A systematic review published in the Canadian Medical Association Journal revealed that while people had good odds of recovering from short term back pain, but if it becomes persistent, then the chances of recovery are greatly reduced. This has important implications for the treatment of chronic back pain, as it points to the pain from the original injury being replaced by pain hypersensitivity.
“The good news is that most episodes of back pain recover, and this is the case even if you have already had back pain for a couple of months,” University of South Australia Professor Lorimer Moseley says.
“The bad news is that once you have had back pain for more than a few months, the chance of recovery is much lower. This reminds us that although nearly everyone experiences back pain, some people do better than others, but we don’t completely understand why.”
The systematic review and meta-analysis, conducted by an international team of researchers, included 95 studies with the goal of understanding the clinical course of acute (< 6 weeks), subacute (six to less than 12 weeks) and persistent (12 to less than 52 weeks) low back pain.
For people with new back pain, pain and mobility problems lessened significantly in the first six weeks, but then recovery slowed.
This study filled a gap in a 2012 paper from the same research team, with new findings showing that many people with persistent low back pain (more than 12 weeks) continue to have moderate-to-high levels of pain and disability.
“These findings make it clear that back pain can persist even when the initial injury has healed,” Prof Moseley says.
“In these situations, back pain is associated with pain system hypersensitivity, not ongoing back injury. This means that if you have chronic back pain – back pain on most days for more than a few months – then it’s time to take a new approach to getting better.”
He notes that there are new treatments based on training both the brain and body that “focus on first understanding that chronic back pain is not a simple problem, which is why it does not have a simple solution, and then on slowly reducing pain system sensitivity while increasing your function and participation in meaningful activities.”
The authors state that identifying slowed recovery in people with subacute low back pain is important so that care can be escalated and the likelihood of persistent pain reduced.
Further research into treatments is needed to help address this common and debilitating condition, and to better understand it in people younger than 18 and older than 60 years.
Colourised electron micrograph image of a macrophage. Credit: NIH
Scientists have created a new treatment for traumatic brain injury (TBI). The new approach leverages macrophages, which can increase or decrease inflammation in response to infection and injury. The team attached “backpacks” containing anti-inflammatory molecules directly to the macrophages. These molecules kept the cells in an anti-inflammatory state when they arrived at the injury site in the brain, enabling them to reduce local inflammation and mitigate the damage caused. The research is reported in PNAS Nexus.
“Every year, millions of people suffer from a TBI, but there is currently no treatment beyond managing symptoms. We have applied our cellular backpack technology – which we previously used to improve macrophages’ inflammatory response to cancerous tumours – to deliver localised anti-inflammatory treatment in the brain, which helps mitigate the cascade of runaway inflammation that causes tissue damage and death in a human-relevant model,” said senior author Samir Mitragotri, PhD, in whose lab the research was performed.
Stopping a runaway inflammation train
There is currently no treatment for the damage caused to brain tissue during a traumatic brain injury (TBI), beyond managing a patient’s symptoms. One of the main drivers of TBI-caused damage is a runaway inflammatory cascade in the brain.
As cells die from the impact, they release a cocktail of pro-inflammatory cytokine molecules that attract immune cells to clean up the damage. But the same cytokine molecules can also disrupt the blood-brain barrier, which causes blood to leak into the brain. Blood accumulation in the brain causes swelling, impaired oxygen delivery, and increased inflammation, and creates a vicious cycle of bleeding and damage that drives even more cell death.
The Mitragotri lab saw an opportunity in this problem.
“It’s generally believed anti-inflammatory therapies can be effective for treating TBI, but so far, none of them have proven effective clinically. Our previous work with macrophages has shown us that we can use our backpack technology to effectively steer their behaviour when they arrive at the injury site. Since these cells are already active players in the body’s natural immune response to a TBI, we had a hunch we could augment that pre-existing biology to reduce the initial damage,” said co-first author Rick Liao, Ph.D., a Postdoctoral Fellow at the Wyss Institute and SEAS.
“Body, heal thyself”…with backpacks
Macrophages are very malleable cells and can “switch” between pro-inflammatory and anti-inflammatory states. While the team’s previous work in cancer had been focused on keeping macrophages in a pro-inflammatory state when they arrive at the inflammation-reducing microenvironment of a tumour, this new project would be trying to do the opposite: keep the macrophages “calm” in the inflammation-riddled setting of a brain injury.
To do so, they used a disc-shaped “backpack” they had previously designed to treat multiple sclerosis that contained layers of two anti-inflammatory molecules: dexamethasone, a steroid, and interleukin-4, a cytokine that encourages macrophages to adopt an anti-inflammatory state. They then incubated these microparticles with both human and pig macrophages in vitro and saw that the backpacks stably stuck to the cells without causing any negative effect. They also observed that application of their backpacks decreased the expression of pro-inflammatory biomarkers and increased the expression of anti-inflammatory biomarkers, retaining the pig macrophages in a healing state.
But to prove that this shift would work in the body, they had to test the backpack-bearing macrophages in vivo. They chose pigs as their model organism because their brains’ structures and responses to injury more closely mimic those of humans than mice.
“Probably our biggest challenge in this project was scaling up production to match what we needed to run the experiments. Our previous studies were done in rodents, which required about two million macrophages and four million backpacks administered per subject. For the porcine study, we needed 100 million macrophages and 200 million backpacks per subject – on the scale of what would be administered in humans – and lots of helping hands,” said co-first author Neha Kapate, PhD, a Postdoctoral Fellow at the Wyss Institute and SEAS.
Once they had generated enough backpack-wearing porcine macrophages, they infused them into the pigs’ bloodstreams four hours after a TBI. Seven days later, they analysed the animals’ brains. Pigs that had received the macrophage treatment showed a high concentration of the cells in the area immediately surrounding the injury site, their lesions were 56% smaller, and there was significantly less haemorrhaging than in untreated animals.
Local immune cells also displayed a lower amount of a pro-inflammatory activation marker called CD80, indicating that the macrophages had accomplished their damage control by reducing inflammation in the brain. Corroborating that data, the levels of two soluble biomarkers for inflammation in the blood and cerebrospinal fluid were lower in treated animals than in untreated animals. The macrophage treatment also did not cause any negative effects.
The team plans to conduct future studies that focus on elucidating exactly how their anti-inflammatory macrophage therapy affects the blood-brain barrier’s integrity to prevent bleeding, which could also hold promise for treating other conditions like hemorrhagic strokes.
“Macrophages’ susceptibility to their local environment has historically prevented scientists from taking full advantage of their immune-modulating capabilities. This impressive study describes a truly novel and potentially powerful macrophage-based therapy for treating the inflammation that is the root cause of so many human afflictions in an effective and non-invasive way that works with biology rather than against it,” said Wyss Founding Director Donald Ingber, MD, PhD.
In the event of an accident or an attack, members of the public can save lives by performing first aid measures until the arrival of emergency medical services. But those people willing and able to serve as first responders will also need access to first aid equipment.
“There must also be certain equipment available to manage major bleeding. The question then is where this equipment should be placed, so that people who want to help can quickly access bleeding control kits,” says Carl-Oscar Jonson, adjunct senior associate professor at the Department of Biomedical and Clinical Sciences at Linköping University and head of research at the Center for Disaster Medicine and Traumatology in Linköping.
The first recommendations
Until now, there have been no guidelines for where such bleeding control kits should be located to ensure maximal utility. The current study, published in the journal Disaster Medicine and Public Health Preparedness, now contributes research-based recommendations.
“We found that the largest number of lives saved correlated with bleeding control kits being placed in two or more locations on the premises, but most importantly they shouldn’t be placed at entrances. We also concluded that the equipment must be accessible within 90 seconds’ walking distance,” says Anna-Maria Grönbäck, doctoral student at the Department of Science and Technology at Linköping University, who was involved in developing the simulation.
This means that bleeding control kits should not be placed at entrances, which is often the case with automated external defibrillators (AEDs). The reason for this is that they may be difficult to reach in a situation where many people have to be evacuated at once, such as in the case of attack or major accident. According to attack statistics, roughly 20 injured people will need first aid including a bleeding control kit each. It may be helpful to locate bleeding control kits in the same places as clearly marked AEDs, as long as not located at the entrances.
Bomb consequences simulated
The recommendations are based on conclusions reached by the research team by developing a computer-based simulation of an explosion in a large shopping centre with thousands of simultaneous visitors. In their simulation, the researchers have looked at what happens right after an explosion. The majority of the simulated people try to get out of the premises and move towards the exits. Simulated people close to the blast suffer varying degrees of injury and start bleeding.
In the simulation, some individuals help those injured by applying direct pressure to reduce bleeding, or by trying to find equipment. It is a race against time. Depending on how long it takes to get the equipment, the simulated casualty may die from blood loss.
To find the best strategy for the placement of bleeding control kits, the researchers tested four different scenarios in their simulation. They weighed together the outcomes of the many simulated courses of events for each scenario and compared them to understand which placement of equipment saved the largest number of lives.
Image of an astrocyte, a subtype of glial cells. Glial cells are the most common cell in the brain.
Credit: Pasca Lab, Stanford University
NIH support from: NINDS, NIMH, NIGMS, NCATS
A new study published in PNAS Nexus provides a better understanding of how the brain responds to injuries. Researchers at the George Washington University discovered that a protein called Snail plays a key role in coordinating the response of brain cells after an injury.
The study shows that after an injury to the central nervous system (CNS), a group of localised cells start to produce Snail, a transcription factor or protein that has been implicated in the repair process. The GW researchers show that changing how much Snail is produced can significantly affect whether the injury starts to heal efficiently or whether there is additional damage.
“Our findings reveal the intricate ways the brain responds to injuries,” said senior author Robert Miller, the Vivian Gill Distinguished Research Professor and Vice Dean of the GW School of Medicine and Health Sciences.
“Snail appears to be a key player in coordinating these responses, opening up promising possibilities for treatments that can minimise damage and enhance recovery from neurological injuries.”
This study identified for the first time a special group of microglial-like cells that produce Snail. Microglial cells are found in the central nervous system. The researchers found that lowering the amount of Snail produced after an injury results in inflammation and increased cell death. During this process, the injury worsens and there are fewer connections or synapses between brain cells. In contrast, when Snail levels are increased the outcome of brain injury improves-suggesting this protein can help limit the spread of injury-induced damage.
The research raises questions about whether an experimental drug that affects Snail production could be used to limit the damage incurred after someone suffers a stroke or has been injured in an accident, Miller said.
Additional studies must be done to show that increasing Snail production could curtail injury or even promote healing of the brain.
Miller and his team also plan to study the regulation of Snail in diseases like multiple sclerosis, a disease resulting in damage to the myelin nerve sheath. If drugs targeting Snail could be used to stop that damage, many of the future symptoms of this disease could be eased, he says.
But researchers have years of work to do before new drugs targeting Snail can be tested in clinical trials. The payoff ultimately might be drugs that can lead to accelerated healing for stroke damage, head wounds and even neurodegenerative diseases like dementia.
A study by researchers at the South African Medical Research Council (MRC) recommends that the murder of men in South Africa deserves an urgent national response.
Richard Matzopoulos of the MRC’s Burden of Disease Unit and his team, which included scientists from the UCT School of Public Health, studied postmortem reports from 2017 to compare murders of women and men. Among the factors looked at were cause of death, age, geographic location and whether alcohol played a role.
The study, published in PLOS Global Public Health, found that 87% of people murdered in 2017 were men. The authors note similar percentages in 2009 (86%) and 2000 (84%).
According to the researchers, this is the first study on male murders in South Africa. Previous studies have focused mainly on femicide (the killing of women). The study focused on 2017 to coincide with the third national femicide study (previous femicide studies were in 2000 and 2009).
The researchers faced challenges getting the paper published in a peer-reviewed journal. Dr Morna Cornell, one of the study’s authors, told GroundUp that men’s health is generally understudied. Cornell believes “we are living in an outdated paradigm which regards all men as powerful and able to navigate health systems etc, and therefore less deserving of care”.
The most common causes of death among male murder victims were sharp stabbings and shootings. For people between the ages of 15 and 44, rates of male murders were more than eight times higher than female murders. The Western Cape has the biggest gap between male and female victims: for every female killed, 11.4 men were killed.
Male murders peaked over December and weekends, suggesting the role alcohol plays.
The study aims to challenge the idea that men are “invulnerable”.
“The fact that men are both perpetrators and victims of homicides masks the strong evidence that men are extremely vulnerable in many contexts,” the study reads.
Murder in South Africa is concentrated in poor neighbourhoods where the effects of poverty and inequality are most significant. According to the study, “violence has been normalised as a frequent feature of civil protest and political discourse”.
High levels of firearm ownership and imprisonment also contribute to violence in South Africa.
“Men are socialised into coping by externalising through anger, irritability, violence against intimate partners and others, and increased engagement in risk-taking behaviours. This, alongside the high levels of violence to which males are exposed across [life], [causes] a continuous, and often intergenerational cycle of violence,” the study says.
While the study acknowledges that “violence against women is endemic in South Africa, with rates almost six times the global figures”, it argues that “men’s disproportionate burden of homicide has not resulted in targeted, meaningful prevention”.
Interventions recommended by the researchers include stricter control of alcohol and firearms, programs to address societal norms that drive physical violence, and efforts to overcome the root causes of poverty and inequality.
Professor Richard Matzopolous, the main author of the study, told GroundUp that more research is needed to understand risks and interventions, especially in a South African context.
“Phase 2 of this study will explore victim/perpetrator and situational contexts,” said Matzopolous.
A major clinical trial has found that vitamin D supplements do not increase bone strength or prevent bone fractures in children with vitamin D deficiency. The findings, published in Lancet Diabetes & Endocrinology, challenge widely held perceptions relating to the effects of vitamin D on bone health.
Around one-third of children have at least one fracture before the age of 18. This is a major global health issue, as childhood fractures can lead to life years of disability and/or poor quality of life. The potential for vitamin D supplements to improve bone strength has attracted growing interest in recent years, based on vitamin D’s role in promoting bone mineralisation. But there have been no clinical trials to test whether vitamin D supplements can prevent bone fractures in children.
Working with partners in Mongolia, a setting with a particularly high fracture burden and where vitamin D deficiency is highly prevalent, researchers from led by Queen Mary University of London and the Harvard T.H. Chan School of Public Health conducted a clinical trial to determine if vitamin D supplementation would decrease risk of bone fractures or increase bone strength in schoolchildren.
This study is also the largest randomised controlled trial of vitamin D supplementation ever conducted in children. Over the course of three years, 8851 schoolchildren aged 6-13 living in Mongolia received a weekly oral dose of vitamin D supplementation.
Testing revealed that 95.5% of participants had vitamin D deficiency at baseline, and study supplements were highly effective in boosting vitamin D levels into the normal range. No effect was seen on fracture risk or on bone strength, measured in a subset of 1438 participants using quantitative ultrasound.
The trial findings are likely to prompt scientists, doctors and public health specialists to re-consider the effects of vitamin D supplements on bone health.
Dr Ganmaa Davaasambuu, Associate Professor at the Harvard T.H. Chan School of Public Health, said:
“The absence of any effect of sustained, generous vitamin D supplementation on fracture risk or bone strength in vitamin D deficient children is striking. In adults, vitamin D supplementation works best for fracture prevention when calcium is given at the same time – so the fact that we did not offer calcium alongside vitamin D to trial participants may explain the null findings from this study.”
Professor Adrian Martineau, Lead of the Centre for Immunobiology at Queen Mary University of London, added:
“It is also important to note that children who were found to have rickets during screening for the trial were excluded from participation, as it would not have been ethical to offer them placebo (dummy medication). Thus, our findings only have relevance for children with low vitamin D status who have not developed bone complications. The importance of adequate vitamin D intake for prevention of rickets should not be ignored, and UK government guidance recommending a daily intake of 400 IU vitamin D remains important and should still be followed.”
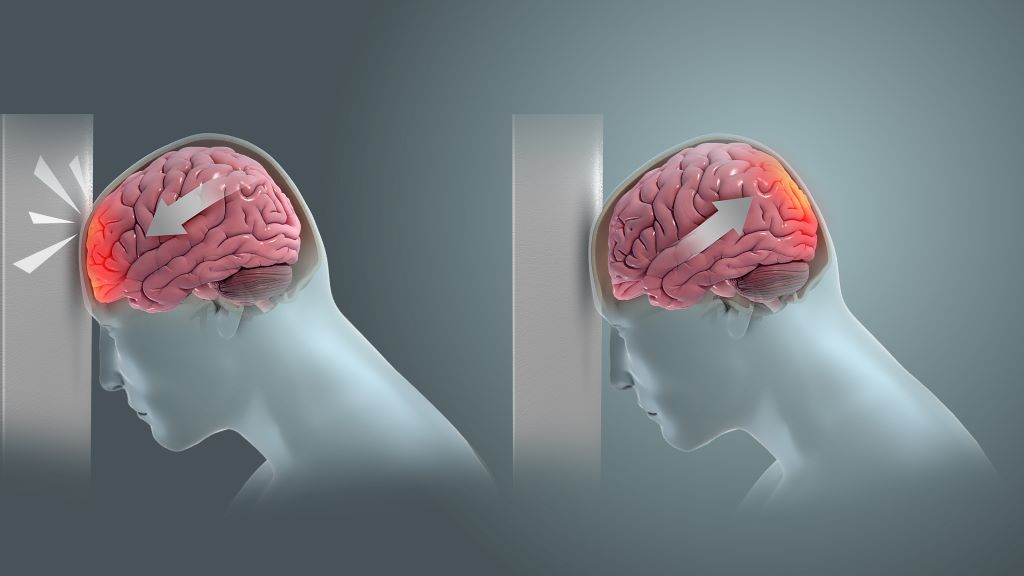
Coup and contrecoup brain injury. Credit: Scientific Animations CC4.0
Recent research has indicated that acoustic stimulation of the brain may ease persistent symptoms in individuals who experienced mild traumatic brain injury in the past.
The study, which appears in Annals of Clinical and Translational Neurology, included 106 military service members, veterans, or their spouses with persistent symptoms after mild traumatic brain injury sustained three months to 10 years ago. Participants were randomised 1:1 to receive either 10 sessions of engineered tones linked to brainwaves (intervention), or random engineered tones not linked to brainwaves (sham control). All participants rested comfortably in the dark in a ‘zero-gravity’ chair, eyes closed and listening to the computer-generated tones via earbud-style headphones. The primary outcome was change in symptom scores, with secondary outcomes of heart rate variability and self-reported measures of sleep, mood, and anxiety.
Among all study participants, symptom scores clinically and statistically improved compared with baseline, with benefits largely sustained at three months and six months; however, there were no significant differences between the intervention and control groups. Similar patterns were observed for secondary outcomes.
The results indicate that although acoustic stimulation is associated with marked improvement in postconcussive symptoms, listening to acoustic stimulation based on brain electrical activity, as it was delivered in this study, may not improve symptoms, brain function, or heart rate variability more than randomly generated, computer engineered acoustic stimulation.
“Postconcussive symptoms have proven very difficult to treat, and the degree of improvement seen in this study is virtually unheard of, though further research is needed to identify what elements are key to its success,” said corresponding author Michael J. Roy, MD, MPH, of Uniformed Services University and the Walter Reed National Military Medical Center, in Bethesda.
Posttraumatic stress disorder (PTSD) is a debilitating condition that arises after experiencing traumatic events. While many people experience trauma, only about 25–35% of them develop PTSD. Understanding the factors that make certain individuals more susceptible is crucial for both prevention and treatment.
A new study led by Carmen Sandi and Simone Astori at EPFL now reveals how the development of PTSD is influenced by glucocorticoids, which are stress hormones such as cortisol. The work, which is published in Biological Psychiatry, provides significant insights into the behavioural and biological traits associated with PTSD vulnerability.
“There are considerable differences in the levels of glucocorticoids that individuals release to the bloodstream when stressed,” says Carmen Sandi. “Low glucocorticoid levels are frequently observed in PTSD patients following trauma exposure and were initially suspected to be a consequence of trauma exposure.”
She continues: “The possibility that this could be a trait constituting a pre-existing PTSD risk factor has been an outstanding open question for many years, but tackling it has been challenging due to the difficulties of both collecting biological measures before trauma exposure, and having access to relevant animal models in which the causal role of these traits can be investigated.”
To explore how a reduced hormonal response to stress might be linked to PTSD symptoms, the researchers used a genetically selected rat model that mimics people with blunted responses to cortisol. To do this, the team used MRI scans to measure the volume of different brain regions, trained rats to associate a cue with fear, recorded their sleep patterns, and measured their brain activity.
By combining these methods, the researchers discovered that a blunted responsiveness to glucocorticoids led to a “correlated multi-trait response” that includes impaired fear extinction (in males), reduced hippocampal volume, and rapid-eye movement sleep disturbances.
To explain the terms: Fear extinction is a process by which a conditioned fear response diminishes over time; problems with fear extinction are a hallmark of PTSD. Rapid-eye movement is crucial for memory consolidation, and disturbances in this type of sleep pattern have long been associated with PTSD.
But the study didn’t end there: the researchers treated the rats with the equivalent of human cognitive and behavioral therapy to reduce their learned fears. After that, they gave the rats corticosterone. As a result, both excessive fear and disturbances in rapid-eye movement sleep receded. Not only that, but the increased levels of the stress-related neurotransmitter norepinephrine in the brain also returned to normal.
“Our study provides causal evidence of a direct implication of low glucocorticoid responsiveness in the development of PTSD symptomatology following exposure to traumatic experiences, i.e., impaired fear extinction,” says Carmen Sandi. “In addition, it shows that low glucocorticoids are causally implicated in the determination of other risk factors and symptoms that were until now only independently related to PTSD.”
Silvia Monari, the study’s first author, adds: “In a nutshell, we present mechanistic evidence – previously missing – that having low glucocorticoids such as cortisol in humans is a condition for causally predisposed individuals to present all to-date vulnerability factors for developing PTSD, and causally involved in deficits to extinguish traumatic memories.”
Researchers at the Institute of Basic Science (IBS) in South Korea have developed a novel approach to healing muscle injury by employing an ‘injectable tissue prosthesis’ in the form of conductive hydrogels and combining it with a robot-assisted rehabilitation system. They describe their research in a recent publication in the journal Nature.
A large wound such as a shark bite, with the loss of muscle and nerve in the wound cavity, results in a complete loss of motor/sensor function in the leg. If left untreated, such severe muscle damage would result in permanent loss of function and disability.
Traditional rehabilitation methods for these kinds of muscle injuries have long sought an efficient closed-loop gait rehabilitation system that merges lightweight exoskeletons and wearable/implantable devices. Such assistive prosthetic system is required to aid the patients through the process of recovering sensory and motor functions linked to nerve and muscle damage.
Unfortunately, the mechanical properties and rigid nature of existing electronic materials render them incompatible with soft tissues. This leads to friction and potential inflammation, stalling patient rehabilitation.
To overcome these limitations, the IBS researchers turned to a material commonly used as a wrinkle-smoothing filler, called hyaluronic acid. Using this substance, an injectable hydrogel was developed for ’tissue prostheses’, which can temporarily fill the gap of the missing muscle/nerve tissues while it regenerates. The injectable nature of this material gives it a significant advantage over traditional bioelectronic devices, which are unsuitable for narrow, deep, or small areas, and necessitate invasive surgeries.
Thanks to its highly ’tissue-like’ properties, this hydrogel seamlessly interfaces with biological tissues and can be easily administered to hard-to-reach body areas without surgery. The reversible and irreversible crosslinks within the hydrogel adapt to high shear stress during injection, ensuring excellent mechanical stability. This hydrogel also incorporates gold nanoparticles, which gives it decent electrical properties. Its conductive nature allows for the effective transmission of electrophysiological signals between the two ends of injured tissues. In addition, the hydrogel is biodegradable, removing the need for additional surgery.
With mechanical properties akin to natural tissues, exceptional tissue adhesion, and injectable characteristics, researchers believe this material offers a novel approach to rehabilitation.
Next, the researchers put this novel idea to the test in rodent models. To simulate volumetric muscle loss injury, a large chunk of muscle has been removed from the hind legs of these animals. By injecting the hydrogel and implanting the two kinds of stretchable tissue-interfacing devices for electrical sensing and stimulation, the researchers were able to improve the gait in the ‘injured’ rodents. The hydrogel prosthetics were combined with robot assistance, guided by muscle electromyography signals. Together, the two helped enhance the animal’s gait without nerve stimulation. Furthermore, muscle tissue regeneration was effectively improved over the long term after the conductive hydrogel was used to fill muscle damage.
The injectable conductive hydrogel developed in this study excels in electrophysiological signal recording and stimulation performance, offering the potential to expand its applications. It presents a fresh approach to the field of bioelectronic devices and holds promise as a soft tissue prosthesis for rehabilitation support.
Emphasizing the significance of the research, Professor SHIN Mikyung notes, “We’ve created an injectable, mechanically tough, and electrically conductive soft tissue prosthesis ideal for addressing severe muscle damage requiring neuromusculoskeletal rehabilitation. The development of this injectable hydrogel, utilizing a novel cross-linking method, is a notable achievement. We believe it will be applicable not only in muscles and peripheral nerves but also in various organs like the brain and heart.”
Professor SON Donghee added, “In this study, the closed-loop gait rehabilitation system entailing tough injectable hydrogel and stretchable and self-healing sensors could significantly enhance the rehabilitation prospects for patients with neurological and musculoskeletal challenges. It could also play a vital role in precise diagnosis and treatment across various organs in the human body.”
The research team is currently pursuing further studies to develop new materials for nerve and muscle tissue regeneration that can be implanted in a minimally invasive manner. They are also exploring the potential for recovery in various tissue damages through the injection of the conductive hydrogel, eliminating the need for open surgery.
Injuries of the knee’s anterior cruciate ligament (ACL) are typically thought to be caused by acute traumatic events, such as sudden twists. Published in the Journal of Orthopaedic Research, new work analysing an animal model of ACLs suggests that such injuries can also occur as a result of chronic overuse, specifically due to a reduced ability to repair microtraumas associated with overuse. Importantly, the team said, females also are less able to heal from these microtraumas than males, which may explain why females are two to eight times more likely to tear their ACL ligaments than males.
“ACL tears are one of the most common injuries, affecting more than 200 000 people in the US each year, and women are known to be particularly susceptible,” said principal investigator Spencer Szczesny, associate professor of biomedical engineering and of orthopaedics and rehabilitation at Penn State. “While recent research suggests that chronic overuse can lead to ACL injuries, until now, no one had investigated the differential biological response of female and male ACLs to applied force.”
In the Penn State-led study, researchers placed ACLs from deceased male and female rabbits in a custom-made bioreactor that simulated the conditions of a living animal but allowed direct observation and measurement of the tissue. Next, they applied repetitive forces to the ACLs that mimicked those that would naturally occur during activities such as standing, walking and trotting and measured the expression of genes related to healing.
In male samples, the team found that low and moderate applied forces, such as those that would occur during standing or walking, resulted in increased expression of anabolic genes, which are related to building molecules needed for healing. By contrast, larger applied forces, such as those that would occur with repetitive trotting, decreased expression of these anabolic genes. For female samples, however, the amount of force applied did not influence the level of anabolic gene expression.
“It didn’t matter whether there was low, medium or high activity for females,” said Lauren Paschall, graduate student in biomedical engineering at Penn State and first author on the paper. “Female ACLs exposed to chronic use just didn’t heal as well as male ACLs, which may explain why women are predisposed to injuries. This supports the hypothesis that noncontact ACL injuries are attributed to microtraumas associated with chronic overuse that predispose the ACL to injury.”
According to the researchers, one explanation for the sex differences the team observed could be due to the higher amounts of oestrogen in females.
“Some studies have found that the overall effect of oestrogen on ACL injury is negative,” Paschall said. “Specifically, studies have shown that human women are more likely to tear their ACLs during the preovulatory phase, when oestrogen levels are high, than during the postovulatory phase, when oestrogen levels are low.”
She said the team plans to further investigate the role of oestrogen on ACL injury.
Szczesny noted that although the team’s study was not in humans, the findings may suggest that providing additional recovery time for women following injuries could be advantageous.
“Ultimately, this work could also help to identify targets for therapeutics to prevent ACL injuries in women,” he said.