Like statins, cholesterol absorption inhibitors are linked with a lower risk of developing liver cancer.
Photo by Towfiqu Barbhuiya on Unsplash
Past studies have suggested that taking cholesterol-lowering statin drugs may lower the risk of developing liver cancer. In a new study of non-statin cholesterol-lowering medications, one type was linked to lower risks of liver cancer. The findings are published by Wiley online in CANCER, a peer-reviewed journal of the American Cancer Society.
Cholesterol absorption inhibitors, bile acid sequestrants, fibrates, niacin, and omega-3 fatty acids are types of non-statin cholesterol-lowering medications prescribed to manage cholesterol and lipid levels. The different classes of drugs work in different ways. A team led by Katherine A. McGlynn, PhD, MPH, of the National Cancer Institute, looked for associations between these five types of non-statin cholesterol-lowering medications and risk of liver cancer, the sixth most commonly occurring cancer globally and the third leading cause of cancer mortality.
The investigators used information from the Clinical Practice Research Datalink (CPRD), a primary care database that covers approximately 7% of the United Kingdom population. Their analysis included 3719 liver cancer cases and 14 876 matched controls without cancer. Additional matches were also made based on individuals’ type 2 diabetes and chronic liver disease status.
Use of cholesterol absorption inhibitors was associated with 31% lower odds of liver cancer risk in the overall analysis. These medications were also linked with a lower risk of liver cancer in analyses based on diabetes and liver disease status. The study also confirmed that statins were associated with 35% lower odds of liver cancer.
No associations with liver cancer risk were observed for fibrates, omega-3 fatty acids, or niacin. While bile acid sequestrant use was associated with higher odds of liver cancer risk in the overall analysis, the results of analyses based on diabetes and liver disease status were inconsistent, suggesting that replication of these observations is important.
“As few studies have examined the effects of non-statin cholesterol-lowering drugs on liver cancer risk, the results of our study require replication in other populations. If our findings are confirmed in other studies, however, our results may inform liver cancer prevention research,” said Dr. McGlynn.
Why do new comorbidities arise because of ischaemic stroke? A study from Germany recently published in the journal Cell has discovered why this can happen – and ways in which it might be countered. The findings from the study show that the immune system is involved in damage to other organs, including the heart.
Besides the early mortality and morbidity resulting from the ischaemic brain injury itself, long-term morbidity after stroke is also due to the high prevalence of secondary comorbidities and complications, such as cognitive impairment and dementia, post-stroke depression, cardiac events, persistent vascular inflammation, and stroke-induced metabolic disturbances.
Liesz is the principal investigator of this new study. The researchers worked on the hypothesis that the high rate of comorbidities that develop after a stroke could have a common immunological cause. And they actually managed to find it: the origin of the dysfunctions in other parts of the body lies in the immunological memory of the blood-forming cells in bone marrow.
Using single-cell sequencing techniques, Liesz and his team demonstrated the presence of permanent proinflammatory changes in the transcriptome of certain immune cells (monocytes/macrophages) in several organs. In other words, certain gene segments are transcribed differently there after the stroke, which unbalances the proteome. These epigenetic modifications occur most frequently in the heart, where they can cause scarring and impair pumping function. “We managed to identify the protein IL-1b as the main culprit for the epigenetic modifications that affect immunological memory after a stroke,” says Liesz.
Promising therapeutic approaches on the horizon
The researchers demonstrated in a mouse model the connection between modified blood formation in bone marrow through overexpressed IL-1b and cardiac dysfunctions. Moreover, they showed that blocking IL-1b and inhibiting migration of the proinflammatory cells to the heart both successfully prevented cardiac problems after a stroke.
“These findings are hugely significant, as they open up the promise of effective therapeutic approaches for the prevention of secondary cardiac conditions after a stroke,” reckons Liesz.
The authors of the study believe that the epigenetic mechanisms they described for the reprogramming of the immune system in the brain-heart axis will create a new framework for explaining the development of various IL-1b-mediated comorbidities.
In the US, nearly 40 million adults have sleep apnoea, and more than 30 million of them use a continuous positive airway pressure (CPAP) machine while sleeping. But the machines tend to be expensive, clunky and uncomfortable – resulting in many users giving up on using them.
Hypertension is often linked with sleep apnoea because the brain works harder to regulate blood flow and breathing during sleep. A recent study at the University of Missouri (Mizzou) offers new insight into the underlying mechanisms within the brain contributing to hypertension for those with sleep apnoea.
The findings, which are published in the Journal of Physiology, can help pave the way for new drugs that target the brainstem to bring blood pressure back down to normal levels for those with sleep apnoea.
The study took place in the lab of David Kline, a professor in Mizzou’s College of Veterinary Medicine and researcher at the Dalton Cardiovascular Research Center.
“When oxygen levels in the blood drop during sleep apnoea, the forebrain sends warning signals to the brainstem area that controls heart and lung functions,” Kline said. “By studying these signals, we found that two neurochemicals, oxytocin and corticotropin-releasing hormone (CRH), cause the brainstem to become overactive. Over time, this leads to hypertension.”
Hypertension leads to an increased risk of stroke, complications in the metabolism and a variety of other health issues.
“Not only do those with sleep apnoea often have high blood pressure, but they also lose a lot of sleep, they have more cognitive and memory issues, and they are more prone to injury at work due to sleepiness,” Kline said.
By being the first to identify the role that oxytocin and CRH play in strengthening and overexciting the pathways and mechanisms involved in sleep apnoea, Kline and his fellow researchers hope to pave the way for the design of better therapeutic approaches for humans and animals.
“Our ultimate goal is to eventually help clinicians develop specific drugs to target either these neurochemicals or the proteins they bind to in a way that reduces high blood pressure,” Kline said. “This discovery opens the door for future research to block the pathways these neurochemicals use, ultimately helping to bring blood pressure back to normal levels.”
A new study shows that women lose more years of life after a heart attack than men. A 50-year-old woman with a large heart attack loses an average of 11 years, while an 80-year-old man with a small heart attack loses an average of 5 months of life. The results of the study, led by researchers at Karolinska Institutet and Danderyd Hospital, are published in the journal Circulation.
The new study examined 335 000 individuals with first-time myocardial infarction registered in the SWEDEHEART quality registry during the period 1991-2022. The individuals with myocardial infarction were compared with 1.6 million individuals without myocardial infarction using data from Statistics Sweden and the National Board of Health and Welfare. Using the comparator population and new statistical methods, the difference in life expectancy between heart attack individuals and comparison individuals could be calculated, providing a measure of how much life expectancy was shortened due to the disease.
“We found that there were large differences between groups. Women and young individuals lost the most life expectancy when they had a heart attack. If the cardiac function was impaired after the infarction, the effects were even greater. For example, a 50-year-old woman with impaired cardiac function loses an average of 11 years in 2022 compared to an 80-year-old man with normal cardiac function who loses an average of 5 months in life expectancy,” says first author Christian Reitan, researcher at the Department of Clinical Sciences, Danderyd Hospital, Karolinska Institut.
Parameters affecting heart attack risk
The researchers were also able to take into account differences in income, education, other illnesses and medication at the time of the illness – which helped to measure the effect of the heart attack itself when everything else was taken into account.
“The results showed that a fairly large part of the reduction in life expectancy disappeared, that is, much of the reduction in life expectancy is explained by factors other than the heart attack itself, but which may still be associated with heart attack, such as socioeconomics or other diseases such as hypertension and diabetes. Provided that the patient had preserved cardiac function, we saw that the gender difference had disappeared. We interpret this to mean that the effect of the heart attack, and thus also the care for heart attacks, is similar between the sexes and that the large reduction in life expectancy we see in women is due to differences in risk factors, other diseases and socioeconomics,” says Christian Reitan.
According to the researchers, there is a lack of individualized heart attack care in Sweden for women. The study shows that women who have a heart attack lose more years of life than men of the same age.
“If a woman had impaired cardiac function, the gender difference was large. We don’t have the data to answer why, but it raises questions about whether women get as good follow-up and treatment for heart failure as men, or whether it is simply a more serious condition for a woman. Our findings are important because they challenge existing guidelines for heart attack treatment today. By identifying high-risk groups, we can hopefully better tailor treatment to the individual. We believe that ‘years of life lost’ is a good and easy-to-understand measure of risk for both doctors and patients. It makes it easier for us to assess and communicate the seriousness of the disease,” concludes Christian Reitan.
For decades, it’s been thought that people with heart failure should drastically reduce their dietary salt intake, but some studies have suggested that salt restriction could be harmful for these patients. A recent review in the European Journal of Clinical Investigation that assessed all relevant studies published between 2000 and 2023 has concluded that there is no proven clinical benefit to this strategy for patients with heart failure.
Most relevant randomised trials were small, and a single large, randomised clinical trial was stopped early due to futility. Although moderate to strict salt restriction was linked with better quality of life and functional status, it did not affect mortality and hospitalisation rates among patients with heart failure.
“Doctors often resist making changes to age-old tenets that have no true scientific basis; however, when new good evidence surfaces, we should make an effort to embrace it,” said author Paolo Raggi MD, PhD, of the University of Alberta.
A new study led by an investigator from Brigham and Women’s Hospital, evaluated a cuffless monitor that uses optical sensors to record blood pressure continually and efficiently, without disruption to the patient. The study, published in Frontiers in Medicine, highlights promising advancements in hypertension diagnosis, risk assessment and management that may be enabled by use of cuffless devices.
“The successful management of hypertension depends on patients being able to take blood pressure measurements easily and reliably outside of the traditional doctor’s office setting,” said corresponding author Naomi Fisher, MD, of the Division of Endocrinology, Diabetes and Hypertension at Brigham and Women’s Hospital. “Cuffless devices have the potential to revolutionise hypertension management. They provide many more readings than traditional devices, during both the day and night, which can help confirm the diagnosis of hypertension and guide medication titration.”
Medical guidelines increasingly recommend the incorporation of at-home blood pressure monitoring into hypertension diagnosis and management. This is because isolated blood pressure readings taken at a clinician’s office may be inaccurate: for some, blood pressure tends to rise in medical settings (“white coat hypertension”) while others have normal blood pressure during examination despite hypertensive readings at home (“masked hypertension”).
Time-in-target-range (TTR) describes how often a patient’s blood pressure is in the normal range, and it is emerging as a promising metric of cardiovascular risk. But TTR requires more frequent blood pressure readings that can feasibly be obtained by patients with traditional blood pressure cuffs, which can be inconvenient, burdensome and sometimes uncomfortable for patients.
Fisher, who designed and led the study, collaborated with co-authors from Aktiia SA, a Swiss biotechnology company, to analyse over 2.2 million blood pressure readings from 5189 subjects in Europe and the U.K. who wore a cuffless wrist monitor manufactured by Aktiia. On average, the Aktiia device collected 29 readings per day, a substantial increase from the number of blood pressure readings patients typically take with home devices (guidelines recommend four per day, which is more than most patients measure). Over a 15-day period, the researchers obtained an average of 434 readings from each patient.
By calculating TTR over a 15-day period, the researchers were able to risk stratify participants by percentage of readings in target range and compare these classifications to those generated via traditional measurement patterns, using either 24-hour or week-long daytime monitoring schedules. They found that the traditional methods misclassified 26 and 45 percent of subjects, respectively, compared to the reference TTR. They determined that continual monitoring for seven days is required to obtain 90 percent or greater accuracy in hypertension risk classification, a frequency of measurement that may only be possible with cuffless monitors.
Though the cuffless device studied here has not been approved by the US Food and Drug Administration, it has been validated in multiple studies and is available for over-the-counter purchase in Europe and the UK. Work to evaluate and set standards for such devices in the U.S. is ongoing.
“For the first time, by using a cuffless device, we can collect continual out-of-office blood pressure readings and use these data to calculate a new metric, time-in-target-range, which shows great promise as a predictor of risk,” Fisher said. “The use of cuffless devices could create a shift in the paradigm of blood pressure monitoring and hypertension management.”
Scientists identify a positive molecular feedback loop which could explain stroke-induced memory loss.
Ischaemic and haemorrhagic stroke. Credit: Scientific Animations CC4.0
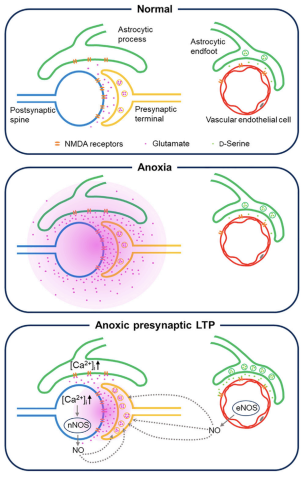
In learning, neurons communicate with each other, and the connections between them getting stronger with repetition. This is known as long-term potentiation or LTP.
Another type of LTP occurs when the brain is deprived of oxygen temporarily – anoxia-induced long-term potentiation or aLTP. aLTP blocks the former process, thereby impairing learning and memory. Therefore, some scientists think that aLTP might be involved in memory problems seen in conditions like stroke.
Researchers at the Okinawa Institute of Science and Technology (OIST) and their collaborators have studied the aLTP process in detail. They found that maintaining aLTP requires the amino acid glutamate, which triggers nitric oxide (NO) production in both neurons and brain blood vessels. This process forms a positive glutamate-NO-glutamate feedback loop. Their study, published in iScience, indicates that the continuous presence of aLTP could potentially hinder the brain’s memory strengthening processes and explain the memory loss observed in certain patients after experiencing a stroke.
The brain’s response to low oxygen
When there is a lack of oxygen in the brain, the neurotransmitter glutamate is released from neurons in large amounts. This increased glutamate causes the production of NO. NO produced in neurons and brain blood vessels boosts glutamate release from neurons during aLTP. This glutamate-NO-glutamate loop continues even after the brain gets enough oxygen.
“We wanted to know how oxygen depletion affects the brain and how these changes occur,” stated Dr Han-Ying Wang, a researcher in the former Cellular and Molecular Synaptic Function Unit at OIST and lead author of the study,. “It’s been known that nitric oxide is involved in releasing glutamate in the brain when there is a shortage of oxygen, but the mechanism was unclear.”
During a stroke, when the brain is deprived of oxygen, amnesia – the loss of recent memories – can be one of the symptoms. Investigating the effects of oxygen deficiency on the brain is important because of the potential medicinal benefits. “If we can work out what’s going wrong in those neurons when they have no oxygen, it may point in the direction of how to treat stroke patients,” Dr Patrick Stoney, a scientist in OIST’s Sensory and Behavioral Neuroscience Unit, explained.
Brain tissues from mice were placed in a saline solution, mimicking the natural environment in the living brain. Normally, this solution is oxygenated to meet the high oxygen demands of brain tissue. However, replacing the oxygen with nitrogen allowed the researchers to deprive the cells of oxygen for precise lengths of time.
The tissues were then examined under a microscope and electrodes were placed on them to record electrical activity of the individual cells. The cells were stimulated in a way that mimics how they would be stimulated in living mice.
Stopping memory and learning activity
The aLTP process is activated when the brain is temporarily deprived of oxygen and glutamate levels increase. If aLTP is maintained for an extended period, this hijacks the normal functioning of the memory strengthening process (LTP), resulting in memory loss. Blocking nitric oxide (NO) synthesis or the molecular pathways that boost glutamate release eventually stops aLTP. Credit: Wang et al., 2024
The scientists found that maintaining aLTP requires NO production in both neurons and in blood vessels in the brain. Collaborating scientists from OIST’s Optical Neuroimaging Unit showed that in addition to neurons and blood vessels, aLTP requires the activity of astrocytes, another type of brain cell. Astrocytes connect and support communication between neurons and blood vessels.
“Long-term maintenance of aLTP requires continuous synthesis of nitric oxide. NO synthesis is self-sustaining, supported by the NO-glutamate loop, but blocking molecular steps for NO-synthesis or those that trigger glutamate release eventually disrupt the loop and stop aLTP,” Prof. Tomoyuki Takahashi, leader of the former Cellular and Molecular Synaptic Function Unit at OIST, explained.
Notably, the cellular processes that support aLTP are shared by those involved in memory strengthening and learning (LTP). When aLTP is present, it hijacks molecular activities required for LTP and removing aLTP can rescue these memory enhancing mechanisms. This suggests that long-lasting aLTP may obstruct memory formation, possibly explaining why some patients have memory loss after a short stroke.
Prof Takahashi emphasised that the formation of a positive feedback loop formed between glutamate and NO when the brain is temporarily deprived of oxygen is an important finding. It explains long-lasting aLTP and may offer a solution for memory loss caused by a lack of oxygen.
Research by West Virginia University has demonstrated that American Heart Association and American Stroke Association guidelines are effective at speeding up hospitals’ response times for stroke treatment and can be mastered even by members of ‘ad hoc‘ medical teams that assemble rapidly on the fly.
When a stroke patient arrives at an emergency room, specialists from across hospital departments – emergency medical services, neurologists, pharmacists, physicians, nurses, radiologists and technicians – rush to coordinate a team response. AHA and ASA guidelines put specific limits on how much time can optimally elapse between the onset of ischaemic stroke, in which blood flow to the brain is blocked, and subsequent events like arrival at the hospital and delivery of an infusion.
But experts have questioned whether the communication of those best practices helps medical teams that assemble temporarily and whose members don’t typically collaborate. In a Journal of Operations Management article, WVU associate professor Bernardo Quiroga and coauthors answer that question using data about more than 8000 patients who received stroke care at a large hospital between 2009 and 2017.
“‘Time is brain’ for stroke victims,” Quiroga explained. “Blocked blood flow to the brain kills almost two million neurons a minute, so your life or ability to walk or talk hinges on how quickly multiple professionals coordinate to restore blood flow. If you’re lucky, you’re treated within the first hour of symptom onset. Better yet, you receive a shot of Tissue Plasminogen Activator, which dissolves clots. TPA works better the earlier it’s given and usually isn’t effective after 4.5 hours.”
In 2010, the AHA and ASA launched Target: Stroke, a program that identifies stroke care best practices and standardises each step in the process. Participating hospitals reduced median treatment times from 79 minutes in 2009 to 51 minutes in 2017, but it wasn’t clear if that improvement was driven by adherence to best practices or by clinicians learning through repetition as they handled more stroke cases.
To figure that out, the researchers investigated whether repeated ‘learning by doing’ decreased the hospital’s stroke care time. Then, they evaluated whether deliberate, ‘induced’ learning and implementation of AHA/ASA best practices decreased the time further.
Learning through repetition worked. The more strokes the hospital treated, the faster it responded. For each doubling of cumulative stroke alerts, ‘door-to-needle time’ – the time to get patients from the hospital door to a TPA infusion – decreased by 10.2%.
Best practices also worked. Specifically, the researchers examined two best practices: the Helsinki Model protocol, which directs that EMS staff keep stroke patients on the stretcher for transport to the CT room rather than transferring them to ER beds; and the Rapid Administration of TPA protocol, which requires the pharmacist to be in the CT room with TPA before completion of the CT scan. Those protocols significantly reduced the hospital’s door-to-needle time beyond improvements from repetition-based learning.
According to Quiroga’s coauthor and former PhD student Brandon Lee, that matters because it demonstrates the efficacy of best practices and shows ad hoc teams learning guidelines and implementing them long-term.
However, Lee emphasised the importance of the presence of the hospital’s stroke advisory committee, which set targets, evaluated stroke teams’ performances and gave feedback.
Without similar “countermeasures to organisational forgetting,” Quiroga acknowledged that best practices aren’t always sustainable, especially on ad hoc teams.
“In the case of the best practice indicated by the Helsinki Model, compliance is difficult because the hospital needs to coordinate with multiple independent EMS systems. Some EMS providers may be reluctant to commit resources to extended time in the CT room, and EMS staff turnover may lead to forgetting,” Quiroga said.
Lee added, “Overall, because ad hoc teams are fluid, information sharing is harder. And when a group of people don’t know each other well, group learning slows. But although ad hoc teams learn more slowly, we determined they still learn.”
The research also assessed whether neurologists’ abilities to meet time goals were affected by their recent experiences treating prior stroke patients.
“As team leaders, neurologists can have an outsized influence on performance,” Quiroga said. “Because other members of the ad hoc team aren’t familiar with each other, they lean on their leader.”
But data showed stroke teams improving response times regardless of how many stroke cases the neurologist had treated individually or what the neurologist’s recent success rate was. Quiroga said that’s good news.
“The implication is that learning and sustaining best practices ensures an even quality of care for patients, regardless of individual neurologists’ experience levels.”
The over-the-counter supplement nicotinamide riboside, a form of vitamin B3, increased the walking endurance of patients with peripheral artery disease, a chronic leg condition for which there are few effective treatments.
In a preliminary, randomised, double-blind clinical trial led by Northwestern University and University of Florida scientists, patients who took nicotinamide riboside daily for six months increased their timed walking distance by more than 17.3m, compared to a placebo group. As expected, walking speed declined in the placebo group, because peripheral artery disease causes progressive declines in walking performance.
“This is a signal that nicotinamide riboside could help these patients,” said Christiaan Leeuwenburgh, PhD, a UF professor of physiology and aging and senior author of the clinical trial report. “We are hoping to conduct a larger follow-up trial to verify our findings.”
Along with other researchers, Leeuwenburgh, whose research specialises in anti-aging treatments, collaborated with Mary M. McDermott, MD, a physician and professor of medicine at Northwestern University and an expert in peripheral artery disease.
The scientists recruited 90 people with an average age of 71 who had peripheral artery disease, or PAD, to test the effects of nicotinamide riboside. The supplement is increasingly popular as an anti-aging treatment (sales exceeded $60 million in 2022 in the US alone) but there has been scant evidence of any benefit in healthy people. Nicotinamide riboside is a precursor for the essential compound NAD, which plays roles in the body related to energy generation, improved blood flow and DNA repair.
Because PAD is associated with problems generating energy within muscle cells, McDermott and Leeuwenburgh thought that nicotinamide riboside, by improving energy generation, could help improve walking in people with the disease.
And indeed that’s what they found. Participants taking the supplement walked an average of 7m more in a six-minute walking test after six months, while those taking a placebo walked 10.3m less. Those who took at least 75% of the pills they were supposed to take performed even better, adding more than 30m to their walking distance, compared to people who took a placebo.
(The researchers also tested if resveratrol, a compound best known for being in red wine, could boost the effects of nicotinamide riboside; they found no additional benefits.)
PAD affects more than 8.5 million Americans over the age of 40. Caused by the buildup of fatty deposits in arteries, and associated with diabetes and smoking, the disease reduces blood flow to the limbs, especially the legs. Walking often becomes painful, and the disease typically causes declines in walking ability over time. Supervised walking exercise is first line therapy for PAD, but most people with the condition do not have access to supervised exercise.
In addition to a larger trial focused on patients suffering from PAD, Leeuwenburgh hopes to test the effects of nicotinamide riboside on walking performance in healthy older adults.
“We need to test it on a healthy older population before we recommend healthy people take it,” he said.
One of the biggest stories in HIV in the last year was that a class of medicines called statins could help reduce cardiovascular disease in people living with the virus. In response, treatment guidelines in the United States were quickly updated, but the picture is more complicated in South Africa. Spotlight’s Elri Voigt explores why the case for widespread use of statins by people living with HIV is less compelling in South Africa than in some other countries.
People living with HIV, provided they are stable on antiretroviral therapy, are affected by the same diseases as those who don’t have HIV, including cardiovascular disease, says Professor Mpiko Ntsekhe, head of Cardiology at Groote Schuur Hospital in Cape Town.
The key difference, he says, is that although both groups of people get the same spectrum of diseases, people living with HIV get those diseases more frequently and earlier. One way to think about this, he explains, is to imagine twins who are identical in every way except one is living with HIV. The twin living with HIV is more likely to get cardiovascular disease than the other twin.
And these differences can be substantial. Current evidence shows that people living with HIV have a twofold increased risk of developing cardiovascular disease compared to people not living with HIV, says Professor Hans Strijdom. He is the Head of the Division of Medical Physiology and Deputy Director of the Centre for Cardio-Metabolic Research in Africa (CARMA) at Stellenbosch University. The cardiovascular risk attributable to HIV, Strijdom adds, is now believed to be equivalent to that posed by traditional risk factors such as smoking. This prompted an editorial in 2018 in one of the top cardiovascular journals, Circulation, advocating for HIV to be recognised as a major cardiovascular risk factor.
He explains that people living with HIV who are stable on treatment are living longer, making them susceptible to the normal risk posed by older age. They also have “modifiable risk factors, in other words lifestyle risk factors”, like a higher smoking and alcohol use incidence, as well as increasing rates of being overweight and obesity. Strijdom says that living with HIV, even when someone is stable on treatment, causes low-grade inflammation, which over time increases a person’s risk for cardiovascular disease. “That all in combination are the current theories [of] why we think that they have a bigger risk of cardiovascular disease,” he says.
Important study findings
Arguably, the biggest news from last year’s International AIDS Society (IAS) Conference in Australia was findings from a study on heart disease in people living with HIV. The trial, called REPRIEVE, showed that a class of cholesterol-busting drugs called statins can prevent a lot of cardiovascular disease events in people living with HIV whose cardiovascular disease (CVD) risk score meets a certain threshold. Spotlight previously reported on these findings, which showed that compared to placebo, daily treatment with 4mg oral pitavastatin – a specific statin – led to a 35% reduction in major adverse cardiovascular events (MACE) in people living with HIV classified to be at risk of cardiovascular disease.
When the findings were presented at the IAS conference, the study’s principal investigator, Dr Steven Grinspoon, said that while the researchers still have to assess more of the data collected to get a clearer picture of things, like the mechanisms driving cardiovascular disease across regions and conduct additional sub-group analyses, the study has already shown that using pitavastatin can save lives.
These sub-group analyses were discussed in greater detail at the Conference on Retroviruses and Opportunistic Infections (CROI) held in Denver in March this year. For the most part, the use of pitavastatin in the manner prescribed by REPRIEVE was considered a huge success, and the United States has since changed its guidelines to include the use of statins in the primary prevention of atherosclerotic cardiovascular disease.
Why it is different in South Africa
However, for low-and-middle-income countries like South Africa, the case for pitavastatin might not be as clear-cut. In fact, a panel discussion at CROI was dedicated to exploring the implications of the REPRIEVE findings for such countries.
Ntsekhe, who was a speaker on the CROI panel, tells Spotlight that data from REPRIEVE’s sub-group analyses reveal there was a striking difference in event rates – which in the case of the study are MACE in those who were getting the placebo – by country income status. He explains that as predicted in high-income countries, the event rates were high, while in low-and-middle income countries – particularly in Sub-Saharan Africa – event rates were very low.
He says one of the reasons for the difference in event rates was that the screening tool used in REPRIEVE worked well to identify those people living with HIV who might benefit from pitavastatin in high-income countries like the United States, but it did not work well in Sub-Saharan Africa.
This means using pitavastatin as part of a primary prevention strategy is a much more effective intervention in high-income countries than in low-and-middle income countries like in Sub-Saharan Africa because the cardiovascular disease profile is so different.
Ntsekhe explains the term cardiovascular disease itself is broad and all-encompassing and there are many forms, including valve disease, heart muscle disease, and vascular disease. The dominant form of cardiovascular disease in the high-income countries (which he refers to as the Global North) is known as atherosclerotic cardiovascular disease, which is characterised by a build-up of fatty deposits and plaque in the arteries.
In Sub-Saharan Africa though, Ntsekhe says “atherosclerotic cardiovascular disease is but one of many forms of cardiovascular disease”, taking the fourth or fifth place in the ranking of types of major heart disease.
Research conducted in high-income countries don’t always take differences in disease burden into account, according to Ntsekhe. This means that interventions researched in high-income countries and shown to be effective in that context won’t necessarily work as well in low-and-middle income countries like South Africa.
Strijdom concurs that while results from REPRIEVE in the global context were a game-changer, the findings are not easily transferable to South Africa’s context because pitavastatin is mainly aimed at reducing “bad cholesterol” and coronary artery disease (also called atherosclerosis).
‘Taking money away’
During the panel discussion at CROI, Ntsekhe asked whether Sub-Saharan Africa could justify taking money away from other health programmes that work in order to invest in pitavastatin.
“I said basically what should be a priority for us is a) finding tools that can better identify those at risk and b) continuing to focus on what our local data suggests are the priority areas,” Ntsekhe says.
“If your entire prevention strategy is aimed at atherosclerotic cardiovascular disease, but it isn’t the dominant cause of disease [in your country], you’re going to be treating a whole host of people to try and tackle this thing that affects very few in a sense,” he says.
“It was not anything about REPRIEVE, it was a wonderful study, the hypothesis was tested, and it was shown to be correct, the intervention we know works,” Ntsekhe says. “It really then comes down to regional areas to think very carefully about how best they’re going to get their biggest bang for their buck,” he says. “We have to carefully consider the local context, local burden, we have set local health priorities, and weigh benefit and cost before we adopt new interventions or recommendations.”
SA’s cardiovascular disease burden
While Strijdom says we don’t have great data, he points to a large systematic review and meta-analysis published in 2018 in Circulation, which estimates that around 15% of the total cardiovascular disease burden in South Africa is attributable to HIV. “It’s probably higher than that. I would say that probably about one in five people with heart disease have heart disease because of HIV in South Africa,” he says, adding “that figure is probably only going to increase”.
Because of this, he says, there is a need for proper and clear primary healthcare guidelines specifically aimed at managing cardiovascular disease in people living with HIV, which we don’t currently have.
Strijdom says what we have at the moment since the rollout of the 2019 National ART Clinical Guidelines is very basic guidelines. This involves screening someone who has just been diagnosed with HIV by taking their blood pressure, and testing urine for glucose and proteins, and an assessment of their general cardiovascular disease risk by taking their medical and family history. These guidelines, according to Strijdom, only make provision for routine screening at baseline, but screening guidelines at follow-up visits are insufficient.
“I am, however, aware of the fact that there is progress especially from the integrated chronic disease management model which is currently being piloted in South Africa – and hopefully with that will come much more definitive and universal guidelines,” he says. “The bottom line is that South Africa, in its public health [sector] especially, really very quickly needs to come up with very clear and more comprehensive guidelines to actively manage cardiovascular disease risk in people with HIV.”
Need for annual screening
Strijdom suggest that to improve screening for cardiovascular disease risk in people living with HIV, there needs to be annual screening of people’s weight, their measure of body fat based on height and weight, waist circumference, blood pressure, cholesterol and triglyceride levels as well as testing urine samples for kidney function. There also needs to be a thorough family and medical history conducted for each patient.
“It’s not really a very expensive or very exhaustive list of stuff that you have to do. Unless of course they have specific symptoms and signs that leads you in a specific direction that you then have to perhaps do an ECG [a test used to evaluate the functioning of the heart] or cardiac imaging but that is usually determined by what you get from their history and clinical examination,” he says.
Ntsekhe says public health strategies to combat the growing burden of non-communicable diseases (NCDs), including cardiovascular disease, in South Africa must be strengthened. These include screening and prevention tools like checking a patient’s blood pressure and blood glucose, advising against smoking and alcohol as well as promoting health lifestyle choices like exercise and weight loss. These interventions should be offered to everyone, regardless of whether they are living with HIV or not, he says.
“The thing about NCDs and cardiovascular disease, for the most part, they are diseases of lifestyle and behaviour. So, when you talk prevention, it’s not always about drug prevention,” he says. “It’s more about intensification of those [interventions] that are already in the public domain, are very effective, and cost very little. Many of the public health and primary healthcare guidelines do advise local ministries, local health authorities on what should be happening.”
In terms of public education, Stritjdom says people need to be aware that there is something like high blood pressure. “If people are aware they will come to the clinic and will say please measure my blood pressure,” he says.
“Our health system is understandably focused on infectious diseases, but if we are not careful, we will then be totally unprepared to tackle the epidemic that will have replaced it. Namely, cancer, heart disease, stroke, obesity, diabetes, and it will totally overwhelm our public healthcare system,” he says.