Pretoria, 16 October 2024: A group of African women leaders have come together to form the Africa Breast Cancer Council, with the support of Roche, one of the world’s largest biotech companies.
The Africa Breast Cancer Council is a response to the growing burden of breast cancer on the African continent. Breast cancer is the most commonly diagnosed cancer in women in Africa and causes the most cancer-related deaths. Only one in two women in sub-Saharan Africa are currently expected to survive for five years after receiving a diagnosis.
The Council will leverage their extensive, diverse and complementary experience to guide and drive policy change in their home countries and across the continent. They will encourage increased collaboration, better data collection and improved patient outcomes. The Council’s work will seek to foster systemic improvements in healthcare infrastructure, access, and funding, driving sustainable, scalable impact for breast cancer care. The Council will focus initially on African healthcare systems which are open to partnership and innovation, then move to scale this work across the continent.
Wendy Cupido, Africa Breast Cancer Council Co-chair and General Manager at Roche South Africa and Sub Region said: “Every woman on this Council has a day job that plays an important role in the fight against breast cancer. Our aim in coming together is to channel our knowledge, expertise, relationships and energy into a collective voice, and a collective force, to focus on significant areas of concern.”
Dr Magda Robalo, Africa Breast Cancer Council member, and President and Co-founder of the Institute for Global Health and Development said: “Most African women with breast cancer are diagnosed too late and, even after a diagnosis, many do not receive the treatment they need. This egregious injustice is utterly preventable. In response, the Africa Breast Cancer Council will work to shape policies and advocate for governments to urgently commit the resources needed.”
It can take more than six months for women in Africa to receive a breast cancer diagnosis after noticing symptoms, due in part to healthcare system inefficiencies and limited access to specialised care. This contributes to 60-70% of African women receiving a diagnosis in the late stage, reducing chances of survival and increasing cancer care costs with more expensive therapies and longer hospital stays. This is exacerbated by a lack of awareness of the importance of breast self-examinations, along with widespread stigma surrounding breast cancer treatment. In light of this need, the Council will work at a national level to reduce the time to diagnosis from six months to 60 days.
In South Africa, the average three-year survival rate for breast cancer is below 45%. This is due in part to poor uptake of early screening and detection for breast cancer, exacerbated by significant stigma, leading to late-stage diagnosis and lower survival rates. Lengthy regulatory pathways and a lack of ring-fenced budget for cancer care also present barriers to progress.
Dr Miriam Mutebi, Africa Breast Cancer Council member and Breast Cancer Surgical Oncologist said: “This Council has chosen to launch during Breast Cancer Awareness Month, a recognised annual global movement to drive awareness, early detection and improved outcomes. We are using this month to start raising our collective voice, alongside others committed to reducing the unacceptable toll of breast cancer on African women.”
I was diagnosed with breast cancer on an ordinary Thursday afternoon in February 2023. I was 34 years old. The December before, my GP had performed a breast exam as part of a general check-up and was concerned that with my dense breast tissue she might be missing something. She wanted me to have an ultrasound, but there was no rush. Her exact words to me were something like: “Don’t worry, it can wait until you have medical aid savings again in January.”
The ultrasound turned up a small shadow, just a centimetre in diameter – something that could be a cyst, but the radiologist thought we should do a mammogram “just in case”. Would I mind waiting? No, I wouldn’t mind. The mammogram was worrying enough that she got approval to do a biopsy the next day. “Just in case”. The results came in the following week.
I had none of the risk factors for breast cancer. I didn’t drink, didn’t smoke, didn’t have any family members with a history of breast cancer, was nowhere near the age of 50. A few months later, I would find out I had none of the genetic markers which can predict risk either – not only did I test negative for the genes associated with breast cancer called BRCA 1 and 2, I didn’t have any of the genes connected with any kind of cancer at all.
As I say, I was diagnosed on a Thursday afternoon. I had my first appointment with an oncologist that Friday morning. I had my first set of scans two days later on Monday and my initial surgery the following Friday. I started chemotherapy treatment within three weeks of first having the word “cancer” used in relation to my body. My doctors moved quickly because they had to. On a scale of 1 to 9 on something called the Bloom and Richardson classification, my cancer was a 9. So, even though I was only stage 1, I was also a grade 3. “Aggressive” doesn’t begin to cover it.
During this time, I held onto five facts. First, we had caught the tumour at exactly the right time. Had I gone in for screening any earlier, we might not have found the cancer yet. Had I gone any later, it likely would have grown and spread to my lymph nodes and other parts of my body and I might have needed more radical treatment and surgeries. Second, it was treatable. My particular kind of cancer ought to respond well to a combination of chemotherapy and radiation. Third, I was otherwise very healthy, aside from the cancer. Fourth, I had a medical aid which was covering almost everything I needed. And, most importantly, fifth, I had a wonderful support system of my partner and his family and our close friends to rely on.
From the beginning, I had an incredible standard of care. To the point where the doctors I saw had heated examination beds – they didn’t want their patients to experience any additional discomfort and distress during such a difficult time. And it was difficult. Chemotherapy and immunotherapy left me feeling battered and broken. Nausea, intense muscular pain, fatigue, vomiting, diarrhoea, constipation, weight gain, hair loss, brain fog, depression – some of the awful side effects it’s impossible to really prepare for. In fact, I had such a hard time mentally during treatment that at one point I had to be hospitalised.
The same day I received my diagnosis, I overheard a woman in my doctor’s office asking if it was possible to make a payment plan for her treatment. The administrators replied that treatment was likely to cost in excess of R300 000 at a minimum. I cannot even begin to imagine having to go into debt to fight off cancer. For treatment that makes you feel more than just sick, more like you’re dying. For treatment that may not necessarily work.
But this is the choice that faces most people with cancer in our country. With a relatively small number of people on comprehensive medical aids with screening benefits and prescribed minimum benefits, many face waiting for treatment in government facilities or running up huge bills at private clinics.
According to the most recent report by Statistics SA, breast cancer is the most commonly diagnosed cancer in women in South Africa, accounting for 23% of all cancers. It is also one of the most deadly, representing 17% of cancer deaths in women, just behind cervical cancer.
The Stats SA report lists “awareness of the symptoms and need for screening” as the main intervention to reduce the risk of death by breast cancer. The report also draws attention to the discrepancy in mortality rates in different population groups. For example, Coloured women have a relatively low incidence of breast cancer, but a high mortality rate – meaning that they are dying of breast cancer after being diagnosed too late. Stats SA points out that this is likely due to “poor access to cancer treatment facilities” as well as a lack of medical aid coverage. It is perhaps unsurprising that Black and Coloured women are the groups least likely to have medical aid in South Africa.
There are also some NGOs trying to step in to fill the gaps, like the aptly named I Love Boobies or the PinkDrive. These organisations make it their mission to give women a fighting chance to beat breast cancer. They provide free screenings to women around the country who would otherwise not be able to afford this necessary medical care.
I am one of the lucky ones. I officially went into remission on 30 August 2023 when I had a lumpectomy to remove the tumour in my right breast. Remission means that the cancer can no longer be detected in your body through scans and blood tests. It doesn’t mean you’re “cured”. There could still be cancerous cells in the body, which is why cancer is also often treated with radiation like mine was. Some people prefer not to use the term “survivor” until they have been in remission for over five years.
Five years is an important milestone for many people diagnosed with cancer. It’s often the period in which someone is most likely to suffer a relapse. I live with the possibility that my cancer will come back every day; I am reminded by my scars and by the fact that I am still recovering physically and mentally from a traumatic year. I still battle with periods of fatigue and depression and I will never be the same person I was before falling ill.
Still, remission is better than relapse. So far, so good. I continue to see my myriad of doctors every few months for scans and tests and examinations to check that nothing has come back yet and I feel like I’m getting stronger.
Almost a year to the day after I went into remission, my fiancé and I ran the Johannesburg Women’s Race in support of the PinkDrive. A mobile health unit was parked on the field in Mark’s Park offering free screenings all morning, which women were queuing up to access after the run. The festive atmosphere was bittersweet to me. Certainly, some of the women in that line would not know that they were starting on a long and painful journey, a journey which sometimes feels like it has no end. Hopefully, they would be starting early enough to be given a chance to become a survivor.
There’s another meaning of “remission” I wasn’t aware of until I looked it up. It can also be defined as “a cancellation of debt”. No-one with cancer should have to crowdfund in order to get treatment, but that is the reality we are faced with in our country. This October, I encourage everyone to contribute in whatever way they can to a cancer survivor’s remission. Join the Imagine Challenge, try a secret swim, pick up a pink bottle of milk or a scrunchie, support someone raising funds on GivenGain, get yourself examined. Every one of us can join the fight against breast cancer.
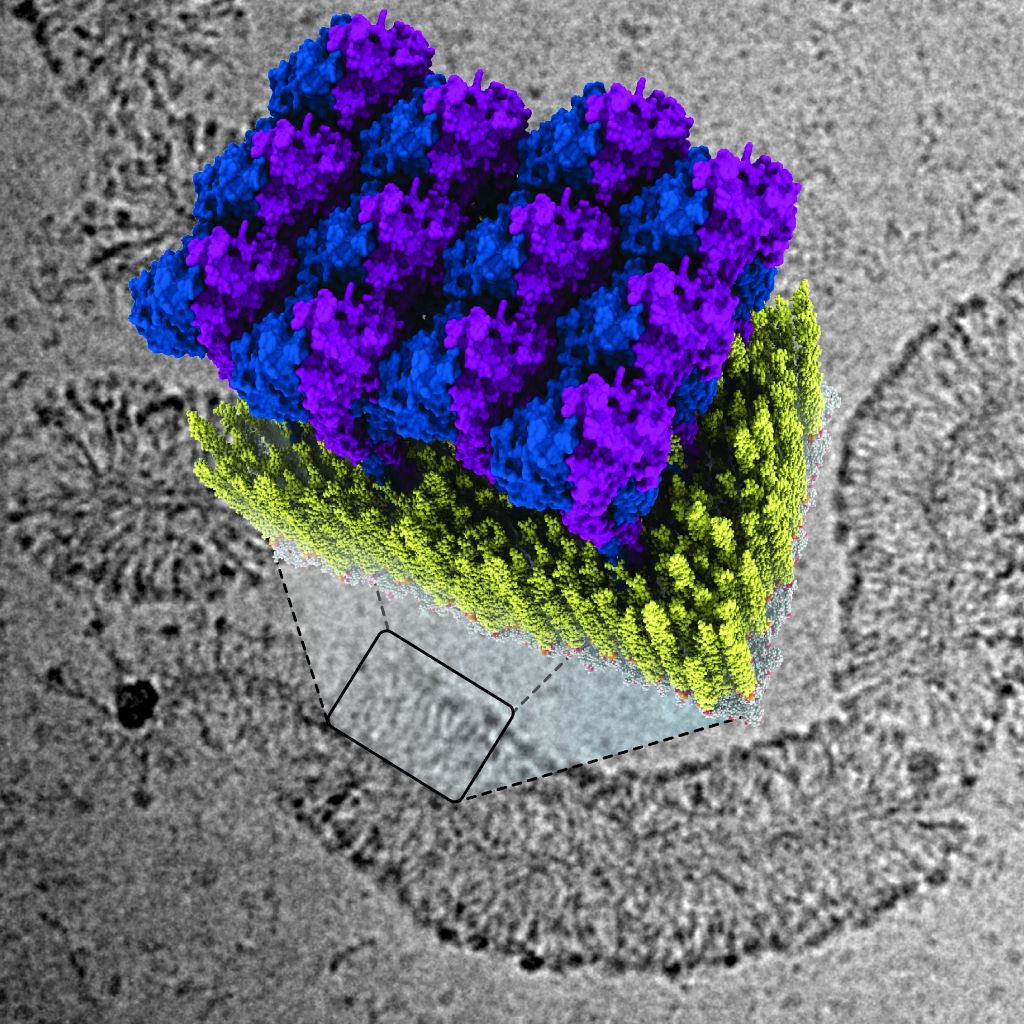
Illustration of how GBP1 proteins (blue and purple) attach to the membrane of a bacterium (yellow), zoomed in from an image taken with an electron microscope (in grayscale). Credit: Delft University
The protein GBP1 is a vital immune system component which fights against bacteria and parasites by enveloping them in a protein coat, but how the substance manages to do this has remained unknown until now. Researchers from Delft University of Technology report in Nature Structural & Molecular Biology how this protein operates – ripping and tearing until the bacterial membrane is undone. Their findings could aid in the development of medications and therapies for individuals with weakened immune systems.
So-called Guanylate Binding Proteins (GBPs) play a crucial role in our innate immune system, explains biophysicist Arjen Jakobi: “GBPs form the first line of defence against various infectious diseases caused by bacteria and parasites. Examples of such diseases include dysentery, typhoid fever caused by Salmonella bacteria, and tuberculosis. The protein also plays a significant role in the sexually transmitted infection chlamydia as well as in toxoplasmosis, which is particularly dangerous during pregnancy and for unborn children.”
Coat around bacteria
In their publication, Jakobi and his colleagues describe for the first time how the innate immune system fights against bacteria using GBP1 proteins. “The protein surrounds bacteria by forming a sort of coat around them,” explains Tanja Kuhm, PhD candidate in Jakobi’s research group and the lead author of the article. “By pulling this coat tighter, it breaks the membrane of the bacteria – the protective layer surrounding the intruder – after which immune cells can clear the infection.”
Deciphering the defence strategy
To decode the defence strategy of GBPs, the researchers examined how GBP1 proteins bind to bacterial membranes using a cryogenic electron microscope. This allowed them to see the process in great detail down to the molecular level. Jakobi: “We were able to obtain a detailed three-dimensional image of how the protein coat forms. Together with biophysical experiments conducted in Sander Tans’ research group at research institute AMOLF, which enabled us to manipulate the system precisely, we succeeded in deciphering the mechanism of the antibacterial function.”
Medications
According to Jakobi, this research helps us understand better how our body is capable of combating bacterial infections. “If we can grasp this well, and we can specifically activate or deactivate the involved proteins through medication, it may offer opportunities to speed up getting rid of certain infections.”
Credit: Darryl Leja National Human Genome Research Institute National Institutes Of Health
A blood test, performed when metastatic prostate cancer is first diagnosed, can predict which patients are likely to respond to treatment and survive the longest. It can help providers decide which patients should receive standard treatment versus who might stand to benefit from riskier, more aggressive new drug trials. The research, which forms part of a Phase III clinical trial, was just published in JAMA Network Open.
Once prostate cancer has metastasised and is no longer curable, systemic treatments are used to prolong survival as much as possible. Biomarkers that predict how patients will respond could allow for better personalisation of treatments, but they are few and far between.
A new study found that measuring circulating tumour cells (CTCs), rare cancer cells shed from tumours into the blood, is a reliable way to predict later treatment response and survival prospects. CTCs have been studied in prostate cancer before, but only in its later stages.
“No one, until now, has looked at whether CTC counts can be used right at the beginning, when a man first presents with metastatic prostate cancer, to tell us whether he’s going to live a long or short time, or whether or not he will progress with therapies,” said Amir Goldkorn, MD, lead author of the study and associate director of translational sciences at the USC Norris Comprehensive Cancer Center at the Keck School of Medicine of USC.
The research leveraged CellSearch (Menarini, Inc.), an FDA-cleared liquid biopsy technology at the Norris Comprehensive Cancer Center, to detect and measure CTCs in blood samples. Patients with more CTCs had shorter median survival lengths and a greater risk of death during the study period. Those with more CTCs also had less “progression-free survival,” which refers to the length of time when a patient’s disease is controlled by treatment without getting worse.
“You couldn’t tell these men apart when they walked through the door,” said Goldkorn, who is also a professor of medicine at the Keck School of Medicine. “All of their other variables and prognostic factors were seemingly the same, and yet they had very, very different outcomes over time.”
The researchers say that the CellSearch blood test, which is already widely available from commercial providers, can help quickly identify patients who are unlikely to respond to standard treatment options. Those men could benefit from a more intensive approach to therapy, including clinical trials of new drugs that may have more side effects but could improve survival in these high-risk patients.
Counting CTCs
The research was part of a phase 3 clinical trial of the NCI-funded SWOG Cancer Research Network, a group of more than 1300 institutions around the country that collaborate to study various cancers. Baseline blood samples from 503 patients with metastatic prostate cancer, who were participating in a new drug trial, were sent to the Keck School of Medicine team for analysis.
To analyze the blood samples, the researchers used the CellSearch platform at the Norris Comprehensive Cancer Center’s Liquid Biopsy Research Core, a facility that Goldkorn founded and directs. CellSearch uses immunomagnetic beads, antibodies attached to small magnetic particles, which bind to CTCs in the blood and pull them out to be detected and counted by specialised equipment.
Patients with five or more CTCs in their blood sample had the worst outcomes. Compared to patients with zero CTCs, they were 3.22 times as likely to die during the study period and 2.46 times as likely to have their cancer progress. They were only 0.26 times as likely to achieve a complete prostate-specific antigen (PSA) response, meaning they responded poorly to treatment.
Men with five or more CTCs had a median survival length of 27.9 months following the blood test, compared to 56.2 months for men with one to four CTCs and at least 78 months for men with zero CTCs. (Many patients in the latter group survived past the date of publication, so the median survival length could not yet be calculated.)
The bottom line: more CTCs meant that patients survived for less time, progressed much more quickly and were unlikely to respond to standard treatments.
Candidates for clinical trials
The new study shows that measuring CTC counts at the start of therapy can predict long-term survival rates, even in men who go on to receive many treatments for metastatic prostate cancer over a years-long period. That means the test can help identify men early on for trials of new and potentially more aggressive therapies.
“We want to enrich these clinical trials with men who need all that extra help – who really would benefit from three drugs versus just two, or from being on a new chemotherapy drug, even though it may have more side effects,” Goldkorn said.
Goldkorn and his team are now testing a new blood test that measures not just CTC counts, but also the molecular composition of CTCs and tumour DNA circulating in the blood, as well as other factors. Their goal is to create biomarkers with even more predictive power, which may ultimately help match patients with specific treatment options.