Canadian singer Celine Dion has revealed that she has been diagnosed with a very rare neurological disease called Stiff Person Syndrome (SPS), BBC News reports. The disease causes muscle spasms, interfering with daily activities. Injuries can be sustained from falls caused by spasms experienced while walking.
The 54-year-old singer had been battling with muscle spasms, and since the disease interferes with her singing, she has cancelled all of her concerts scheduled for 2023, putting them off to 2024.
SPS is an extremely rare disease, thought to affect only one in a million individuals. As such, relatively little is known about it and what causes it, although it is associated with autoimmune disorders and often misdiagnosed as Parkinson’s disease.
After a hiatus from 2014 to be with her husband while he battled cancer, she returned to the stage in 2019 with her new album Courage. This tour had a number of cancellations due to the COVID pandemic.
Speaking on an Instagram post, Dion said that she had “a great team of doctors working alongside me to help me get better” and had the support of her “precious children”.
The singer explained: “I’m working hard with my sports medicine therapist every day to build back my strength and my ability to perform again, but I have to admit it’s been a struggle.
“All I know is singing. It’s what I’ve done all my life and it’s what I love to do the most.
“I miss you so much. I miss seeing all of you [and] being on the stage, performing for you.
“I always give 100 per cent when I do my show but my condition is not allowing me to give you that right now.”
What is stiff person syndrome?
According to the National Institute for Neurological Disorders, SPS is characterised by “fluctuating muscle rigidity in the trunk and limbs and a heightened sensitivity to stimuli such as noise, touch, and emotional distress, which can set off muscle spasms. Abnormal postures, often hunched over and stiffened, are characteristic of the disorder. People with SPS can be too disabled to walk or move, or they are afraid to leave the house because street noises, such as the sound of a horn, can trigger spasms and falls. SPS affects twice as many women as men.”
A definitive diagnosis can be made by measuring the level of glutamic acid decarboxylase (GAD) antibodies in the blood, which is elevated in people with SPS. GAD is the rate-limiting enzyme that catalyses the conversion of glutamate to GABA
As for management, the symptoms can be well controlled. Pharmacological treatment includes IVIg, anti-anxiety drugs, muscle relaxants, anti-convulsants, and pain relievers.
Work continues for better treatments; so far rituximab proved ineffective. At present, research is focused on aetiology and the role of anti-GAD antibodies.
The decriminalisation of cannabis for private use does not include the workplace, a Johannesburg Labour Court judge has ruled.
Judge Connie Prinsloo, in a recent ruling, said submissions by the National Union of Metalworkers of South Africa (NUMSA) that the Constitutional Court had ruled that cannabis was no longer a “drug” but just a “plant or a herb” were wrong.
She said the Concourt “Prince” judgment in 2018 did not offer any protection to employees against disciplinary action should they contravene company policies or disciplinary codes.
She said the apex court had not said cannabis was no longer a drug, as the union had argued, but had merely allowed for its personal consumption, in private, by adults.
The case before Judge Prinsloo was a review of the dismissal of two PFG Building Glass employees in October 2020 who had tested positive for cannabis while on duty. The National Bargaining Council for the Chemical Industry had found their dismissal to be fair. The union said it was unfair since cannabis was not a drug according to the Constitutional Court.
The company, through its witnesses, presented evidence that being under the influence of alcohol or drugs within the workplace was an offence for which dismissal was the prescribed sanction for the first offence.
This was because the company took workplace safety very seriously and it had a moral and legal duty to ensure that the working environment was safe.
On site, there was gas, large forklifts, extremely hot processes and dangerous chemicals used to make heavy glass which could potentially cut or crush someone.
The company followed the Occupational Health and Safety Act and had a zero-tolerance policy towards alcohol and drugs.
Referring to evidence at the bargaining council, Judge Prinsloo said it had been suggested by the employees that the company was “sticking to the old stigmatisation” of cannabis, whereas the Constitutional Court, in the Prince judgment, had said it was “just a plant … a herb” and could be legally possessed and used.
Company representatives, however, said it was still recognised as a drug and an employee was not permitted to be on site under the influence of alcohol or drugs.
One of the dismissed employees, Mr Nhlabathi, testified that he had used cannabis three days before he reported to work on the day he tested positive. He said he had been employed since 2016 and had “been smoking dagga and doing his job properly”. He disputed that the alcohol and drug policy related to cannabis but only to “alcohol and substances”.
His colleague, Mr Mthimkhulu, also relied on the Constitutional Court judgment that “dagga was a herb and not a substance”. Both claimed they were not aware that they could be fired for testing positive for cannabis.
Judge Prinsloo said the arbitrator had accepted that the company had a zero tolerance policy and that it treated cannabis as a drug because it was a “mind altering substance”.
The arbitrator had said the Prince judgment did not overrule the provisions of the Occupational Safety Act.
Judge Prinsloo said it was evident that the union and the employees had confused issues relating to the decriminalisation of the use of cannabis in private and the rights of employers to take disciplinary action against an employee who contravened a disciplinary code.
The Prince judgment declared specific provisions of the Drugs and Trafficking Act to be inconsistent with the right to privacy and therefore invalid to the extent that they made the use or possession of cannabis in private, by an adult person, a criminal offence.
The Constitutional Court had held, however, that it was common cause that cannabis was a harmful drug.
“The court did not interfere with the definition of a drug, nor did it declare dagga to be a plant or a herb,” Judge Prinsloo said.
“The applicant’s understanding of the judgment was either very limited or totally wrong,” she said.
The company was entitled to set its own standards of conduct and dismissal was an appropriate sanction, she said, dismissing the review.
Public transport is used by more than 10 million commuters in South Africa every day. It’s how people get to work, how they get to the grocery store, how they get their children to school. It’s quite simply a way of life.
For many of these commuters, there is no alternative to minibus taxis. They are an indisputably dominant pillar of the informal public transport system, but they are also notoriously unsafe. The constant threat of an accident is a real concern for commuters, especially those who cannot afford private medical aid.
“We live in a country where 73% of the population doesn’t have access to private medical aid. Couple this with the high number of road accidents in South Africa, and what recourse do the vast majority of commuters have if they are involved in a road accident?” asks Rikus Scheepers, managing director at AcciCare Medical Service Providers.
AcciCare is a medical funding company that assists people who do not have medical aid, to get access to private hospital care when they are involved in a motor vehicle accident. Scheepers started AcciCare in 2017, with the intention of making private medical care accessible to all commuters.
“We started AcciCare in a few hospitals and had limited capital to work with but soon realised the extensive need for this type of service. As a start-up without a long trading history, it became impossible to grow the business to meet the demand. We needed a business partner who shared our vision to supply this essential service throughout the country, and so we approached Standard Bank,” says Scheepers.
“AcciCare is a unique concept not offered in South Africa,” says Jocelyn Hamilton at Standard Bank. “When they approached us for finance we had to apply some out-the-box thinking in order to provide a working capital solution that would enable the business to grow and expand into more provinces in the country.”
In the event a person is injured in a motor vehicle accident, AcciCare will assist treating doctors and hospitals to collect and complete the correct documentation in order for medical costs to be claimed back from the Road Accident Fund (RAF). AcciCare provides financial assistance to these service providers, so they don’t carry the costs while waiting for the RAF to settle accounts.
“We firmly believe that all commuters should have access to private medical care when they need it the most. Through our partnership with Standard Bank we are expanding our footprint and we have exciting initiatives in place for 2023, to educate more people about the reliable private care that is available to them,” says Scheepers. “Together with Standard Bank, AcciCare has saved countless lives and has significantly improved the quality of life of those who have unfortunately been involved in a motor vehicle accident.”
“Our business banking model is centred on partnering with clients to grow their businesses in the communities in which they exist. While we came in as a working capital solution that would see AcciCare achieve their vision, in return we indirectly partnered in improving the long-term quality of life for those unfortunate enough to be in need of medical care at critical times. We hope to continue with this partnership, as they take their business to new heights,” says Hamilton.
On Tuesday 22 November, healthcare workers were among the public sector employees who engaged in a strike action to protest a lack of pay increase. A number of hospitals and clinics across South Africa and particularly Gauteng were affected, the Daily Maverick reports.
Unions had been offered a 3% increase plus an additional R1000, which the negotiating unions refused. Union leaders rejected this, demanding a 10% increase. Inflation is running at 6%, and food prices have risen by 12% from the start of the year to September – largely driven up by the war in Ukraine.
Union leaders say the strikes and protests are driven by wages staying the same over the past few years. Healthcare workers had already been suffering high rates of burnout battling COVID waves. In addition, workers complained of being understaffed, and enduring dire working conditions from lack of equipment, medication and food.
On Tuesday morning, burning tires were placed on Chris Hani Road in Soweto. Striking workers wearing union colours were preventing many vehicles, including ambulances, from entering Chris Hani Baragwanath Hospital. Patients inside were being left unattended.
Sebokeng Hospital in Sedibeng meanwhile was running on a skeleton staff, with doctors and nurses prevented from entering. Emergency services were being diverted to nearby facilities.
Meanwhile, GroundUp reported that patients were being turned away from Mabandla Clinic in the Eastern Cape. In Gqeberha, Motherwell NU8 clinic and the Motherwell Healthcare Centre were both reported to be closed.
On Tuesday afternoon, the Gauteng Department of Health received an interdict against the strikes, preventing striking workers from interfering with access to hospitals, EWN reports. The public healthcare systems in Gauteng and other provinces have already been strained, with recent high-profile protests and resignations over inadequate funding and allegations of corruption.
With summer and the holidays approaching, soon thousands of adults and children will flock to the country’s shorelines and public pools. But many who live inland and in poor communities do not have access to safe water bodies and have not learned how to swim. Children play unsupervised in rivers and farm dams.
In Riebeek Kasteel last year, a grade six learner found his way into a dam within walking distance of his school, Meiring Primary. Just 12 years old, he drowned.
Now a bright red container stands at the school. It is one of the National Sea Rescue Institute’s (NSRI) “survival swimming centres”.
Andrew Ingram, NSRI drowning prevention manager, says swimming is an “essential skill”.
The first of its kind, the 12-metre shipping container contains a six-metre heated swimming pool, a changing room, an office and a camera monitored by the NSRI. The water is one metre deep, making it possible for the learners’ feet to touch the ground. The facility can also be locked up to avoid children accessing it unsupervised.
The design is inspired by previous work done withlifeguard containers. Almost everything is donated – the container, the pool’s fibreglass and resin, pumps and the filtration systems. The cost would otherwise be about R650 000.
After the Riebeek Kasteel installation in March, a second centre was set up in Tombo Village, Eastern Cape. Two more are expected next year – in KZN and the Northern Cape.
“We don’t teach the children how to swim, we teach them how to survive,” says Petro Meyer, an NSRI Instructor in Riebeek Kasteel. She said the valley gets very hot in summer and parents are away working. Children then “go to the dams and to the rivers and they swim alone without supervision”.
Meyer says they teach students four things: breath control, orientation, floating and moving through water. Children should be able to swim at least five metres once training is complete. Since the survival school opened, she says that they’ve given about 1,400 lessons.
A 2021 study on drowning prevention by the World Health Organisation found drowning to be the third most common accidental death in the world.
Brenton Cupido, principal at Meiring Primary, said there are no other public pools. The closest public one is 20 minutes by bus to Malmesbury and costs R30.
Riebeek Kasteel has many poor families and many parents at his school are farm workers and the majority depend on social grants.
“The farmers try to stop the learners [from using the farm dams] but they can’t be everywhere,” he says.
Cupido said the government should see that “there is a need for swimming pools in the rural areas with proper supervision”, and this would “prevent further tragedy”. “I don’t want to go through another … drowning again,” said Cupido.
“We have that peace of mind, that if our children … fall in the water, they know how to survive,” he said.
Another NSRI project is the over 1300 pink buoys across South Africa used as assisted floating devices in case of emergencies. These can be found in dams, rivers and the seaside. The NSRI also runs free swimming lessons at various municipal pools in the Western Cape.
According to the NSRI, only 15% of South Africans can swim (we cannot verify this statistic but it is highly likely that most South Africans cannot swim – editor). “If your parents can’t swim, it’s very likely that you won’t learn to swim,” said Ingram. “It’s expensive to learn to swim”.
With the survival centres, the NSRI hopes to “instil a culture of swimming in poor communities where it wouldn’t have been possible previously”.
Actor Chris Hemsworth. Credit: Gage Skidmore / Wikimedia Commons
Actor Chris Hemsworth has announced that he is stepping back from acting in order to focus on preventative measures for Alzheimer’s disease.
The 39-year-old star of ‘Thor’ told Vanity Fair that genetic testing had confirmed that he had two pairs of a gene, APOE4. which is highly predictive of developing Alzheimer’s. About one in four have a single copy while 2–3% carry two copies of the gene.
The reason APOE4 increases Alzheimer’s risk isn’t not well understood. The APOE protein helps carry cholesterol and other types of fat in the bloodstream. Recent studies suggest that problems with brain cells’ ability to process lipids may play a key role in Alzheimer’s and related diseases.
Lipid imbalances can impair many of a cell’s essential processes. This includes creating cell membranes, moving molecules within the cell, and generating energy.
Hemsworth had made the discovery while making the TV series ‘Limitless‘, in which he engages in a variety of activities to push the limits of his own body and mind and explores ways of extending the lifespan.
“My concern was I just didn’t want to manipulate it and overdramatise it, and make it into some sort of hokey grab at empathy, or whatever, for entertainment,” said Hemsworth. “It’s not like I’ve been handed my resignation.”
He emphasises that he is thankful at having made the discovery, as it has made him more appreciative of his life, and it now means he can now take steps to protect his health.
Fortunately, research suggests that there are lifestyle changes that may offer preventative effects for APOE4 carriers, such as reducing stress and getting regular exercise – though the latter is unlikely to be a problem for the already athletic actor. Dietary measures include various low-carbohydrate diets (including ketogenic diets), regular portions of oily fish, cruciferous vegetables and abstaining from alcohol.
Supplements with potential benefits include DHA, quercetin, resveratrol, vitamin D3, vitamin K2, B-vitamin complex and possibly lithium.
Fikile (Sr Fikx) Dikolomela-Lengene, a nurse activist says she has had a front-row seat to corruption unfolding in Gauteng’s public health sector. PHOTO: Supplied/Facebook
Fiery nurse activist Fikile Dikolomela-Lengene says she has had a front-row seat to corruption unfolding in Gauteng’s public health sector, and she is not afraid to speak out.
Dikolomela-Lengene grew up in the corridors of Chris Hani Baragwanath Academic Hospital in Soweto, Johannesburg – Africa’s largest health facility.
The youngest of nine siblings and the only daughter, her father died when she was three years old. After this, her mother, a nurse at Baragwanath Hospital, would take her along to work.
“There were times when my mum didn’t have a nanny so she would take me to Bara [a nickname among healthcare workers for Baragwanath], where she worked in the same surgery theatre for 40 years,” says Dikolomela-Lengene. “I was actually sleeping on stretcher beds. I would accompany her to go fetch patients. This was a single mom with a little girl and nobody to look after her and she needed to work.”
At the hospital, a young Dikolomela-Lengene grew inspired to become a nurse, while cultivating her first inkling of justice. “I saw what was happening, and I thought, this is something I would like to do,” she says. “It came with a lot of context of the profession. I mean, I saw my mom and how the profession didn’t upskill her, how she suffered because of having a child, the shifts, and all of that. And I think it’s where the love for professional activism came in. To say, if I go into this profession, I wanted to be in a place where I could influence change.”
Nurse activist
Today, with a string of qualifications behind her name, including a Bachelor’s degree in nursing from North West University and a Mandela Washington Fellowship for Young African Leaders, 36-year-old Dikolomela-Lengene describes herself as a “nurse activist” and calls herself ‘Sr Fikx’ because she is passionate about influencing change in the public health sector. Currently based at the Stretford Community Health Centre – which serves the township of Orange Farm in the south of Johannesburg – she is passionate about HIV care and heads several public health campaigns at community level.
“What is interesting to me is the non-acquiring of condoms, today in an era when HIV is so rife
Commenting on the report findings of the Stop Stockouts Project (the SSP monitors shortages in essential medicines across South Africa) launched in August, Dikolomela-Lengene laments the shortfall of contraceptives – particularly injectable contraceptives and condoms – in the country’s public health sector.
“What is interesting to me is the non-acquiring of condoms, today in an era when HIV is so rife,” she says. “We ran out of [government-issued] condoms in May. And they actually don’t even have a new tender yet. And this shocked me. We should plan, right?”
She points out the ripple effects of this shortfall, such as an increase in required abortions. “Since there are none of these types of contraceptives, how has it impacted on our TOP [termination of pregnancy] services, you know? Especially in clinics where these services are burdened as it stands?”
“rot of corruption”
Dikolomela-Lengene says “the rot” of corruption in Gauteng’s health sector runs deep.
In 2015, she was a founding member of The Young Nurses Indaba Trade Union (YNITU), which represented over 10 000 workers, who pay R70 per month for membership.
Speaking to Spotlight, Dikolomela-Lengene alleges that the union’s leadership was “hijacked” at a congress in October last year and that millions of rands from the union’s coffers disappeared. In the midst of the clash, the union’s FNB business account was frozen in November 2021. However, allegedly membership fees are still being paid into private accounts. AmaBhungane reported on the alleged hijacking of the trade union in September. The new leadership rejected claims of wrong-doing.
In February this year, Dikolomela-Lengene and fellow former union leaders put the allegations before the Department of Labour. “We told them we need assistance because the union is hijacked and is being used for activities that currently… we actually don’t even know what is happening,” she says.
Dikolomela-Lengene adds that the union had been given notice to deregister on September 28. She will continue to meet with the Department of Labour. “Let me just say it’s been a hassle,” she adds. (AmaBhungane reported on the deregistration here.)
Last year in August, Gauteng health official Babita Deokaran was assassinated shortly after flagging up to R850 million in suspicious payments authorised at Tembisa Hospital in Johannesburg. (Spotlight earlier asked the new Gauteng Health MEC Nomantu Nkomo-Ralehoko about the alleged corruption flagged by Deokaran and other corruption-related issues here.)
According to media reports, one of the people accused of capturing the YNITU – Lerato Mthunzi – is the wife of embattled Tembisa Hospital chief executive officer (CEO), Ashley Mthunzi, who was suspended on August 26 over allegations of widespread corruption – including R498 000 of the hospital budget spent on 200 pairs of skinny jeans. After his suspension, one of Mthunzi’s notable supporters had been the nursing union, now headed by his wife. Mthunzi (Lerato) has denied any wrongdoing.
‘defending and defending’
During the interview with Spotlight, Dikolomela-Lengene shakes her head, laughing. “I’m laughing, you know because it’s so sad. People are defending and defending, but there’s a family here that lost somebody. There are kids currently who don’t have a mother because there are people in positions who don’t want to do their job.
“You get to ask yourself, who authorises codes for jeans, skinny jeans, in a hospital?
“I don’t know how they’re going to get rid of corruption in health in Gauteng. You get to ask yourself, who authorises codes for jeans, skinny jeans, in a hospital? It’s like somebody’s mocking the governance.
“You have to ask yourself, how many processes are there before payment is actually made? So all those processes were flawed, or were people in those processes flawed themselves? And then, you have condoms not being on tender. You start asking yourself [how are] people able to get money for jeans, but there’s no money for a tender for condoms?”
Looted
Shaking her head, Dikolomela-Lengene says the province’s health budget is being looted.
“We’re not going anywhere unless they actually bring a lot of people to account,” she says. “R850 million, imagine! I’m looking at my clinic. Our budget is around R20 million. How many clinics could have been revamped for R850 million? How many hospitals could have been looking A-class, private style, with that money? It is possible to revamp our clinics. It is possible to revamp our hospitals. There is money. There is money, but there is no political will.”
“into the lion’s den”
On Gauteng’s new health MEC Nomantu Nkomo-Ralehoko, Dikolomela-Lengene says, “We’ll see with the new MEC. The past two MECs disappointed us and they were both health professionals. (Nkomo-Ralehoko is not a healthcare professional by training).”
“I mean, having to fight with a patient because you don’t have a Panado. You don’t have Panado! A simple thing like that.
Nkomo-Ralehoko, in response to questions by Spotlight, vowed to act on recommendations by a Special Investigating Unit (SIU) currently conducting a forensic investigation into transactions at Tembisa Hospital.
“At this moment, I’m not going to be judgmental,” says Dikolomela-Lengene. “You know, we just want to see change. I mean, having to fight with a patient because you don’t have a Panado. You don’t have Panado! A simple thing like that. And as a nurse, you have to take the brunt of it. She’s [Nkomo-Ralehoko] going into a lion’s den. She will need a thick skin.”
Earlier this year, Dikolomela-Lengene was one of 700 young African leaders who studied in the United States for six weeks as Mandela Washington Fellows. She was placed at Howard University, which counts former US President Barack Obama among its alumni.
“It’s what we call a historically black college, one of the colleges that Barack Obama went to. So I think that was an honour on its own,” she says.
As part of her training, she got to shadow and even debate with high-ranking American government officials. “I learned a lot of skills, but what stood out was the ‘huddle system’. This is a programme whereby we have meetings more frequently so that changes can be made more frequently. I think in South Africa, we stick with things that are wrong for too long. If a policy isn’t working, we wait for five years. If a system isn’t working, we wait for five years. So with the huddle approach, you continuously monitor and make changes when things are not working.”
a “downgrade” in nurse training
Dikolomela-Lengene lives in Johannesburg but says she prefers not to divulge particulars due to safety concerns.
She did, however, share about her current reading material.
The book currently on her bedside table is ‘Who Ate My Cheese? The Road to Freedom’ by Rowland Rose – a gift from the United States embassy during her recent trip.
Another issue keeping Dikolomela-Lengene awake at night is South Africa’s nurse training curriculum. In 2019, she served on the ministerial task team that oversaw amendments brought to South Africa’s nurse training strategy, as chronicled in The National Strategic Direction for Nursing Education and Practice: A Road Map for Strengthening Nursing and Midwifery in South Africa (2020/21−2025/26).
“Our qualifications have been downgraded.
She is highly critical of this new strategy, calling it a “big mistake”, and effectively a “downgrade” in nurse training in the country.
“I’ve got a four-year diploma. I’ve got a one-year post-graduate, [and] I’ve got a three-year degree. I’m not even going to talk about the side courses I’ve done. There are more than ten. Can I tell you that I cannot access a university in South Africa? Our qualifications have been downgraded. I’ve got more than nine years of formal study and I can’t do my Masters [degree] because my accreditation has been brought two to one level lower,” says Dikolomela-Lengene.
“You’ve got academia and professors making a curriculum for nurses – not nurses. It’s shocking… So there is a big fight between the National Department of Health, the South African Nursing Council, which is the regulatory body of nursing, and the Department of Higher Education.”
The nurse activist says that her salary could triple if she moved from the public sector into private, but that she wouldn’t dream of such a step. “The passion I have for what I do is what fuels me,” she says. “And it’s effortless, you know? I love what I do. Whatever time they call me, I’m ready. I just show up – always.”
Republished from Spotlight under a Creative Commons 4.0 Licence. Read the original article here.
When dealing with risks, the often-used metric of “deaths per 100 000 population” can be a bit unwieldy, especially when explaining risk to patients. During the COVID pandemic, this became something of a problem when trying to convey the risks of vaccination to the general public. Many felt that the risk of adverse effects outweighed the protection that the vaccination conferred against the coronavirus.
But there is a different, more approachable metric – in 1979, Ronald A. Howard introduced the ‘micromort’ – defined as one chance of death in a million. One in a million is about the same odds as flipping a coin 20 times a row and getting the same result.
Though its name is sure to make some people giggle, the micromort is commonly used in actuarial sciences and decision analyses to quantify the risk of death per unit of exposure to a risk factor or event (Howard, 1980). micromorts have the advantage of being easier to interpret and comprehend than abstract numerical figures, and have been used to convey risks associated with surgical operations and medical treatments.
For example, the mortality risk of general anaesthesia is 10 micromorts per procedure (ie, a 0.001% chance of dying), which is comparable to the mortality risk of an experienced skydiver takes when doing a parachute jump. Chronic cigarette smoking reduces adult life expectancy by 6.5 years on average; said differently, averaged over a lifetime, smoking reduces life expectancy by 7 micromorts per day (3.5 hours per day) (Shaw et al., 2000).
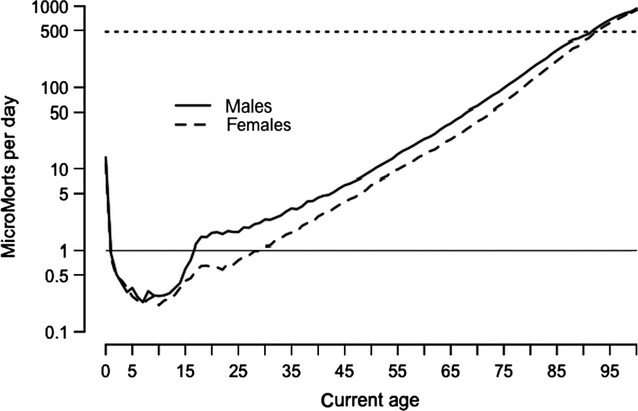
Simply being being alive carries a risk in itself: it is highest on the first day of lift at around 500 micromorts, drops rapidly in childhood and then increases steadily throughout adult life until the 90s, when each day is as risky as that person’s first day.
MicroMorts per day for average person in England and Wales—dashed line shows rate for first day of life. (Spiegelhalter, 2014)
Perhaps unsurprisingly, one UK estimate showed that travelling by motorbike carries the highest risk of death at 9.6km for each MicroMort. Travelling by car is far safer at 400km per MicroMort. But somewhat counterintuitively, walking is not much safer than travelling by motorbike: hitting the pavement results in one MicroMort per 27.2km walked. This can be partly explained by the greater amount of time spent walking and exposed to environmental hazards such as traffic, air pollution, crime and so on.
The concept of micromorts can also be applied to pregnancies and risks to the foetus. The risk per unit due to stillbirth is only about 19 or 3710 micromorts when drinking 5 units/week throughout pregnancy. For low risk women in the UK, planned first birth at home carries an additional 843 (-200 to 2620) micromorts compared with in hospital, and planned vaginal breech birth an additional 5870 (-4400 to 18 500), compared with planned caesarean. By contrast, the risk from the mother eating a serving of unpasteurised cheese, is negligible at 0.00026 micromorts (Hickson et al., 2020).
The award was based on strides made by ASASA towards improving the quality of life of people living with AxSpa, as well as training done to build awareness in the medical fraternity around AxSpA in the country. With 36 posters entered into the awards by organisations across the globe, ASASA came out tops.
When asked about the award, van Dam said, “This was a real honour to represent South Africa at PARE. 2022 is also the first year that an African country was invited to attend PARE. Winning this award sheds light on our country and our unique problems. The delay to diagnosis of 10.8 years is just unacceptable. The access to the correct medication in both the private and public sector is also not sufficient for a debilitating, progressive disease that can lead to disability if left untreated.”
ASASA estimates that there are approximately 160 000 people suffering from the AxSpA in South Africa, with many of these sufferers undiagnosed. ASASA has made significant strides this year in the training of over 100 General Practitioners and over 250 optometrists around AxSpA diagnosis and the effects it can have on other parts of the body, like the eyes. In addition, ASASA, along with other partners, assisted in gathering data from South African respondents in the first ever live patient survey, called the International Map of Axial Spondyloarthritis (IMAS) survey, which is run by the Axial Spondyloarthritis International Federation that surveys people diagnosed with AxSpA and assesses the impact and burden that AxSpA has on the lives of patients, from their perspective.
Van Dam concluded, “There is still a lot we can do in South Africa and ASASA is busy growing its team of volunteers to help to build awareness around AxSpA in the country. We aim to continue to build support structures for patients in the country, as well as continually working with the medical fraternity, assisting with early diagnosis and access to treatment.”
A study in the Journal of Hospital Medicine found that the general public does not have a good grasp of the medical jargon that physicians typically use in their introductions to patients. They found speciality names and seniority titles are sources of misunderstanding.
“Jargon is pervasive in medicine and the opportunity for misunderstanding due to this terminology begins the instant that physicians introduce themselves to patients,” explained Emily Hause, MD, MPH, a paediatric rheumatology fellow at the U of M Medical School. “We found that most people can’t define specialty names nor correctly rank medical seniority titles. Physicians should describe their medical specialty and role on the patient’s care team in plain language to help reduce this source of potential confusion.”
Volunteer participants at the 2021 Minnesota State Fair completed an electronic survey that measured their knowledge of medical specialties and titles. Of the 14 specialties included in the survey, six specialties were correctly defined by less than half of the respondents:
Neonatologists: 48%
Pulmonologists: 43%
Hospitalists: 31%
Intensivists: 29%
Internists: 21%
Nephrologists: 20%
When asked to rank medical roles, only 12% of participants correctly placed these titles in order: medical student, intern, senior resident, fellow and attending.
Further research is suggested to survey knowledge on additional specialties and obtain more demographic information.