A novel tool for rapidly identifying the genetic “fingerprints” of cancer cells may enable future surgeons to more accurately remove brain tumours while a patient is in the operating room, new research reveals. Many cancer types can be identified by certain mutations, changes in the instructions encoded in the DNA of the abnormal cells.
Led by a research team from NYU Langone Health, the new study describes the development of Ultra-Rapid droplet digital PCR, or UR-ddPCR, which the team found can measure the level of tumour cells in a tissue sample in only 15 minutes while also being able to detect small numbers of cancer cells (as few as five cells/mm2).
The researchers say their tool is fast and accurate enough, at least in initial tests on brain tissue samples, to become the first practical tool of its kind for detecting cancer cells directly using mutations in real time during brain surgery.
The researchers showed that UR-ddPCR had markedly faster processing speed than standard droplet digital polymerase chain reaction (ddPCR). Standard ddPCR can accurately quantify tumor cells, but it typically takes several hours to produce a result, making it impractical as a surgical guide.
“For many cancers, such as tumors in the brain, the success of cancer surgery and preventing the cancer’s return is predicated on removing as much of the tumor and surrounding cancer cells as is safely possible,” said study co-senior study investigator and neurosurgeon Daniel A. Orringer, MD.
“With Ultra-Rapid droplet digital PCR, surgeons may now be able to determine what cells are cancerous and how many of these cancer cells are present in any particular tissue region at a level of accuracy that has never before been possible,” said Dr Orringer.
Published in the journal Med, the study showed that UR-ddPCR produced the same results as standard ddPCR and genetic sequencing in more than 75 tissue samples from 22 patients at NYU Langone undergoing surgery to remove glioma tumours. Results from UR-ddPCR were also checked against known samples with cancer cells and samples without any cancer.
“Our study shows that Ultra-Rapid droplet digital PCR could be a fast and efficient tool for making a molecular diagnosis during surgery for brain cancer, and it has potential to also be used for cancers outside the brain,” said senior study investigator Gilad Evrony, MD, PhD.
To develop UR-ddPCR, researchers looked for efficiencies in each of the steps involved in standard ddPCR. The team shortened the time needed to extract DNA from tumour samples from 30 minutes to less than 5 minutes in a manner that is still compatible with subsequent ddPCR. The researchers also found efficiencies by increasing the concentrations of the chemicals used in testing, reducing the overall time needed for some steps from two hours to less than three minutes. Time savings were also achieved by using reaction vessels prewarmed to each of the two temperatures required by the PCR rather than repeatedly cycling the temperature of a single reaction vessel between two temperatures.
For the study, researchers used UR-ddPCR to measure the levels of two genetic mutations, IDH1 R132H and BRAF V600E, which are prevalent in brain cancers. They combined UR-ddPCR with another technique the researchers developed earlier, called stimulated Raman histology, to calculate both the fraction and the density of tumour cells within each tissue sample.
Researchers caution that widespread use of the tool awaits further refinements and clinical trials. They say their next step is to automate UR-ddPCR to make it faster and simpler to use in the operating room. Subsequent clinical trials will be necessary to compare patient outcomes using their tool compared to current diagnostic technologies. They also plan to develop the technology to identify other common genetic mutations for other cancer types.
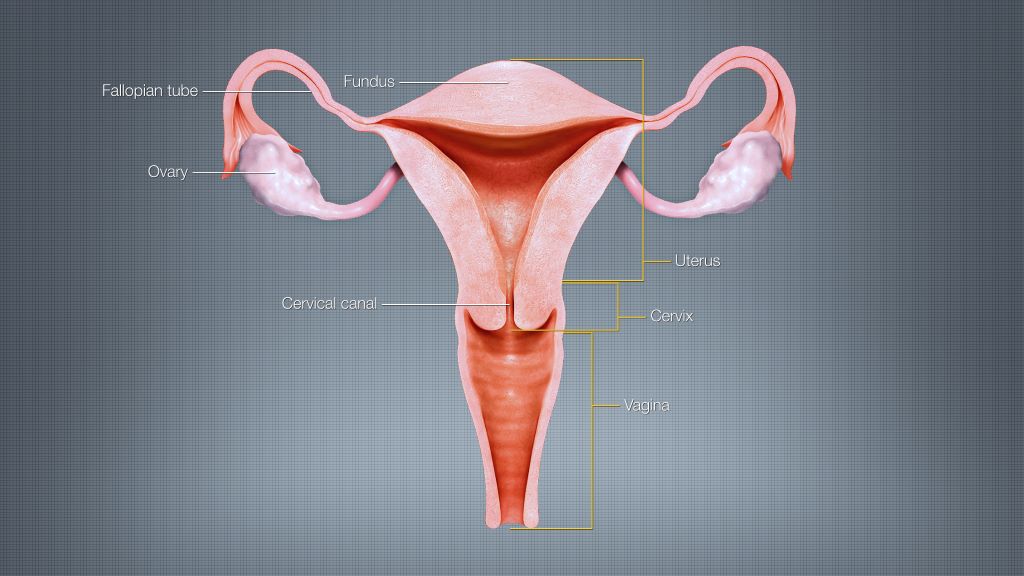
A mathematical modelling study conducted in Germany suggests that ovarian cancer incidence could be reduced and healthcare savings boosted if women who have already completed their families were offered fallopian tube removal during any other suitable abdominal surgeries. Angela Kather and Ingo Runnebaum of Jena University Hospital, Germany, and colleagues present these findings on January 30th in the open-access journal PLOS Medicine.
Some of the most widespread and serious forms of ovarian cancer begin in the fallopian tubes, and removing them may reduce ovarian cancer risk. While women at average risk of ovarian cancer are not recommended to have surgery solely to remove their fallopian tubes, many surgeons offer “opportunistic” tube removal during other gynaecologic surgeries such as hysterectomy or tubal sterilisation. Opportunistic removal may also be feasible during other abdominal surgeries, such as gallbladder removal.
However, the overall potential benefits of opportunistic fallopian tube removal have been unclear. To help clarify, Kather and colleagues developed a mathematical model that incorporates real-world patient statistics to predict population-level risks of ovarian cancer after opportunistic fallopian tube removal, as well as the potential healthcare cost savings.
By applying the model to statistics from Germany, the researchers predicted that opportunistic fallopian tube removal during every hysterectomy and tubal sterilisation could reduce ovarian cancer cases by 5% across the female population of Germany. Removal during every suitable abdominal surgery for women who are done having children could reduce nationwide cancer cases by 15%, the analysis suggests, and it could save more than €10 million in healthcare costs annually.
Ovarian cancer is the third most common gynaecologic cancer in the world and has a mortality rate of 66%. Overall, these findings suggest that opportunistic fallopian tube removal during appropriate abdominal surgeries could not only lower population-level ovarian cancer risks and prevent ovarian cancer deaths, but also provide economic benefits. This study could help inform health policy and insurance costs for the procedure.
The authors add, “We developed a mathematical model to estimate the likelihood of women undergoing surgeries that offer an opportunity for fallopian tube removal and the potential for reducing their ovarian cancer risk. Applying this model to the entire female population of Germany revealed that 15% of ovarian cancer cases could be prevented if fallopian tubes were removed during every suitable abdominal surgery in women who have completed their families. This approach has the potential to extend healthy years of life and significantly save healthcare costs.”
For people with an injured anterior cruciate ligament (ACL) in the knee, surgical ACL reconstruction (ACLR) is an effective treatment for restoring joint stability, however, many treated patients still develop additional long-term knee problems, such as knee osteoarthritis. New research published in the Journal of Orthopaedic Research reveals that individuals exhibit an altered gait after ACLR, which can contribute to these problems.
For the study, investigators compared gait biomechanics between the ACLR and uninjured limbs of 58 patients who underwent ACLR and 58 uninjured control individuals.
Although gait biomechanics became more symmetrical in patients with ACLR over the first 12 months post‐ACLR, the ACLR and uninvolved limbs demonstrated persistent aberrant gait biomechanics compared with the uninjured control individuals.
“A persistent aberrant gait pattern following ACLR, like that observed in our study, can induce joint loads that may contribute to further long-term knee joint problems,” said corresponding author Christin Büttner, MS, of the University of North Carolina at Chapel Hill. Implementing early rehabilitative measures to normalise gait following ACLR could help to maintain long-term knee joint health in both the injured and uninjured limb.”
Obesity and type 2 diabetes are risk factors for various malignancies, including pancreatic cancer, which has a high death rate. A new analysis in Diabetes/Metabolism Research and Reviews suggests that metabolic-bariatric surgery may lower the risk of developing pancreatic cancer in people with obesity, especially in those who also have type 2 diabetes.
In the systematic review and meta-analysis, investigators identified 12 relevant studies that explored the effects of metabolic-bariatric surgery on pancreatic cancer incidence, with a total of 3 711 243 adults with obesity. Surgery was associated with a 44% reduction in pancreatic cancer risk among individuals with obesity but without type 2 diabetes and a 79% risk reduction in those with both obesity and type 2 diabetes.
“Metabolic-bariatric surgery not only has beneficial effects on obesity and type 2 diabetes but also may play a crucial role in reducing the risk of pancreatic cancer in these individuals,” said corresponding author Angeliki M. Angelidi, PhD, of the Broad Institute of MIT and Harvard. “These findings underscore the need for further research to elucidate the underlying mechanisms and understand the full spectrum of health benefits of metabolic-bariatric surgery beyond weight loss.”
Fluorescein angiography capable of assessing neural blood flow in chronic nerve compression neuropathy
Fluorescein-enhanced contrast imaging shows a rabbit’s normal sciatic nerve, left, and a damaged one. Credit: Osaka Metropolitan University
In the modern office, it’s a daily struggle against the onset of carpal tunnel syndrome. The worst case could mean needing surgery to alleviate compression of the nerves or to repair damaged nerves. Helping surgeons visually check the areas where neural blood flow has decreased due to chronic nerve compression can lead to improvements in diagnostic accuracy, severity assessments, and outcome predictions.
With this in mind, an Osaka Metropolitan University-led research team involving Graduate School of Medicine student Kosuke Saito and Associate Professor Mitsuhiro Okada investigated the use of fluorescein angiography, a method employed in neurosurgery and ophthalmology to highlight blood vessels, to visualise neural blood flow in chronic nerve compression neuropathies like carpal tunnel syndrome. The findings were published in Neurology International.
The team found that fluorescein angiography could detect a decrease in neural blood flow in rats and rabbits with chronic nerve compression neuropathy. The results also correlated with electrodiagnostic findings.
Then fluorescein angiography was used for human patients undergoing open carpal tunnel release surgery, and the data also correlated strongly with electrodiagnostic testing. The findings indicate that fluorescein angiography might possess high diagnostic capabilities to assess neural blood flow during surgery.
“In surgery for severe chronic nerve compression neuropathy, the surgeon’s experience plays a big role in judging whether the surgical range is appropriate or whether additional treatment is necessary,” graduate student Saito noted. “This research has shown that fluorescein angiography can visualise impaired areas and assess the impairment severity, so we believe that it has the potential to contribute to improving accuracy for related surgeries.”
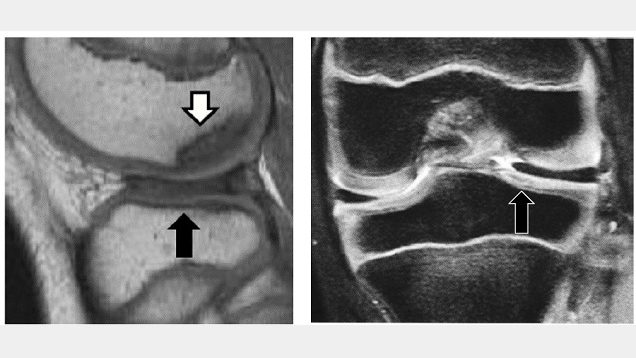
Discoid lateral meniscus and osteochondritis dissecans in adolescent patients. The black arrow represents DLM and the white arrow represents osteochondritis dissecans. Credit: Osaka Metropolitan University
Growing pains are common in maturing children, but sometimes this growth can be irregular and cause injury. Discoid lateral meniscus (DLM), a misshapen knee cartilage, is one such occurrence that can degenerate into osteochondritis dissecans, a joint disorder where the bone and joint begin to separate from the rest of the bones. It has been reported that osteochondritis dissecans of the femoral condyle occurs in approximately 14.5% of cases of DLM, but there has been little analysis of its treatment to date.
Dr Ken Iida and Specially Appointed Professor Yusuke Hashimoto’s team at Osaka Metropolitan University’s Graduate School of Medicine analysed the incidence of post-surgery osteochondritis dissecans. This analysis consisted of two groups, a pre-osteochondritis group with DLM and osteochondritis dissecans of the outer femoral epicondyle, and a non-osteochondritis dissecans DLM group. They studied 95 cases of DLM patients under the age of 15 who underwent surgery between 2003 and 2017 and had five years of post-surgery records. There were 15 cases in the pre-osteochondritis dissecans group and 80 non-osteochondritis dissecans cases.
Their analysis found that the surgical results for osteochondritis dissecans were good in pre-osteochondritis cases, but 28.5% had a recurrence of the joint disorder. In the non-osteochondritis dissecans group, 8.8% were diagnosed with the disorder after surgery. Additionally, age was found to be a risk factor for relapse or post-surgical osteochondritis dissecans, and surgery on patients ages 9 and under was also involved in the occurrence of osteochondritis dissecans.
“Patients with DLM accompanied by osteochondritis dissecans of the femoral condyle often have difficulty in deciding on a treatment method,” Dr Iida explained. “Based on the results of this study, we believe for patients ages 9 years or younger, it is necessary to consider conservative treatment methods rather than immediate surgery.”
A UCLA research team has created the Comorbid Operative Risk Evaluation (CORE) score to better account for the role chronic illness plays in patient’s risk of mortality after operation, allowing surgeons to adjust to patients’ pre-existing conditions and more easily determine mortality risk.
For almost 40 years, researchers have used two tools, the Charlson Comorbidity Index (CCI) and Elixhauser Comorbidity Index (ECI), to measure the impact of existing health conditions on patient outcomes. These tools use ICD codes that are input by medical professionals and billers to account for patient illness. These tools, however, were not designed for patients undergoing surgery and often address chronic illnesses that are not relevant to surgical populations. They often capture data from medical billing records and lack nuanced information regarding pre-existing health conditions.
A total of 699 155 patients were used to develop the model, of which 139 831 (20%) comprised the testing cohort. The researchers queried adults undergoing 62 operations across 14 specialties from the 2019 National Inpatient Sample (NIS) using International Classification of Diseases, 10th Revision (ICD-10) codes. They sorted ICD-10 codes for chronic diseases into Clinical Classifications Software Refined (CCSR) groups. They used logistic regression on CCSR with non-zero feature importance across four machine learning algorithms predicting in-hospital mortality, and used the resultant coefficients to calculate the Comorbid Operative Risk Evaluation (CORE) score based on previously validated methodology. The final score ranges from zero, representing lowest risk, to 100, which represents highest risk.
Impact
Health services and outcomes research using retrospective databases continues to represent a growing proportion of surgical research. Researchers highlighting quality issues and disparities are well-intentioned. However, without appropriate tools, it can be unclear if poor outcomes are independent of pre-existing conditions.
“The advent of novel statistical software and methodology have enabled researchers to exploit large databases to answer questions of healthcare quality, disparities, and outcomes,” said Dr Nikhil Chervu, a resident physician in the UCLA Department of Surgery and the study’s lead author. “These databases, however, often capture data from medical billing records and lack nuanced information regarding pre-existing health conditions. Without addressing differences in patients’ chronic illnesses, population comparisons may fall flat. Incorporation of this score in additional research will further validate its use and help improve analysis of surgical outcomes using large databases.”
A handful of common surgical procedures account for large shares of all opioids dispensed after surgery in children and adults, according to two studies recently published by researchers at the University of Michigan.
The studies, published this week in Pediatrics and JAMA Network Open, report that the top three procedures for children ages 0–11 account for 59% of opioids dispensed after surgery (tonsillectomies and adenoidectomies 50%, upper extremity fractures 5% and removal of deep implants 4%). Among those ages 12–21, the top three procedures account for about a third of post-surgery opioid prescriptions (tonsillectomies and adenoidectomies 13%, knee arthroscopies 13% and caesarean deliveries 8%).
For adults ages 18–44, C-sections account for the highest share of opioids dispensed post-surgery (19%), followed by hysterectomies (7%) and knee arthroscopies (6%). Among those ages 45-64, four of the top five procedures were orthopaedic procedures, collectively accounting for 27% of total opioid prescriptions dispensed after surgery.
“Our findings suggest that surgical opioid prescribing is highly concentrated among a small group of procedures. Efforts to ensure safe and appropriate surgical opioid prescribing should focus on these procedures,” said Kao-Ping Chua, lead author of the study in Pediatrics, assistant professor at the U-M Medical School and School of Public Health, and co-director of the Research and Data Domain at the U-M Opioid Research Institute.
To conduct the study, the researchers developed an algorithm to identify 1082 major surgical procedures using procedure codes, a medical classification tool used to identify specific surgical, medical or diagnostic interventions. The algorithm was then applied to identify privately and publicly insured children and adults undergoing surgery from Dec. 1, 2020 through Nov. 30, 2021.
The information was organized through a novel system developed by the study team, which allowed them to connect different sets of data that had previously been seen as unrelated. This new method allows for improved comparability and contrast, according to lead investigators.
In addition to determining which procedures accounted for the highest shares of opioids, the researchers also examined the size of opioid prescriptions for each procedure. For many procedures, prescriptions were far larger than the amount patients typically need for a particular procedure.
“Our findings suggest that there are important opportunities to reduce surgical opioid prescribing without compromising pain control,” said Dominic Alessio-Bilowus, lead author of the paper focused on adults published in JAMA Network Open and a medical student at Wayne State University who just completed a research year at U-M.
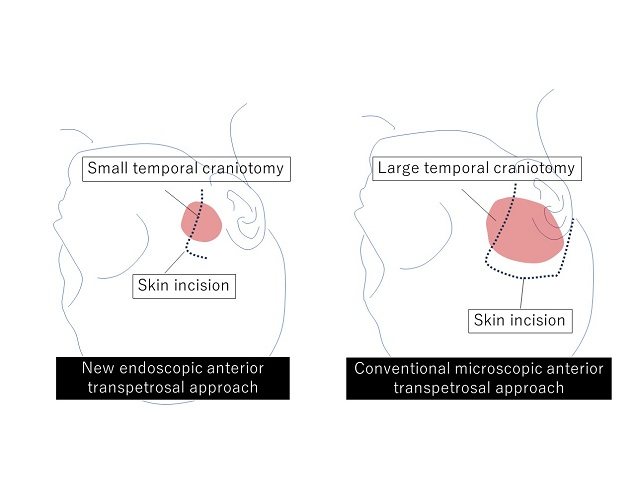
Tumours arising in the base of the skull are among the most difficult to remove in neurosurgery. The current treatment method is to perform surgical removal by what is known as the microscopic anterior transpetrosal approach (ATPA). Seeking to lessen the risk of damage and postoperative complications, as the skull base is densely packed with nerves, blood vessels, and other tissues, not to mention the brain stem, an Osaka Metropolitan University medical research team is taking a new approach.
Led by Dr Hiroki Morisako, a lecturer in the Graduate School of Medicine’s Department of Neurosurgery, and its department head Professor Takeo Goto, the team has developed a minimally invasive surgical technique called a purely endoscopic subtemporal keyhole ATPA. The team members write in The Journal of Neurosurgery that this is, to their knowledge, the first time this procedure to remove lesions in the skull base region known as the petrous apex has been described in an article.
Diagram of skin incision and extent of craniotomy. New endoscopic neurosurgery approach does not require a large craniotomy, so the result is a smaller scar. Credit: Osaka Metropolitan University
The endoscopic technique means a smaller area of the skull needs to be surgically opened compared to the microscopic approach, an average of only 11.2 cm² versus 33.9 cm². The risk of damage to the brain is also reduced.
The team performed 10 neurosurgeries using their method from 2022 to 2023 at Osaka Metropolitan University Hospital and compared the results to 13 surgeries using the microscopic ATPA from 2014 to 2021. In terms of operative time, the endoscopic approach reduced it noticeably, from an average of 410.9 minutes to 252.9 minutes. Similarly, blood loss lessened from a mean of 193 ml to 90 ml. The degree of tumour resection (surgical removal) was just as high as the microscopic method, while neurological functions were preserved at a rate equal to or higher than with the conventional approach.
“Comparison of the new endoscopic method and the conventional microscopic method showed no significant difference in tumour resection rate or in the ability to perform daily activities before and after surgery, with the new endoscopic approach resulting in shorter operative times and less blood loss,” Professor Goto stated. “The widespread use of this surgical procedure is expected to improve the treatment results of brain tumours in the base of the skull, not only in Japan but also worldwide.”
Dr Tim Forgan at the surgeon’s console of the da Vinci robotic system. (Photo: Biénne Huisman/Spotlight)
By Biénne Huisman
Within South Africa’s beleaguered public health sector – unsettled by budget cuts, understaffing, and divisive NHI legislation – cutting edge surgical robots that have been used to perform more than 600 surgeries at two Cape Town public hospitals are beacons of excellence that offer a glimmer of hope. Spotlight’s Biénne Huisman visited Dr Tim Forgan at Tygerberg Hospital to learn more.
Cutting edge robotic surgery might not immediately come to mind when one thinks of public hospitals, but in a first for public healthcare in South Africa, such systems are being used at two hospitals in the Western Cape.
The da Vinci Xi systems enable surgeons to control operations from a console – steering three arms with steel “hands” equipped with tiny surgical instruments; plus a fourth arm bearing a video camera (the laparoscope). The system translates a surgeon’s hand movements in real time, with enhanced precision, range and visuals, compared to manual surgery.
“It really is next level, it feels like you’re inside the patient,” says colorectal specialist Dr Tim Forgan, Tygerberg Hospital’s da Vinci robotics coordinator. “With this technology we can operate so much finer. You can see ten times better with this robot than with the naked eye; you can see tiny, tiny nerves you wouldn’t normally see. And you can manoeuvre surgical instruments so much better. Because of that, people have way better function after the procedure.”
He explains that the technology allows major surgery to be completed through small incisions – instead of larger cuts made by a doctor’s hand – leading to less bleeding and a faster recovery time.
Over 600 surgeries in two years
Lorraine Gys from Phillipstown in the Northern Cape can attest. On 22 February 2022, the 65-year-old pensioner became the first patient to undergo da Vinci robotic surgery in South Africa’s public sector. Forgan was behind the console, at Tygerberg Hospital.
Gys tells Spotlight: “The next day the sisters offered to wash me, I said to them ‘no, I’m not helpless.’ My recovery was very quick. I was up and about in no time, while the other patients had to be assisted. I was discharged on day four, and back at home I could even continue doing my own chores.”
Two years later, Gys is cancer free. The mother of three, who now lives in Eerste River, recalls how she made news headlines: “Before the operation, Dr Forgan explained everything to me. They asked my permission, saying that media will be there and the [provincial health] minister.”
Indeed, on the day Forgan operated on Gys, removing a cancerous rectal tumour, he was joined in theatre by several onlookers including former Western Cape MEC of Health and Wellness Nomafrench Mbombo.
“Yes it was a circus,” says Forgan, laughing. “A whole bunch of people watching me operate, quite bloody nerve-wracking. Fortunately I’m experienced at having lots of students around watching; plus performing surgery is just so immersive, everything else fades out.”
On that day, also in the operating room was colorectal surgeon Dr Roger Gerjy, keeping an eye. “He’s a very well-known robotic surgeon; a Swedish surgeon who works in Dubai,” says Forgan. “And if there was a problem, Roger would’ve taken over. He was also there to impart tips and tricks: move the instrument like this, shape it like a hockey stick; because with the robot it’s like having your whole arm inside [the body]. He’d give me advice on what to do with my extra floating arm – where to place it and how to manipulate it – because remember you’re controlling three arms at a time.”
Since 2022, the da Vinci robots installed at Cape Town’s two tertiary hospitals: Groote Schuur and Tygerberg, have enabled over 600 minimally invasive surgeries – including colorectal operations, prostatectomies, cystectomies (bladder removal surgery), and gynaecological procedures to treat endometriosis.
Groote Schuur Hospital has the other da Vinci Xi system run by Western Cape public healthcare
A spokesperson for the Western Cape Ministry of Health and Wellness, under former MEC Mbombo, Luke Albert explains: “We can see the immense impact it has for patients and the health system. For example, a traditional open cystectomy patient would require three days of ICU stay, as well as two weeks of hospital stay to recuperate. During this time, on average, 42% of patients require blood transfusions and almost 20% need total parenteral nutrition (when a patient is fed intravenously). A patient undergoing robotic surgery for a cystectomy requires no ICU stay and goes straight to a general ward for no more than six days on average, with no blood transfusions needed.”
Where the money came from
Asked how the department was able to afford R40 million per system for these machines in the context of severe budget cuts, Albert says: “The purchase was applicable to 2021/22 and not the current financial year; with all provincial health departments currently managing the effects of budget cuts.”
Asked the same question, Forgan explains the investment derived from surplus budget discovered within the throes of the COVID-19 pandemic: “There was a surplus because certain services just couldn’t be done. I mean, for us, we couldn’t do elective surgery. And how state funding works; if you don’t spend your [provincial] budget within the financial year, it goes back to central government.”
What it looks like
On a Friday afternoon at Tygerberg Hospital, Forgan is guiding Spotlight along corridors and up grey linoleum stairs, to the theatre where the da Vinci system is used. Dressed in black surgical scrubs bearing his name and a cap; on his feet Forgan is wearing bright pink crocs. In passing, he waves hello to fellow healthcare staff.
Inside the small blindingly white room, Forgan points out the three core components of the da Vinci system. There is a console with two control levers similar to refined joysticks – he demonstrates how to delicately hold them between forefingers and thumbs – a patient-side cart with four interactive metal arms (they are disposable; each arm can be used on twelve patients), and another trolley with a television screen. All connected by blue fibre optic cables.
As we speak, nurses arrive in the theatre, preparing it for upcoming gynaecology procedures scheduled for Monday. Forgan greets them, then continues to expand on his passion for colorectal surgery.
“With colorectal surgery, there’s a high rate of complications, but I really enjoy it, I really enjoy my job. When you have a successful outcome, saving a person from their cancer and prolonging their life through your intervention, that is the reward. Colorectal cancer is a very unpleasant disease, and operating like this can make one hell of a difference in a patient’s life.”
Colorectal cancer on the increase
Forgan adds that colorectal cancer is on the increase: “There aren’t many colorectal surgeons in South Africa, with a dire need for people to operate in this subspecialty. I mean, there are so few of us, we’re all on a WhatsApp group.”
Colorectal or colon cancer is the second most common cancer in South African men (following prostate cancer), and the third most common cancer in women (following breast and cervical cancer), according to the Cancer Association of South Africa.
Originally from Johannesburg, Forgan attended medical school at the University of the Witwatersrand. He qualified as a general surgeon at Stellenbosch University, sub-specialising in colorectal surgery at the University of Cape Town, before studying minimally invasive colorectal surgery at the Academic Medical Centre in Amsterdam.
He is also president of the South African Colorectal Society and runs a part-time private practise with his Tygerberg colleague, Dr Imraan Mia, at Cape Town’s Christiaan Barnard Hospital, where he has 32 all five-star Google reviews.
‘Early adopter’
Forgan considers himself an early adopter. But learning to use the da Vinci system did not happen overnight.
“We trained for ages,” he says. “On the surgical console there’s a simulator, so you spend hours and days and days doing procedures, over and over and over again. You have to get over 95% for each one of the procedures, before you can move on to the next skill.
“Then it’s how to use the machine, how to put it together, what to do if there’s an emergency; what if there’s a power failure and the machine stops working? How to safely remove it from the person. Then we went to the University of Lyon [in France] for two days of hands-on robotics training. And then a proctor – an international expert – comes to your theatre and does the procedures with you. So that was Dr Roger Gerjy, and that’s when we did Lorraine…”
First introduced by American biotechnology company Intuitive Surgical in 1999, the da Vinci Xi systems have sparked some liability lawsuits. An article from the Tampa Bay Times in February cites a lawsuit filed at the United States District Court in West Palm Beach, with a man claiming that a stray electrical arc from a surgical robot burned his wife’s small intestine during a colon cancer procedure, causing her death. The article quotes Intuitive Surgical’s 2023 financial report, which notes 8 606 da Vinci systems in use worldwide, having performed 2 286 000 procedures in 2023. The financial report mentions an undisclosed number of pending lawsuits, which the company disputes.
Nevertheless, Forgan remains an advocate.
Exiting via Tygerberg’s maze of corridors, he continues to reflect on his job. After our meeting, he is set to deliver a talk at the Cape Town International Convention Centre. His manner is earnest. Shrugging, he describes himself as a “glorified plumber”.