The brain controls the release of glucose in a wide range of stressful circumstances, including fasting and low blood sugar levels.
However, less attention has been paid to its role in day-to-day situations.
In a study published in Molecular Metabolism, University of Michigan researchers have shown that a specific population of neurons in the hypothalamus help the brain maintain blood glucose levels under routine circumstances.
Over the past five decades, researchers have shown that dysfunction of the nervous system can lead to fluctuations in blood glucose levels, especially in patients with diabetes.
Some of these neurons are in the ventromedial nucleus of the hypothalamus, a region of the brain that controls hunger, fear, temperature regulation and sexual activity.
“Most studies have shown that this region is involved in raising blood sugar during emergencies,” said Alison Affinati, MD, PhD, assistant professor of internal medicine and member of Caswell Diabetes Institute.
“We wanted to understand whether it is also important in controlling blood sugar during day-to-day activities because that’s when diabetes develops.”
The group focused on VMHCckbr neurons, which contain a protein called the cholecystokinin b receptor.
They used mouse models in which these neurons were inactivated.
By monitoring the blood glucose levels, the researchers found that VMHCckbr neurons play an important role in maintaining glucose during normal activities, including the early part of the fasting period between the last meal of the day and waking up in the morning.
“In the first four hours after you go to bed, these neurons ensure that you have enough glucose so that you don’t become hypoglycaemic overnight,” Affinati said.
To do so, the neurons direct the body to burn fat through a process called lipolysis.
The fats are broken down to produce glycerol, which is used to make sugar.
When the group activated the VMHCckbr neurons in mice, the animals had increased glycerol levels in their bodies.
These findings could explain what happens in patients with prediabetes, since they show an increase in lipolysis during the night.
The researchers believe that in these patients, the VMHCckbr neurons could be overactive, contributing to higher blood sugar.
These nerve cells, however, only controlled lipolysis, which raises the possibility that other cells might be controlling glucose levels through different mechanisms.
“Our studies show that the control of glucose is not an on-or-off switch as previously thought,” Affinati said.
“Different populations of neurons work together, and everything gets turned on in an emergency. However, under routine conditions, it allows for subtle changes.”
The team is working to understand how all the neurons in the ventromedial nucleus co-ordinate their functions to regulate sugar levels during different conditions, including fasting, feeding and stress.
They are also interested in understanding how the brain and nervous system together affect the body’s control of sugar, especially in the liver and pancreas.
A new study from Pitt researchers challenges a decades-old assumption in neuroscience by showing that the brain uses distinct transmission sites – not a shared site – to achieve different types of plasticity. The findings, published in Science Advances, offer a deeper understanding of how the brain balances stability with flexibility, a process essential for learning, memory and mental health.
Neurons communicate through a process called synaptic transmission, where one neuron releases chemical messengers called neurotransmitters from a presynaptic terminal. These molecules travel across a microscopic gap called a synaptic cleft and bind to receptors on a neighbouring postsynaptic neuron, triggering a response.
Traditionally, scientists believed spontaneous transmissions (signals that occur randomly) and evoked transmissions (signals triggered by sensory input or experience) originated from one type of canonical synaptic site and relied on shared molecular machinery. Using a mouse model, the research team, led by Oliver Schlüter, associate professor of neuroscience, discovered that the brain instead uses separate synaptic transmission sites to carry out regulation of these two types of activity, each with its own developmental timeline and regulatory rules.
“We focused on the primary visual cortex, where cortical visual processing begins,” said Yue Yang, a research associate in the Department of Neuroscience and first author of the study. “We expected spontaneous and evoked transmissions to follow a similar developmental trajectory, but instead, we found that they diverged after eye opening.”
As the brain began receiving visual input, evoked transmissions continued to strengthen. In contrast, spontaneous transmissions plateaued, suggesting that the brain applies different forms of control to the two signaling modes.
To understand why, the researchers applied a chemical that activates otherwise silent receptors on the postsynaptic side. This caused spontaneous activity to increase, while evoked signals remained unchanged – strong evidence that the two types of transmission operate through functionally distinct synaptic sites.
This division likely enables the brain to maintain consistent background activity through spontaneous signaling while refining behaviourally relevant pathways through evoked activity. This dual system supports both homeostasis and Hebbian plasticity, the experience-dependent process that strengthens neural connections during learning.
“Our findings reveal a key organizational strategy in the brain,” said Yang. “By separating these two signaling modes, the brain can remain stable while still being flexible enough to adapt and learn.”
The implications could be broad. Abnormalities in synaptic signaling have been linked to conditions like autism, Alzheimer’s disease and substance use disorders. A better understanding of how these systems operate in the healthy brain may help researchers identify how they become disrupted in disease.
“Learning how the brain normally separates and regulates different types of signals brings us closer to understanding what might be going wrong in neurological and psychiatric conditions,” Yang said.
Innovative research paves way for more effective treatment for ALS and other neurodegenerative diseases
View of the spinal cord. Credit: Scientific Animations CC4.0
Respiratory complications are the most common cause of illness and death for the 300 000 Americans living with spinal cord injury, according to the Christopher & Dana Reeve Foundation.
But the results of a new study, led by researchers at Case Western Reserve University’s School of Medicine, show promise that a group of nerve cells in the brain and spinal cord, called interneurons, can boost breathing when the body faces certain physiological challenges, such as exercise and environmental conditions associated with altitude.
The researchers believe their discovery could lead to therapeutic treatments for patients with spinal cord injuries who struggle to breathe on their own. Their findings were recently published in the journal Cell Reports.
“While we know the brainstem sets the rhythm for breathing,” said Polyxeni Philippidou, an associate professor in the Department of Neurosciences at Case Western Reserve University School of Medicine and lead researcher, “the exact pathways that increase respiratory motor neuron output, have been unclear – until now.”
The research team included collaborators from the University of St. Andrews in the United Kingdom, the University of Calgary in Canada and the Biomedical Research Foundation Academy of Athens in Greece.
The study
By identifying a subset of interneurons as a new and potentially easy-to-reach point for treatment in spinal cord injuries and breathing-related diseases, the researchers believe doctors may be able to develop therapies to help improve breathing in people with such conditions.
The study showed that blocking signals from these spinal cord cells made it harder for the body to breathe properly when there was too much CO2 in the blood, a condition known as hypercapnia.
“These spinal cord cells are important for helping the body adjust its breathing in response to changes like high CO2 levels,” Philippidou said.
In this study, the team used genetically modified mouse models to explore the pathways involved in breathing. The researchers mapped neuron connections, measured neuron electrical activity, observed the models’ behaviour and used microscopy to visualise neuron structure and function – all focused on spinal cord nerve cells involved in breathing.
“We were able to define the genetic identity, activity patterns and role of a specialized subset of spinal cord neurons involved in controlling breathing,” Philippidou said.
The team is now testing whether targeting these neurons in neurodegenerative diseases like amyotrophic lateral sclerosis (ALS), also known as Lou Gehrig’s disease, and Alzheimer’s disease can help restore breathing.
A world-first Swinburne-led study into young adults’ brain activity has found that TV and gaming are associated with increased focus, while social media is associated with decreased focus.
In this study, published in Nature, 18-25 year olds exposed to phone screens for only three minutes experienced changes in mood, energy, tension, focus and happiness, explains one of the lead researchers Swinburne’s Dr Alexandra Gaillard.
“Our study was the first to record brain activity during different forms of screen use on young adults using functional near-infrared spectroscopy (fNIRS). We found that different forms of screen use, including social media, are associated with distinct patterns in activity and mood states.”
“Almost everyone owns a smart phone which they use for at least three hours a day for entertainment. Mood disorders are increasing in prevalence worldwide and we shouldn’t rule out the possibility that phones are a contributor.”
The study found that oxygenated haemoglobin (HbO) levels increased more following social media use and gaming compared to TV viewing, while deoxygenated haemoglobin (HbR) levels increased more following gaming.
“These findings suggest that interactive types of entertainment really do get the brain more engaged,” says Dr Gaillard.
“Interestingly, though, when it came to social media, people reported feeling less focused—and those who felt less focused also showed lower levels of brain activity. On the flip side, gaming actually helped boost focus and showed a rise in deoxygenated haemoglobin, which means the brain was actively using more of the oxygen it was getting. In other words, gaming seemed to get the brain working harder in a good way.”
With six months to go until Australia’s impending teen social media ban, there are still no clear pathways for age-checking tools and the positive impacts of the policy on different types of technology and platforms.
Dr Gaillard says that while this study looked at young adults, these findings suggest a similar outcome to teenagers which should be considered by experts when implementing the ban.
“If this is the effect on a fully developed brain, we urgently need to consider the impacts on teenagers and children who are increasingly using these technologies.”
The Swinburne research team is calling for further research to understand the complex and nuanced relationship between screen activities and how they engage they brain.
“Excessive screen time can negatively impact cognitive abilities, attention and executive functioning, but we also know how invaluable they can be in forming connections and a sense of belonging as well as improving educational outcomes.”
“This isn’t a call for blanket reductions; screens certainly serve a purpose for unwinding and leisure. We ask that young people are conscious of how their activity impacts them and that they make choices that are right for them.”
Creatine is popularly known as a muscle-building supplement, but its influence on human muscle function can be a matter of life or death. But getting it to one particular organ that needs it – the brain – is challenging.
“Creatine is very crucial for energy-consuming cells in skeletal muscle throughout the body, but also in the brain and in the heart,” said Chin-Yi Chen, a research scientist at Virginia Tech’s Fralin Biomedical Research Institute at VTC.
Chen is part of a research team working to develop a technique that uses focused ultrasound to deliver creatine directly to the brain. The work, being conducted in the lab of Fralin Biomedical Research Institute Assistant Professor Cheng-Chia “Fred” Wu, will be supported by a $30 000 grant from the Association for Creatine Deficiencies.
Creatine plays a vital role in the brain, where it interacts with phosphoric acid to help create the key energy molecule adenosine triphosphate (ATP). In addition to its role in energy production, creatine also influences neurotransmitter systems.
For example, creatine influences the brain’s major inhibitory pathways that use the neurotransmitter gamma-aminobutyric acid (GABA), which limits neuronal excitability in the central nervous system. It may play a role in a variety of functions, including seizure control, learning, memory, and brain development.
A growing body of research suggests that creatine may itself function as a neurotransmitter, as it is delivered to neurons from glial cells in the brain and can influence signalling processes between other neurons. While creatine deficiency disorders can weaken the skeletal muscle and the heart, they can also severely affect the brain. Many patients see increased muscle mass and body weight with creatine supplements, but they often continue to face neurodevelopmental challenges that can hinder their ability to speak, read, or write.
This is largely caused by the brain’s protective blood-brain barrier preventing creatine entry.
Wu studies therapeutic focused ultrasound, which precisely directs sound waves to temporarily accessed areas of the brain. The process allows drugs to reach diseased tissue without harming surrounding healthy cells. While Wu is investigating this method as a potential treatment for paediatric brain cancer, he also sees potential in applying it to creatine deficiency.
“Through the partnership between Virginia Tech and Children’s National Hospital, I was able to present our work in focused ultrasound at the Children’s National Research & Innovation Campus,” Wu said. “There, I met Dr Seth Berger, a medical geneticist, who introduced me to creatine transporter deficiency. Together, we saw the promise that focused ultrasound had to offer.”
The Focused Ultrasound Foundation has recognised Virginia Tech and Children’s National as Centers of Excellence. Wu said the two organisations bring together clinical specialists, trial experts, and research scientists who can design experiments that could inform future clinical trials.
“It was a moment that made me really excited – that I had found a lab where I could move from basic research to something that could help patients,” Chen said. “When Fred asked me, ‘Are you interested in this project?’ I said, ‘Yes, of course.’”
Because creatine deficiencies can impair brain development, the early stages of Chen’s project will concentrate on using focused ultrasound to deliver creatine across the blood-brain barrier. Chen hopes the technique will restore normal brain mass in models of creatine deficiency.
Johns Hopkins University researchers have grown a novel whole-brain organoid, complete with neural tissues and rudimentary blood vessels, in an advance that could usher in a new era of research into neuropsychiatric disorders such as autism.
“We’ve made the next generation of brain organoids,” said senior author Annie Kathuria, an assistant professor in JHU’s Department of Biomedical Engineering who studies brain development and neuropsychiatric disorders. “Most brain organoids that you see in papers are one brain region, like the cortex or the hindbrain or midbrain. We’ve grown a rudimentary whole-brain organoid; we call it the multi-region brain organoid (MRBO).”
The research, published in Advanced Science, marks one of the first times scientists have been able to generate an organoid with tissues from each region of the brain connected and acting in concert. Having a human cell-based model of the brain will open possibilities for studying schizophrenia, autism, and other neurological diseases that affect the whole brain – work that typically is conducted in animal models.
To generate a whole-brain organoid, Kathuria and members of her team first grew neural cells from the separate regions of the brain and rudimentary forms of blood vessels in separate lab dishes. The researchers then stuck the individual parts together with sticky proteins that act as a biological superglue and allowed the tissues to form connections. As the tissues began to grow together, they started producing electrical activity and responding as a network.
Much smaller compared to a real brain – weighing in at 6 million to 7 million neurons compared with tens of billions in adult brains – these organoids provide a unique platform on which to study whole-brain development.
The researchers also saw the creation of an early blood–brain barrier formation, a layer of cells that surround the brain and control which molecules can pass through.
“We need to study models with human cells if you want to understand neurodevelopmental disorders or neuropsychiatric disorders, but I can’t ask a person to let me take a peek at their brain just to study autism,” Kathuria said. “Whole-brain organoids let us watch disorders develop in real time, see if treatments work, and even tailor therapies to individual patients.”
Using whole-brain organoids to test experimental drugs may also help improve the rate of clinical trial success, researchers said. Roughly 85% to 90% of drugs fail during Phase 1 clinical trials. For neuropsychiatric drugs, the fail rate is closer to 96%. This is because scientists predominantly study animal models during the early stages of drug development. Whole-brain organoids more closely resemble the natural development of a human brain and likely will make better test subjects.
“Diseases such as schizophrenia, autism, and Alzheimer’s affect the whole brain, not just one part of the brain. If you can understand what goes wrong early in development, we may be able to find new targets for drug screening,” Kathuria said. “We can test new drugs or treatments on the organoids and determine whether they’re actually having an impact on the organoids.”
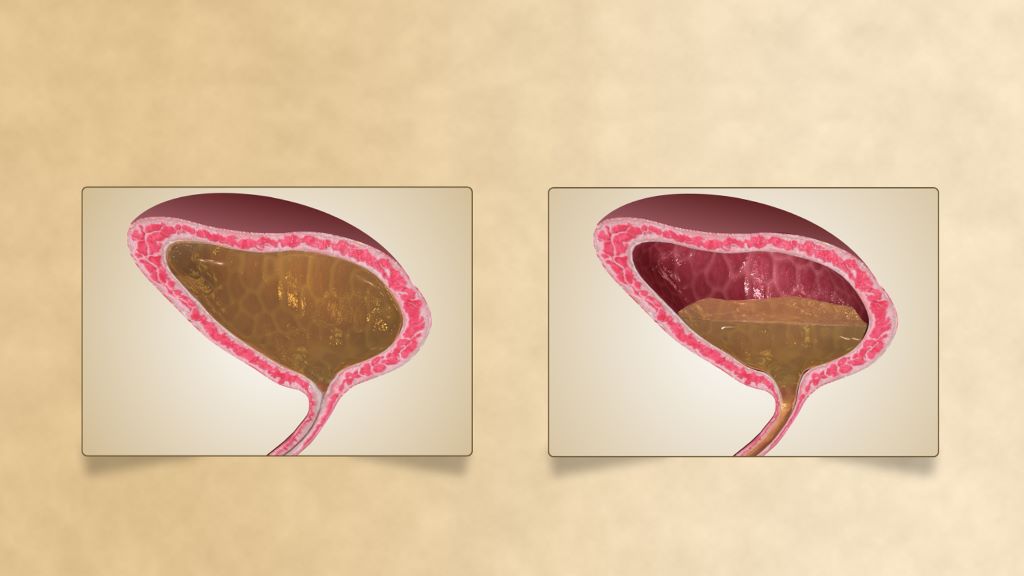
Urinary incontinence is a devastating condition, leading to significant adverse impacts on patients’ mental health and quality of life. Disorders of urination are also a key feature of all neurological disorders.
A USC research team has now made major progress in understanding how the human spinal cord triggers the bladder emptying process. The discovery could lead to exciting new therapies to help patients regain control of this essential function.
In the pioneering study, a team from USC Viterbi School of Engineering and Keck School of Medicine of USC has harnessed functional ultrasound imaging to observe real-time changes in blood flow dynamics in the human spinal cord during bladder filling and emptying.
The work was published in Nature Communications and was led by Charles Liu, the USC Neurorestoration Center director at Keck School of Medicine of USC and professor of biomedical engineering at USC Viterbi, and Vasileios Christopoulos, assistant professor at the Alfred E. Mann Department of Biomedical Engineering.
The spinal cord regulates many essential human functions, including autonomic processes like bladder, bowel, and sexual function. These processes can break down when the spinal cord is damaged or degenerated due to injury, disease, stroke, or aging. However, the spinal cord’s small size and intricate bony enclosure have made it notoriously challenging to study directly in humans.
Unlike in the brain, routine clinical care does not involve invasive electrodes and biopsies in the spinal cord due to the obvious risks of paralysis.
Furthermore, fMRI imaging, which comprises most of human functional neuroimaging, does not exist in practical reality for the spinal cord, especially in the thoracic and lumbar regions where much of the critical function localises.
“The spinal cord is a very undiscovered area,” Christopoulos said. “It’s very surprising to me because when I started doing neuroscience, everybody was talking about the brain. And Dr. Liu and I asked, “What about the spinal cord?”
“For many, it was just a cable that transfers information from the brain to the peripheral system. The truth was that we didn’t know how to go there—how to study the spinal cord in action, visualize its dynamics and truly grasp its role in physiological functions.”
Functional ultrasound imaging: A new window into the spinal cord
To overcome these barriers, the USC team employed functional ultrasound imaging (fUSI), an emerging neuroimaging technology that is minimally invasive. The fUSI process allowed the team to measure where changes in blood volume occur on the spinal cord during the cycle of urination.
However, fUSI requires a “window” through the bone to image the spinal cord. The researchers found a unique opportunity by working with a group of patients undergoing standard-of-care epidural spinal cord stimulation surgery for chronic low back pain.
“During the implantation of the spinal cord stimulator, the window we create in the bone through which we insert the leads gives us a perfect and safe opportunity to image the spinal cord using fUSI with no risk or discomfort to the study volunteers,” said co-first author Darrin Lee, associate director of the USC Neurorestoration Center, who performed the surgeries.
“While the surgical team was preparing the stimulator, we gently filled and emptied the bladder with saline to simulate a full urination cycle under anaesthesia while the research team gathered the fUSI data,” added Evgeniy Kreydin from the Rancho Los Amigos National Rehabilitation Center and the USC Institute of Urology, who was already working closely with Liu to study the brain of stroke patients during micturition using fMRI.
“This is the first study where we’ve shown that there are areas in the spinal cord where activity is correlated with the pressure inside the bladder,” Christopoulos said.
“Nobody had ever shown a network in the spinal cord correlated with bladder pressure. What this means is I can look at the activity of your spinal cord in these specific areas and tell you your stage of the bladder cycle – how full your bladder is and whether you’re about to urinate.”
Christopoulos said the experiments identified that some spinal cord regions showed positive correlation, meaning their activity increased as bladder pressure rose, while others showed negative (anti-correlation), with activity decreasing as pressure increased. This suggests the involvement of both excitatory and inhibitory spinal cord networks in bladder control.
“It was extremely exciting to take data straight from the fUSI scanner in the OR to the lab, where advanced data science techniques quickly revealed results that have never been seen before, even in animal models, let alone in humans,” said co-first author Kofi Agyeman, biomedical engineering postdoc.
New hope for patients
Liu has worked for two decades at the intersection of engineering and medicine to develop transformative strategies to restore function to the nervous system. Christopoulos has spent much of his research career developing neuromodulation techniques to help patients regain motor control.
Together, they noted that for patients, retaining control of the autonomic processes that many of us take for granted is more fundamental than even walking.
“If you ask these patients, the most important function they wanted to restore was not their motor or sensory function. It was things like sexual function and bowel and bladder control,” Christopoulos said, noting that urinary dysfunction often leads to poor mental health. “It’s a very dehumanising problem to deal with.”
Worse still, urinary incontinence leads to more frequent urinary tract infections (UTIs) because patients must often be fitted with a catheter. Due to limited sensory function, they may not be able to feel that they have an infection until it is more severe and has spread to the kidneys, resulting in hospitalisation.
This study offers a tangible path toward addressing this critical need for patients suffering from neurogenic lower urinary tract dysfunction. The ability to decode bladder pressure from spinal cord activity provides proof-of-concept for developing personalised spinal cord interfaces that could warn patients about their bladder state, helping them regain control.
Currently, almost all neuromodulation strategies for disorders of micturition are focused on the lower urinary tract, largely because the neural basis of this critical process remains unclear.
“One has to understand a process before one can rationally improve it,” Liu said.
This latest research marks a significant step forward, opening new avenues for precision medicine interventions that combine invasive and noninvasive neuromodulation with pharmacological therapeutics to make neurorestoration of the genitourinary system a clinical reality for millions worldwide.
Excessive astrocytic GABA impairs fear extinction in PTSD, new drug target offers hope for treatment
Figure 1. Astrocyte-Derived GABA and Therapeutic Effects of KDS2010 in PTSD. Brain imaging of PTSD patients revealed unusually high levels of GABA and reduced cerebral blood flow in the prefrontal cortex, showing that changes strongly correlated with symptom severity. In animal models, this excess GABA was traced to reactive astrocytes producing it abnormally due to increased MAOB and reduced levels of the GABA-degrading enzyme ABAT. This disrupted normal brain function and impaired the ability to extinguish fear. Treatment with KDS2010, a selective MAOB inhibitor, successfully lowered astrocytic GABA, restored brain activity, and rescued fear extinction, highlighting its potential as a therapeutic option. Credit: Institute for Basic Science
Why do patients with post traumatic stress disorder (PTSD) often struggle to forget traumatic memories, even long after the danger has passed? This failure to extinguish fear memories has long puzzled scientists and posed a major hurdle for treatment, especially since current medications targeting serotonin receptors offer limited relief for only a subset of patients.
In a new discovery, scientists at the Institute for Basic Science (IBS) and Ewha Womans University have uncovered a new brain mechanism driving PTSD – and a promising drug that may counteract its effects. The research is reported in Signal Transduction and Target Therapy.
Led by Dr C. Justin Lee at the IBS Center for Cognition and Sociality and Professor Lyoo In Kyoon at Ewha Womans University, the team has shown that excessive GABA (gamma-aminobutyric acid) produced by astrocytes, which are star-shaped support cells in the brain, impairs the brain’s ability to extinguish fear memories. This deficit is a core feature of PTSD and helps explain why traumatic memories can persist long after the threat has passed.
Crucially, the researchers found that a brain-permeable drug called KDS2010, which selectively blocks the monoamine oxidase B enzyme responsible for this abnormal GABA production, can reverse PTSD-like symptoms in mice. The drug has already passed Phase 1 safety trials in humans, making it a strong candidate for future PTSD treatments.
PTSD remains difficult to treat, with current medications targeting serotonin pathways providing limited relief for many patients. The new study focused on the medial prefrontal cortex (mPFC), a region of the brain critical for regulating fear, and found that PTSD patients had unusually high levels of GABA and reduced cerebral blood flow in this area. These findings emerged from brain imaging studies of more than 380 participants. Importantly, GABA levels decreased in patients who showed clinical improvement, pointing to the chemical’s central role in recovery.
To uncover the origin of this excess GABA, the researchers examined postmortem human brain tissue and used PTSD-like mouse models. They discovered that astrocytes, not neurons, were producing abnormal amounts of GABA via the enzyme monoamine oxidase B (MAOB). This astrocyte-derived GABA impaired neural activity, blocking the brain’s ability to forget traumatic memories.
When the researchers administered KDS2010, a highly selective, reversible MAOB inhibitor developed at IBS, the mice showed normalized brain activity and were able to extinguish fear responses. The drug reduced GABA levels, restored blood flow in the mPFC, and re-enabled memory extinction mechanisms. The study thus confirms astrocytic MAOB as a central driver of PTSD symptoms, and MAOB inhibition as a viable therapeutic path.
A major challenge of the study was linking clinical findings in humans with cellular mechanisms in the lab. The researchers addressed this by applying a “reverse translational” strategy: they began with clinical brain scans and moved backward to identify the cellular source of dysfunction, then confirmed the mechanism and tested drug effects in animal models. This approach led to a new understanding of how glial cells – long thought to be passive – actively shape psychiatric symptoms.
“This study is the first to identify astrocyte-derived GABA as a key pathological driver of fear extinction deficit in PTSD,” said Dr Won Woojin, a postdoctoral researcher and co-first author of the study. “Our findings not only uncover a novel astrocyte-based mechanism underlying PTSD, but also provide preclinical evidence for a new therapeutic approach using an MAOB inhibitor.”
Director C. Justin LEE, who led the study, emphasized that “This work represents a successful example of reverse translational research, where clinical findings in human guided the discovery of underlying mechanisms in animal models. By identifying astrocytic GABA as a pathological driver in PTSD and targeting it via MAOB inhibition, the study opens a completely new therapeutic paradigm not only for PTSD but also for other neuropsychiatric disorders such as panic disorder, depression, and schizophrenia.”
The researchers plan to further investigate astrocyte-targeted therapies for various neuropsychiatric disorders. With KDS2010 currently undergoing Phase 2 clinical trials, this discovery may soon lead to new options for patients whose symptoms have not responded to conventional treatments.
Inhibitory neurons and astrocytes hold the key to sharper functional brain imaging –
Image of an astrocyte, a subtype of glial cells. Glial cells are the most common cell in the brain. Credit: Pasca Lab, Stanford University
NIH support from: NINDS, NIMH, NIGMS, NCATS
Researchers at the Center for Neuroscience Imaging Research within the Institute for Basic Science (IBS) have uncovered a two-step mechanism by which the brain regulates blood volume – a breakthrough with significant implications for how scientists understand and interpret functional magnetic resonance imaging (fMRI).
At the core of this study are somatostatin-expressing interneurons (SST neurons), a specialised type of inhibitory neuron. Among all neurons in the brain, approximately 15% are inhibitory neurons, but the role of these neurons in regulating cerebral blood volume has not been clearly elucidated in previous studies, with most of earlier research mainly focusing on the excitatory neurons. The new study by the IBS team sheds light on how inhibitory neurons interact with astrocytes, a type of support cell, to precisely control blood vessel dilation in the brain.
To unravel this complex process, the research team developed mouse models (e.g., SST-ChR2, SST-hM4Di) that allowed selective activation or inhibition of SST neurons. The researchers also used advanced neuroscience techniques in these mice. Specifically, they applied optogenetics and chemogenetics to precisely control the activity of these neurons. To observe the cellular and vascular responses, the team employed calcium imaging to visualise astrocyte activity, electrophysiology to measure neural signals, and intrinsic optical imaging (OIS) alongside ultra-high-field functional MRI (fMRI) to track blood volume dynamics with high spatial and temporal resolution.
Through these experiments, the team uncovered a two-step mechanism of vasodilation. In the early phase, SST neurons, when activated, released nitric oxide (NO) – a powerful vasodilator that triggered rapid and widespread expansion of nearby blood vessels. This was followed by a late phase, in which astrocytes became activated and induced slower, more localised vasodilation, especially during periods of prolonged sensory stimulation.
Figure 1. Somatostatin neurons regulate astrocytes surrounding cerebral blood vessels, enabling more precise delivery of blood volume to specific brain regions, thereby enhancing the spatial accuracy of neurovascular responses. Credit: Institute for Basic Science
Notably, when SST neurons were silenced, the layer-specific precision of blood volume signals observed in fMRI was lost – a finding that links cellular activity directly to spatial specificity in imaging data.
“This two-step mechanism involving inhibitory neurons and astrocytes helps explain why high-resolution fMRI can distinguish activity between different layers of the brain cortex,” the researchers explained. “Our study fills a major gap in understanding how neural signals are translated into the blood volume changes we measure in brain imaging.”
The team also overcame several technical challenges – including distinguishing overlapping signals and timing differences – by integrating multiple imaging techniques and running extensive repeat experiments to validate the causal link between SST neuron activity and vascular responses.
Their findings not only advance basic knowledge of neurovascular coupling, but also open new avenues for investigating neurological and psychiatric conditions in which SST neuron function is impaired, such as Alzheimer’s disease, depression, and autism. The group plans to study disease-model mice to identify how disruptions in this neuron–astrocyte–vascular pathway affect blood volume, brain function, and fMRI signals.
Ultimately, this research lays the groundwork for improving the accuracy of brain imaging interpretation and may lead to better diagnostic and therapeutic strategies for brain disorders.
New study uncovers how a metabolic “overload” in specialised brain cells triggers the need to sleep.
Photo by Cottonbro on Pexels
Sleep may not just be rest for the mind – it may be essential maintenance for the body’s power supply. A new study by University of Oxford researchers, published in Nature, reveals that the pressure to sleep arises from a build-up of electrical stress in the tiny energy generators inside brain cells.
The discovery offers a physical explanation for the biological drive to sleep and could reshape how scientists think about sleep, ageing, and neurological disease.
When the mitochondria of certain sleep-regulating brain cells (studied in fruit flies) become overcharged, they start to leak electrons, producing potentially damaging byproducts known as reactive oxygen species. This leak appears to act as a warning signal that pushes the brain into sleep, restoring equilibrium before damage spreads more widely.
‘You don’t want your mitochondria to leak too many electrons,’ said Dr Sarnataro. ‘When they do, they generate reactive molecules that damage cells.’
The researchers found that specialised neurons act like circuit breakers – measuring this mitochondrial electron leak and triggering sleep when a threshold is crossed. By manipulating the energy handling in these cells – either increasing or decreasing electron flow – the scientists could directly control how much the flies slept.
Even replacing electrons with energy from light (using proteins borrowed from microorganisms) had the same effect: more energy, more leak, more sleep.
Professor Miesenböck said: ‘We set out to understand what sleep is for, and why we feel the need to sleep at all. Despite decades of research, no one had identified a clear physical trigger. Our findings show that the answer may lie in the very process that fuels our bodies: aerobic metabolism. In certain sleep-regulating neurons, we discovered that mitochondria – the cell’s energy producers – leak electrons when there is an oversupply. When the leak becomes too large, these cells act like circuit breakers, tripping the system into sleep to prevent overload.’
The findings help explain well-known links between metabolism, sleep, and lifespan. Smaller animals, which consume more oxygen per gram of body weight, tend to sleep more and live shorter lives. Humans with mitochondrial diseases often experience debilitating fatigue even without exertion, now potentially explained by the same mechanism.
‘This research answers one of biology’s big mysteries,’ said Dr Sarnataro.
‘Why do we need sleep? The answer appears to be written into the very way our cells convert oxygen into energy.’