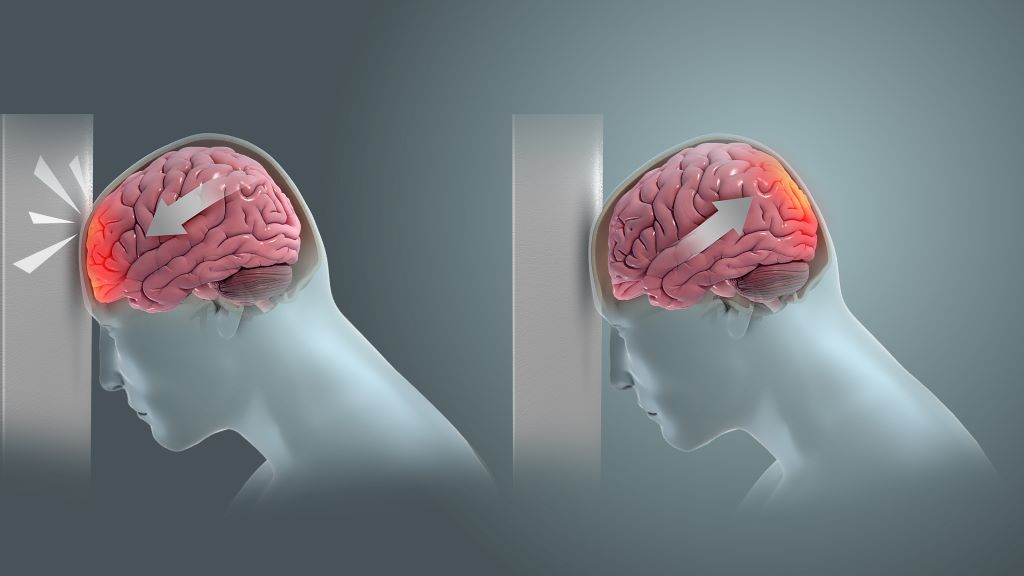
Coup and contrecoup brain injury. Credit: Scientific Animations CC4.0
Birmingham scientists have shown light therapy delivered transcranially can aid tissue repair after mild traumatic brain injury (mTBI). Their research, published in Bioengineering & Translational Medicine, indicates that this novel method could result in a new treatment option in an area of medicine that currently has few, if any, treatment options.
Traumatic brain injury (mTBI) results when the initial trauma of head injury is magnified by a complex set of inflammatory changes that occur in the brain. These secondary processes, which take place from minutes to hours after head injury, can dramatically worsen outcomes for patients.
The method invented by scientists at the University of Birmingham, UK and patented by University of Birmingham Enterprise aims to protect against this secondary damage, and stimulate faster, and better recovery for patients.
We want to develop this method into a medical device that can be used to enhance recovery for patients with traumatic brain or spinal cord injury, with the aim of improving outcomes for patients.
Professor Zubair Ahmed, College of Medicine & Health
In the study, the Birmingham team, comprising researchers Professor Zubair Ahmed, Professor Will Palin, Dr Mohammed Hadis and surgeons Mr Andrew Stevens and Mr David Davies, examined the effect of two wavelengths of near infrared light (660nm and 810nm) on recovery following injury.
The study in preclinical models used daily two-minute bursts of infrared light, delivered by a laser, for three days post-injury.
The findings showed significant reductions in the activation of astrocytes and microglial cells, which are heavily implicated in the inflammatory processes in the brain that follow head trauma, and significant reductions in biochemical markers of apoptosis (cell death).
At four weeks, there were significant improvements in performance in functional tests involving balance and cognitive function. The red light therapy also accelerated recovery compared to controls, with superior outcomes for light with a wavelength of 810nm.
The study builds on research published earlier this year which showed near infrared light delivered directly to the site of spinal cord injury both improves survival of nerve cells and stimulates new nerve cell growth.
Professor Ahmed, who led the study, said: “We want to develop this method into a medical device that can be used to enhance recovery for patients with traumatic brain or spinal cord injury, with the aim of improving outcomes for patients.”
The researchers are seeking commercial partners to co-develop the device and take it to market.
Fluorescein angiography capable of assessing neural blood flow in chronic nerve compression neuropathy
Fluorescein-enhanced contrast imaging shows a rabbit’s normal sciatic nerve, left, and a damaged one. Credit: Osaka Metropolitan University
In the modern office, it’s a daily struggle against the onset of carpal tunnel syndrome. The worst case could mean needing surgery to alleviate compression of the nerves or to repair damaged nerves. Helping surgeons visually check the areas where neural blood flow has decreased due to chronic nerve compression can lead to improvements in diagnostic accuracy, severity assessments, and outcome predictions.
With this in mind, an Osaka Metropolitan University-led research team involving Graduate School of Medicine student Kosuke Saito and Associate Professor Mitsuhiro Okada investigated the use of fluorescein angiography, a method employed in neurosurgery and ophthalmology to highlight blood vessels, to visualise neural blood flow in chronic nerve compression neuropathies like carpal tunnel syndrome. The findings were published in Neurology International.
The team found that fluorescein angiography could detect a decrease in neural blood flow in rats and rabbits with chronic nerve compression neuropathy. The results also correlated with electrodiagnostic findings.
Then fluorescein angiography was used for human patients undergoing open carpal tunnel release surgery, and the data also correlated strongly with electrodiagnostic testing. The findings indicate that fluorescein angiography might possess high diagnostic capabilities to assess neural blood flow during surgery.
“In surgery for severe chronic nerve compression neuropathy, the surgeon’s experience plays a big role in judging whether the surgical range is appropriate or whether additional treatment is necessary,” graduate student Saito noted. “This research has shown that fluorescein angiography can visualise impaired areas and assess the impairment severity, so we believe that it has the potential to contribute to improving accuracy for related surgeries.”
For the first time, researchers have linked specific frequent defects in sperm to risk of pregnancy complications and negative impacts on the health of the baby. The study from Lund University in Sweden shows that a high proportion of father’s spermatozoa possessing DNA strand breaks is associated with a doubled risk of preeclampsia in women who have become pregnant by IVF. It also increases the risk of the baby being born prematurely.
Infertility is a growing problem and the number of in vitro fertilisation procedures is increasing rapidly. It is already known that women who become pregnant by assisted reproduction techniques have an increased risk of preeclampsia, repeated miscarriages and the baby being born prematurely and with a lower birth weight. Yet, the reasons behind this have not been fully understood.
“Before a planned in vitro fertilisation, the man’s sperm sample is analysed for concentration, motility and morphology. But there are men who, according to this analysis, have normal sperm, but still have reduced fertility,” says Amelie Stenqvist, lecturer at Lund University and first author of the study published in Fertility and Sterility. She received her PhD from Lund and now works as a specialist in gynaecology and obstetrics at Skåne University Hospital in Malmö.
Around 20-30% of babies born through IVF have fathers with damaged DNA in their sperm, as shown by elevated levels of DNA fragmentation. The DNA fragmentation index (DFI) is a measure of the amount of strand breaks in the DNA and is used to provide important new information about male fertility. Sperm with DNA damage may still be fertile, but the chances of fertilisation are lower and if the percentage of DFI exceeds 30%, the chances of natural conception are close to zero.
Although current in vitro techniques mean that men with a high DFI can become fathers, until now very little has been known about the impact of DNA fragmentation on pregnancy and the health of the baby. It has been difficult to research the topic because the DFI value is not included in the standard measurements currently taken by Sweden’s fertility clinics. It also requires a large study population and access to national medical registries.
“Since half of the placenta’s DNA comes from the father and placental development and function play a central role in preeclampsia, we wanted to investigate whether a high percentage of DNA damage in the sperm affected the risk of preeclampsia,” says Aleksander Giwercman.
He is a professor of reproductive medicine at Lund University, a consultant at Skåne University Hospital in Malmö. Aleksander Giwercman also led a research study that included 1660 children conceived through IVF and ICSI at the Reproductive Medicine Centre in Malmö over the period 2007-2018.
The results showed that in the 841 couples who underwent IVF, a DFI of over 20% doubled the risk of the woman developing preeclampsia (10.5%) and also increased the risk of premature birth. In the IVF group with a DFI below 20%, there was a 4.8% risk of preeclampsia, which is comparable to pregnancies that occur naturally. For couples undergoing ICSI, there was no association with preeclampsia.
“Today, DFI analysis is only performed at some fertility clinics in Sweden, but we think that it should be introduced as standard at all clinics. It can give couples answers as to why they are not getting pregnant and can influence the chosen method of assisted fertilisation. Not only that, our latest results show that a DFI analysis could be used to identify high-risk pregnancies,” says Aleksander Giwercman.
What makes this finding even more interesting is that high DNA fragmentation in sperm is linked to the overall health of the father and is potentially treatable. Most DNA damage is caused by oxidative stress, which is an imbalance between harmful molecules and the antioxidants that protect cells. Other factors that increase DNA fragmentation include the man’s age, smoking, obesity and infections.
“The next step is to identify which group of men respond best to methods to prevent and treat sperm DNA damage, and to test these methods to prevent pregnancy complications,” concludes Amelie Stenqvist.
South Africa’s medical schemes industry is taking a strong, zero-tolerance stance against fraud, waste, and abuse – practices that are undermining the healthcare system. Fraudulent claims, unnecessary procedures, and mismanagement of resources are costing billions of rand, inflating healthcare costs, and putting additional financial strain on members. Instead of supporting essential treatments and care, these resources are being misused and misallocated, writes Dr Katlego Mothudi, Managing Director at the Board of Healthcare Funders (BHF).
At the recent BHF Healthcare Collab Hub, industry leaders highlighted the need for immediate reforms to curb these harmful practices and safeguard the future of medical schemes. As healthcare costs continue to rise, tackling fraud (deliberate deception), waste (inefficient use of resources), and abuse (excessive or improper use of services) is essential for ensuring that medical schemes remain affordable and sustainable. Without swift action, members may face higher premiums, with fewer resources available for the critical care they depend on.
Fraud, waste, and abuse (FWA) in the healthcare sector is not just a regulatory issue or an administrative headache, but a direct assault on the wellbeing of medical scheme members. Every fraudulent claim, and every misuse of resources, drains the pool of funds that are meant to ensure that individuals have access to necessary healthcare services. For millions of members, the repercussions of unchecked FWA include increased premiums, reduced benefits, and the potential for schemes to become financially unsustainable. It is a burden borne by all members, regardless of whether they have directly engaged with healthcare services or not.
The healthcare industry, specifically medical schemes and their administrators, has a significant responsibility to address this problem head-on. Their duty extends beyond managing funds – they are custodians of a system designed to protect individuals’ access to essential healthcare services.
If these schemes fail to adequately combat FWA, the entire medical scheme ecosystem becomes compromised, undermining trust in healthcare funding and leaving members exposed to higher costs and decreased quality of care.
The ripple effect of FWA
The scale of FWA in the medical schemes sector is staggering. According to industry reports, billions of rands are lost annually to fraudulent activities. Whether through inflated billing, unnecessary procedures, or outright false claims, these actions take funds directly from the pockets of members. Medical schemes are forced to increase premiums to cover these losses, meaning that honest, hardworking individuals are paying more for their healthcare – not because of rising medical costs, but because of the unethical behaviour of a few.
Moreover, the administrative costs associated with managing and investigating FWA claims are significant. These costs divert funds that could otherwise be used to enhance member benefits or improve healthcare services.
The long-term impact is even more worrying. If left unchecked, FWA can destabilise the entire medical scheme system. Ultimately, it is the members who suffer the most, facing financial uncertainty and diminished healthcare support when they need it most.
What the industry can do: Curbing FWA
The healthcare industry has both the tools and the responsibility to take decisive action against FWA. Key stakeholders, including medical schemes, administrators, and regulatory bodies, must collaborate to develop comprehensive strategies that can curtail the losses associated with these unethical practices. Here are some key strategies:
1. Enhanced use of technology and data analytics
The industry is already moving towards the use of automated systems and data analytics to detect unusual patterns and potential fraud. However, the systems need continuous improvement to keep up with the evolving tactics of fraudsters. Schemes should invest in advanced algorithms and artificial intelligence (AI) tools that can analyse claims in real-time, flagging high-risk transactions before they are paid. Machine learning models, for instance, could identify patterns that suggest fraudulent behaviour, such as repeated claims for the same procedure or suspiciously high billing from certain providers.
This not only helps in early detection but also ensures that members who follow the rules aren’t unfairly penalised. It is essential, however, that these systems remain transparent to avoid unintended biases or discriminatory practices.
2. Collaboration across the healthcare ecosystem
The fight against FWA cannot be won by medical schemes alone. There needs to be greater collaboration between schemes, healthcare providers, and regulatory bodies. Sharing data across schemes and industries can help to identify serial offenders who hop between schemes, committing fraud on a wide scale.
Additionally, healthcare providers themselves play a critical role. They should be incentivised to report fraudulent activities or billing irregularities they observe within their network. Schemes can establish anonymous reporting systems and offer rewards for whistleblowers who help to uncover fraud. By creating a network of accountability, the industry can make it more difficult for fraudsters to operate with impunity.
3. Member education and engagement
Members are the first line of defence against fraud. If they are empowered with the right information, they can help to identify fraudulent or abusive practices. Medical schemes should launch educational campaigns that inform members about how to scrutinise their healthcare bills and understand their benefits better.
Simple actions such as checking that all billed procedures were performed or verifying service dates can catch many fraudulent claims early. Members who understand the importance of vigilance are less likely to be unwittingly complicit in fraud and can help schemes prevent abuse of the system.
4. Improved consequent management
Strong consequent management is one sure way of deterring this fraudulent behaviour. The Health Professions Council should impose appropriate penalties on healthcare professionals found guilty. Schemes should not hesitate to take legal action against individuals or providers who commit fraud.
Stronger penalties, including prison sentences and significant fines, can serve as a deterrent.
Moreover, schemes must ensure that once a provider or member has been found guilty of fraud, they are blacklisted across all schemes. Allowing repeat offenders to continue exploiting the system is a failure that impacts all members.
At the heart of any medical scheme is the promise to its members that they will be provided with financial protection when they need healthcare. Fraud, waste, and abuse erode this promise, making it harder for schemes to deliver on their commitments. To safeguard the integrity of the system and ensure that members receive the care they deserve, the healthcare industry must step up its efforts to curb these damaging practices.
By embracing technology, fostering collaboration, educating members, and enforcing strict penalties, the industry can make significant strides in reducing FWA. In doing so, they will not only protect their financial stability but also uphold the trust and confidence that members place in them. This, above all, is the most important goal.
Findings suggest significant increase in emergency department utilisation for hypertensive disorders of pregnancy over 14 year span
Photo by Camilo Jimenez on Unsplash
Hypertensive disorders of pregnancy, the second leading cause of maternal deaths worldwide, may be sending a significantly higher number of pregnant people to the emergency department. Between 2006 and 2020, researchers found a surge in emergency visits and admissions for the condition that causes serious maternal and neonatal complications and accounts for 6.3% of all pregnancy-related deaths in the United States.
The study, which appears in JAMA Network Open, also suggests greater emergency utilisation for the disease among underrepresented racial and ethnic groups.
“Hypertensive disorders of pregnancy often develop suddenly, even in healthy women, and symptoms may appear without warning and progress rapidly,” said senior author Erica Marsh, MD, professor of obstetrics and gynaecology at the University of Michigan Medical School and chief of the division of reproductive endocrinology and infertility at U-M Health Von Voigtlander Women’s Hospital, of Michigan Medicine.
“Ideally, this risk would be detected during prenatal care and lead to early intervention. Our study indicates more people turning to the emergency department, which may reflect a higher prevalence of the condition or an increased awareness for prompt assessment and treatment.”
Hypertensive disorders of pregnancy, which could include preeclampsia, gestational hypertension, and eclampsia, are serious complications that involve elevated blood pressure.
The American College of Obstetricians and Gynecologists recommends management of severe blood pressure in pregnancy within 30 to 60 minutes of diagnosis to prevent complications such as stroke, myocardial ischaemia, seizure, placental abruption, and maternal and neonatal mortality.
Disparities in ED reliance, disease severity
Researchers analysed nationally representative data, finding a 76% increase in emergency encounters related to the condition over the 14-year span, up from 31 623 to 55 893, and nearly 1.5 times as many ED admissions – up from 17 338 to 43 563.
Concerns about costs, time constraints, misconceptions about the necessity of early care or barriers to accessing prenatal care may be possible factors for the increase, authors say.
“The disparities in reliance on emergency rooms for this disease may imply limited access to timely outpatient care or other health system barriers,” said lead author Courtney Townsel, MD, MSc, who was at Michigan Medicine at the time of the study and is now at the University of Maryland.
Black, Hispanic, and Asian or Pacific Islander groups were also more likely to both utilise emergency care and be admitted to the hospital for hypertensive disorders of pregnancy.
“The disproportionate rate of admissions among certain racial and ethnic groups suggests worse disease severity by the time people seek care,” Townsel said.
“Racial differences in emergency care utilisation for hypertensive disorders of pregnancy underscore the ongoing racial disparities in US maternal morbidity and mortality and highlight a critical need for accessible, culturally competent community-level interventions for all.”