The United Nations International Day of Persons with Disabilities (IDPD) is celebrated annually on 3 December, aiming to promote an understanding of disability issues and to mobilise support for the dignity, rights and well-being of persons with disabilities. An estimated 1.3 billion people experience significant disability.1a This represents 16% of the world’s population, or 1 in 6 of us.1a In South Africa, that figure is 15%, or 8,9 million.2a
Persons with disabilities face many health inequities, including stigma, discrimination, poverty, and exclusion from education and employment. They also face barriers in all aspects of the health system, such as negative attitudes and discriminatory practices and lack of information or data collection and analysis on disability.1b+c
“Disability inclusion is critical to achieving the Sustainable Development Goals (SDGs) and global health priorities to achieve health for all, as envisioned in the 2030 Agenda for Sustainable Development,” says Prudence Selani, Head of Corporate Affairs at Sanofi South Africa. On this International Day of Persons with Disabilities, Sanofi is celebrating its commitment to the 2023 theme, ‘United in Action to Rescue and Achieve the Sustainable Development Goals (SDGs) For, With, and By Persons with Disabilities,’ through several initiatives.
In collaboration with its implementation partners, Sanofi has launched a unique external training programme for persons with disabilities, especially those from disadvantaged communities. This programme is designed to break barriers to education post-matriculation, offering management training and entrepreneurship skills in areas like financial literacy and marketing. This initiative also supports people with post-matric qualifications striving for employment, enhancing their employability and professional growth.
“As part of our commitment to Broad-Based Black Economic Empowerment (B-BBEE), 10% of learners on our Youth Employment Service “Y.E.S.” programme are persons with disabilities, underlining our commitment to diversity and inclusion,” says Selani.
Sanofi’s Diversity, Equity and Inclusion is bolstered through Employee Resource Groups (ERGs). The Ability+ ERG promotes a safe environment for employees to declare their disabilities, offering support and resources. Sanofi is also offering employees the chance to enrol in South African Sign Language courses, to transform its workplace into a disability-friendly space.
“Our partnerships with local and global organisations that are focused on disabilities will enable us to conduct workshops with leaders and employees, fostering a culture of understanding and empathy.”
“Sanofi also emphasises employee wellness and mental health, offering extensive support and wellness programmes,” says Selani. “These initiatives underscore our dedication to the well-being of all our employees.”
“As we mark IDPD 2023, Sanofi encourages organisations across all sectors to join us in these efforts. Together, we can make significant strides towards a more inclusive society and achieving the SDGs for, with, and by persons with disabilities,” concludes Selani.
Together, we are making a difference. Join us in our journey towards an inclusive future.
A “gentle and loving” person who “paid the ultimate sacrifice” for making sure those who needed it received aid. This was how Ahmed Abbasi, who headed the Gift of the Givers office in Gaza, was remembered at an interfaith memorial service in St George’s Cathedral, Cape Town, on Sunday evening.
At least 400 people came to pay their respects. Several faith leaders were in attendance as well as government officials, including Cape Town Mayor Geordin Hill-Lewis and former international relations minister Lindiwe Sisulu.
Gift of the Givers’ Western Cape project coordinator Ali Sablay told GroundUp that Abbasi and his brother, Mustafa, were killed by a missile while returning from their morning prayer.
Abbasi leaves behind his wife and three children. They have been relocated to a place of safety.
Sablay said that Abbasi was responsible for setting up a women and children care centre, three desalination plants, supplying medicines to hospitals, and more.
“He was the head of this operation and in the last 40 days of this war, he’s been remarkable in the work he’s been doing in getting aid to those affected. He had the option to relocate but he said he could not leave the people behind. He stayed on with his family. Unfortunately, he paid the ultimate price.”
Sablay said the organisation backed President Cyril Ramaphosa’s decision to refer members of the Israeli government to the International Criminal Court (ICC). “We support the political parties that are asking that the Israeli ambassador be expelled. This is not an act of war, this is an act of genocide,” he said.
Reverend Michael Weeder, dean of the cathedral, led the service. Reverend Allan Boesak gave the sermon.
Megan Choritz read out a letter of condolence on behalf of South African Jews for a Free Palestine. “There has never been a moment of crisis where Gift of the Givers has not stepped up and offered help, solace, dignity and hope to those affected. Please, in this dark moment for you and your organisation, accept our prayers, solidarity and support.”
“We will continue to speak up, continue to disavow any claims that this war is waged in our names, or in the name of Judaism,” she said.
The service was interspersed with hymns, songs and poetry readings. Several faith leaders addressed the congregation.
In a pre-recorded message, Dr Imtiaz Sooliman, founder of Gift of the Givers, thanked Father Weeder for organising a memorial service for someone he had never met. “This is not a head of state, a minister, or a person of high rank. He’s just an ordinary Palestinian, but he works for Gift of the Givers and that makes him special, even if I say so myself.”
In an interview with GroundUp last month, Sooliman described Gaza as “the worst situation in the world because there is no exit route”.
“You can’t get out. The area is so small. It’s so easy to bomb it … Nobody can have a safety plan. Where are you going to hide? There’s no such thing as safety in Gaza,” he said.
The New York Times reported last week that over 100 aid workers in Gaza have been killed in the past five weeks.
I hope this newsletter finds you in good health and high spirits. As part of Doctors’ Day on 16 November, my team and I wanted to take a moment to express our deepest gratitude and appreciation for the incredible work you do every day.
On this special occasion, we celebrate you and your fellow doctors for the remarkable impact you make on the lives of those you serve. Your expertise, resilience, and compassionate care contribute to the betterment of our community and the well-being of countless individuals. We recognise the challenges you face, especially in these unprecedented times, and we are inspired by your continued efforts to provide exceptional healthcare.
At EthiQal, we take pride in supporting doctors like you. We are committed to ensuring that you have the comprehensive insurance coverage you need, allowing you to focus on what matters most – your patients.
To mark this occasion, we extend our warmest wishes for a Happy Doctors’ Day! May you find time to reflect on your accomplishments and the positive impact you’ve made on the lives you’ve touched.
As a token of our appreciation, we have created a small thank you video. Please click on the video below – it may be a small gesture, but we hope it brings a smile to your face and serves as a reminder of the impact you make every day.
We are also donating, on your behalf, to the Healthcare Workers Care Network (HWCN), a nationwide healthcare worker mental health support network with the slogan ‘Caring for the Carers by Carers’. They do great work supporting doctors, sustained only by financial donations and pro bono work.
Thank you for your tireless dedication, and we look forward to continuing to support you whilst you focus on making our nation healthier.
Members of the University of Cape Town’s Holistic Drug Discovery and Development Centre H3D
A formidable disease that has plagued humanity for centuries, malaria has exacted a heavy toll on human lives, disrupting communities and hindering socio-economic progress across some of the most vulnerable regions of the world, particularly the African continent.
With its stealthy transmission through the bites of infected mosquitoes, malaria has earned the dubious reputation of being one of the deadliest vector-borne diseases on the planet. So much so that the World Health Organization’s World Malaria Report reveals that malaria cases are on the rise, with instances rising from 245 million cases in 2020 to over 247 million a year later1.
With an estimated 619,000 people succumbing to the disease in 20211, it remains a defining challenge for global healthcare systems. However, through the unyielding persistence and spirit of medical innovation and scientific ingenuity exemplified by research facilities such as the University of Cape Town’s Holistic Drug Discovery and Development Centre (H3D), solutions to mitigate the severity of malaria are on the horizon.
“As the first and only integrated drug discovery platform on the African continent, H3D’s mission is to discover and develop innovative life-saving medicines for diseases that predominantly affect African patients,” explains Bada Pharasi, CEO of the Innovative Pharmaceutical Association of South Africa (IPASA).
H3D’s focus on building Africa-specific models aims to improve treatment outcomes in African patients and to educate and train a critical mass of skilled African-based drug discovery scientists. H3D’s scientific output and research model includes attracting international investment in local innovative pharmaceutical research and development (R&D) across the African continent to address the disproportionately high global disease burden. Importantly, H3D targets critical infectious diseases, including tuberculosis, antibiotic-resistant microbial diseases, and malaria.
“Given the vulnerability of many of the African populations, the continent accounted for 95% of malaria cases and 96% of malaria deaths in 20211. Accordingly, continued antimalarial drug research and development, such as the studies conducted by H3D, is important to prevent and treat the millions of cases that arise each year, all of which have consequences on both the health and socioeconomic development of the continent,” adds Pharasi.
Since the official launch of H3D’s programs in April 2011, there have been notable advances in innovative drug discovery projects. The centre has demonstrated a strong track record with multiple chemical series discovered and being progressed at H3D in each stage of the drug development pipeline.
A significant achievement reached by H3D was the discovery of the malaria clinical candidate, MMV390048, which reached phase II human trials in African patients. This was the first ever small molecule clinical candidate, for any disease, researched on African soil by an African drug discovery research unit.
According to Dr Candice Soares de Melo, Chief Investigator at H3D, the centre’s current anti-malarial programmes will focus on the identification of quality leads suitable for optimisation and candidate selection as potential agents for the treatment of uncomplicated Plasmodium falciparum malaria, ideally with additional activity against liver-stage parasites to offer protection and prevent relapses (in case of malaria caused by the species Plasmodium vivax), as well as blocking the transmission of the disease.
“A critical component of the research conducted at H3D is to develop medicines that are safe and sufficiently tolerated to be given to the widest range of recipients, including infants and pregnant women,” says Soares de Melo.
Besides the potential benefits of providing a new cure for malaria, H3D serves as a catalyst for training scientists in infectious disease research and influencing the R&D environment in Africa. As part of its partnership with the South African Medical Research Council, H3D has worked to mentor and develop scientists at other African universities, including those at Historically Disadvantaged Institutions (HDIs) within South Africa.
Furthermore, apart from strengthening drug discovery innovation at UCT, the centre has also taken a lead role in partnership with the Bill & Melinda Gates Foundation in catalysing drug discovery across sub-Saharan Africa, with upwards of 16 university research groups working on malaria and tuberculosis drug discovery.
“An example of this is the Phase 1 clinical trial for the H3D clinical candidate MMV390048, which was carried out at the UCT Division of Clinical Pharmacology,” adds Soares de Melo.
Another is the MATRIX independent special project, which has the potential to transform local drug manufacturing across the continent. Funded by the United States Agency for International Development (USAID), the project aims to pilot cost-effective local manufacture of antiretroviral Active Pharmaceutical Ingredients using flow reactor technology.
“Should Africa intend on a path to self-sufficiency, it’s important to drive continued investment in health innovations developed for and by Africa.
“We support the research efforts of H3D, and strongly believe that now is the time to take a deliberate and systematic approach to develop new capabilities, transfer technologies, leverage partnerships and networks, and train scientists, all while delivering on drug discovery projects to help address the continent’s, and the world’s, greatest health challenges,” concludes Pharasi.
Medshield Medical Scheme, a prominent medical aid scheme, and Clicks, a leading retail pharmacy chain and Designated Service Provider on the Medshield Pharmacy and SmartCare Networks, are pleased to announce the expansion and enhancement of their partnership. This partnership aims to empower members with even greater access to quality care through Medshield’s SmartCare benefit, allowing access to a network of Clicks clinics for professional nurse and nurse-led virtual Family Practitioner (GP) consultations. This further cements their commitment to delivering healthcare excellence through technology.
Expanding the SmartCare Network
Medshield and Clicks have partnered to add 123 Clicks clinics to the existing 255 clinics in the SmartCare Network. This expansion guarantees that Medshield members can conveniently and efficiently access their SmartCare benefits at these selected Clicks clinics.
SmartCare: The Gateway to Modern Healthcare
Medshield’s flagship member benefit, SmartCare, is leading the charge in digital innovation in healthcare. By utilising the power of technology, SmartCare provides access to pharmacy clinics that offer a one-stop-shop for members to access professional nurse consultations, health risk assessments, sick notes, specialist referrals, medication and nurse-led virtual access to Family Practitioners (GP) when required. This benefit is redefining the way healthcare services are accessed and delivered, making it more convenient and efficient for both healthcare providers and members.
Medshield members have access to an unprecedented level of convenience through Clicks clinics, which are powered by the Udok telemedicine solution. These consultations cover prevention, diagnosis, and treatment, focusing on connecting patients, nurses, doctors, and medication for fast and convenient care.
Kevin Aron, Principal Officer at Medshield, explains, “When we introduced SmartCare, we aimed to offer a cutting-edge solution that would add more value for our members. Medshield was the pioneer medical scheme in South Africa to integrate this service as a new benefit for all members, without additional costs.”
The Medshield SmartCare Benefit
SmartCare offers a multitude of benefits to Medshield members, providing them with a holistic approach to healthcare:
Enhanced Access to Care: SmartCare provides Medshield members with easy access to quality care led by professional, licensed nurses at pharmacy clinics. The nurse will facilitate a virtual Family Practitioner (GP) consultation depending on the patient’s ailment. Once the patient has been diagnosed and treatment prescribed, the relevant medication is easily obtained from the pharmacy.
Stretch day-to-day medical aid benefits: Healthcare services offered by SmartCare pharmacy clinics such as Clicks are cost-effective, and enable members to receive quality care and their medication as a complete solution. Utilising the SmartCare benefits allows the member to receive quality care whilst minimising the use of their day-to-day benefit.
Improved Health Outcomes: SmartCare services implemented by pharmacy providers allow members to manage and receive preventative care through wellness checks and health risk assessments, providing access to early intervention services and ultimately leading to better health outcomes.
The Vision of Collaboration
“We are excited to announce our enhanced partnership with Clicks, a valued partner on the Medshield DSP Network. With the addition of 123 Clicks clinics to the SmartCare Network, we are reinforcing our commitment to provide Medshield members with access to high-quality healthcare services,” said Kevin Aron, Principal Officer at Medshield. “SmartCare is revolutionising healthcare delivery, and we are proud to offer this innovative solution to our members.”
The Medshield SmartCare way of adding value:
A Medshield member can visit any Clicks clinic on the SmartCare network for primary healthcare needs such as acute conditions, wellness checks, health risk assessments, vaccinations, or chronic medication prescriptions as prescribed by a Family practitioner (GP).
A registered nurse performs a thorough medical history and examination of the patient.
The nurse can advise the patient on over-the-counter medication available at the pharmacy.
A virtual consultation with a family practitioner is requested by the nurse through Clicks clinic’s Udok technology when further treatment is necessary. The doctor then completes the consultation with the assistance of the nurse.
The nurse can print the doctor’s written documentation, and the patient can fill their prescription at the pharmacy immediately.
Accessible Medications and Comprehensive Care
In addition to SmartCare consultations, Clicks pharmacies are available on all Medshield plans, making access to prescription medication convenient for members.
Rachel Wrigglesworth, Clicks’ Chief Healthcare Officer stated, “This partnership between Clicks and Medshield focuses on the wellbeing of our customers, which is our top priority. The collaboration has expanded to include Clicks clinics powered by Udok, a solution that offers real-time access to registered family practitioners through our Nurse-led consultations on the SmartCare benefit, funded by Medshield Medical Scheme. As a leader in the healthcare market, this partnership perfectly aligns with our commitment to increasing access to affordable primary healthcare for all South Africans. We are committed to the continued success of this collaboration.”
Embracing the Future of Healthcare
As the healthcare industry continues to evolve in the digital age, SmartCare stands as a shining example of how technology and innovation come together to provide added convenience and efficiency in healthcare. It empowers nurses to provide additional care for Medshield members through accessible technology. Unless it is a trauma situation, members can visit a Clicks clinic on the SmartCare network for acute and chronic conditions. By embracing the future of healthcare through the SmartCare benefit, Medshield members can expect to experience efficient and reliable medical consultations to enhance their wellbeing.
“Medshield is continuing to reinvent healthcare the smart way. The SmartCare benefit offers our members a new level of convenience, connecting members with nurses, doctors and medicine like never before,” concluded Aron.
A Strengthened Partnership
Expanding the Medshield and Clicks partnership demonstrates a solid commitment to providing excellent healthcare services and a shared vision of creating a more accessible and convenient healthcare experience for Medshield members. It is a testament to the excellent collaboration between Medshield and Clicks, ensuring that quality care is always easily accessible.
A newly compiled dataset quantitatively captures witchcraft beliefs in countries around the world, enabling investigation of key factors associated with such beliefs. The findings, from Boris Gershman of American University, are published in the open-access journal PLOS ONE.
Many prior studies conducted around the world have documented people’s beliefs in witchcraft, defined as the idea that certain individuals have supernatural abilities to inflict harm. Understanding people’s witchcraft beliefs can be important for policymaking and other community engagement efforts. However, due to a lack of data, global-scale statistical analyses of witchcraft beliefs have been lacking.
To deepen understanding of witchcraft beliefs, Gershman compiled a new dataset that captures such beliefs among more than 140 000 people from 95 countries and territories. The data come from face-to-face and telephone surveys conducted by the Pew Research Center and professional survey organisations between 2008 and 2017, which included questions about religious beliefs and belief in witchcraft.
According to the dataset, over 40% of survey participants said they believe that “certain people can cast curses or spells that cause bad things to happen to someone.” Witchcraft beliefs appear to exist around the world but vary substantially between countries and within world regions. For instance, 9% of participants in Sweden reported belief in witchcraft, compared to 90% in Tunisia.
Using this dataset, Gershman then conducted an investigation of various individual-level factors associated with witchcraft beliefs. This analysis suggests that, while beliefs cut across socio-demographic groups, people with higher levels of education and economic security are less likely to believe in witchcraft.
Gershman also combined this dataset with other country-level data, finding that witchcraft beliefs differ between countries according to various cultural, institutional, psychological, and socioeconomic factors. For instance, witchcraft beliefs are linked to weak institutions, low levels of social trust, and low innovation, as well as conformist culture and higher levels of in-group bias, ie the tendency for people to favour others who are similar to them.
These findings, as well as future research using the new dataset, could be applied to help optimise policies and development projects by accounting for local witchcraft beliefs.
The author adds: “The study documents that witchcraft beliefs are still widespread around the world. Moreover, their prevalence is systematically related to a number of cultural, institutional, psychological, and socioeconomic characteristics.”
Professor Shabir Madhi has been appointed as an honorary Commander of the Most Excellent Order of the British Empire (CBE) by King Charles III.
Wits Professor of Vaccinology Shabir Madhi led the Oxford University sponsored Oxford/AstraZeneca Covid-19 vaccine clinical trials in South Africa
Wits University and the University of Oxford contributed scientifically to informing the public health response to the Covid-19 pandemic in South Africa and globally.
Madhi receives the Order in recognition of his services to science and public health in a global pandemic.
Madhi led South Africa and the continent’s first Covid-19 vaccine trials in 2020/2021 as founder and Director of the South African Medical Research Council (SAMRC) Wits Vaccines and Infectious Diseases Analytics (Wits VIDA) Research Unit.
An internationally recognised leader in his field, the National Research Foundation A-rated scientist was involved in multiple clinical and serology epidemiology studies on Covid-19, in addition to his research on vaccines against other life-threatening diseases.
The first of (subsequently two) Wits University-led South African Covid-19 vaccine trials, Madhi led the Oxford/AstraZeneca Covid-19 vaccine clinical trials in South Africa, in association with the University of Oxford.
Professor Sir Andrew Pollard, Director of the Oxford Vaccine Group, University of Oxford, and Madhi’s UK counterpart in these Covid-19 vaccine trials, says of Madhi’s CBE appointment: “I am delighted that Professor Shabir Madhi CBE has been honoured by King Charles for his remarkable contributions to global public health and particularly for his extraordinary leadership in the midst of a global pandemic. It has been a huge privilege for me to work alongside him and his team on the development of the globally impactful Oxford-AstraZeneca vaccine.”
Over the course of the pandemic (2020-2022), Madhi had been an outspoken, articulate, and ardent advocate of Covid-19 vaccination as well as for increased access to these and other vaccines in Africa.
On his appointment as CBE, Madhi says: “The privilege of being conferred this honour is credit to the tremendous effort of the incredible Wits VIDA research team that I have the privilege of leading at Wits University – before, during and beyond the Covid-19 pandemic. As a collective, and together with colleagues at the University of Oxford and in South Africa, we are proud to have contributed scientifically to informing the public health response to the Covid-19 pandemic in South Africa and globally.”
Mediaeval tyrant and inspiration for vampires, protein analysis reveals health secrets about Vlad the Impaler
New research analysing ancient protein residues left in letters written by the sadistic 15th century tyrant – and vampire inspiration – Vlad Dracula the Impaler suggests that he suffered from a number of health conditions. One of these conditions seemingly confirms one of the more outlandish tales about him – that he cried tears of blood.
Vlad the Impaler got his nickname because he impaled thousands of people on stakes: enemies (mainly the Ottoman Empire), criminals and anyone suspected of conspiring against his rule. He was eventually defeated in 1460, but the newly invented printing press spread the tale of his gruesome deeds all over Europe. Tales surrounding him may have inspired the iconic character of Bram Stoker’s Count Dracula in 1897. Nevertheless, more modern vampire stories such as Netflix’s ‘Castlevania’ make use of Vlad as inspiration.
This terrifying reputation made him an interesting topic for a bit of genetic archaeology in a paper published in Analytical Chemistry. Using sophisticated proteomic techniques, scientists analysed three letters written in 1457 and 1475 by the voivode of Wallachia, Vlad III, also known as Vlad the Impaler, or Vlad Dracula. This allowed them to tease out information about the man who wrote the letters as well as general information about the environmental conditions of 15th century Wallachia, a place of regional trade and conflict as well as disease transmission.
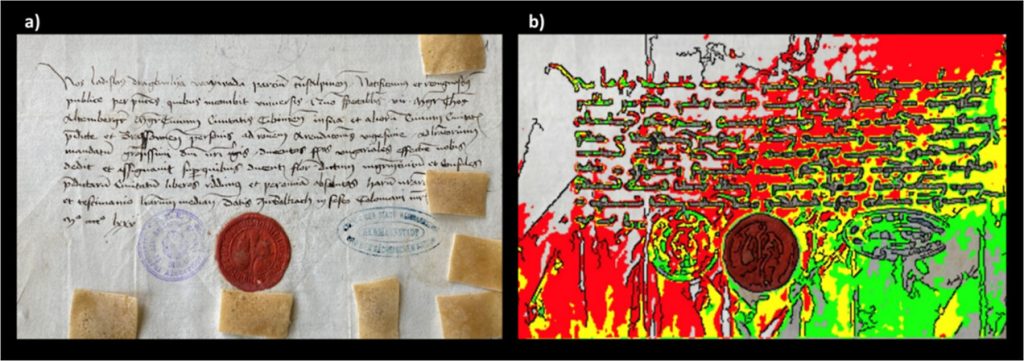
While centuries-old paper is unlikely to hold entire DNA strands, scientists were still able to piece together genetic information about the writer. The technique depends on the notion that a person’s writing hand will tend to rest on the paper being written upon, rubbing off a surprising amount of organic molecules in the process. They applied ethylene vinyl acetate to the papers, and with mass spectrometry, they discovered over 500 peptides – short chains of amino acids – with about 100 being of human origin, which they looked up in database searches.
Figure 1. (a) First letter (archive catalog number is II 365), dated August 4, 1475, here investigated, also showing the positions of the EVA strips (brownish rectangles) applied to its surface for capturing biological material; (b) mapping of the fluorescence of phenylalanine, tyrosine, and tryptophan under flash UV illumination (see the original article). Anal. Chem. 2023, 95, 34, 12732-12744
The researchers noted that while many mediaeval people may have handled these papers, it is also presumable that the most prominent ancient proteins can be attributed to the one who wrote and signed them – Prince Vlad the Impaler.
First, they discovered proteins pointing to ciliopathy, which affects the cellular cilia or the cilia anchoring structures, the basal bodies or ciliary function. This can manifest in a wide range of disorders, ranging from cerebral malformation to liver disease and intellectual disability.
They also uncovered signs of an undetermined inflammatory disease which likely involved his skin and respiratory tract.
Proteomics data also suggests that, according to some stories, he might also have suffered from a pathological condition called haemolacria – he could shed tears admixed with blood. This appears to confirm what some stories said about Vlad – that he sometimes cried tears of blood. While it is a known medical condition, it would have no doubt been terrifying for superstitious mediaeval people to behold when seen in someone with a reputation like Vlad the Impaler’s.
Non-human peptides also proved to be a window into the conditions of the time, hinting at common foods, pests and diseases. Database searches of the identified, as potential endogenous original components, 3 proteins from bacteria, 24 from viruses, 4 from fungi, 17 from insects (suggesting fruit flies), and 5 from plants (including rice, wheat and thale cress). Of the bacteria, they noted that some peptides related to Enterobacterales are specific to Yersinia pestis, the pathogenic bacterium causing plague, whereas another group is specific to E. coli.
Dr Imtiaz Sooliman, founder of The Gift of the Givers Foundation, has appealed for negotiations, compromise and peace in the Middle East. The respected South African aid organisation has had a presence in Gaza for nine years.
Gift of the Givers doesn’t have an office in Gaza. Instead, the team of three people moves around distributing medical supplies, food and water. They are also involved in a women and child care centre, a health facility, and schools.
Sooliman says the organisation wants to send more people. “We are preparing to send medical teams but only if it’s not any risk to them.” He says a ceasefire or safe corridor is needed before the teams can enter Gaza. The organisation has 40 medical personnel ready to go in, Sooliman told GroundUp.
On Sunday Gift of the Givers reported that the team has been under severe physical and mental stress.
In 2014 Israel attacked Gaza for seven weeks. Sooliman said his team is reporting that this time it’s completely different. “They said it’s so difficult to move around. There’s so much anxiety and so much fear. The amount of bombs being dropped has never happened before.”
On Tuesday the UN High Commissioner for Human Rights said that 4200 people have been killed, and over one million people displaced, in just ten days, while large areas of the Gaza strip have been reduced to rubble.
The death toll includes a large number of women and children, as well as at least 11 Palestinian journalists, 28 medical staff and 14 UN workers. It also includes over 1300 Israelis, mostly civilians, killed by Hamas on 7 October.
Sooliman said that Gaza’s people face challenges with access to food and water. “Because there’s no electricity, the sewage plants don’t work. Because they can’t do burials, the decomposed bodies are going to cause infections. Because hospitals don’t have antibiotics, there’s a threat of infection there.
“They managed to do some mass funerals yesterday. As the bodies are coming in they are doing it straight away. There are thousands of bodies lying under the rubble that they can’t reach. They don’t have the equipment, they don’t have the personnel, but above all, it’s bloody dangerous to get there,” said Sooliman.
Sooliman said that he had a meeting with the Egyptian ambassador and South Africa’s Foreign Affairs Department on Monday in an attempt to get a humanitarian aid corridor open. “We are also looking at flying supplies on a cargo plane from South Africa and sending trucks to the border in Cairo.”
Asked how this situation compared to other humanitarian relief efforts the organisation had been involved in, Sooliman responded: “This is the worst situation in the world because there is no exit route. You can’t get out. The area is so small. It’s so easy to bomb it … Nobody can have a safety plan. Where are you going to hide? There’s no such thing as safety in Gaza.”
Gaza is only 350km2. It could fit into Cape Town nearly seven times, yet it has half Cape Town’s population.
Sooliman described Israel’s call to evacuate more than one million people from the north to the south of Gaza as “quite ludicrous”. “How can you move 1 million people in 24 hours when there’s no fuel and no cars? Where are you going to go to? Everything is bombed. How do you move an intensive care unit patient?”
He also called for restraint from both sides. “Civilians cannot be attacked in a war and that applies to both sides … At the end of the day, both sides must remember that there is no winner in war. Everybody loses out. The only way to solve this problem in the Middle East is to make peace, act rationally and make compromises.”
“This is not a thing about Jews against Muslims; it’s human against human. It’s not a religious thing, it’s a human thing … it’s about humanity. It’s in the interests of all parties to make compromises. The only way to solve the problem is to do what is just,” he stressed.
“When you act justly you will have peace, prosperity and peace in the entire region. Nobody loses out. Actually everybody gains more. They should go to the negotiating table, make compromises and give a just solution. If you do that then we never have to send any more supplies to the Middle East again,“ Sooliman added.
Dr Bukiwe Spondo recently received the Rural Doctor of the Year award at the Rural Health Conference held in Chintsa in the Eastern Cape. PHOTO: Supplied
By Biénne Huisman for Spotlight
Describing the rutted gravel road between Butterworth and Tafalofefe District Hospital in the Eastern Cape, Dr Bukiwe Spondo uses the word “terrible” at least eighteen times. Dipping through the Amatole District, the 55-kilometre journey can take several hours. With heavy rain, tractors may be required to dislodge ambulances and often even staff have difficulty getting to work because of the mud.
Since 2007, Spondo and her colleagues have offered a multitude of services at Tafalofefe in the lush but impoverished Centane village. First off, she moved the hospital’s ARV clinic from an out-building to inside the premises – reducing stigma – “because if patients went into that building on the outside, automatically everyone knew,” she says.
In 2012, having observed how patients stopped taking treatment due to travel costs, she started driving up to 40 kilometres a day twice weekly to nine clinics in the area, where up to fifty patients would be queuing to see her. To make life easier for patients, she started pre-packing medication to take to them at the clinics. Later she opened a CHAMP (Clinical HIV /AIDS Management Programme) site at Tafalofefe to see complicated cases referred from the clinics, and a multi-drug-resistant TB (MDR-TB) review clinic in conjunction with Butterworth Provincial Hospital.
“As a rural doctor, you become a social worker, a pharmacist, a priest – you do everything,” she says, laughing.
Rural doctor of the year
Spondo’s efforts have not gone unnoticed. Last month at the Rural Doctor’s Association of South Africa (RuDASA’s) annual Rural Health Conference, she received the Rural Doctor of the Year award. RuDASA chairperson Dr Lungile Hobe conferred the award at the event hosted near Chintsa. Spondo is quick to point out that she also won an Amatole District leadership award last year.
Speaking to Spotlight over Zoom, she says, “So the roads here at Centane are terrible. It becomes a challenge to get ambulances through and the chopper cannot fly either when it’s raining. I mean, the other day a truck was stuck, crossing the road so the ambulance couldn’t pass. We had to take a private car from the hospital to go meet the ambulance halfway.”
She adds that the community hoped that roads would be improved after a devastating accident five kilometres from Tafalofefe in 2020 when an overloaded 65-seater bus plunged into a gorge, causing 25 deaths and 62 injuries. But, she says, the improvements never come.
At Tafalofefe, the two nearest referral hospitals are Cecilia Makiwane and Frere Provincial in East London, situated an additional 110 kilometres or 90-minute drive from Butterworth along the N2 highway. Housed in a pale building, Tafalofefe has 160 beds served by 41 professional nurses and seven doctors – including three community service doctors who joined last year. The additions have increased capacity, for example, emergency caesareans are now available around the clock.
Taking healthcare to the people
The hospital has three 4×4 bakkies [pick-ups] for visiting or transporting patients. It is in one of these that Spondo travels to see patients in remote corners between the Kobonqaba and Kei Rivers on Tuesdays and Thursdays.
“Clinics are part of decentralised primary healthcare goals,” she says. “But the problem was that if there were complicated cases – like if a patient is taking ARVs and then develop side effects, the sisters are not equipped to handle that. For example, if there is a kidney problem, they [cannot] do anything about that.
“And in time, I realised that for these people traveling to the hospital costs too much money. Let’s say, for example, the clinic at Qolora – for a person to travel from Qolora to Tafalofefe is R100. A return ticket is R200. And you know, most people here are unemployed. They can’t afford this. By the time they have saved up enough money to travel to the hospital, it’s too late. Like it would be the end stage of their kidney problem. You could not send this patient for dialysis, nothing could be done to help them. This is why I started my outreach trips.”
In motivating for Spondo to receive the RuDASA award, Tafalofefe’s CEO Masizakhe Madlebe pointed out how her work days start at 7am, only finishing once all patients had been seen, whether at the hospital or at one of the local clinics. In addition, he notes how, over the years, Spondo has mentored youth in the area, including children whose parents had succumbed to AIDS, and school girls on topics like life goals and contraceptives. He adds that Spondo even reached into her own pocket to pay school fees for children without parents.
Spondo relays how she noticed girls as young as twelve years old in their maternity ward, giving birth. “Myself and some nurses we went to two schools in the area to educate them, to discuss goals and contraceptives,” she says. “We started with grade 12 pupils. No teachers were present. It was just us and them. And I was surprised at how free they were talking. I said to them education is more important. I said to them – You see me? I am a doctor. One day you can be a doctor too, but you need to be educated. I told them they could come to Tafalofefe any time if they needed to talk, that I could help them apply for tertiary degrees, to college or to university.”
Spondo has kept a close eye on children orphaned by AIDS in the area. “I tell them to bring me their June, September, and December school reports, so I can see how they’re doing, so I can motivate them,” she says.
“These kids, I’ve seen them grow up. Some of them I saw angry – with everyone, with their own deceased parents. And I explained to them, don’t be angry. It’s not your mother’s fault. It’s not your father’s fault. It was the government’s fault for not giving your parents access to ARVs. But now, take your own ARVs and you will be fine. Some of them have passed high school with distinction, some even now have access to universities.”
Bringing her skills back home
Alongside two brothers whom she describes as “wonderful”, Spondo grew up in the village of Nqamakwe, on the opposite side of Butterworth. Her parents have passed away, but she still considers Nqamakwe her home. Here her family’s farming interests include cattle, goats, and sheep.
She attended Blythswood Secondary School in Nqamakwe – excelling at biology and physics, even though maths was hard work. “Becoming a doctor was just something I always wanted,” she says, relaying how in her formative years she had been a sickly child who often required medical care. This changed, she says, as she cannot remember ever being sick as an adult.
Spondo graduated from medical school at the University of KwaZulu-Natal in 2002, completing her internship at Cecilia Makiwane and her community service at Tafalofefe and Frere in 2004.
Speaking with rapid enthusiasm, she says how happy she is to bring her healthcare skills back home to serve the community that shaped her own humanity.
“I mean, I know these people inside out. I was born in front of them, raised in front of them,” she says. “These are our relatives, our aunts, our grannies. It’s giving back to them, to the community that raised you, that has done everything for you. Who supported you through all these years.”
She adds that Tafalofefe’s clinical manager, Sambona Ntamo, grew up near Butterworth too.
“Who would look after these people if we didn’t?” she asks.
Where does she find the resilience that drives her passion to care for sick people, often queuing at the end of long rutted roads?
“Lots of exercise,” she says, smiling.
At Tafalofefe there is a staff gym with a treadmill, a bicycle, weight lifts, and pilates balls.
“I tell the guys after work it’s gym time, it’s gym time, it’s gym time!” she says. “We’ve got a key and everyone knows that even if they want to go to the gym after midnight, they may get the key and go.”
Photographs capture an air of camaraderie at Tafalofefe. Staff sharing a meal of tripe and creamed spinach on heritage day, a farewell gathering for a retiring nurse with balloons and huge gifts in silver wrapping, [and] women knitting countless bright beanies for babies delivered in the maternity ward. A picture inside the hospital’s paediatric room shows youngsters on plastic motorbikes and mothers holding toddlers wrapped in blankets.
Spondo and her own eight-year-old son, Lutho desperately – which means the greatest one – live in a doctor’s house on the hospital’s premises. They travel to their family home in Nqamakwe over weekends.
For Spondo, being a doctor does not feel like a job. “When you do something you love, it doesn’t feel like a job,” she says. “Being a doctor is something I look forward to every morning. When patients return to me, saying they feel better with a smile on their faces, saying thank you for the treatment – that just makes my day.”