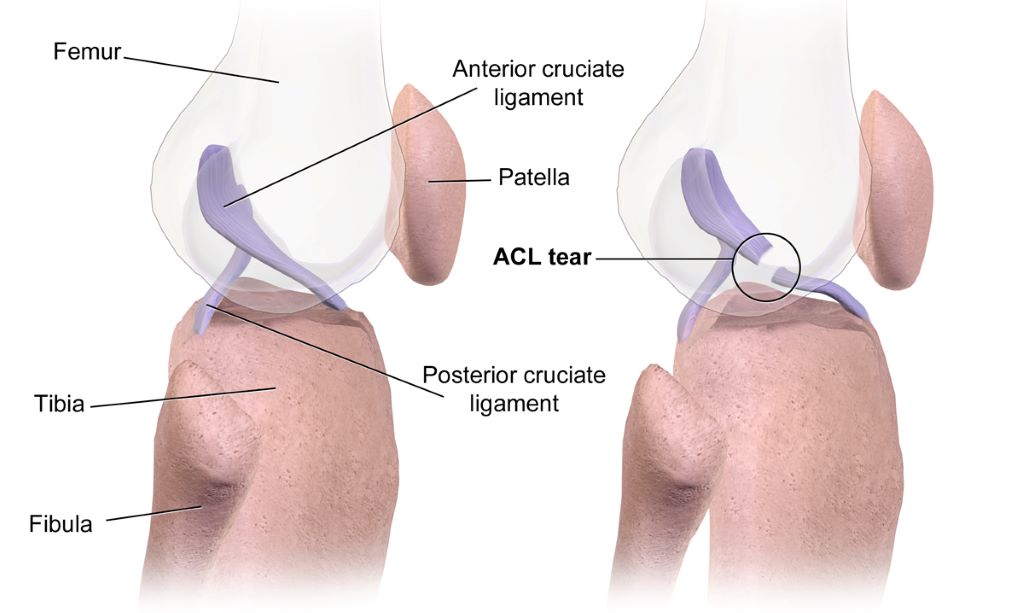
Some individuals who have had anterior-cruciate-ligament reconstruction (ACLR), the kind of surgery often performed on athletes’ knees, may develop early-onset knee osteoarthritis. A new study in the Journal of Orthopaedic Research indicates that altered knee joint movement after ACLR could be a contributing factor.
The study used a unique dynamic X-ray imaging system to accurately measure knee joint movement during walking in people who had undergone ACLR surgery and those with healthy knees. Compared with healthy controls, ACLR patients had a higher vertical position of the patella and a higher location of articular contact between the patella and the femur. A higher riding patella in the ACLR patients was caused by a longer-than-normal patellar tendon, the structure connecting the patella to the tibia. A surprising finding was that a higher riding patella was observed in both the ACLR knee and the uninjured contralateral knee of the ACLR patients.
Investigators suspect that a higher riding patella may contribute to the development of knee osteoarthritis by shifting the load bearing areas between the patella and the femur to regions of cartilage unaccustomed to load and leaving previously loaded regions unloaded.
“We don’t know whether a longer-than-normal patellar tendon that resulted in a higher riding patella existed prior to the ACL injury or resulted from the ACL injury or ACLR surgery. Further research is needed to determine the cause of a longer-than-normal patellar tendon in individuals who have undergone ACLR surgery,” said corresponding author Marcus G. Pandy, PhD, MEngSc, of the University of Melbourne, in Australia.
In one of the first studies of its kind, a team of researchers from Keck School of Medicine of USC has found that proteins and pathways involved in inflammation are associated with changes in bone mineral density (BMD) over time. Findings from the study were published in the Journal of Bone and Mineral Research.
The research, which was supported by the National Institutes of Health, could potentially lead to the identification of biomarkers that would serve as early indicators of a person’s risk for bone health issues later in life.
Bone mineral density is a measure of bone strength quantified by the amount of minerals in bone tissue. It peaks during young adulthood and slowly declines over the rest of the life cycle. BMD serves as an important marker for bone health and is commonly used to predict the risk of osteoporosis and other bone health conditions.
“Proteins are also substantial in the formation and maintenance of bone, and recently more studies have been trying to identify individual proteins associated with bone health,” says Emily Beglarian, the lead author and an epidemiology doctoral candidate in the Department of Population and Public Health Sciences at the Keck School of Medicine.
The study followed 304 obese/overweight Latino adolescents between the ages of 8 to 13 at baseline from the Study of Latino Adolescents at Risk for Type 2 Diabetes over an average period of three years. The researchers examined associations between over 650 proteins and annual measures of BMD, making this one of the first studies to evaluate these associations over years of follow-up. The proteins found to be associated with BMD were then inputted into a protein pathway database.
“The software determined what pathways the proteins were involved in within the human body. Our primary findings were that many of the proteins associated with BMD were involved in inflammatory and immune pathways in adolescent populations. There are other studies that found some of these same pathways were associated in older adult populations,” says Beglarian.
Existing studies suggest chronic inflammation can disrupt normal bone metabolism leading to lower BMD.
Importance of inclusive research
Childhood is a critical period for the development of BMD and this period can predict lifelong bone health.
“Until now, existing studies have centred on very specific populations. Most of them have small sample sizes, include either Chinese or non-Hispanic white populations, and focus on older adults – primarily on women because osteoporosis is four times more common in women than men,” says Beglarian.
“This is one of the first studies to investigate associations between proteins and BMD in younger populations. Investigating bone mineral density in early stages of life is important to determine how to address factors that may prevent people from reaching their potential peak bone density,” says Beglarian.
Advancing the understanding of bone health biomarkers
Additionally, Beglarian examined associations between BMD and a subset of protein markers from the initial proteins, in a separate cohort of young adults. Here she found that several proteins had similar associations with lower BMD. Low BMD is a risk factor for development of adulthood osteopenia and osteoporosis.
The study’s findings could potentially inform the development of biomarkers of bone health to identify people at risk that might benefit from intervention.
“It was interesting to see the way in which our study overlapped and differed with existing studies. Previous research was investigating BMD at the end of life when levels are already much lower,” she says. “Through my research I hope to address factors that decrease BMD earlier in life to help people get to their highest potential peak density, so they are set up over the rest of their lifetime to have a higher BMD.”
“Lipocartilage” is a type of supportive skeletal tissue, that consists of densely packed, bubble-like cells containing fat. This image shows a scan of mouse ear lipocartilage stained with a green fluorescent dye. Charlie Dunlop School of Biological Sciences
An international research team led by the University of California, Irvine has discovered a new type of skeletal tissue that offers great potential for advancing regenerative medicine and tissue engineering.
Most cartilage relies on an external extracellular matrix for strength, but “lipocartilage,” which is found in the ears, nose and throat of mammals, is uniquely packed with fat-filled cells called “lipochondrocytes” that provide super-stable internal support, enabling the tissue to remain soft and springy – similar to bubbled packaging material.
The study, published in the journal Science, describes how lipocartilage cells create and maintain their own lipid reservoirs, remaining constant in size. Unlike ordinary adipocyte fat cells, lipochondrocytes never shrink or expand in response to food availability.
“Lipocartilage’s resilience and stability provide a compliant, elastic quality that’s perfect for flexible body parts such as earlobes or the tip of the nose, opening exciting possibilities in regenerative medicine and tissue engineering, particularly for facial defects or injuries,” said corresponding author Maksim Plikus, UC Irvine professor of developmental and cell biology. “Currently, cartilage reconstruction often requires harvesting tissue from the patient’s rib – a painful and invasive procedure. In the future, patient-specific lipochondrocytes could be derived from stem cells, purified and used to manufacture living cartilage tailored to individual needs. With the help of 3D printing, these engineered tissues could be shaped to fit precisely, offering new solutions for treating birth defects, trauma and various cartilage diseases.”
Dr Franz Leydig first recognised lipochondrocytes in 1854, when he noted the presence of fat droplets in the cartilage of rat ears, a finding that was largely forgotten until now. With modern biochemical tools and advanced imaging methods, UC Irvine researchers comprehensively characterised lipocartilage’s molecular biology, metabolism and structural role in skeletal tissues.
They also uncovered the genetic process that suppresses the activity of enzymes that break down fats and reduce the absorption of new fat molecules, effectively locking lipochondrocytes’s lipid reserves in place. When stripped of its lipids, the lipocartilage becomes stiff and brittle, highlighting the importance of its fat-filled cells in maintaining the tissue’s combination of durability and flexibility. In addition, the team noted that in some mammals, such as bats, lipochondrocytes assemble into intricate shapes, like parallel ridges in their oversized ears, which may enhance hearing acuity by modulating sound waves.
“The discovery of the unique lipid biology of lipocartilage challenges long-standing assumptions in biomechanics and opens doors to countless research opportunities,” said the study’s lead author, Raul Ramos, a postdoctoral researcher in the Plikus laboratory for developmental and regenerative biology. “Future directions include gaining an understanding of how lipochondrocytes maintain their stability over time and the molecular programs that govern their form and function, as well as insights into the mechanisms of cellular aging. Our findings underscore the versatility of lipids beyond metabolism and suggest new ways to harness their properties in tissue engineering and medicine.”
Diagnosing osteoarthritis often occurs in the late stages when cartilage degradation is severe, making it difficult to distinguish it from other types of arthritis and to determine the best treatment plan. In work published in the Journal of Orthopaedic Research, investigators have developed and tested a new diagnostic test that uses two markers found in the synovial fluid of patients’ joints.
After assessing levels of cartilage oligomeric matrix protein and interleukin‐8, the team came up with an algorithm based on the ratio of these two markers and validated its efficacy in differentiating osteoarthritis from inflammatory arthritis in 171 human knee synovial fluid specimens.
“This study addresses an unmet need for objective diagnosis of osteoarthritis to improve clinical decision-making and patient outcomes,” said corresponding author Daniel Keter, BA, of CD Diagnostics, A Division of Zimmer Biomet.
(Left) An image of a 3D-printed material implanted in vivo for 4 weeks. The photo was taken using a scanning electron microscope. Credit: Dr Zhidao Xia. (Right) A photo of coral. Credit: Jesus Cobaleda.
Researchers at Swansea University have developed a revolutionary bone graft substitute inspired by coral which not only promotes faster healing but dissolves naturally in the body after the repair is complete.
Bone defects caused by conditions like fractures, tumours, and non-healing injuries are one of the leading causes of disability worldwide. Traditionally, doctors use either a patient’s own bone (autograft) or donor bone (allograft) to fill these gaps. However, these methods come with challenges, including a limited supply, the risk of infection and ethical concerns.
By using advanced 3D-printing technology, the team have developed a biomimetic material that mimics the porous structure and chemical composition of coral-converted bone graft substitute, blending perfectly with human bone and offering several incredible benefits:
Rapid Healing – It helps new bone grow within just 2–4 weeks.
Complete Integration – The material naturally degrades within 6–12 months after enhanced regeneration, leaving behind only healthy bone.
Cost-Effective – Unlike natural coral or donor bone, this material is easy to produce in large quantities.
In preclinical in vivo studies, the material showed remarkable results: it fully repaired bone defects within 3–6 months and even triggered the formation of a new layer of strong, healthy cortical bone in 4 weeks.
Most synthetic bone graft substitutes currently on the market can’t match the performance of natural bone. They either take too long to dissolve, don’t integrate well, or cause side effects like inflammation. This new material overcomes these problems by closely mimicking natural bone in both structure and biological behaviour.
Dr Xia explained: “Our invention bridges the gap between synthetic substitutes and donor bone. We’ve shown that it’s possible to create a material that is safe, effective, and scalable to meet global demand. This could end the reliance on donor bone and tackle the ethical and supply issues in bone grafting.”
Innovations like this not only promise to improve patient quality of life but also reduce healthcare costs and provide new opportunities for the biomedical industry.
The Swansea University team is now looking to partner with companies and healthcare organisations to bring this life-changing technology to patients around the world.
Hip implants with a delta ceramic or oxidised zirconium head and highly crosslinked polyethylene liner or cup had the lowest risk of revision during the 15 years after surgery, a new University of Bristol-led study has found. The research could help hospitals, surgeons and patients to choose what hip implant to use for replacement surgery.
The aim of the study, which appears in PLOS Medicine, was to establish hip implant materials at risk of revision. This would help orthopaedic surgeons, and patients, and to improve shared decision making before surgery by identifying hip implants with the lowest risk of revision.
The researchers analysed the UK’s National Joint Registry (NJR) data from 1 026 481 hip replacement patients carried out in the NHS and private sectors in England and Wales for up to 15 years after initial hip replacement operations (between 2003 to 2019).
After reviewing hip implants from the NJR data, the research team found the risk of revision following a hip replacement is influenced by the type of material used in the bearing surface. Bearing surfaces are the moving parts of an artificial hip joint that glide against each other during activity.
The data indicated that hip implants with a delta ceramic or oxidised zirconium head and highly crosslinked polyethylene liner or cup had the lowest risk of revision throughout the 15 years following hip replacement surgery.
These findings were confirmed when the research team investigated the specific reasons for revision hip replacements being performed. The data also showed 20 869 (2%) of hip replacement patients had to undergo revision after the initial surgery.
Senior author Dr Erik Lenguerrand, Senior Lecturer in Medical Statistics and Quantitative Epidemiologist in the Bristol Medical School:Translational Health Sciences (THS), said: “Our research has found the risk of hip replacement revision depends on the hip implant materials used in the original surgery. The lowest risk of revision are from implants with delta ceramic or oxidised zirconium head and a highly crosslinked polyethylene (HCLPE) liner or cup.
“Further research is needed to find out the association of implant materials with the risk of rehospitalisation, re-operation other than revision, mortality and the cost-effectiveness of these materials.”
Michael Whitehouse, Professor of Trauma and Orthopaedics at Bristol Medical School: THS, and senior clinical lead for the paper, explained: “Our study has used data from one of the largest registries in the world that includes all public and private health care sectors in England and Wales. This means that the data is more generally applicable than that available previously, which was limited by broad groupings of implant types or much smaller study size. It highlights the importance of considering the whole structure that is created when implants are put together to make up a hip replacement rather than focusing on individual components.
“Our findings will help hospitals, surgeons and patients to choose hip implants and combinations of them with the lowest risk of revision following an initial hip replacement operation.”
Tim Wilton, Medical Director of the National Joint Registry (NJR), added: “We are always delighted when the data from the NJR can be used by researchers to produce important research of this kind which gives meaningful analysis to guide surgeons and patients in their decisions. An important value of the NJR data is that it allows researchers a unique insight to assess the long-term performance of different hip implant materials.
“By tracking the combinations of materials used and subsequent revision rates, this research highlights the role of implant material choice in surgical outcomes. This ensures that the materials used can be optimised for longevity and patient health. Surgeons would be well advised to study these findings carefully in relation to the implant choices they make, and to use the information in pre-operative discussions with their patients. As the demand for joint replacements continues to rise, this insight can be invaluable in reducing revision surgery.”
The research was not a randomised controlled trial and therefore it was not possible to control all factors that can influence the risk of revision.
The categorisation of hip implants used as part of hip replacements is often broad in national joint replacement surgery registries and does not fully show differences in revision risks associated within the different types of implant materials grouped together.
For those of a certain age, Coneheads is an iconic 90s film. But for breakdancers, it seems, developing a cone-shaped head can be an occupational hazard.
According to a 2024 medical case report, a breakdancer who’d been performing for 19 years was treated for “headspin hole”, a condition also known as “breakdancer bulge” that’s unique to breakdancers. It entails a cone shaped mass developing on top of the scalp after repetitive head-spinning. Additional symptoms can include hair loss and sometimes pain around the lump.
Approximately 30% of breakdancers report hair loss and inflammation of their scalp from head-spinning. A headspin hole is caused by the body trying to protect itself. The repeated trauma from head-spinning causes the epicranial aponeurosis – a layer of connective tissue similar to a tendon, running from the back of your head to the front – to thicken along with the layer of fat under the skin on top of the head in an attempt to protect the bones of skull from injury.
The body causes a similar protective reaction to friction on the hands and feet, where callouses form to spread the pressure and protect the underlying tissues from damage. Everyday repetitive activities from holding smartphones or heavy weights through to poorly fitting shoes can result in callouses.
But a cone-shaped head isn’t the only injury to which breakdancers are prone, however. Common issues can include wrist, knee, hip, ankle, foot and elbow injuries, and moves such as the “windmill” and the “backspin” can cause bursitis – inflammation of the fluid filled sacs that protect the vertebrae of the spine. A headspin hole isn’t the worst injury you could sustain from breakdancing either. One dancer broke their neck but thankfully they were lucky enough not to have any major complications.
Others, such as Ukrainian breakdancer Anna Ponomarenko, have experienced pinched nerves that have left them paralysed. Ponomarenko recovered to represent her country in the Paris 2024 Olympics.
As with other sports, it’s unsurprising to hear that the use of protective equipment results in the reduction of injuries in breakdancing too.
But breakdancers aren’t the only ones to develop cone shaped heads.
Newborns
Some babies are born with a conical head after their pliable skull has been squeezed and squashed during the journey through the vaginal canal and the muscular contractions of mother’s uterus.
A misshapen head can also be caused by caput secundum, where fluid collects under the skin, above the skull bones. Usually, this condition resolves itself within a few days. Babies who’ve been delivered using a vacuum assisted cup (known as a Ventouse) – where the cup is applied to the top of the baby’s head to pull them out – can develop a similar fluid lump called a chignon.
Vacuum assisted delivery can also result in a more significant lump and bruising called a cephalohematoma, where blood vessels in the bones of the skull rupture. This is twice as common in boys than in girls and resolves within two weeks to six months.
If you’ve ever seen newborns wearing tiny hats in the first few hours of their life, then one of these conditions may be the reason.
Newborn skulls are made up of lots of small bony plates that aren’t fused together, which enables babies’ brains to grow without restriction. Usually, once the brain reaches a slower growth pace that the bones can keep up with, the plates fuse together. In craniosynostosis, the plates fuse together too early creating differently shaped heads. Surgery can prevent brain growth restriction but is usually unnecessary if the child hasn’t been identified as having an shaped head by six months of age.
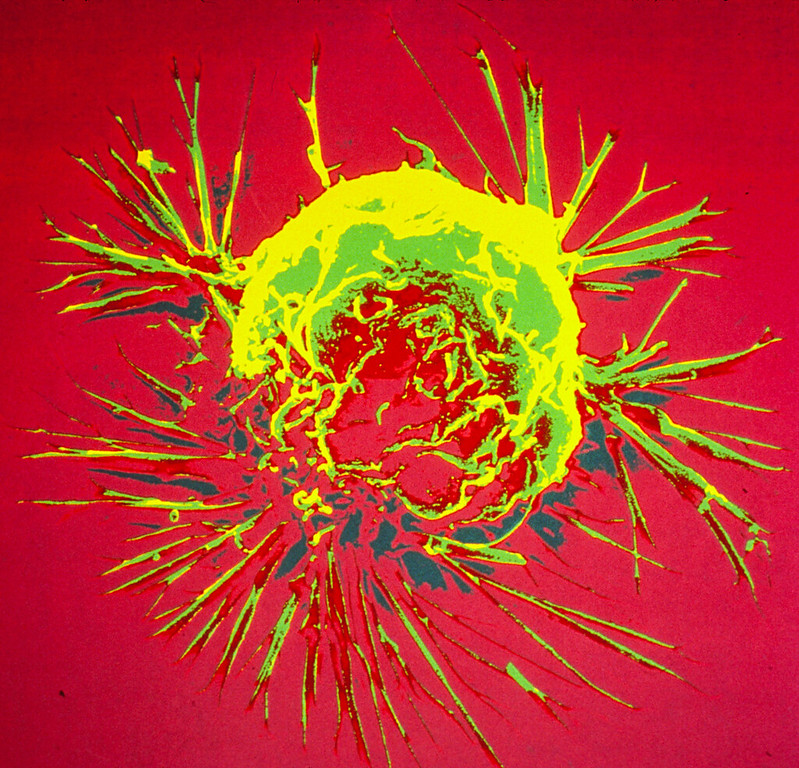
Colourised scanning electron micrograph of a breast cancer cell. Credit: NIH
Researchers from Tampere University, Finland, and Izmir Institute of Technology, Turkey, have developed an in vitro cancer model to investigate why breast cancer spreads to bone. Their findings, published in PLOS One, hold promise for advancing the development of preclinical tools to predict breast cancer bone metastasis.
Breast canceris a significant global public health challenge, with 2.3 million new cases and 700 000 deaths every year. Approximately 80% of patients with primary breast cancer can be cured, if they are diagnosed and treated promptly. However, in many cases, the cancer has already metastasised at the time of diagnosis.
Metastatic cancer is incurable and accounts for more than 90% of cancer-related deaths. Currently, there are no reliable in vitro models to study how breast cancer spreads to secondary organs such as bone, lung, liver or brain. Now, researchers from the Precision Nanomaterials Group at Tampere University in Finland, and the Cancer Molecular Biology Lab at Izmir Institute of Technology in Turkey, have used lab-on-a-chip platforms to create a physiologically relevant metastasis model to study the factors controlling breast cancer bone metastasis.
“Breast cancer most frequently spreads to bone, with an estimated rate of 53%, resulting in severe symptoms such as pain, pathological bone fractures, and spinal cord compressions. Our research provides a laboratory model that estimates the likelihood and mechanism of bone metastasis occurring within a living organism. This advances the understanding of molecular mechanisms in breast cancer bone metastasis and provides the groundwork for developing preclinical tools for predicting bone metastasis risk,” says Burcu Firatligil-Yildirir, postdoctoral researcher at Tampere University and the first author of the paper.
According to Nonappa, Associate Professor and leader of the Precision Nanomaterials Group at Tampere University, developing sustainable in vitro models that mimic the complexity of the native breast and bone microenvironment is a multidisciplinary challenge.
“Our work shows that physiologically relevant in vitro models can be generated by combining cancer biology, microfluidics and soft materials. The results open new possibilities for developing predictive disease, diagnostic and treatment models,” he says.
Scientists have identified a protein that blocks the activity of bone-forming cells (osteoblasts) by stopping them from maturing during the journey to sites of bone formation, finds a new study published in Communications Biology.
A team of researchers led by Dr Amy Naylor and Professor Roy Bicknell along with their team including Dr Georgiana Neag from the University of Birmingham have found that protein CLEC14A, which is found on endothelial cells in bone, block the function of bone development cells called osteoblasts.
During bone development, the endothelial cell’s job is to transport immature osteoblasts to sites where new bone is needed. However, when the protein CLEC14A is also present on the outside of the endothelial cell, osteoblasts are prevented from maturing to the point where they can form bone tissue.
This additional understanding of how blood vessel cells control bone-forming osteoblasts under normal, healthy conditions provide an avenue to develop treatments for patients who have insufficient bone formation
Dr Amy Naylor
In this study, osteoblast cells were taken from transgenic mice that either have been bred to produce CLEC14A or not. The osteoblasts were subsequently used in vitro in an induction solution, and the team found that cells taken from the protein-free mice reached maturation after 4 days while those in the presence of CLEC14A matured 8 days later. Furthermore, the CLEC14A-free samples saw a significant increase in mineralised bone tissue at day 18 in the study.
Dr Amy Naylor, Associate Professor in the School of Infection, Inflammation and Immunology at the University of Birmingham said:
“In the last decade, a specific type of blood vessel cell was identified within bones. This blood vessel is called ‘type-H’ and is responsible for guiding bone-forming osteoblasts to the places where bone growth is needed. Now we have discovered that a protein called CLEC14A can be found on the surface of type-H blood vessel cells.
“In the experiments we performed, when CLEC14A protein is present the osteoblasts that were sharing a ride on the endothelial cells produce less bone. Conversely, when the protein is removed, they produce more bone.
“This additional understanding of how blood vessel cells control bone-forming osteoblasts under normal, healthy conditions provide an avenue to develop treatments for patients who have insufficient bone formation, for example in patients with fractures that do not heal, osteoporosis or with chronic inflammatory diseases.”
Muscle activation in people suffering from hip osteoarthritis might be a case of ‘mind over matter’, new research from Edith Cowan University (ECU) has shown.
Research undertaken by ECU post-doctoral research fellow Dr Myles Murphy investigated muscle function in people with hip osteoarthritis and found that these patients were unable to activate their muscles as efficiently. The findings are published in Sports Medicine and Health Science.
“Previous research has well established that the degree to which a joint degenerates is not directly related to the amount of pain a person with arthritis will experience. In fact, the stronger your muscles are, the more protected your joint is, and the less pain you will experience.
“Our research has shown that people with hip osteoarthritis were unable to activate their muscles as efficiently, irrespective of strength.”
As part of this research, Dr Murphy and his team studied the brain function of people with hip arthritis, finding that the mind played an enormous part in this equation.
“Basically, people with hip arthritis are unable to activate their muscles properly because the brain is actively putting on the brake to stop them from using the muscle. We don’t know why that is, yet. But the brain seems to really be hampering the progress of rehabilitation and the muscles to protect the joint,” Dr Murphy said.
“We suspect that it is a short-term, protective response gone wrong. Unlike a rolled ankle or a hurt knee, chronic pain like osteoarthritis tends to hang around for a long time. Instead of being a protective response in the short term, the brain’s protective response becomes a really problematic and maladaptive response in the long term.”
Hip osteoarthritis is more prevalent in people over the age of 45, and women are much more like to develop the condition. People who have reported previous joint damage, from a sports injury or accident, are more likely to present with hip osteoarthritis, as are those with joint abnormalities, such as developmental dysplasia of the hip.
People living with hip arthritis often presents with different walking patterns than those without and could struggle with everyday activities like getting out of a chair, or vehicle.
“The impact on their daily lives is the biggest burden of osteoarthritis. The condition also results in substantial time-loss from work, and is associated with a high economic cost,” Dr Murphy said.
“The level of disability for normal activity within our study cohort was about 25%, compared to the 0% reported in our healthy control group.”
Dr Murphy is currently investigating novel ways in which to overcome this automatic muscle inhibition to effectively rehabilitate patients.
In the meantime, those living with hip osteoarthritis have been urged to continue strength training and to work with a qualified physiotherapist or exercise physiologist.
“You will need to work quite hard to build the strength in those muscles, but it can be done. There is no quick fix. Staying strong is something that people with hip osteoarthritis will need to actively keep working on,” he said.