The Achilles tendon, although considered the toughest in the body, can rupture, with many such injuries involving sports enthusiasts in their 30s or 40s. Surgery might be required, and a prolonged period of rest, immobilisation, and treatment can be difficult to endure. Researchers in Japan have developed an approach using irradiation with plasma to accelerate healing.
A research team led by Osaka Metropolitan University Graduate School of Medicine’s Katsumasa Nakazawa, a graduate student in the Department of Orthopedic Surgery, Associate Professor Hiromitsu Toyoda, and Professor Hiroaki Nakamura, and Graduate School of Engineering Professor Jun-Seok Oh has focused on non-thermal atmospheric-pressure plasma (the electrically-charged gas such as found in a neon lamp – not blood plasma!) as a treatment method for tendon repair.
Their study, published in PLOS ONE, is the first to show that such plasma irradiation can accelerate tendon repair.
The team ruptured then sutured the Achilles tendon of lab rats. For one group of rats, the sutured area was irradiated with a helium plasma jet.
The plasma-irradiated group exhibited faster tendon regeneration and increased strength at two, four, and six weeks after surgery compared to the untreated group.
“We have previously discovered that irradiation of non-thermal atmospheric-pressure plasma has the effect of promoting bone regeneration. In this study, we discovered that the technology also promotes tendon regeneration and healing, showing that it has applications for a wide range of fields,” Professor Toyoda declared. “Combined with current tendon treatments, it is expected to contribute to more reliable tendon regeneration and shorter treatment time.”
Professor Susan Cleary delivering her inaugural lecture as part of a lecture series by the University of Cape Town. (Photo: Supplied)
President Cyril Ramaphosa recently signed the NHI Bill into law. The question is whether this will bring South Africa closer towards Universal Health Coverage. Professor Susan Cleary argues that the NHI is a wide ranging reform with both positive and controversial aspects. The key will be to find a middle ground in order to continue on the journey to UHC.
President Cyril Ramaphosa signing the National Health Insurance (NHI) Act on the eve of the elections is a smart move from the perspective of a political party seeking to shore up its base. The concern though to those of us working to strengthen the health system is whether the NHI will enable the country to move closer towards Universal Health Coverage.
For the NHI naysayers, perhaps it would be important to alleviate some fears and concerns. The NHI is a long-term project. In the 2024 budget, National Treasury reduced the conditional grant allocations to the NHI in comparison to what was allocated in the 2023 budget. While signing the NHI Bill into law is a step forward, the reduction in resources towards NHI implementation reminds us that this is a long term project. In addition, it is likely that there will be legal challenges which will lead to considerable delays for the scheme to be fully implemented.
The NHI is a wide-ranging reform, with many positive aspects sitting alongside some key controversial aspects. Positive aspects include the opportunity to enable greater use of evidence and transparency in priority setting through the further institutionalisation of Health Technology Assessment processes (akin to ‘NICE’ in the UK), as well as the opportunity to use national-level purchasing power to drive down the prices of commodities such as medicines. The role of private multidisciplinary practices (GPs, nurses, health and rehabilitation professionals, etc) in the future NHI also holds some promise to improve access to healthcare particularly to parts of the country with limited access to public clinics.
On the other hand, there are two key controversial aspects. The first is related to what may or may not happen to medical schemes and medical scheme administrators once the NHI is fully implemented. My sense is that there is no short-term concern in this regard. A bigger concern is whether a single pot of money in the NHI fund will present a larger or a smaller corruption risk than the current situation of multiple pots spread across provincial treasuries and medical aid schemes.
Another concern is that the NHI reform might disrupt our ongoing progress towards Universal Health Coverage within our existing public sector. Our public sector is not perfect, but it is a system that has equity at its heart. The common definition of Universal Health Coverage is to provide all individuals and communities with access to needed promotive, preventive, resuscitative, curative, rehabilitative and palliative health services of sufficient quality to be effective, while ensuring that the utilisation of these services does not expose users to financial hardship.
The two main goals of Universal Health Coverage are: (1) the provision of quality health care services to those in need and (2) the avoidance of financial catastrophe in this process. Clearly healthcare is far from free – indeed it is very expensive – and so the goal of avoiding financial catastrophe is about implementing prepayment and risk pooling mechanisms, whether these are tax or insurance based.
Let’s first look at how we are doing on the provision of quality services. The below figure plots countries according to their achievements on the Universal Health Coverage Service Coverage Index. In this context, coverage of essential health services is measured based on indicators that include reproductive, maternal, newborn and child health, infectious diseases, non-communicable diseases and service capacity and access, among the general and the most disadvantaged populations.
On this index, South Africa’s achievement is at just over 70%, similar to many other middle-income countries. While there would be room for improvement, our performance is in line with our global peers.
Global comparison of countries in terms of service coverage and quality
Source: World Health Organization – Global Health Observatory (2024) processed by Our World in Data. Accessed May 2024.
The second indicator is financial risk protection. The below figure plots countries against the percent of total health expenditure that is paid out of pocket at the point of use. On this indicator, we score 5.7%, indicating extremely high levels of financial risk protection.
Global comparison of countries in terms of the percent of total health expenditure that is paid out of pocket
Source: World Health Organization (via World Bank) processed by Our World in Data. Accessed May 2024.
While this does not mean that there are no instances of financial catastrophe, undoubtedly there would be, particularly for those seeking treatment for certain types of cancers. That said, over the past two decades I have studied this issue extensively. Across a wide range of conditions in diverse settings, we have interviewed tens of thousands of people to understand the costs that they face in using health services, including everything from transport costs, to costs of food, shelter or accommodation, costs of child care, lost income, under the counter payments to public sector providers (which we never found), fees paid to private providers or money spent at pharmacies. This research consistently showed that the level of catastrophic spending was very low. Our performance on financial risk protection is outstanding. I celebrate the work of those colleagues that shepherded in the removal of user fees in our national health system during the dawning of our democracy. We should all be thanking them.
Despite these successes on Universal Health Coverage, there are areas of concern for the South African health system. We do not achieve health outcomes commensurate with our level of investment. My sense is that this is driven by our relatively high burden of disease; for example we continue to have the world’s largest HIV treatment programme. While our average life expectancy steadily increased with the introduction of antiretroviral therapy (although note the downturn from 2020 which coincides with the Covid-19 pandemic – see the below figure), the HIV epidemic has been a cruel setback that needs to be considered when we seek to make global comparisons on life expectancy and avertable mortality.
Global comparisons of life expectancy: 1970 – 2020
Source: United Nations World Population Prospects (2022) processed by Our World in Data. Accessed May 2024.
Now that the NHI Bill has become the NHI Act, it is time to move on from debates about whether we need NHI or not, and rather focus on how we can make the NHI work for us.
Our public sector will be the backbone of our future NHI and so we should seek to continue to strengthen this system. It would also be wise to put in place measures to strengthen our private system given that private providers are intended to play a key role in the NHI. We should be pragmatic.
The NHI includes many exciting opportunities for leveraging big data and artificial intelligence in health systems strengthening, but at this stage we hardly have any electronic health data. A clear step forward would be the further implementation of the National Digital Health Strategy (2019-2024) which includes the establishment of a patient electronic health record, amongst other needed developments.
In addition, the NHI places emphasis on the achievement of a purchaser provider split via establishing ‘Contracting Units for Primary Health Care’ (CUPS). These new entities will contract with both public and private providers within a defined geographic area, on behalf of a particular population. The establishment of CUP ‘proof of concept’ sites is therefore a priority, but must be done in a way that generates learning and enables adaptation to different contexts.
Let’s continue to push forward on many of these complex undertakings. It is going to take time, but it is needed, irrespective of the name that we choose to give to our health system.
*Cleary is professor of health economics and the head of the School of Public Health at the University of Cape Town.
Note: The views expressed in this opinion piece are not necessarily shared by the Spotlight editors. Spotlight is committed to publishing a variety of views and facilitating informed discussion that deepens public understanding of health issues.
New research indicates that various features assessed through imaging tests can reveal an individual’s risk of developing meniscus tears, which is one of the most common knee injuries.
The study, which is published in the Journal of Orthopaedic Research, was based on the use of radiomics, which unveils imperceptible patterns in medical images. Investigators used magnetic resonance images from 215 people with intact menisci at the start of the study who had 4-year meniscal status data.
Over 4 years, 34 participants developed meniscus tears. Use of radiomics at the start of the study correctly classified 24 of these 34 cases and 172 of 181 controls with a sensitivity of 70.6% and a specificity of 95.0%. Therefore, the technique provides sensitive and quantitative measures of meniscus alterations that could help clinicians know when to intervene to safeguard against meniscus tears.
“Understanding meniscus tear risk through radiomics opens new possibilities for proactive knee health management, offering clinicians a valuable tool to anticipate and prevent such injuries,” said corresponding author Matthew Harkey, PhD, ATC, of Michigan State University.
As research continues to produce evidence about the underlying causes of obesity and optimal strategies to treat and manage obesity have evolved, there are disparities in application of the latest scientific advances in the clinical care for people with obesity. Widespread adoption of current findings, consistency of care and expertise in obesity care varies by health care professional and institution. These findings are detailed in a new American Heart Association scientific statement, “Implementation of Obesity Science Into Clinical Practice,” published in the journal Circulation.
“Obesity is undeniably a critical public health concern in the U.S. and around the world, affecting nearly all populations and straining our health care systems,” said Deepika Laddu, Ph.D., FAHA, chair of the statement writing committee and a senior research scientist at Arbor Research Collaborative for Health in Ann Arbor, Michigan. “As a major risk factor for heart disease, obesity has significantly hindered progress in reducing heart disease rates. Despite advancements in understanding the complexities of obesity and newer treatment options, major gaps remain between obesity research and real-world implementation in clinical practice.”
Studies show intensive lifestyle therapy is considerably more effective for weight loss than brief advice from a health care professional. However, general educational information is offered more frequently by health professionals rather than referrals to classes, programs or tangible resources for lifestyle changes. One study revealed that only 16% of health care professionals had working knowledge about evidence-based lifestyle treatments for obesity, including diet and nutrition, physical activity and intensive behavioral therapy referral. Other barriers to addressing weight loss are exacerbated by socioeconomic and racial or ethnic inequities. People of diverse races and ethnicities and people who are covered by Medicare or Medicaid are less likely to be referred to weight management programs or to have them covered by insurance.
For about 30 years, the prevalence of obesity in the US and around the world has been escalating. Recent estimates indicate more than 40% of US adults ages 20 and older are living with obesity, according to the US Centers for Disease Control and Prevention.
Research has led experts to unlock the multifactorial causes of obesity, including sociological and physiological determinants of health. Treatments for obesity have also evolved with more strategies for lifestyle modifications, medication therapy and bariatric surgery – but each treatment approach comes with challenges.
“While significant strides have been made in advancing the science to help us understand obesity, there remains a considerable gap between what we know and what happens in the doctor’s office,” said Laddu. “Health care professionals and health care systems need to find better ways to put what we know about obesity into action so more people can get the right support and treatment. Adopting new technologies and telemedicine, making referrals to community-based weight management programs to encourage behavioural change, providing social support and increasing reach and access to treatments are just some of the promising methods we could implement to unlock successful, evidence-based obesity care.”
Weight loss medications
Glucagon-like peptide-1 (GLP-1) agonists, such as high-dose semaglutide and tirzepatide, are the most recently FDA-approved medications for long-term weight management, and both are associated with an average weight loss of more than 10% at six months in clinical studies. However, despite half of adults in the U.S. meeting the BMI criteria for obesity and being eligible for these medications, a small proportion of this population is currently taking them.
Weight loss surgery
In the decades since bariatric (weight loss) surgery was first introduced as an option for people with severe obesity, there have been advances in the expertise and safety of the procedures, as well as an increased understanding of the health benefits that often result after bariatric surgery. A comprehensive review of studies focused on weight loss surgeries showed that patients who underwent bariatric surgery had lower risks of cardiovascular disease and decreased risks for multiple other obesity-associated conditions, including Type 2 diabetes and high blood pressure. One challenge facing health care professionals is ensuring that the populations with the greatest needs have access to bariatric surgery in terms of costs, resources and social support.
The statement describes strategies that both address these challenges and improve how obesity-based research is incorporated into clinical care. The statement also identifies the need to develop solutions across populations in order to manage obesity at the community level. Potential improved public health policies and future research to expand patient care models and optimize the delivery and sustainability of equitable obesity-related care are suggested.
Specific approaches are highlighted in the statement to help bridge the gap between the science about obesity and clinical care, such as:
To reach and successfully impact populations in need, health care professionals may consider how social determinants of health, including insurance type, household income, race and ethnicity, environment, health literacy, access to health-promoting resources and social supports all influence the likelihood of successful patient treatment.
Education for health care professionals explaining the complex origins and clinical consequences of obesity is discussed. Such training should emphasize information about diagnosis, prevention and treatment of obesity. Despite the high prevalence of obesity around the world, there is a lack of education programs centered on obesity for medical professionals.
Further evaluation of health policy changes that health care systems and insurance plans can implement and scale in order to make obesity treatment affordable for patients, especially those at high risk for adverse outcomes such as cardiovascular disease.
A framework for delivering obesity care into clinical practice settings is reviewed, as well as efforts by some professional societies for developing interventions that make obesity treatment more accessible.
“The statement emphasises the importance of a comprehensive approach across different levels of health care delivery and public policy, along with the adoption of feasible, evidence-based strategies in clinical settings,” said Laddu. “It also underscores the need for future research and policy changes to improve current patient care models and ensure equitable access to obesity-related care for people in underrepresented groups.”
The scientific statement also provides possible solutions for how to help people in their day-to-day lives, including interventions with digital technology and access through telemedicine. However, more research is needed in obesity science and treatment. Limited understanding of the cost-effectiveness of obesity prevention and the long-term health outcomes for established therapies has hindered the implementation of obesity science into clinical settings. Cross-collaborative obesity science research between stakeholders and health economists may serve as the bridge to developing and scaling cost-effective prevention programs.
Study could challenge widespread view that fleas, rats are the only contributors to outbreaks
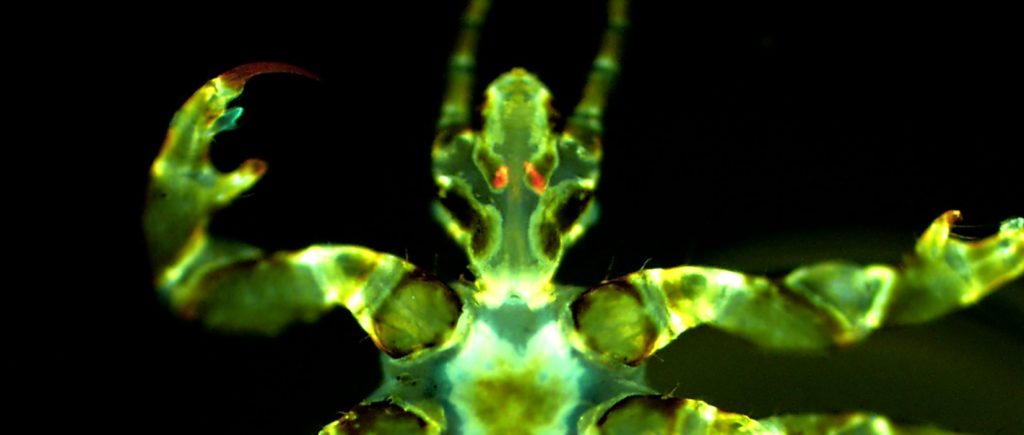
Fluorescent image of a human body louse with Yersinia pestis infection (orange/red) in the Pawlowsky glands. Image Credit:David M. Bland (CC0)
A new laboratory study suggests that human body lice are more efficient at transmitting Yersinia pestis, the bacterium that causes plague, than previously thought, supporting the possibility that they may have contributed to past pandemics. David Bland and colleagues at the United States’ National Institute of Allergy and Infectious Diseases present these findings in the open-access journal PLOS Biology on May 21st.
Y. pestis has been the culprit behind numerous pandemics, including the Black Death of the Middle Ages that killed millions of people in Europe. It naturally cycles between rodents and fleas, and fleas sometimes infect humans through bites; thus, fleas and rats are thought to be the primary drivers of plague pandemics. Body lice – which feed on human blood – can also carry Y. pestis, but are widely considered to be too inefficient at spreading it to contribute substantially to outbreaks. However, the few studies that have addressed lice transmission efficiency have disagreed considerably.
To help clarify the potential role of body lice in plague transmission, Bland and colleagues conducted a series of laboratory experiments in which body lice fed on blood samples containing Y. pestis. These experiments involved the use of membrane feeders, which simulate warm human skin, enabling scientists to study transmission potential in a laboratory setting.
They found that the body lice became infected with Y. pestis and were capable of routinely transmitting it after feeding on blood containing levels of the pathogen similar to those found in actual human plague cases.
They also found that Y. pestis can infect a pair of salivary glands found in body lice known as the Pawlowsky glands, and lice with infected Pawlowsky glands transmitted the pathogen more consistently than lice whose infection was limited to their digestive tract. It is thought that Pawlowsky glands secrete lubricant onto the lice’s mouthparts, leading the researchers to hypothesise that, in infected lice, such secretions may contaminate mouthparts with Y. pestis, which may then spread to humans when bitten.
These findings suggest that body lice may be more efficient spreaders of Y. pestis than previously thought, and they could have played a role in past plague outbreaks.
The authors add, “We have found that human body lice are better at transmitting Yersinia pestis than once appreciated and achieve this in more than one way. We describe a new bite-based mechanism in which a set of accessory salivary glands unique to lice, termed the Pawlowsky glands, become infected with Y. pestis and secrete lubricant containing plague bacilli onto the insect’s mouthparts prior to blood feeding.”