Surrounding areas that control critical functions and should be avoided show up in green.
The study also showed that the device can visualise the onset and map the propagation of an epileptic seizure on the surface of the brain. This would allow physicians to isolate the ‘nodes’ of the brain that are involved in epilepsy. It also would allow physicians to deliver necessary treatment by removing tissue or by using electrical pulses to stimulate the brain.
“Neurosurgeons could see and stop a seizure before it spreads, view what brain areas are involved in different cognitive processes, and visualise the functional extent of tumour spread. This work will provide a powerful tool for the difficult task of removing a tumour from the most sensitive brain areas,” said Daniel Cleary, one of the study’s coauthors, a neurosurgeon and assistant professor at Oregon Health and Science University.
The device was conceived and developed by a team of engineers and physicians from University of California San Diego and Massachusetts General Hospital (MGH) and was led by Shadi Dayeh, the paper’s corresponding author and a professor in the Department of Electrical and Computer Engineering at UC San Diego.
Protecting critical brain functions
During brain surgery, physicians need to map brain function to define which areas of the organ control critical functions and can’t be removed. Currently, neurosurgeons work with a team of electrophysiologists during the procedure. But that team and their monitoring equipment are located in a different part of the operating room.
Brain areas that need to be protected and those that need to be operated on are either marked by electrophysiologists on a paper that is brought to the surgeon or communicated verbally to the surgeon, who then places sterile papers on the brain surface to mark these regions.
“Both are inefficient ways of communicating critical information during a procedure, and could impact its outcomes,” said Dr Angelique Paulk of MGH, who is a co-author and co-inventor of the technology.
In addition, the electrodes currently used to monitor brain activity during surgery do not produce detailed fine grained data. So surgeons need to keep a buffer zone, known as resection margin, of 5 to 7mm around the area they are removing inside the brain.
This means that they might leave some harmful tissue in. The new device provides a level of detail that would shrink this buffer zone to less than 1mm.
“We invented the brain microdisplay to display with precision critical cortical boundaries and to guide neurosurgery in a cost-effective device that simplifies and reduces the time of brain mapping procedures,” said Shadi Dayeh, the paper’s corresponding author and a professor in the Department of Electrical and Computer Engineering at the UC San Diego Jacobs School of Engineering.
Researchers installed the LEDs on top of another innovation from the Dayeh lab, the platinum nanorod electrode grid (PtNRGrid). Using the PtNRGrids since 2019, Dayeh’s team pioneered human brain and spinal cord mapping with thousands of channels to monitor brain neural activity.
They reported early safety and effectiveness results in a series of articles in Science Translational Medicine in 2022 in tens of human subjects.
(New sensor grids record human brain signals with record breaking resolution and Microelectrode array can enable safer spinal cord surgery) — ahead of Neuralink and other companies in this space.
The PtNRGrid also includes perforations, which enable physicians to insert probes to stimulate the brain with electrical signals, both for mapping and for therapy.
How it’s made
The display uses gallium nitride-based micro-LEDs, bright enough to be seen under surgical lights. The two models built measures 5mm or 32mm on a side, with 1024 or 2048 LEDs. They capture brain activity at 20 000 samples a second, enabling .
“This enables precise and real-time displays of cortical dynamics during critical surgical interventions,” said Youngbin Tchoe, the first author and co-inventor, formerly a postdoc in the Dayeh group at UC San Diego and now an assistant professor at Ulsan National Institute of Science and Technology.
In addition to the LEDs, the device includes acquisition and control electronics as well as software drivers to analyse and project cortical activity directly from the surface of the brain.
“The brain iEEG-microdisplay can impressively both record the activity of the brain to a very fine degree and display this activity for a neurosurgeon to use in the course of surgery. We hope that this device will ultimately lead to better clinical outcomes for patients with its ability to both reveal and communicate the detailed activity of the underlying brain during surgery,” said study coauthor Jimmy Yang, a neurosurgeon and assistant professor at The Ohio State University.
Next steps
Dayeh’s team is working to build a microdisplay that will include 100 000 LEDs, with a resolution equivalent to that of a smartphone screen – for a fraction of the cost of a high-end smartphone. Each LED in those displays would reflect the activity of a few hundred neurons.
These brain microdisplays would also include a foldable portion. This would allow surgeons to operate within the foldable portion and monitor the impact of the procedure as the other, unfolded portion of the microdisplay shows the status of the brain in real time.
Researchers are also working on one limitation of the study – the close proximity of the LED sensors and the PtNRGrids led to a slight interference and noise in the data.
The team plans to build customised hardware to change the frequency of the pulses that turn on the LEDs to make it easier to screen out that signal, which is not relevant to the brain’s electrical activity.
Professor Bob Mash. (Photo: Division of Family Medicine and Primary Care, Stellenbosch University)
By Bob Mash for Spotlight
To drum up support as South Africans head to the polls, President Cyril Ramaphosa reportedly vowed to “end the apartheid that remains in healthcare” when he hit the campaign trail. Professor Bob Mash has three health reforms on his wishlist for the incoming administration to prioritise.
South Africa is battling a quadruple burden of disease that includes HIV and tuberculosis (TB), non-communicable diseases such as diabetes, hypertension and mental health problems, challenges with maternal and child health, as well as substantial trauma from interpersonal violence and road traffic accidents.
At least 80% of the population is dependent on public sector health services. However, currently, we are in a state of austerity, with substantial cuts to the health budget that undermine years of work to improve the quality and coverage of health services.
In this context, what health reforms can be recommended?
In 2008, the World Health Organization (WHO) told us that we need primary healthcare “now more than ever” and recommended four health reforms. Universal health coverage has become a mantra for governments and implies that everyone should have easy access to quality primary care without any significant financial barriers. They also recommended that services should move away from a focus on a few priority diseases (such as HIV) and selected health programmes (such as immunisations). Rather, services should be integrated and built around the needs of people, across the life course, and in a comprehensive approach that spans health promotion, disease prevention, treatment, rehabilitation, and palliative care.
The WHO also recommended that integrated primary care be combined with essential public health functions. In other words, we don’t just worry about the people who enter the doors of the clinic but think about the health needs of all the people living in the catchment area. Finally, they recommended transformation of the leadership in health to make it more collaborative and to dialogue on policy with multiple stakeholders.
In South Africa, our last set of reforms were known as primary healthcare re-engineering. This led to the establishment of specialist clinical teams in each district to improve maternal and child healthcare, the establishment of teams of community health workers to extend the work of the clinic into the community and a focus on better health services – like health screenings and HPV vaccinations – at primary and secondary schools.
Of course, the other major policy reform that is still on the table is the introduction of national health insurance (NHI) to improve health equity and universal health coverage.
Going forward, three areas need urgent reform and attention.
More family physicians
Firstly, notwithstanding the 2030 Human Resources for Health Strategy, South Africa does not really have a comprehensive policy on the human resources for health that are needed. Thinking on primary healthcare and district hospitals has been particularly flawed in relation to family physicians. South Africa created a new medical speciality of family medicine in 2008 which has led to the training of family physicians in all nine medical schools. These are doctors who spend four years of additional training to be specialists in family medicine and to work in primary healthcare and district hospitals.
Family physicians are known to improve the quality of primary and district hospital care. They bring expertise closer to the community, capacitate the whole clinical team, improve quality, patient safety and reduce litigation. Adding a family physician to the clinical team is a cost-effective intervention. Despite this, only one province has really gone to scale with the employment of family physicians. This is a wasted opportunity and a low-hanging fruit in terms of reform.
The South African Academy of Family Physicians has a medium-term goal of one family physician at every community health centre, every district hospital and subdistrict (without a health centre). To achieve this, we need provinces to incrementally create posts over the next 10 years and to support an increase in the number of training opportunities.
Community-orientated primary care
As previously mentioned, we have introduced community health worker (CHW) teams into primary healthcare across the country. Unfortunately, many of these teams are dysfunctional due, for example, to an absence of supportive supervision, lack of resources or poor collaboration with the local primary care facility. Often, they are regarded as just extensions of the facility-based services and expected to perform tasks allocated by the clinic nurses.
The presence of these community health worker teams is, however, a huge opportunity to introduce community-orientated primary care (COPC). This model of primary care makes the switch to a focus on the health needs of the whole population served. Introducing COPC requires commitment to nine essential principles for organising primary healthcare.
Firstly, there must be a clear delineation of the community served and CHWs given responsibility for designated households (typically 250 households per CHW). Facility-based and community-based health care workers must operate as one multidisciplinary team and offer a comprehensive approach as described earlier. The team must make a careful analysis of the health needs in their community and also the resources available (government, non-government and private, health and social services) to address these needs.
At this local level, the team should prioritise the health needs in a participatory process with community and other stakeholders, and develop interventions tailored to their community. This process requires a commitment to community and stakeholder engagement. It also requires data to provide information on the health needs and this can come from households, facilities, and other sources. Finally, the service should be built around the needs of people and ensure that equity is improved.
The implementation of CHWs across the country needs to be reframed within a clearer policy on COPC. One province has already published its intention to make COPC the model of care and other provinces have examples of best practice.
Honing in on diabetes, hypertension, and mental health care
The final area that needs reform with more resources and attention is non-communicable diseases – particularly diabetes, hypertension, and mental healthcare. Historically, we have focused on the challenges of HIV and TB in service delivery, research, and donor funding. We have also been mindful of the need to improve maternal and child health.
Diabetes is now the leading cause of death in women in South Africa. Hypertension, heart disease and stroke are together the largest cause of deaths across all causes. Mental health, substance abuse and psychosocial problems may not cause death, but are a huge cause of morbidity and illness.
There is a danger of inequity by disease, and we need to ensure that we allocate resources commensurate to the problem of non-communicable diseases. In particular, we need to ensure that we have patient education and counselling that empowers people for lifestyle change, self-management and better mental health. Interventions are also needed in communities and the population to make healthier choices (on problem-solving, physical activity, healthy eating, tobacco smoking, alcohol and substance use) the easier choice.
Improving people’s health and healthcare is essential for sustainable development in South Africa. As the country heads to the polls, the incoming government would do well to keep this in mind. Such reforms will lead to higher quality primary healthcare and help pave the way for the proposed national health insurance.
*Mash is the Executive and Divisional Head of the Department of Family and Emergency Medicine in the Faculty of Medicine and Health Sciences at Stellenbosch University. The views expressed are those of the author and do not necessarily reflect those of Stellenbosch University.
Stimulating a small cluster of neurons in the brain appears to create a response in mice that mimics nociplastic pain, a type of unexplained chronic pain, researchers at the University of Washington School of Medicine in Seattle have found.
“When we stimulate these neurons, the mouse behaves as though gentle touch is very painful, which is one of the characteristics of nociplastic pain,” said Richard Palmiter, a professor of biochemistry and investigator of the Howard Hughes Medical Institute. Dr Logan Condon, who spearheaded this research as a PhD student at UW, was lead author on the paper, which was published in Cell Reports.
Chronic pain can arise from ongoing injury or persistent damage to the nervous system. Pain caused by injury is called nociceptive from the Latin nocere “to harm.” Pain due to nerve damage is called neuropathic. But these categories do not explain a common form of chronic pain the persists even after an injury has fully healed and there is no evidence of neurological damage. This led the International Association for the Study of Pain to define a new category called nociplastic pain, meaning “able to be moulded.”
Although the cause of nociplastic pain is unknown, scientists think it involves changes in pain circuits in the spinal cord and brain. These changes result in the perception of pain even when no nerve injury exists.
In the new study, researchers demonstrated that stimulating a cluster of cells in the brain’s parabrachial nucleus can generate chronic pain behaviour typical of nociplastic pain. They also showed that inhibiting these cells can prevent pain from nerve injury.
The parabrachial nucleus is in an area of the brain known as the pons. It acts as a hub that relays aversive sensory information from the body to different parts of the brain. The parabrachial neurons found to create nociplastic pain are called Calca neurons, named for a defining gene for these cells.
“You can think of these Calca neurons as a warning system for the brain,” said Palmiter. “They respond to any aversive event you can think of – a pinch, a visual threat, a bad odour, a loud noise – and they tell your brain that something bad is happening in the environment and you’d better do something about it.”
It is possible to manipulate genetically defined neurons using viral techniques to express molecules that activate, or inhibit, those neurons.
The researchers also found that the nociplastic pain behaviour continues even after the Calca-neuron activation has stopped. This suggests signals from the stimulated Calca neurons cause persistent effects – a sign of plasticity – in the nerve circuits leading to the spinal cord.
They also showed that it was possible to create nociplastic behaviours in the mice by exposing them to unpleasant, aversive experiences like nausea, chemotherapy drugs or migraine-like conditions.
Palmiter’s team is currently focusing on the neural circuits and plasticity that arises when parabrachial Calca neurons are activated.
“The brain is somehow sending signals to the spinal cord,” he said. “We want to figure out the pathway for those signals.”
NIH-led study finds genetic markers that explain up to 12% of the differences between two people’s blood pressure.
Photo by CDC on Unsplash
National Institutes of Health researchers and collaborators have discovered over 100 new regions of the human genome, also known as genomic loci, that appear to influence a person’s blood pressure. Results of the study also point to several specific genomic loci that may be relevant to iron metabolism and a type of cellular receptor known as adrenergic receptors.
The study, published in Nature Genetics, is one of the largest such genomic studies of blood pressure to date, including data from over 1 million participants and laying the groundwork for researchers to better understand how blood pressure is regulated. Such insights could point to potential new drug targets.
“Our study helps explain a much larger proportion of the differences between two people’s blood pressure than was previously known,” said first author Jacob Keaton, PhD. “Our study found additional genomic locations that together explain a much larger part of the genetic differences in people’s blood pressure. Knowing a person’s risk for developing hypertension could lead to tailored treatments, which are more likely to be effective.”
Hypertension often runs in families, meaning that there is a genetic component to developing the condition in addition to environmental contributions such as a high-salt diet, lack of exercise, smoking and stress.
To understand the genetics of blood pressure, the researchers combined four large datasets from genome-wide association studies of blood pressure and hypertension. After analysing the data, they found over 2000 genomic loci linked to blood pressure, including 113 new regions. Among the newly discovered genomic loci, several reside in genes that play a role in iron metabolism, confirming previous reports that high levels of accumulated iron can contribute to cardiovascular disease.
The researchers also confirmed the association between variants in the ADRA1A gene and blood pressure. ADRA1A encodes a type of cell receptor, called an adrenergic receptor, that is currently a target for blood pressure medication, suggesting that other genomic variants discovered in the study may also have the potential to be drug targets to alter blood pressure.
“This study shows that these big genome-wide association studies have clinical relevance for finding new drug targets and are needed to discover more drug targets as we go forward,” said Dr Keaton.
From these analyses, the researchers were able to calculate a polygenic risk score, which combines the effects of all genomic variants together to predict blood pressure and risk for hypertension. These risk scores consider which genomic variants confer risk for hypertension and reveal clinically meaningful differences between people’s blood pressure.
Polygenic risk scores have potential to serve as a useful tool in precision medicine, but more diverse genomic data is needed for them to be applicable broadly in routine health care. While the collected data was mostly from people of European ancestry, the polygenic risk scores were also applicable to people of African ancestry.