Preventive health technologies, such as wrist-worn activity trackers or health and fitness apps, are popular tools for promoting wellbeing, but new research published in the Journal of Consumer Affairs reveals that consumer engagement with these technologies can be considered a double-edged sword.
The study, which involved 30 in-depth interviews with users, found that consumers engage with preventive health technologies based on a variety of health goals—for example, to lose weight, improve performance, monitor data of an enjoyable activity, or acquire a healthy routine.
These diverse goals led users to experience different “engagement trajectories.” For example, some people had increased engagement initially and then reached a stabilization point of engagement, while others had reduced engagement after their initial interest. Still others became obsessive and over-engaged with the technology over time, while others had fluctuating cycles of engagement.
Investigators found that consumer engagement with preventive health technologies can have beneficial or detrimental effects on wellbeing depending on these types of trajectories. Particularly, while these technologies can support healthy routines, they can also lead to compulsive usage, ultimately leading to users’ ill-being.
“As preventive health technologies become more integrated into our daily lives, it’s crucial to understand the factors that lead to over-engagement and ill-being, so that designers of health apps can mitigate these risks,” said corresponding author Lisa Baiwir, a PhD candidate at the University of Liège, in Belgium.
Exhaled breath contains chemical clues to what’s going on inside the body, including diseases like lung cancer. And devising ways to sense these compounds could help doctors provide early diagnoses — and improve patients’ prospects. In a study in ACS Sensors, researchers report the development of ultrasensitive, nanoscale sensors that in small-scale tests distinguished a key change in the chemistry of the breath of people with lung cancer.
Besides carbon dioxide, people also exhale other airborne compounds. Researchers have determined that declines in one exhaled chemical — isoprene — can indicate the presence of lung cancer. However, to detect such small shifts, a sensor would need to be highly sensitive, capable of detecting isoprene levels in the parts-per-billion (ppb) range. It would also need to differentiate isoprene from other volatile chemicals and withstand breath’s natural humidity. Previous attempts to engineer gas sensors with characteristics like these have focused on metal oxides, including one particularly promising compound made with indium oxide. A team led by Pingwei Liu and Qingyue Wangset out to refine indium oxide-based sensors to detect isoprene at the level at which it naturally occurs in breath.
The researchers developed a series of indium(III) oxide (In2O3)-based nanoflake sensors. In experiments, they found one type, which they called Pt@InNiOx for the platinum (Pt), indium (In) and nickel (Ni) it contains, performed best. These Pt@InNiOx sensors:
Detected isoprene levels as low as 2ppb, a sensitivity that far surpassed earlier sensors.
Responded to isoprene more than other volatile compounds commonly found in breath.
Performed consistently during nine simulated uses.
More importantly, the authors’ real-time analysis of the nanoflakes’ structure and electrochemical properties revealed that Pt nanoclusters uniformly anchored on the nanoflakes catalyzed the activation of isoprene sensing, leading to the ultrasensitive performance.
Finally, to showcase the potential medical use of these sensors, the researchers incorporated the Pt@InNiOx nanoflakes into a portable sensing device. Into this device they introduced breath collected earlier from 13 people, five of whom had lung cancer. The device detected isoprene levels lower than 40 ppb in samples from participants with cancer and more than 60 ppb from cancer-free participants. This sensing technology could provide a breakthrough in non-invasive lung cancer screening and has the potential to improve outcomes and even save lives, the researchers say.
Peng Zheng shows off the heart of the blood test, chip with a groundbreaking nanostructured surface on which blood is tested. Image: Will Kirk / Johns Hopkins University
With heart attacks, every second counts. A newly developed blood test on a chip diagnoses them in minutes rather than hours and could be adapted as a tool for first responders and people at home.
“Heart attacks require immediate medical intervention in order to improve patient outcomes, but while early diagnosis is critical, it can also be very challenging – and near impossible outside of a clinical setting,” said lead author Peng Zheng, an assistant research scientist at Johns Hopkins University. “We were able to invent a new technology that can quickly and accurately establish if someone is having a heart attack.”
The proof-of-concept work, which can be modified to detect infectious diseases and cancer biomarkers, is described in Advanced Science.
Zheng and senior author Ishan Barman develop diagnostic tools through biophotonics, using laser light to detect biomarkers, which are bodily responses to conditions including disease. Here they used the technology to find the earliest signs in the blood that someone was having a heart attack. Heart attacks remain one of the trickiest conditions to diagnose, with symptoms that vary widely and biological signals that can be subtle and easy to miss in the early stages of an attack, when medical intervention can do the most good.
Will be like ‘ Star Trek tricorder’
People suspected of having heart attacks typically are given a combination of tests to confirm the diagnosis – usually starting with electrocardiograms to measure the electrical activity of the heart, a procedure that takes about five minutes, and blood tests to detect the hallmarks of a heart attack, where lab work can take at least an hour and often has to be repeated.
The stand-alone blood test the team created provides results in five to seven minutes. It’s also more accurate and more affordable than current methods, the researchers say.
Though created for speedy diagnostic work in a clinical setting, the test could be adapted as a hand-held tool that first responders could use in the field, or that people might even be able to use themselves at home.
“We’re talking about speed, we’re talking about accuracy, and we’re talking of the ability to perform measurements outside of a hospital,” said Barman, a bioengineer in JHU’s Department of Mechanical Engineering. “In the future we hope this could be made into a hand-held instrument like a Star Trek tricorder, where you have a drop of blood and then, voilà, in a few seconds you have detection.”
The heart of the invention is a tiny chip with a groundbreaking nanostructured surface on which blood is tested. The chip’s “metasurface” enhances electric and magnetic signals during Raman spectroscopy analysis, making heart attack biomarkers visible in seconds, even in ultra-low concentrations. The tool is sensitive enough to flag heart attack biomarkers that might not be detected at all with current tests, or not detected until much later in an attack.
Though designed to diagnose heart attacks, the tool could be adapted to detect cancer and infectious diseases, the researchers say.
“There is enormous commercial potential,” Barman said. “There’s nothing that limits this platform technology.”
Next the team plans to refine the blood test and explore larger clinical trials.
Erin Yamamoto, MD, and Juan Piantino, MD, are among the co-authors of a new study from Oregon Health & Science University that used imaging of neurosurgery patients to definitively reveal the existence of waste-clearance pathways in the human brain known as the glymphatic system. (OHSU/Christine Torres Hicks)
Scientists have long theorised about a network of pathways in the brain that are believed to clear metabolic proteins that would otherwise build up and potentially lead to Alzheimer’s and other forms of dementia. But they had never definitively revealed this network in people – until now.
A new study involving five patients undergoing brain surgery at Oregon Health & Science University provides imaging of this network of perivascular spaces (fluid-filled structures along arteries and veins) within the brain for the first time.
“Nobody has shown it before now,” said senior author Juan Piantino, MD, associate professor of pediatrics (neurology) in the OHSU School of Medicine and a faculty member of the Neuroscience Section of the Papé Family Pediatric Research Institute at OHSU. “I was always skeptical about it myself, and there are still a lot of skeptics out there who still don’t believe it. That’s what makes this finding so remarkable.”
The study combined the injection of an inert contrasting agent with a special type of magnetic resonance imaging to discern cerebrospinal fluid flowing along distinct pathways in the brain 12, 24 and 48 hours following surgery. In definitively revealing the presence of an efficient waste-clearance system within the human brain, the new study supports the promotion of lifestyle measures and medications already being developed to maintain and enhance it.
“This shows that cerebrospinal fluid doesn’t just get into the brain randomly, as if you put a sponge in a bucket of water,” Piantino said. “It goes through these channels.”
More than a decade ago, scientists at the University of Rochester first proposed the existence of a network of waste-clearance pathways in the brain akin to the body’s lymphatic system, part of the immune system. Those researchers confirmed it with real-time imaging of the brains of living mice. Due to its dependence on glial cells in the brain, they coined the term “glymphatic system” to describe it.
However, scientists had yet to confirm the existence of the glymphatic system through imaging in people.
Pathways revealed in patients
The new study examined five OHSU patients who underwent neurosurgery to remove tumours in their brains between 2020 and 2023. In each case, the patients consented to having a gadolinium-based inert contrasting agent injected through a lumbar drain used as part of the normal surgical procedure for tumour removal. The tracer would be carried with cerebrospinal fluid into the brain.
Afterward, each patient underwent magnetic resonance imaging, or an MRI, at different time points to trace the spread of cerebrospinal fluid.
Rather than diffusing uniformly through brain tissue, the images revealed fluid moving along pathways — through perivascular spaces in clearly defined channels. Researchers documented the finding with a specific kind of MRI known as fluid attenuated inversion recovery, or FLAIR. This type of imaging is sometimes used following the removal of tumors in the brain. As it turns out, it also revealed the gadolinium tracer in the brain, whereas the standard MRI sequences did not.
“That was the key,” Piantino said.
“You can actually see dark perivascular spaces in the brain turn bright,” said co-lead author Erin Yamamoto, MD, a resident in neurological surgery in the OHSU School of Medicine. “It was quite similar to the imaging the Rochester group showed in mice.”
Clearing waste from the brain
Scientists believe this network of pathways effectively flushes the brain of metabolic wastes generated by its energy-intensive work. Wastes include proteins such as amyloid and tau, which have been shown to form clumps and tangles in brain images of patients with Alzheimer’s disease.
Emerging research suggests medications that may be useful, but much of the focus around the glymphatic system has revolved around lifestyle-based measures to improve the quality of sleep, such as maintaining a regular sleep schedule, establishing a relaxing routine, and avoiding screens in the bedroom before bed. Especially at night during deep sleep, researchers believe a well-functioning glymphatic system efficiently carries waste proteins toward veins exiting the brain.
“People thought these perivascular spaces were important, but it had never been proved,” Piantino said. “Now it has.”
The authors credited the late Justin Cetas, MD, PhD, who initiated the study as an OHSU neurosurgeon before leaving the university to become chair of neurological surgery at his alma mater, the University of Arizona Health Sciences Center in Tucson. He died in a motorcycle accident in 2022.
Credit: Darryl Leja National Human Genome Research Institute National Institutes Of Health
A blood test, performed when metastatic prostate cancer is first diagnosed, can predict which patients are likely to respond to treatment and survive the longest. It can help providers decide which patients should receive standard treatment versus who might stand to benefit from riskier, more aggressive new drug trials. The research, which forms part of a Phase III clinical trial, was just published in JAMA Network Open.
Once prostate cancer has metastasised and is no longer curable, systemic treatments are used to prolong survival as much as possible. Biomarkers that predict how patients will respond could allow for better personalisation of treatments, but they are few and far between.
A new study found that measuring circulating tumour cells (CTCs), rare cancer cells shed from tumours into the blood, is a reliable way to predict later treatment response and survival prospects. CTCs have been studied in prostate cancer before, but only in its later stages.
“No one, until now, has looked at whether CTC counts can be used right at the beginning, when a man first presents with metastatic prostate cancer, to tell us whether he’s going to live a long or short time, or whether or not he will progress with therapies,” said Amir Goldkorn, MD, lead author of the study and associate director of translational sciences at the USC Norris Comprehensive Cancer Center at the Keck School of Medicine of USC.
The research leveraged CellSearch (Menarini, Inc.), an FDA-cleared liquid biopsy technology at the Norris Comprehensive Cancer Center, to detect and measure CTCs in blood samples. Patients with more CTCs had shorter median survival lengths and a greater risk of death during the study period. Those with more CTCs also had less “progression-free survival,” which refers to the length of time when a patient’s disease is controlled by treatment without getting worse.
“You couldn’t tell these men apart when they walked through the door,” said Goldkorn, who is also a professor of medicine at the Keck School of Medicine. “All of their other variables and prognostic factors were seemingly the same, and yet they had very, very different outcomes over time.”
The researchers say that the CellSearch blood test, which is already widely available from commercial providers, can help quickly identify patients who are unlikely to respond to standard treatment options. Those men could benefit from a more intensive approach to therapy, including clinical trials of new drugs that may have more side effects but could improve survival in these high-risk patients.
Counting CTCs
The research was part of a phase 3 clinical trial of the NCI-funded SWOG Cancer Research Network, a group of more than 1300 institutions around the country that collaborate to study various cancers. Baseline blood samples from 503 patients with metastatic prostate cancer, who were participating in a new drug trial, were sent to the Keck School of Medicine team for analysis.
To analyze the blood samples, the researchers used the CellSearch platform at the Norris Comprehensive Cancer Center’s Liquid Biopsy Research Core, a facility that Goldkorn founded and directs. CellSearch uses immunomagnetic beads, antibodies attached to small magnetic particles, which bind to CTCs in the blood and pull them out to be detected and counted by specialised equipment.
Patients with five or more CTCs in their blood sample had the worst outcomes. Compared to patients with zero CTCs, they were 3.22 times as likely to die during the study period and 2.46 times as likely to have their cancer progress. They were only 0.26 times as likely to achieve a complete prostate-specific antigen (PSA) response, meaning they responded poorly to treatment.
Men with five or more CTCs had a median survival length of 27.9 months following the blood test, compared to 56.2 months for men with one to four CTCs and at least 78 months for men with zero CTCs. (Many patients in the latter group survived past the date of publication, so the median survival length could not yet be calculated.)
The bottom line: more CTCs meant that patients survived for less time, progressed much more quickly and were unlikely to respond to standard treatments.
Candidates for clinical trials
The new study shows that measuring CTC counts at the start of therapy can predict long-term survival rates, even in men who go on to receive many treatments for metastatic prostate cancer over a years-long period. That means the test can help identify men early on for trials of new and potentially more aggressive therapies.
“We want to enrich these clinical trials with men who need all that extra help – who really would benefit from three drugs versus just two, or from being on a new chemotherapy drug, even though it may have more side effects,” Goldkorn said.
Goldkorn and his team are now testing a new blood test that measures not just CTC counts, but also the molecular composition of CTCs and tumour DNA circulating in the blood, as well as other factors. Their goal is to create biomarkers with even more predictive power, which may ultimately help match patients with specific treatment options.
Promising findings by researchers at Baylor College of Medicine and collaborating institutions could lead to the development of a non-invasive stool test and a new therapy for endometriosis, a painful condition that affects nearly 200 million women worldwide. The study appeared in the journal Med.
“Endometriosis develops when lining inside the womb grows outside its normal location, for instance attached to surrounding intestine or the membrane lining the abdominal cavity. This typically causes bleeding, pain, inflammation and infertility,” said corresponding author Dr Rama Kommagani, associate professor in the Department of Pathology and Immunology at Baylor. “Generally, it takes approximately seven years to detect endometriosis and is often diagnosed incorrectly as a bowel condition. Thus, delayed diagnosis, together with the current use of invasive diagnostic procedures and ineffective treatments underscore the need for improvements in the management of endometriosis.”
“Our previous studies in mice have shown that the microbiome, the communities of bacteria living in the body, or their metabolites, the products they produce, can contribute to endometriosis progression,” Kommagani said. “In the current study, we took a closer look at the role of the microbiome in endometriosis by comparing the bacteria and metabolites present in stools of women with the condition with those of healthy women. We discovered significant differences between them.”
The findings suggested that stool metabolites found in women with endometriosis could be the basis for a non-invasive diagnostic test as well as a potential strategy to reduce disease progression.
The researchers discovered a combination of bacterial metabolites that is unique to endometriosis. Among them is the metabolite called 4-hydroxyindole. “This compound is produced by ‘good bacteria,’ but there is less of it in women with endometriosis than in women without the condition,” said first author Dr Chandni Talwar, postdoctoral associate in Kommagani’s lab.
“These findings are very exciting,” Talwar said. “There are studies in animal models of the disease that have shown specific bacterial metabolite signatures associated with endometriosis. Our study is the first to discover a unique metabolite profile linked to human endometriosis, which brings us closer to better understanding the human condition and potentially identifying better ways to manage it.”
Furthermore, extensive studies also showed that administering 4-hydroxyindole to animal models of the disease prevented the initiation and progression of endometriosis-associated inflammation and pain.
“Interestingly, our findings also may have implications for another condition. The metabolite profile we identified in endometriosis is similar to that observed in inflammatory bowel disease (IBD), revealing intriguing connections between these two conditions,” Kommagani said. “Our findings support a role for the microbiome in endometriosis and IBD.”
The researchers are continuing their work toward the development of a non-invasive stool test for endometriosis. They are also conducting the necessary studies to evaluate the safety and efficacy of 4-hydroxyindole as a potential treatment for this condition.
An ultrasound test that detected 96% of ovarian cancers in postmenopausal women should replace current standard of care test in the UK according to a new study.
In a paper published in Lancet Oncology, research led by Professor Sudha Sundar from the University of Birmingham compared all currently available tests to diagnose ovarian cancer in postmenopausal women head-to-head in a high-quality diagnostic test accuracy study.
Of the six diagnostic tests investigated, the IOTA ADNEX model which looks at ultrasound features (how the lump looked like on ultrasound) had the best accuracy of all and could detect up to 96% of women with ovarian cancer.
The ultrasound test outperforms the current standard of care in the UK significantly and so the researchers recommend that the IOTA ultrasound ADNEX model should replace the current standard of care test called risk of malignancy (RMI1) test in the UK which identifies 83% of ovarian cancers.
Sudha Sundar, Professor of Gynaecological Cancer at the University of Birmingham and consultant in gynaecological cancer surgery at Sandwell and West Birmingham NHS Trust said:
“This is the first time that a head-to-head study of all available ovarian cancer tests have been done in the same population. Here we studied their use with symptomatic, postmenopausal women who are most at risk of this cancer. Our trial found that the IOTA ADNEX ultrasound protocol had highest sensitivity for detecting ovarian cancer compared to the standard of care and other test.
“The ultrasound test also performs well when delivered by a trained sonographer who have received specific training and certification and quality assurance, and as the vast majority of ultrasound scans are performed by sonographers it is important that a new standard is able to be delivered by as many clinical professionals as possible.
“We found that the higher sensitivity of the IOTA ADNEX model is likely to lead to some women who don’t have cancer also being flagged up as having a higher risk of cancer. We however did discuss this extensively with patients, cancer charity Target ovarian cancer and NHS experts who all agreed that in postmenopausal women who are at higher risk of ovarian cancer, picking up more women with cancer would benefit women overall.”
The research team note that the IOTA ADNEX model achieved 96% accuracy when delivered by NHS sonographers who were appropriately trained and received quality assurance. As most scans worldwide are carried out by sonographers rather than gynaecologists, introductory free online resources have been created by the researchers for NHS staff to undergo the specialist ultrasound training and get certification and quality assurance.
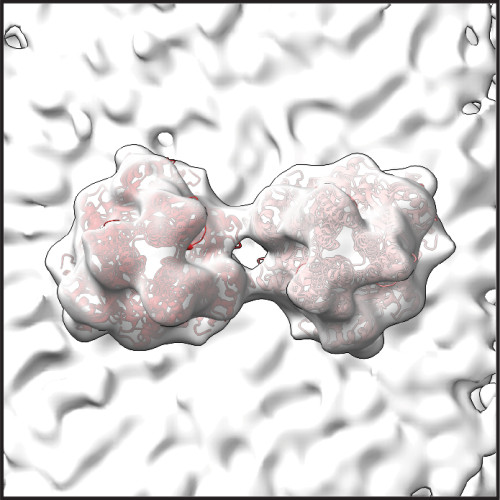
The complex shape of respiratory syncytial virus is one hurdle limiting the development of treatments for an infection that leads to hospitalisation or worse. New images of the virus published in Nature from researchers at the University of Wisconsin–Madison may hold the key to preventing or slowing RSV infections.
RSV is of greatest concern in young children, the elderly and adults at high risk for respiratory complications. Yet unlike the flu and other common, communicable respiratory illnesses that annually sweep through schools, there are few options for fighting RSV. In the US, prophylactic treatments are available for young children, and existing vaccines are approved only for pregnant women and the elderly.
The virus’s structure, which consists of tiny, bending filaments, have eluded researchers. This has made it difficult to identify key drug targets, including viral components that are conserved across related viruses.
RSV F proteins, shown in this image created by University of Wisconsin–Madison researchers using a technique called cryo-electron tomography, may make RSV more potent by keeping it from infecting cells prematurely. Image by Wright Lab, UW–Madison
“There are a number of viruses related to RSV that are also significant human pathogens, including measles,” says Elizabeth Wright, a UW–Madison biochemistry professor. “What we know about related viruses gives us clues about RSV protein structures, but to identify drug targets we need a closer look at RSV proteins that are intimately associated with the membranes of host cells.”
Using an imaging technique called cryo-electron tomography, Wright and her team have now revealed details of molecules and structures essential to RSV’s form and function. They published their findings recently in Nature.
Cryo-ET freezes viral particles or other molecules at ultracold temperatures, stopping biological processes in action. This allows researchers to examine the structures of organisms, cells and organelles, and viruses and capture small-scale images of structures frozen in time. Flash-freeze many RSV particles, and cryo-ET imaging will capture (nearly) all the virus’s possible configurations from many different angles. These 2D images are combined to produce a representation of the virus’s 3D structures at high resolutions – even at the level of individual atoms.
Wright’s recent study produced high-resolution images detailing the structure of two RSV proteins, RSV M protein and RSV F protein, that are crucial to the interaction between the virus and the host cell membrane. Both proteins are also present in related viruses.
RSV M protein interacts with host cell membranes, holding together the virus’s filamentous structure and coordinating viral components and other proteins – including RSV F proteins. RSV F proteins sit on the viral surface, ready to engage with host cell receptors and regulate the virus’s fusion and entry into the host cell. The scientists’ images reveal that in RSV, two F proteins come together to form a more stable unit. Wright says that this association may prevent the F proteins from prematurely infecting the host cell.
“Our primary findings reveal structural details that allow us to better understand not only how the protein regulates assembly of viral particles, but also the coordination of proteins that enable the virus to be infectious,” says Wright.
The scientists believe that F protein pairs may be a key to destabilising the virus before it is ready to infect its next host, making pairs of F proteins a possible target for future drug development. They will continue to explore how RSV proteins interact with each other to cause infection.
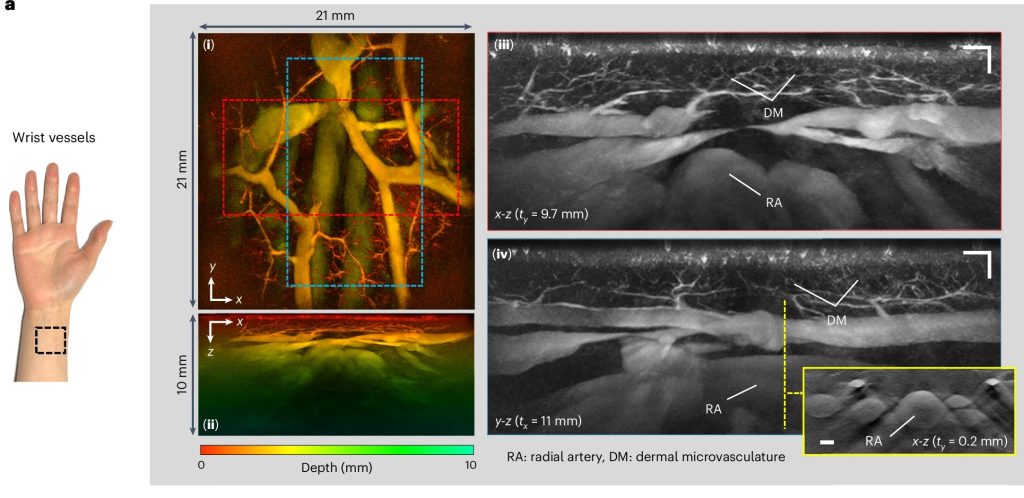
PAT images of wrist vasculature acquired in high-resolution scan mode. Wrist region, (i) x-y and (ii) x-z depth-to-colour encoded MIPs, (iii) x-z and (iv) y-z greyscale MIP slices of regions indicated by dashed red and blue rectangles in (i) showing fine dermal microvasculature (DM), radial artery (RA) and large wrist veins. Inset: x-z greyscale MIP showing cross-sectional view of the radial artery and adjacent veins in the plane indicated by the dashed yellow line in (iv). Huynh et al., Nature Communications, 2024.
A new hand-held scanner developed by UCL researchers and tested in a series of clinical trials on UCLH patients can generate highly detailed 3D photoacoustic images in just seconds, paving the way for their use in a clinical setting for the first time and offering the potential for earlier disease diagnosis.
In the study, published in Nature Biomedical Engineering, the UCL and UCLH team show their technology can deliver photoacoustic tomography (PAT) imaging scans to doctors in real time, providing them with accurate and intricate images of blood vessels, helping inform patient care.
Photoacoustic tomography imaging uses laser-generated ultrasound waves to visualise subtle changes (an early marker of disease) in the sub-millimetre-scale veins and arteries up to 15mm deep in human tissues.
However, up until now, existing PAT technology has been too slow to produce high-enough quality 3D images for use by clinicians.
The older PAT scanners took more than five minutes to take an image – by reducing that time to a few seconds or less, image quality is much improved and far more suitable for people who are frail or poorly.
The researchers say the new scanner could help to diagnose cancer, cardiovascular disease and arthritis in three to five years’ time, subject to further testing.
In this study, the team tested the scanner during pre-clinical tests on 10 UCLH patients with type-2 diabetes, rheumatoid arthritis or breast cancer, along with seven healthy volunteers. They also compared the PAT scans to regular clinical scans taken at UCLH. Larger scale trials of the device are ongoing at UCLH and UCL.
In three patients with type-2 diabetes, the scanner was able to produce detailed 3D images of the microvasculature in the feet, highlighting deformities and structural changes in the vessels. The scanner was also used to visualise the skin inflammation linked to breast cancer.
UCLH consultant radiologist Andrew Plumb, a senior author of the study and Chief Investigator of the clinical PAT studies, said: “One of the complications often suffered by people with diabetes is low blood flow in the extremities, such as the feet and lower legs, due to damage to the tiny blood vessels in these areas. But until now we haven’t been able to see exactly what is happening to cause this damage or characterise how it develops.
“In one of our patients, we could see smooth, uniform vessels in the left foot and deformed, squiggly vessels in the same region of the right foot, indicative of problems that may lead to tissue damage in future. Photoacoustic imaging could give us much more detailed information to facilitate early diagnosis, as well as better understand disease progression more generally.” Dr Plumb is also Associate Professor of Medical Imaging at UCL.
Patients were identified and recruited from a number of clinics at UCLH, including consultant rheumatologist Madhura Castelino, consultant interventional radiologist Conrad von Stempel and research staff Katerina Soteriou and Antonia Yeung who co-ordinated safe, timely scanning at UCLH and UCL on the new PAT scanner.
UCL Professor of Biomedical Photoacoustics Paul Beard, corresponding author, said: “We’ve come a long way with photoacoustic imaging in recent years, but there were still barriers to using it in the clinic.
“The breakthrough in this study is the acceleration in the time it takes to acquire images, which is between 100 and 1000 times faster than previous scanners.
“This speed avoids motion-induced blurring, providing highly-detailed images of a quality that no other scanner can provide. It also means that rather than taking five minutes or longer, images can be acquired in real time, making it possible to visualise dynamic physiological events.
“These technical advances make the system suitable for clinical use for the first time, allowing us to look at aspects of human biology and disease that we haven’t been able to before.
“Now more research is needed with larger groups of patients to confirm our findings.”
Professor Beard added that a key potential use for the new scanner was to assess inflammatory arthritis, which requires scanning all 20 finger joints in both hands. With the new scanner, this can be done in a few minutes – older PAT scanners take nearly an hour, which is too long for elderly, frail patients, he said.
Over half of people with iron deficiency were found to still have low iron levels three years after diagnosis, and among patients whose condition was effectively treated within that timeframe, they faced longer-than-expected delays, pointing to substantial gaps in appropriate recognition and efficient treatment of the condition, according to a study published in Blood Advances.
Iron deficiency is common, and affecting up to 40% of adolescents and young women. Previous work reported that up to 70% of cases go undiagnosed in high-risk populations, such as those with bleeding disorders, issues with malabsorption, or women who menstruate.
“Iron deficiency is probably a bigger problem than we realise. I’ve seen a lot of cases where people don’t have anaemia, but they are walking around with very little to no iron in their body and it can have a big impact on how people feel in their day-to-day life,” said Jacob Cogan, MD, assistant professor of medicine at the University of Minnesota and the study’s lead author. “Iron deficiency can be challenging to diagnose, but it’s easy to treat. Our findings underscore the need for a more coordinated effort to recognise and treat iron deficiency to help improve quality of life.”
If untreated, low iron stores can lead to mood changes, fatigue, hair loss, exercise intolerance, and eventually anaemia. The condition is generally first treated with oral iron supplementation, and if low iron levels persist after a few months or the patient reports side effects, intravenous (IV) iron is started.
For this study, the researchers retrospectively analysed medical records from one of Minnesota’s largest health system database and identified 13 084 adults with a laboratory diagnosis of iron deficiency (defined as a ferritin value of 25ng/mL, with and without anaemia) between 2010 and 2020 who had available follow-up data for three years.
In the study, iron deficiency was d or less. Patients had to have at least two ferritin values – one initial value and at least one more within the three-year study period. Adequate treatment and resolution was defined as a subsequent ferritin value of at least 50ng/mL. Most patients received some form of treatment, consistent across sex.
Of the 13,084 patients included in the study, 5,485 (42%) patients had normal iron levels within three years of diagnosis, while 7,599 (58%) had persisting iron deficiency based on low ferritin levels. Only 7% of patients had their iron levels return back to normal within the first year of diagnosis.
Factors associated with a higher likelihood of getting iron levels back to normal included older age (age 60 and up), male sex, Medicare insurance, and treatment with IV iron alone. Additionally, compared with patients who were still iron deficient, those whose condition was resolved had more follow-up blood work to check ferritin values (six vs four ferritin tests). Of note, younger patients, females, and Black individuals were most likely to remain iron deficient or experience longer lags in getting their iron stores back to a healthy level.
Even among patients whose iron levels were restored to normal during the study duration, it took nearly two years (the median time to resolution was 1.9 years), which researchers say is longer than expected and signals missed opportunities to more effectively manage the condition. While there was no data to look at whether anaemia iron deficiency was more apt to be treated, Dr Cogan says it’s reasonable to think this might be the case as iron deficiency without anaemia is harder to recognise.
“Two years is too long and well beyond the timeframe within which iron deficiency should be able to be sufficiently treated and resolved [with oral or IV treatments],” said Dr Cogan. “The numbers are pretty striking and suggest a need to put systems in place to better identify patients and treat them more efficiently.”
As with trends showing persisting iron deficiency, Dr Cogan attributes the delays in resolution to the diagnosis either being missed or not treated to resolution. He added that there is a clear need for education about non-anaemic iron deficiency and who is at high risk, more universal agreement on the best ferritin cut off for diagnosis, and efforts to create an iron deficiency clinic or pathway to “assess and treat patients more efficiently and get people feeling better faster.”
The study was limited by its reliance on EMR data and retrospective nature, which prevented researchers from determining why ferritin tests were ordered for patients or the cause of their iron deficiency.