People who drink more than three litres of fluid a day may be suffering from a rare condition known as vasopressin deficiency. For many, however, it is just a harmless habit. Failing to differentiate the two correctly can be fatal, so researchers have been investigating what kind of test delivers a reliable diagnosis.
In most cases, drinking excessive amounts of fluid, known as polyuria-polydipsia syndrome, either arises out of habit over time or is concomitant with a psychological illness. In rare cases, however, it can be caused by vasopressin deficiency. This hormone, released by the pituitary gland, regulates the body’s water and salt content. People with vasopressin deficiency cannot concentrate their urine, causing them to lose large quantities of fluid and to feel very thirsty.
It is extremely important to differentiate between a “harmless” form of excessive fluid ingestion and vasopressin deficiency: in the first case, those affected receive behavioural therapy to help them reduce their fluid intake gradually. People with vasopressin deficiency, however, are given the hormone vasopressin. If a patient is mistakenly treated with vasopressin, it can lead to water intoxication, which can be life-threatening.
Test with salt or arginine?
Over the past few years, the two research group leaders Professor Mirjam Christ-Crain and PD Dr Julie Refardt, together with a number of national and international centres, have been working intensively on testing methods to distinguish between these two disorders. They have found that a test that stimulates vasopressin release via a highly concentrated salt infusion is very reliable. “However, due to the resulting increase in salt concentration, constant monitoring is necessary, including half-hourly measurements of the salt levels in the patients’ blood,” explains Professor Christ-Crain.
A simplified and more easily tolerated test uses an infusion of arginine. Arginine, an essential amino acid, also stimulates the release of vasopressin and was shown to deliver a reliable diagnosis.
Clarity in diagnostics
With an international team, Christ-Crain and Refardt have now performed a direct comparison between the two tests and have published the results in the New England Journal of Medicine. The study, involving 158 participants, shows that the salt infusion resulted in a correct diagnosis for over 95% of patients. The test that uses arginine infusion, however, only led to a correct diagnosis in just under 75% of cases. Dr Refardt sums up: “In view of these results, we recommend the salt infusion test as the gold standard for reliable differentiation between polydipsia and vasopressin deficiency.”
Vitamin B12 is a well-known micronutrient that has long been acknowledged for its essential role in maintaining nerve function, supporting red blood cell production, and facilitating DNA synthesis, all vital processes for overall health. Researchers have now discovered that vitamin B12 also plays a pivotal role in cellular reprogramming and tissue regeneration. The findings have been published in the journal Nature Metabolism.
The research was focused on an experimental process known as cellular reprogramming which is thought to mimic the early phases of tissue repair. The IRB team found that cellular reprogramming in mice consumes large amounts of vitamin B12. Indeed, the depletion of vitamin B12 becomes a limiting factor that delays and impairs some aspects of the reprogramming process. Considering the abundance of vitamin B12 in the normal diet of mice, the investigators were surprised to observe that the simple supplementation of vitamin B12 significantly enhanced the efficiency of reprogramming.
Therapeutic potential in ulcerative colitis
The researchers validated their findings in a model of ulcerative colitis, demonstrating that the intestinal cells initiating repair undergo a process similar to cellular reprogramming and also benefit from vitamin B12 supplementation. Patients with intestinal bowel disease could potentially benefit from vitamin B12 supplementation.
“Our research uncovers a critical role of vitamin B12 in cellular reprogramming and tissue repair. These findings hold promise for regenerative medicine, with the potential to benefit patients through an improved nutrition,” says lead researcher Dr Manuel Serrano at IRB.
Understanding the role of vitamin B12 in cellular reprogramming
In this study, the researchers delved into the metabolic requirements of cellular reprogramming and found that vitamin B12 is a limiting factor for a particular branch of metabolism involved in a reaction known as methylation. Precisely, the DNA of the cells initiating reprogramming or tissue repair require very high levels of this methylation reaction and therefore of vitamin B12. The researchers discovered that vitamin B12 insufficiency during reprogramming or tissue repair resulted in significant epigenetic changes, leading to errors in the function of multiple genes.
“Supplementation with vitamin B12 corrected this imbalance, resulting in enhanced gene function fidelity and overall improved reprogramming efficiency,” confirms Dr. Marta Kovatcheva, first author of the study and a postdoctoral researcher in the same laboratory. Dr. Kovatcheva will open a new laboratory in 2024 at the Istituto Fondazione di Oncologia Molecolare ETS (IFOM) in Milan, Italy, which will be focused on the study of partially reprogrammed cells in vivo.
Separate study links vitamin B12 to lower inflammation
The group led by Dr. Serrano has recently published another study, in collaboration with the laboratory of Dr. Rosa Lamuela-Raventós at the University of Barcelona (UB), and Dr. Ramon Estruch at the Hospital Clínic of Barcelona, in which they concluded that people with higher levels of vitamin B12 in blood had lower levels of inflammatory markers (IL-6 and CRP). The researchers also observed a similar relationship in aged mice. These observations suggest that vitamin B12 exerts anti-inflammatory action by reducing these markers in the body and they provide valuable insights into the potential health benefits of vitamin B12.
A meta-analysis of studies published over the past 40 years on cannabis use during pregnancy has found an association between foetal exposure to cannabis in the womb and preterm delivery, low birth weight and the need for neonatal intensive care admission (NICU). The study was published today in the journal Addiction.
Previous research has indicated that THC, the main psychoactive component in cannabis, can cross the placenta to the foetus during pregnancy and bind to receptors in the foetal brain.
The meta-analysis examined the results of 57 studies around the world that included almost 13 million infants in total. Based on either self-reports from pregnant women, or blood and saliva testing depending on the study, just over 100 000 infants were found to be exposed to cannabis in the womb. While none of the studies found a direct causal relationship between cannabis use during pregnancy and adverse birth outcomes, the combined results indicated that newborns exposed to cannabis during pregnancy were twice as likely to require NICU admission, twice as likely to have a low birth rate and one and a half times more likely to be born early.
While there has been little research on cannabis use during pregnancy since cannabis was legalised in Canada five years ago, an American study has indicated an increase in cannabis use during pregnancy in states where it has been legalised and the perceived risk of harm from cannabis has decreased. The study states that overall cannabis use in pregnancy has doubled in the past 20 years, with approximately 10% of pregnancies associated with cannabis exposure. Some studies indicated it was being used to alleviate symptoms of nausea, poor appetite, insomnia or anxiety during pregnancy.
“This research emphasizes the importance of healthcare providers making an effort to create a safe space talking to pregnant women and women planning to be pregnant about their cannabis use and their motivations for using it to educate them about the potential risks and empower them to make informed decisions for their child,” says lead author Maryam Sorkhou, a PHD student within the addictions division at CAMH as well as the University of Toronto. Ms Sorkhou is overseen at CAMH by Senior Scientist and paper co-author Dr Tony George.
Researchers have been trying to develop antiretroviral medicines that can last for weeks, months or even years per dose. It is thought that such long-acting therapies may eventually end up replacing the daily pills taken by most people living with HIV today.
As pointed out by Dr Anushka Naidoo, a Clinical Pharmacologist and Principal Investigator and Scientist at the Centre for AIDS Programme of Research in South Africa (CAPRISA), three such long-acting HIV medicines have made it to market so far. They are the injectables cabotegravir (CAB-LA) and rilpivirine (RPV-LA) and the dapivirine vaginal ring (DPV-VR). Of these only CAB-LA (two-monthly) and DPV-VR (monthly) have so far been approved by the South African Health Products Regulatory Authority (SAHPRA) for HIV prevention. CAB-LA and RPV-LA have been approved for HIV treatment in the United States, but not yet by SAHPRA.
Image: DOH
CAB-LA and DPV-VR are being rolled out as HIV pre-exposure prophylaxis (PrEP) in pilot studies in South Africa. Spotlight earlier this year provided an update on these pilots here.
How do long-acting formulations work?
Dr Sindiswa Maphumulo, a Specialist Virologist and lecturer at the University of the Free State, tells Spotlight that designing long-acting formulations is a very complex and costly process. She explains that when designing any drug, whether it is long-acting or not you need to look at two things – pharmacodynamics and pharmacokinetics. Basically, she says, pharmacokinetics refers to what the body does with the drug in question while pharmacodynamics refers to what the drug does to the body.
“So you’re going to have to know what is the human body going to do to this drug once you’ve administered it and also what is the drug targeting or aiming to do in the human body once it has been given,” she says. For long-acting drugs, studies need to determine what the half-life (how long it lasts in the body) of the drug is so the doses can be timed correctly. It is also essential that different populations are studied to determine how individual’s bodies react to the drug.
“You want to make sure that there is a steady release of that specific drug, which depends on the drug class that you’ve chosen because we target different sites of HIV [with different drug classes],” she adds.
Naidoo tells Spotlight that: “Long-acting drug delivery formulations enable slow drug release after administering a single dose over the course of days, weeks, months or even years, and can maintain a steady pharmacokinetics profile.”
Naidoo says that long-acting drugs are formulated so that they form a “depot” of the drug, either through the way the drug is released into the body or the way device that contains the drug is designed to slowly release it over time. Several ways of achieving this has been investigated, including long-acting injectables, implants, infusion pumps, and patches. Long-acting injections and implants, for example, are already widely used in South Africa as contraceptives.
For HIV this means that ARVs can either be stored in the body and slowly absorbed or be stored in a device that is placed in the body which releases consistent drug levels over time. For example, “long-acting injectables are usually the same medication that is taken in pill form but when injected they allow for the slow release of medication into the blood over a longer period of time,” says Naidoo.
How CAB-LA works
Maphumulo explains that CAB-LA and DPV-VR fall under different drug classes which target different stages of the HIV viral replication cycle inside the human body. Cabotegravir is an Integrase Strand Transfer Inhibitor (INSTI) – which is to say it targets the integrase enzyme that allow HIV to integrate itself into a cell’s DNA.
“Cabotegravir’s unique physiochemical and pharmacokinetic properties have permitted its formulation and delivery both as an oral tablet for daily administration and as a long-acting nanosuspension for monthly to quarterly intramuscular injection,” Naidoo says.
“Cabotegravir LA is made from the free acid form of cabotegravir, which has a low water solubility, a long systemic half-life and high antiviral potency,” says Emmanuella Chinonso Osuala, a Research fellow and PhD student based at CAPRISA.
She explains that the properties of this drug make it suitable for a so-called nanosuspension delivery system and allows for high levels of the drug be contained in a small volume that can be administered through an intramuscular injection. This is achieved by manufacturing cabotegravir, through a process called wet-bead milling, to form nanocrystals – approximately 200nm in size. These have a large surface which allows for “a slower and controlled release of the drug over time”.
“[The] drug is released from the injectable suspension over several months due to the slow dissolution of crystals from the suspension,” Osuala explains.
How DPV-VR works
Naidoo explains that DPV-VR is a ring made of “a flexible silicone polymer” and contains the drug dapivirine, which is slowly released over the course of a month and can be inserted and replaced by the women themselves each month. A three-month ring is also currently in development.
“The ring delivers dapivirine directly at the site of potential infection, with low systemic exposure (it acts at the site of action in the vagina and is not released in significant amounts into the blood circulation), which could minimise side effects…and reduce the risk of developing HIV (drug) resistance,” she says.
Dapivirine, according to Maphumulo is part of a drug class called Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs), which block the reverse transcriptase enzyme on the HIV virus that allows for the transcription of HIV – which is an RNA virus into DNA. It is this transcription which would allow HIV to enter the human cell nucleus and replicate there.
Making current treatments long-acting
While long-acting forms of cabotegravir and dapivirine are clearly useful, these are far from the most widely used ARVs. Most HIV treatment in South Africa today is with a combination of three drugs, with the key one being dolutegravir. Earlier this year we reported on how more than 4.7 million people in the country have started or switched to dolutegravir-based HIV treatment in the last five years.
One group of researchers are trying to develop long-acting formulations of these commonly used ARVs. Using so-called drug combination nanoparticles (DcNP) they have developed a long-acting formulation of the ARVs tenofovir, lamivudine, and dolutegravir (LA-TLD) that shows some promise as a monthly injection. Early findings presented at this year’s International AIDS Society (IAS) conference in Australia and published in the journal AIDS suggest that the formulation achieves sufficient drug concentrations in non-human primates to allow for monthly dosing.
Dr Rodney Ho, an expert in biomedical science and pharmacology based at the University of Washington in the United States who led the research, tells Spotlight the study wanted to address a seemingly impossible question.
“Can we make three incompatible oral antivirals – tenofovir, lamivudine (which are water soluble) and dolutegravir (which is oil soluble and water-insoluble) – compatible and create a long-acting drug combination injectable product? With creativity and hard work, our team finally found a way to make this happen,” he says.
He explains that the three drugs were bound to lipid (fatty) nanoparticles using DcNP technology, which stabilises them so that the combination of drugs do not get released at the injection site immediately. Instead, the drugs are taken up by the body’s lymph and lymph nodes, which allows the drug to be metabolised within the body’s cells, which host the HIV virus, before it is taken up in the blood stream.
“As a result of this intentional design, LA-TLD has now provided data verifying that we are able to provide the necessary long-acting drug profile while achieving targeted drug exposure in cells and tissues of interest for an extended time,” Ho says.
“These results verified that a stable and scalable long-acting product, previously considered impossible, is now proven to be possible. This novel LA-TLD product can be administered via subcutaneous injection and will reach therapeutic drug levels within hours (not days which is needed for CABENUVA – LA-CAB and LA-RPV taken as HIV treatment). Thus, two-month oral leading doses may not be necessary,” he says.
Challenges around long-acting formulations
Osuala says there are several scientific challenges when it comes to long-acting formulations. This includes ensuring that: the drugs remain stable when released over long periods of time; sustained drug release is maintained; and the biocompatibility of the materials used in the product. Other challenges include issues around drug potency, as the amount of drug required for the formulation depends on its potency; as well as the cost and access to the formulations, as it is currently expensive to develop and manufacture which may hinder the accessibility of these products in low-and-middle-income (LMIC) countries.
Further challenges, according to Naidoo include the added complication that if adverse events occur for long-acting injectables, “one cannot simply stop taking the medication like one can with daily pills” since the drug will continue to be released into the body. One way to reduce this risk is through having an oral lead-in period where the drugs, like cabotegravir and rilpivirine that are set to be injected are first taken in pill form for four weeks, which can be stopped if an adverse event like hypersensitivity, an allergy or a severe side effect occurs.
Other challenges include the cold-chain storage requirements that some long-acting formulations and injections have, Naidoo says, “which can be challenging in LMIC settings so formulations without cold chain needs are needed.”
“The development of long-acting injectable formulations are a complex, time-consuming, and costly process. One of the challenges in the development of long-acting injectable formulations is the limited selection of ‘polymers’ and ’excipients’ (materials used to formulate the long-acting injectables that are available). As a result, some innovator companies develop proprietary excipients for use in long-acting injectable formulations, which can delay the development of generic long-acting injectable products,” she adds.
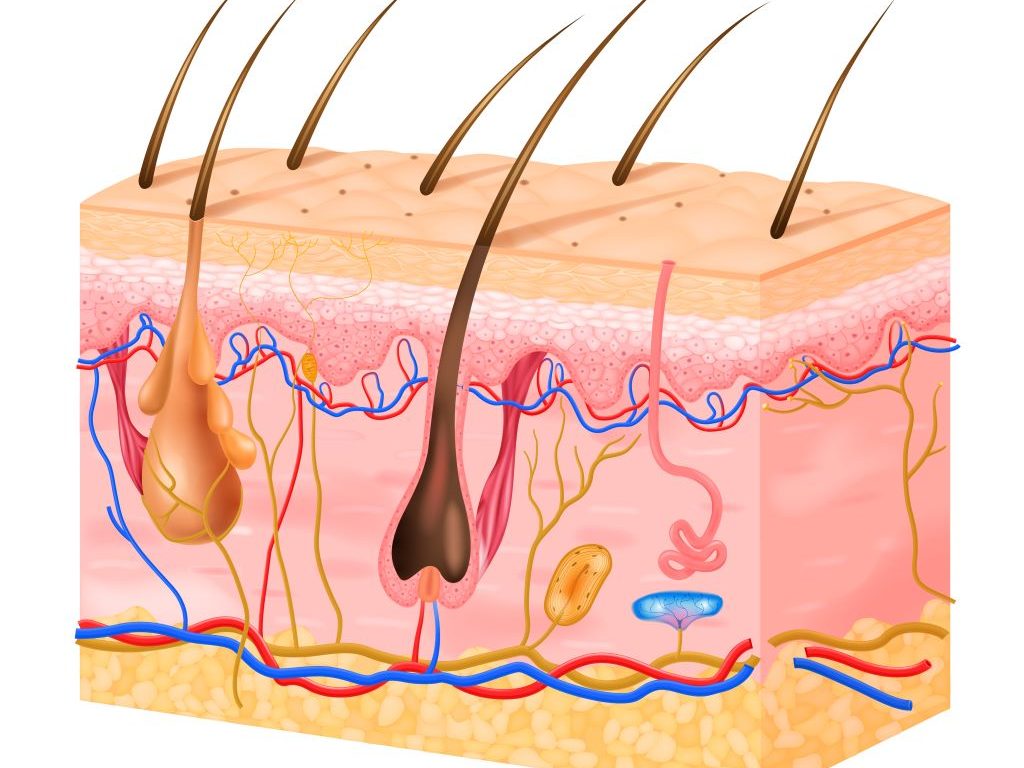
Researchers have shown for the first time that haemoglobin, a protein found in red blood cells where it binds oxygen, is also present in the epidermis. The study, which appears in the Journal of Investigative Dermatology, published by Elsevier, provides important insights into the properties of the skin’s protective external layer.
This research was driven by a curiosity about the protective role of the epidermis and what unexpected molecules are expressed in it. Researchers discovered the haemoglobin α protein in keratinocytes of the epidermis and in hair follicles. This unexpected evidence adds a new facet to the understanding of the workings of the skin’s defence mechanisms.
Lead investigator of the study Masayuki Amagai, MD, PhD, Department of Dermatology, Keio University School of Medicine, Tokyo, and Laboratory for Skin Homeostasis, RIKEN Center for Integrative Medical Sciences, Yokohama, explains: “The epidermis consists of keratinised stratified squamous epithelium, which is primarily composed of keratinocytes. Previous studies have identified the expression of various genes with protective functions in keratinocytes during their differentiation and formation of the outer skin barrier. However, other barrier-related genes escaped prior detection because of difficulties obtaining adequate amounts of isolated terminally differentiated keratinocytes for transcriptome analysis.”
Haemoglobin binds gases such as oxygen, carbon dioxide, and nitric oxide, and it is an iron carrier via the heme complex. These properties make epidermal haemoglobin a prime candidate for antioxidant activity and potentially other roles in barrier function.
Professor Amagai continues: “We conducted a comparative transcriptome analysis of the whole and upper epidermis, both of which were enzymatically separated as cell sheets from human and mouse skin. We discovered that the genes responsible for producing haemoglobin were highly active in the upper part of the epidermis. To confirm our findings, we used immunostaining to visualise the presence of haemoglobin α protein in keratinocytes of the upper epidermis.”
Professor Amagai concludes: “Our study showed that epidermal haemoglobin was upregulated by oxidative stress and inhibited the production of reactive oxygen species in human keratinocyte cell cultures. Our findings suggest that haemoglobin α protects keratinocytes from oxidative stress derived from external or internal sources such as UV irradiation and impaired mitochondrial function, respectively. Therefore, the expression of haemoglobin by keratinocytes represents an endogenous defence mechanism against skin aging and skin cancer.”