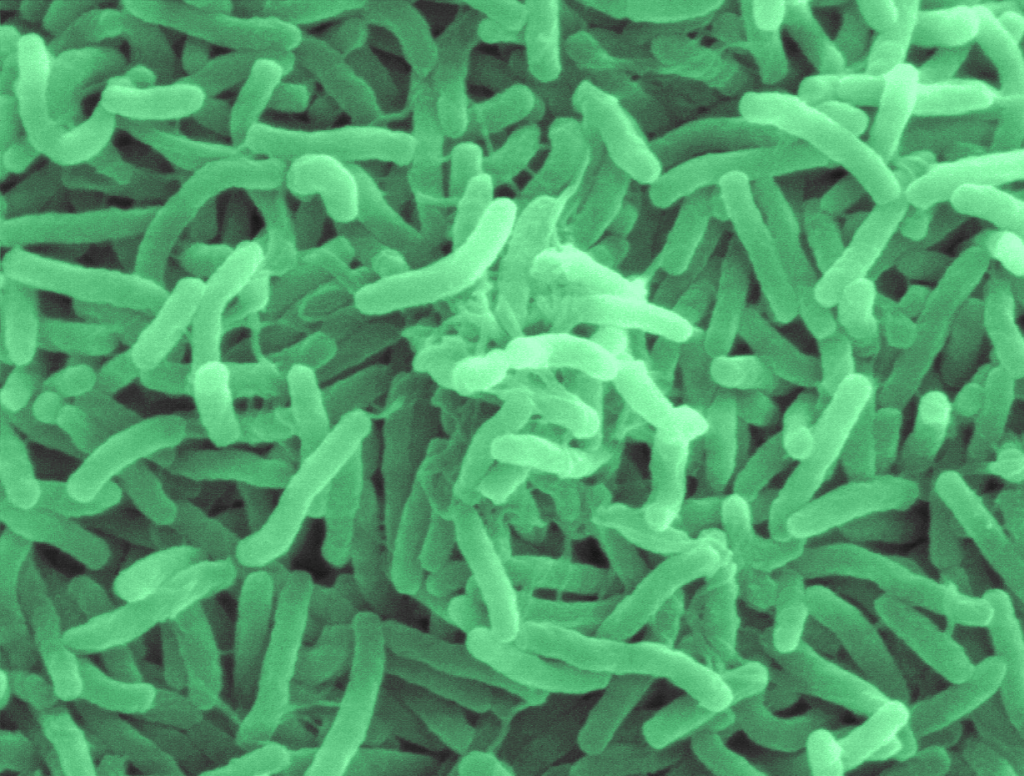
Scanning electron micrograph image of cholera bacteria.
Scientists from the National Reference Center for Vibrios and Cholera at the Institut Pasteur, in collaboration with the Centre hospitalier de Mayotte, have revealed the spread of a highly drug-resistant cholera strain from Yemen down through Africa. The study was published in the New England Journal of Medicine.
Cholera is caused by the bacteria Vibrio cholerae and in its most severe forms, it is one of the most rapidly fatal infectious diseases: in the absence of treatment, patients can die within hours. Treatment primarily involves replacing lost water and electrolytes, but antibiotics are also used in addition to rehydration therapy. They are essential in reducing the duration of infection and breaking chains of transmission as quickly as possible.
A strain resistant to ten antibiotics – including azithromycin and ciprofloxacin, two of the three recommended for treating cholera – was identified for the first time in Yemen during the cholera outbreak in 2018-2019[1].
Scientists have now been able to trace the spread of this strain by studying the bacterial genomes. After Yemen, it was identified again in Lebanon in 2022[2], then in Kenya in 2023, and finally in Tanzania and the Comoros Islands – including Mayotte, a French département off the south-east coast of Africa – in 2024. Between March and July 2024, the island of Mayotte was affected by an outbreak of 221 cases caused by this highly drug-resistant strain.
“This study demonstrates the need to strengthen global surveillance of the cholera agent, and especially to determine how it reacts to antibiotics in real time. If the new strain that is currently circulating acquires additional resistance to tetracycline, this would compromise all possible oral antibiotic treatment,” concludes Professor François-Xavier Weill, Head of the Vibrios CNR at the Institut Pasteur and lead author of the study.
Three influenza A (H5N1/bird flu) virus particles (rod-shaped). Note: Layout incorporates two CDC transmission electron micrographs that have been inverted, repositioned, and colourised by NIAID. Scale has been modified. Credit: CDC and NIAID
WHO spokesperson Dr Margaret Harris told reporters in Geneva that the H5N1 virus causing the disease is “not circulating in humans but jumping into humans” who are exposed to poultry or dairy cattle. “We’re not seeing sustained circulation,” she insisted.
Underlying conditions
The man who died of the disease in Louisiana was over 65 and reportedly had underlying medical conditions, Dr Harris said.
According to the health authorities, he had been exposed to chickens and wild birds. Several dozen people in the US have contracted avian influenza – commonly referred to as bird flu – during the current outbreak, mainly farmworkers in close contact with poultry flocks and cattle herds.
Dr Harris stressed that WHO’s assessment of the risk to the general population “is still low and remains set”. The main concern is for people who work in animal industries because they need to be better protected from infection.
The WHO spokesperson added that the United States was continuing to carry out “a lot of surveillance” in the human and animal population, “in the methods we use for farming, for our food production…all those things need to be combined because indeed it always does pose a risk”.
China respiratory virus is not new
Meanwhile, a respiratory virus gaining ground in China, known as the human metapneumovirus, or hMPV, has been sparking media attention in recent weeks, but it does not represent a new or major threat, Dr. Harris insisted.
The UN health agency spokesperson said that such infections are on the rise in China “as expected during winter”, with seasonal influenza being “by far the most common among them”, as reported by the Chinese Center for Disease Control and Prevention.
“China’s reported levels of respiratory infections are within the usual range for the winter season,” Dr. Harris explained. “Authorities report that hospital utilization is currently lower than this time last year, and there have been no emergency declarations or responses triggered,” she added.
As for hMPV, it was first identified in 2001 and “has been in the human population for a long time”, Dr. Harris clarified.
‘Very, very low’ risk
She added that it is a common virus that circulates in winter and spring and usually “causes respiratory symptoms similar to the common cold”.
Like any of the hundreds of common cold viruses known to exist, it can lead to more serious disease in patients with low immunity, particularly but not limited to newborns and the elderly.
Asked about hMPV’s mortality rate, Dr Harris described it as “very, very low”. It is not a pathogen that normally leads to deaths in humans, save for the most vulnerable, she concluded, recommending “simple” prevention measures, such as wearing a mask, improving ventilation of closed spaces and handwashing.
Electron micrograph imagery of Treponema pallidum, the bacteria that cause syphilis, including a foreground close-up of a single particle (right). Spiral-shaped bacteria are colourised in gold. Credit: NIAID
A research team led by members of the Max Planck Institute for Evolutionary Anthropology has taken a crucial step towards resolving a long-standing controversy – was syphilis introduced to Europe from the Americas at the end of the 15th century, or had it been there all along? Ancient pathogen genomes from skeletons that pre-date 1492 confirm its introduction from the Americas, but its world-wide spread remains a grim legacy of the colonial period.
In spring 1495, the Italian campaign of Charles VIII of France was interrupted by an intense outbreak of an apparently unknown illness – a disease of high mortality that quickly engulfed the whole of Europe and left its survivors with life changing impairments to their bodies and minds. This documented epidemic is now interpreted to be the first historical account of syphilis.
The origin of syphilis is the subject of a decades-long debate. The late 15th century outbreak occurred shortly after the return of Columbus and his crew from their early expeditions to the Americas, which led some to believe that contact with new lands and people may have had something to do with the sudden disease onset. Though many communicable diseases made a westward journey from Europe to the Americas during the early colonial period where they imparted devastating consequences on indigenous groups, syphilis is one of the few that possibly made the reverse journey.
This “Columbian theory” for syphilis has gained popularity over the years, but still has its critics. Its simple narrative starts to unravel when experts turn their attention to lesions seen in bones from Mediaeval Europe. Both long-term sufferers and those born with an infection can develop changes in their bones or teeth, and over the past several decades, a number of such skeletons have been found in Europe that predate 1492. Many now believe the history of syphilis in Europe began long before Columbus, and the late 15th century pandemic happened for reasons independent of new contacts. But neither theory has been confirmed.
Analysing five ancient pathogen genomes
Pathogen DNA retrieved from archaeological bone has the potential to tip the scales in support of one theory over another. It has already told us volumes about the deep history of plague, tuberculosis, leprosy, and smallpox, though unthreading the history of syphilis has proven more challenging. “Several genomes from the syphilis family have been reconstructed from archaeological bone, but these haven’t been able to address core questions related to the pre- or post-Columbian theories surrounding syphilis”, says Kirsten Bos, group leader for molecular paleopathology at the Max Planck Institute for Evolutionary Anthropology.
A new study led by Bos and Johannes Krause, director of the Department of Archaeogenetics at the Max Planck Institute for Evolutionary Anthropology in Leipzig, has taken a critical step toward resolving this debate. Working with scientists and archaeologists from several countries in the Americas, the study focused on archaeological bone from these regions, where infections that left lesion patterns similar to syphilis are apparent from deep time periods. It is published in Nature.
“We’ve known for some time that syphilis-like infections occurred in the Americas for millennia, but from the lesions alone it’s impossible to fully characterise the disease”, comments Casey Kirkpatrick, a postdoctoral researcher and paleopathologist who contributed to the current study. Bone pathology also cannot tell us whether the disease originated in the Americas, or if it came from Asia deep in our past and merely accompanied groups during the early peopling events of the Americas some 15000 years ago.
Using state of the art techniques, the team was able to recover and analyse five ancient genomes of the syphilis disease family from Mexico, Chile, Peru, and Argentina. Computational microbiologist and postdoctoral researcher Lesley Sitter undertook the task of putting together the ancient molecular puzzles and adds “while preservation posed some analytical challenges, we were able to confidently determine the relationships between these extinct forms and the strains that impact global health today”.
Syphilis family of diseases in the Americas pre-dates “Columbus”
Syphilis is part of a small family of diseases that also includes yaws and bejel, both classified as neglected tropical diseases that are found in equatorial regions across the globe. Postdoctoral researcher Rodrigo Barquera has worked previously with archaeological bone from colonial Mexico, and has confirmed the presence of both syphilis and yaws in Mexico City by the 17th century.
Drawing upon the latest ancient genomic data, it is now clear that the Americas were a hub for ancient diversity within this disease group before the arrival of Columbus. “We see extinct sister lineages for all known forms of this disease family, which means syphilis, yaws, and bejel are the modern legacies of pathogens that once circulated in the Americas”, asserts Barquera.
“The data clearly support a root in the Americas for syphilis and its known relatives, and their introduction to Europe starting in the late 15th century is most consistent with the data”, adds Bos. Subsequent to this, an explosion in cases of syphilis and yaws seems to have occurred around AD 1500. This is likely behind the breadth and intensity of the 16th century outbreak in Europe, whose global spread was facilitated by human trafficking networks and European expansions across the Americas and Africa in the decades and centuries that followed. “While indigenous American groups harboured early forms of these diseases, Europeans were instrumental in spreading them around the world,” she concludes.
With support for an American origin of syphilis, how does the current narrative square up with the evidence of syphilis-like bone lesions that many claim to have identified in pre-1492 Europe? “The search will continue to define these earlier forms, and ancient DNA will surely be a valuable resource”, comments Krause. “Who knows what older related diseases made it around the world in humans or other animals before the syphilis family appeared.”
Debilitating chronic fatigue syndrome creates conditions T cells becomes exhausted, according to a new study published in Proceedings of the National Academy of Sciences. The findings point the way for important new lines of investigation.
The study’s authors knew the immune system was dysregulated in patients with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), so they began by asking, which parts shift with the condition? A systematic exploration revealed that key CD8+ T cells displayed one of the most pronounced signatures of dysregulation, with signs of constant stimulation that lead to an exhausted state, a condition that is well-studied in cancer.
ME/CFS affects an estimated 3 million people in the United States and some 65 million worldwide, leaving some patients ill for decades and unable to work. Symptoms include overwhelming fatigue that is not helped by rest, and can also include brain fog, body pains, headaches, difficulty sleeping and prolonged increases in symptoms after mild physical exertion or exercise. Causes are unknown and there is no treatment for the disease.
“This is an important finding for ME/CFS because now we can examine the T cells more carefully, and hopefully by looking in the exhausted cells we can start to get hints as to what they are responding to,” said Andrew Grimson, professor of molecular biology and genetics in the College of Arts and Sciences.
Grimson is co-corresponding author of the study. Maureen Hanson, Professor in the Department of Molecular Biology and Genetics, is the other corresponding author.
“Therapies have been developed to reverse T cell exhaustion as treatments for cancer,” Hanson said. “Our findings raise the question of whether such anti-exhaustion drugs might also be helpful in ME/CFS.”
Strong evidence for the phenomenon of T cell exhaustion in ME/CFS has also been reported in long COVID, Hanson added.
The study was led by co-first authors David Iu, a doctoral student in Grimson’s lab, and Jessica Maya, PhD ‘24, formerly in Hanson’s lab and currently a researcher at the Centers for Disease Control and Prevention.
In a paper published earlier this year, Grimson and collaborators used a technology called single cell RNA sequencing to examine and identify all the circulating immune cells in ME/CFS patients. In the current paper, they used that data to examine which of the different types of T cells, including CD8+ T cells, were most altered in ME/CFS patients.
“That pointed us in the direction of CD8+ cells,” Grimson said. After purifying those cells, they used additional advanced technologies to precisely determine which genes were being expressed and pinpoint which genes were getting switched on or off.
“When we looked at all of the differences [compared to normal functioning], they really pointed us towards an exhaustion-like state for the CD8+ T cells,” Grimson said.
Meanwhile, in Hanson’s lab, Maya led a different approach of purifying patients’ T cells and then determining expression patterns of proteins on the surface of these cells. The team examined two series of different markers on the various proteins, one of which allowed them to subdivide all the different types of CD8+ T cells, while the other allowed them to detect proteins known to be involved in exhaustion.
“Immune cells from ME/CFS patients exhibited higher levels of proteins on their surface that are characteristic of cells that have become exhausted, which can be caused by long-term exposure to a virus protein or by continuous stimulation of the immune system, a state that is also found in cancer patients,” Hanson said.
Future work will try to determine whether a virus is in fact involved, which is currently not known. “We need to understand what is pushing them to this exhausted state,” Grimson said.
The team also plans to take cells from patients and controls, purify those cells and treat patients with drugs that reverse exhaustion and see if the immune cells resume normal function. If CD8+ T cell exhaustion can be reversed, the next question is whether such reversal actually benefits a patient, as exhaustion can have protective qualities.
Another future line of inquiry will include distinguishing T cell receptors in exhausted cells from patients, to try to find which molecules those T cell receptors are recognising, and if from those clues, they can work out whether specific pathogens are involved.
Hepatitis B virus (HBV) infection is a leading cause of chronic liver diseases, that spreads among individuals through blood or body fluids. According to the World Health Organization, globally 1.2 million new HBV infections are reported every year – most in low- and middle-income countries. HBV infections are limited to a few species, including humans and chimpanzees. Despite their close evolutionary relationship with these animals, old-world monkeys are not susceptible to HBV infections.
In a new study published in Nature Communications, scientists led by Visiting Professor Koichi Watashi from the Tokyo University of Science to uncover why monkeys are naturally resistant to HBV infection.
Using cryo-electron microscopy, scientists solved the structure of a membrane receptor found in liver cells called the sodium taurocholate co-transporting polypeptide (NTCP) in macaques. HBV binds to human NTCP using its preS1 region in the surface protein. Prof Watashi explains, “We identified a binding mode for NTCP-preS1 where two functional sites are involved in human NTCP (hNTCP). In contrast, macaque NTCP (mNTCP) loses both binding functions due to steric hindrance and instability in the preS1 binding state.”
To understand this ‘interspecies barrier’ against viral transmission, Prof Watashi and his team compared the structures of hNTCP and mNTCP, identifying differences in amino acid residues critical for HBV binding and entry into liver cells. hNTCP and mNTCP share 96% amino acid homology, with 14 amino acids distinct between the two receptors. A key distinction among these differences is the bulky side chain of arginine at position 158 in mNTCP, which prevents deep preS1 insertion into the NTCP bile acid pocket. For successful viral entry into liver cells, a smaller amino acid like glycine, as found in hNTCP, is necessary.
Interestingly, the substitution of Glycine by Arginine in mNTCP was at a position far away from the binding site for bile acid. Prof Watashi adds, “These animals probably evolved to acquire escape mechanisms from HBV infections without altering their bile acid transport capacity. Consistently, phylogenetic analysis showed strong positive selection at position 158 of NTCP, probably due to pressure from HBV. Such molecular evolution driven to escape virus infection has been reported for other virus receptors.” Further lab experiments and simulations revealed that an amino acid at position 86 is also critical for stabilising NTCP’s bound state with HBV’s preS1 domain. Non-susceptible species lack lysine at this position, which has a large side chain; macaques instead have asparagine, which contributes to HBV resistance.
The researchers also noted that bile acids and HBV’s preS1 competed to bind to NTCP, where the long tail-chain structure of the bile acid inhibited the binding of preS1. Commenting on these findings, Prof Watashi stated, “Bile acids with long conjugated chains exhibited anti-HBV potency. Development of bile acid-based anti-HBV compounds is underway and our results will be useful for the design of such anti-HBV entry inhibitors.”
By unravelling the structure of mNTCP and pinpointing the amino acids that facilitate viral entry into liver cells, researchers have opened the door to new therapeutic avenues. Furthermore, the implications extend beyond HBV, offering critical insights into other viruses, including SARS-CoV-2, and their potential to cross species barriers. This research not only enhances our understanding of viral dynamics but also serves as a crucial tool in the ongoing quest to predict and prevent future pandemics.
The future of global health hinges on these revelations, promising a path toward more equitable access to treatments and a stronger defence against emerging viral threats.
Indiana University School of Medicine researchers, in collaboration with colleagues at Makerere University in Uganda, have uncovered evidence of partial resistance to artemisinin derivatives – the primary treatment for malaria – in young children with severe, or “complicated,” malaria.
Earlier studies have shown partial resistance to artemisinin in children with uncomplicated malaria, but the new study, published in the Journal of the American Medical Association (JAMA), is the first to document such resistance in African children with well-defined signs of severe disease from malaria.
“Artemisinin-based therapies have been quintessential in the fight against malaria for the past 20 years,” said corresponding author Chandy C. John, MD, the professor of paediatrics at the IU School of Medicine. “Growing evidence of artemisinin partial resistance in African children with uncomplicated malaria has led to concerns that new therapies, like triple artemisinin combination therapies, may be needed in uncomplicated malaria. The findings of artemisinin partial resistance in children with severe or complicated malaria, as well as the findings of a high rate of recurrent malaria with current standard treatment in these areas raise the question of whether new treatments are needed for severe malaria as well.”
Led by John and co-authors Ruth Namazzi, MBChB, MMEd, and Robert Opoka, MD, MPH, of Makerere University; Ryan Henrici, MD, PhD, of the University of Pennsylvania; and Colin Sutherland, PhD, MPH, of the London School of Tropical Medicine and Hygiene, the study examined 100 Ugandan children aged 6 months to 12 years who were undergoing treatment for severe malaria complications caused by Plasmodium falciparum, the deadly malaria parasite transmitted by mosquitos.
In the study, 10 children had parasites with genetic mutations previously associated with artemisinin partial resistance. The most common mutation, which was seen in eight of these children, was associated with a longer parasite clearance half-life — the time it takes the parasite’s burden in the body to reach half of its initial level. The study also showed that 10% of children returned within 28 days of treatment with an infection from the same malaria strain they had during their original admission. These were all children who had received complete intravenous and then oral treatment for severe malaria, and all had cleared the parasite by microscopic examination. John said these findings suggest that the standard intravenous and oral treatment lowers the parasite level to where it cannot be detected by microscopy, but it does not completely eliminate the parasite in some children.
Reports of artemisinin resistance first surfaced in Southeast Asia in 2008 before emerging in East Africa, a trend the IU research team unexpectedly observed through their ongoing work in Uganda. While studying why severe malaria develops in children, the researchers noticed slower responses to artemisinin in some of their Ugandan study participants, prompting the present study.
“The study findings point to a need for more data on artemisinin resistance and recurrence of clinical malaria in children with severe malaria,” John said. “If our study findings are confirmed in other areas, that would suggest that treatment guidelines for severe malaria may require revision.”
John presented the study’s results at the Annual Meeting of the American Society of Tropical Medicine and Hygiene on Nov. 14 in New Orleans, Louisiana.
This illustration depicts a 3D computer-generated image of a group of Gram-positive, Streptococcus pneumoniae bacteria. The artistic recreation was based upon scanning electron microscopic (SEM) imagery. Credit: CDC on Unsplash
A concerning increase in global rates of severe invasive infections becoming resistant to key antibiotics has a team of infectious disease researchers at the Houston Methodist Research Institute studying a recently emerged strain of bacteria, Streptococcus dysgalactiae subspecies equisimilis (SDSE). SDSE infects humans via the skin, throat, gastrointestinal tract and female genital tract to cause infections ranging in severity from pharyngitis to necrotising fasciitis. The findings of this study are described in a paper appearing in the journal mBio.
Though closely related to group A streptococcus (also commonly known as Streptococcus pyogenes), which has been very well studied, little is known about SDSE.
“Given its great emerging importance to human health, our limited understanding of SDSE molecular pathogenesis is remarkable,” said Jesus M. Eraso, PhD, an assistant research professor of pathology & genomic medicine with Houston Methodist and lead author on the study.
To close this knowledge gap, the Houston Methodist team used a sophisticated integrative approach to study 120 human isolates of a particular SDSE subtype, called stG62647. They analysed the subtype’s genome, where the information of its DNA is stored, its transcriptome, which provides a snapshot of the complete gene expression profile at the time the SDSE cells were collected, and its virulence, which refers to the degree of damage it causes to its host. The stG62647 SDSE strains are important to study because they have been reported to cause unusually severe infections, and understanding the relationships and interplay between these three entities gave the researchers a richer understanding of how it causes disease.
The data from this integrative analysis provided much new data about this important emerging human bacterial pathogen and are useful in vaccine research. It also raised many new questions and generated new hypotheses to be studied in this ongoing line of investigation.
In people with a rare condition called light chain amyloidosis, light chain proteins – which are a component of antibodies – mutate and build up in different organs. In new research published in The FEBS Journal, investigators have identified and characterised an antibody fragment that can bind to abnormal light chains to stabilise them and prevent their aggregation.
The findings could have an important clinical impact because the current prognosis for individuals with light chain amyloidosis is extremely poor, and current treatments, which rely on attacking the defective light chain–producing cells, are difficult to tolerate.
The results may also be applicable to other forms of amyloidosis, including Alzheimer’s disease.
“We are excited by this finding, which has potential to provide a much-needed treatment for people diagnosed with light chain amyloidosis,” said corresponding author Jillian Madine, PhD, of the University of Liverpool, in the UK.
A new study reveals widespread resistance of a major bacterial pathogen to the active ingredients in cleaning agents commonly used in hospitals and homes. The American Chemical Society Infectious Diseases published the research led by chemists at Emory University. It demonstrates the surprising level of resistance to cleaning agents of multidrug-resistant Pseudomonas aeruginosa, a pathogen of particular concern in hospital settings.
The study also identifies biocides that are highly effective against P. aeruginosa, including a novel compound developed at Emory in collaboration with Villanova University. The researchers describe how these biocides work differently than most disinfectants currently in use.
“We hope our findings can help guide hospitals to reconsider protocols for the sanitation of patient rooms and other facilities,” says William Wuest, Emory professor of chemistry and a senior author of the study. “We also hope that our findings of a new mechanism of action against these bacterial strains may help in the design of future disinfectant products.”
First authors of the study are Christian Sanchez (who did the work as an Emory PhD student in chemistry and, following graduation, joined the faculty at Samford University) and German Vargas-Cuebas, an Emory PhD candidate in microbiology through Laney Graduate School.
“Resistance of pathogens to cleaning agents is an area that’s often overlooked,” Vargas-Cuebas says, “but it’s an important area of study, especially with the rise in antibiotic-resistant pathogens worldwide.”
Kevin Minbiole, professor of chemistry at Villanova, is co-senior author of the paper.
Workhorse disinfectants losing steam
Quaternary ammonium compounds, or QACs, are active ingredients commonly seen in household and hospital cleaners, including some disinfectant sprays and liquids, antibacterial sanitizing wipes and soaps.
“There are a handful of QACs that have been the workhorse disinfectants for around 100 years, on the frontline of most homes and hospitals,” Wuest says. “Very little has been done to modify their structures because they have long worked so well against many common bacteria, viruses, molds and fungi and they’re so simple and cheap to make.”
The Wuest lab is a leader in studies of QACs and other disinfecting agents. One issue Wuest and his colleagues have identified is that some bacterial strains are developing resistance to QACs. That trend could cause serious problems for sanitation in hospitals.
A pathogen of critical priority
More than 2.8 million antimicrobial-resistant infections occur in the United States each year, leading to more than 35,000 deaths, according to the Centers for Disease Control and Prevention (CDC).
The CDC names multidrug-resistant P. aeruginosa as one of seven pathogens causing infections that increased in the United States during the COVID-19 pandemic and remain above prepandemic levels.
Worldwide, P. aeruginosa causes more than 500,000 deaths annually and has been named a pathogen of critical priority by the World Health Organization.
P. aeruginosa is commonly found in the environment, including in soil and freshwater. Reservoirs in hospital settings can include drains, taps, sinks and equipment washers.
While the bacterium generally does not affect healthy people it can cause infections in individuals with cystic fibrosis and those who are immunocompromised, such as patients with burns, cancer and many other serious conditions. Patients with invasive devices such as catheters are also at risk due to the ability of P. aeruginosa to form biofilms on the surfaces of these devices.
P. aeruginosa, like other gram-negative bacteria, is enclosed in a second, fatty outer membrane that acts as a protective capsule, making it more difficult to kill.
How QACs kill
QACs have a nitrogen atom at the center of four carbon chains. In simplest terms, the positively charged head of the nitrogen center is drawn to the negatively charged phosphates of the fatty acids encasing P. aeruginosa and many other bacteria and viruses. The heads of the carbon chains act like spearpoints, stabbing into both protective fatty membranes and inner cellular membranes and causing pathogens to disintegrate.
The researchers tested 20 different drug-resistant strains of P. aeruginosa collected from hospitals around the world by the Walter Reed National Military Medical Center as part of the Multidrug-Resistant Organism Repository and Surveillance Network.
The results showed that all 20 strains were at least partially resistant to QACs — the common active ingredient in most front-line cleaning agents — and 80% of the strains were fully resistant to QACs.
“This mechanism has worked for 100 years essentially by slicing into the outer and inner membranes of a pathogen and destroying them,” Wuest says. “We were surprised to see the level at which that appears to no longer be the case.”
Improper use of cleaning agents may be one factor leading to resistance, Wuest theorizes.
“QACs don’t immediately kill,” he explains. “After application, it’s important to wait four or five minutes before wiping these cleaning agents away. It’s also important to use the right concentration. If used inappropriately, some bacteria can survive, which can lead to them developing resistance.”
Greater use of cleaning agents during the COVID-19 pandemic may have given P. aeruginosa and some other hard-to-kill pathogens more opportunities to develop resistance, he adds.
A new method that ‘works surprisingly well’
For the current paper, the researchers also tested the resistance of the panel of multidrug-resistant P. aeruginosa strains against a new quaternary phosphonium compound, or QPC, developed in the Wuest and Minbiole labs. The results showed that the compound was highly effective at killing all 20 of the resistant P. aeruginosa strains.
“It works surprisingly well even at a low concentration,” Vargas-Cuebas says.
The researchers demonstrated that their novel QPC works not by piercing the protective outer capsule of a P. aeruginosa bacterium but by diffusing through this outer membrane and then selectively attacking the inner cellular membrane.
“It’s counterintuitive,” Wuest remarks. “You would think that the approach of conventional biocides, to take out both membranes, would be a more effective way to kill P. aeruginosa. Why does passively diffusing through the outer membrane and focusing on attacking the inner membrane make our QPC compound more effective? We don’t know yet. It’s like a magic trick.”
They showed that this same mechanism underlies the effectiveness of two commercial antiseptics: octenidine, more commonly used in Europe as a hospital antiseptic, and chlorhexidine, a common ingredient in mouthwashes.
Wuest and colleagues plan to continue research into how this newly identified mechanism may work against an array of pathogens and how that might translate into new biocides and more effective cleaning protocols in hospitals and other settings.
“Our work is paving the way for much-needed innovations in disinfectant research,” Wuest says.
The portion of our nervous systems responsible for the “fight or flight” response can shape the severity of potentially deadly Clostridioides difficile infections, new research from the School of Medicine reveals in Cell Reports Medicine.
The findings suggest that doctors may be able to save patients from the infections – a plague for hospitals and nursing homes – by using drugs to quiet the hyperactive nervous system response, the researchers say.
“Compared to how much we know about immune system influences in C. difficile infections, the field is just scratching the surface in understanding neuronal contributions to disease,” said researcher William A. Petri Jr., MD, PhD, of UVA Health’s Division of Infectious Diseases and International Health. “Newly identifying components of the nervous system that worsen inflammation will allow us to determine potential therapeutic targets and biomarkers for patients at risk of severe disease.”
C. difficile, is a perpetual burden for healthcare facilities. Extensive antibiotic use, particularly among patients who are hospitalised or in nursing care, can allow it to establish dangerous infections. Further, patients who make it through the severe diarrhoea, nausea, fever and colitis C. difficile can cause are not necessarily in the clear: One in six will develop another C. diff infection within eight weeks, according to the federal Centers for Disease Control and Prevention.
The new UVA research reveals the critical role the nervous system plays in severe C. difficile infections. The researchers found that the “sympathetic” nervous system – the branch that responds to dangerous situations – can be a key driver of serious C. diff.
Normally, our “fight or flight” response is helpful for avoiding danger. It helps us respond quickly, improves our eyesight, boosts our strength. It also can stimulate our immune system and help us recover from injury. But in C. difficile cases, the nervous system can have a hyperactive response that becomes part of the problem, and UVA’s new research explains why.
“Neurons are the first responders that coordinate defences against toxic attacks. Sometimes those responders don’t recruit the right size and kind of artillery and that can make things worse,” said researcher David Tyus, a neuroscience graduate student at UVA. “Interestingly, the receptor we identified as important in C. difficile infection [the alpha 2 adrenergic receptor] has also been linked to irritable bowel syndrome. I’m curious to know if there could be a unifying underlying mechanism between the two disease contexts.”
Promisingly, the researchers found that targeting the receptor in lab mice reduced intestinal inflammation and decreased C. difficile severity and mortality. That suggests that, with further research, doctors may be able to take a similar tact to better treat severe C. diff infections in patients. For example, they may be able to surgically remove a portion of nerves in the gut, or they may be able to develop medicines to target the alpha 2 receptor – as Petri and Tyus are attempting to do.
“Our next step is to determine which cells with the alpha 2 receptor are receiving signals from the sympathetic nervous system and play a role in C. difficile-mediated disease,” Petri said. “We are very excited to think about how our findings translate to clinic and how the sympathetic nervous system might play a role in recurrent infection. I hope that this study sets the foundation for future findings of how neurons affect the course of C. difficile infection outcomes.”