Overall, there was a 14% reduction in skin cancer risk. When nicotinamide was taken after a first skin cancer, the risk reduction rose to 54%.
3D structure of a melanoma cell derived by ion abrasion scanning electron microscopy. Credit: Sriram Subramaniam/ National Cancer Institute
The dietary supplement nicotinamide has been recommended by dermatologists for people with a history of skin cancer since 2015, when a clinical study with 386 participants showed that those who took the vitamin B3 derivative developed fewer new occurrences.
But data to validate those findings in a larger study group has been lacking because nicotinamide can be purchased over the counter without being entered into patients’ medical records.
In a new study published in JAMA Dermatology, researchers found a way to get that data by analysing records from the Veterans Affairs Corporate Data Warehouse. Nicotinamide is on the VA’s official formulary, so the researchers checked the outcomes of 33 833 patients for their next skin cancer diagnosis following baseline treatment with 500 milligrams of nicotinamide twice daily for longer than 30 days. They looked for occurrences of basal cell carcinoma and cutaneous squamous cell carcinoma.
The researchers compared 12 287 patients who received the treatment with 21 479 who did not. Overall, there was a 14% reduction in skin cancer risk. When nicotinamide was taken after a first skin cancer, the risk reduction rose to 54%, but the benefit declined with treatment initiation following subsequent skin cancers. The risk reduction was much larger for squamous cell carcinoma.
“There are no guidelines for when to start treatment with nicotinamide for skin cancer prevention in the general population. These results would really shift our practice from starting it once patients have developed numerous skin cancers to starting it earlier. We still need to do a better job of identifying who will actually benefit, as roughly only half of patients will develop multiple skin cancers,” said the study’s corresponding author, Lee Wheless, MD, PhD, assistant professor of Dermatology and Medicine at Vanderbilt University Medical Center and a staff physician at VA Tennessee Valley Healthcare System.
The researchers were also able to ascertain the outcomes of 1,334 patients who were immunocompromised due to having received solid organ transplants. Among solid organ transplant recipients, no overall significant risk reduction was observed, although early nicotinamide use was associated with reduced occurrences of cutaneous squamous cell carcinoma.
The findings from the current study suggest that magnesium also increases the gut synthesis of vitamin D, which does not go to the blood and takes effect locally.
Photo by Danilo Alvesd on Unsplash
Researchers from Vanderbilt University Medical Center have demonstrated in a precision-based clinical trial that a magnesium supplement increases gut bacteria in humans that have been shown to synthesise vitamin D and inhibit colorectal cancer carcinogenesis.
However, the effect was observed primarily in females – an outcome that the researchers surmised may be attributable to the role that oestrogen plays in shifting magnesium from circulation into cellular uptake.
Intestinal microbiome data and colonoscopy results were analysed from participants who were randomised by whether they had the TRPM7 genotype, which plays a crucial role in regulating magnesium and calcium uptake.
Previously, the investigators showed in the same randomised trial that magnesium enhances the synthesis of vitamin D and increases the blood levels of vitamin D. The findings from the current study suggest that magnesium also increases the gut synthesis of vitamin D, which does not go to the blood and takes effect locally.
“Our previous study showed magnesium supplementation increased blood levels of vitamin D when vitamin D levels were low,” said Qi Dai, MD, PhD, professor of Medicine. “The current study reveals that magnesium supplementation also increases the gut microbes which have been shown to synthesise vitamin D in the gut without sunlight and locally inhibit colorectal cancer development.”
The participants were divided into two arms, one that received the magnesium supplement and another that received a placebo. Their gut microbiome was analysed from stools, rectal swabs and rectal tissues. Among participants with adequate TRPM7 function, the magnesium supplement increased Carnobacterium maltaromaticum and Faecalibacterium prausnitzii, which were previously found to work synergistically to increase vitamin D and decrease colorectal carcinogenesis. Among those with inadequate TRPM7 function, the magnesium supplement reduced the abundance of F. prausnitzii in rectal mucosa.
Among 236 participants who all had a history of colorectal polyps, 124 underwent colonoscopies after completing the trial with a 3.5-year median follow-up time. A higher abundance of F. prausnitzii in rectal mucosa was associated with an almost threefold increase in developing additional polyps.
Study of nearly 4 million children and adolescents finds that 10% of paediatric blood and bone marrow cancers may have stemmed from radiation exposure.
Credit: Pixabay CC0
A study led by UC San Francisco and UC Davis has concluded that radiation from medical imaging is associated with a higher risk of blood cancers in children.
For the study, which appears in NEJM, the researchers examined data from nearly 4 million children and estimated that 1 in 10 blood cancers – some 3000 cancers in all – may be attributable to radiation exposure from medical imaging. The risk increased proportionally based on the cumulative amount of radiation the children received.
The investigation is the first comprehensive assessment using data from children and adolescents in North America that quantifies the association between radiation exposure from medical imaging and blood and bone marrow cancers, such as leukaemia and lymphoma, which are the most common forms of cancer in children and adolescents.
Medical imaging saves lives by enabling timely diagnosis and effective treatment, but it also exposes patients to ionizing radiation, a known carcinogen, particularly through computed tomography (CT).
The authors caution that doctors and parents should avoid excessive radiation doses and minimize exposure when clinically feasible.
“Children are particularly vulnerable to radiation-induced cancer due to their heightened radiosensitivity and longer life expectancy,” said Rebecca Smith-Bindman, MD, a radiologist and professor of Epidemiology and Biostatistics, as well as Obstetrics, Gynecology and Reproductive Sciences at UCSF and the first author of the paper.
“While medical imaging can be lifesaving, our findings underscore the critical need to carefully evaluate and minimise radiation exposure during paediatric imaging to safeguard children’s long-term health,” said Smith-Bindman, who is also a member of the Philip R. Lee Institute for Health Policy Studies. “This involves ensuring that imaging is performed only when it provides essential information for the child’s care and, in cases such as CT scans, using the lowest possible radiation doses.”
Documenting risks in children
The study uses a retrospective cohort design, looking back at the complete imaging histories of 3.7 million children who were born between 1996 and 2016. The children were treated at six health care systems in the U.S. and Ontario, Canada. Investigators found a significant relationship between cumulative radiation dose and the risk of a hematologic malignancy, which includes tumours affecting the blood, bone marrow, lymph, and lymphatic system.
The risk of developing cancer varied significantly by imaging modality. CT, which is used to detect many abnormalities such as tumours, heart disease, and injuries of the spinal cord and brain, entails significant radiation exposure. But radiographs, which are used to diagnose both broken bones and pneumonia, expose children to much lower doses.
Among all the forms of medical imaging, the study found that chest radiography was the most common imaging exam that doctors performed. The most common form of CT was of the head and brain.
For children who underwent a head CT, the researchers attributed about a quarter of the children’s subsequent hematologic malignancies to radiation exposure. For those who had radiographs, by contrast, they estimated that only a small fraction of the children’s subsequent cancers were associated with radiation exposure.
Getting one or two head CTs was associated with a 1.8-fold increased risk of a cancer diagnosis, and this rose to 3.5 times for children who received more scans and were therefore exposed to more radiation.
Altogether, 2961 haematologic malignancies were diagnosed during the study period. Lymphoid malignancies accounted for 79.3%, while myeloid malignancies and acute leukaemia together accounted for 15.5%. About 58% of cancers occurred in males, and about half were diagnosed in children under 5.
The authors said that up to 10% of haematologic malignancies in children and adolescents could be prevented by reducing unnecessary imaging and optimising radiation doses. In many cases, the authors said, substituting non-ionising imaging modalities like ultrasound or MRI may be feasible without compromising diagnostic accuracy.
Benefits vs risks
The authors emphasised that while medical imaging remains an invaluable tool in paediatric care, their findings highlight the need to carefully balance its diagnostic benefits with potential long-term risks.
“This study provides robust, directly observed evidence of a clear dose–response relationship between radiation from medical imaging and hematologic malignancy risk in children and adolescents,” said Diana Miglioretti, PhD, UC Davis Health professor and chief of the Division of Biostatistics.
“Our findings align with international research highlighting that children are especially radiosensitive,” Miglioretti added. “It’s crucial for clinicians to weigh the immediate benefits of imaging against potential long-term health risks and to optimise imaging protocols to minimize radiation exposure.”
For women who’ve overcome cervical cancer, new research from MUSC Hollings Cancer Center points to another health risk that may not be on their radar: anal cancer.
While cervical cancer is one of the most preventable cancers, with a survival rate of over 90% when found early, clinical guidelines have not addressed what comes next for these patients, who may be at high risk for a related type of cancer.
“We’ve known for a long time that both cervical and anal cancers are caused by HPV, the human papillomavirus,” Deshmukh said. “But what hasn’t been well-understood is how that shared risk might connect the two diseases over a woman’s lifetime.”
Currently, anal cancer screening is recommended for certain high-risk groups, such as people living with HIV, organ transplant recipients and women with a history of vulvar cancer. But there are no clear screening guidelines for women with cervical cancer.
One problem has been a lack of long-term data on their risk and how that risk changes with age and over time. This study helps to fill that gap using high-quality, population-based data.
The researchers turned to the National Cancer Institute’s SEER (Surveillance, Epidemiology and End Results) program – a comprehensive set of registries that tracks cancer diagnoses across the US. They analysed data from more than 85 000 women diagnosed with cervical cancer, tracking them over two decades to see how many went on to develop anal cancer and when those diagnoses occurred.
What they found was striking. Compared with the general population, women with a history of cervical cancer had nearly twice the risk of developing anal cancer.
Anal cancer rates increased with age and over time, with the most diagnoses found in women ages 65 to 74 who were more than 15 years out from their original diagnosis. For women in this age group, the rate of anal cancer diagnoses surpassed a widely accepted threshold for recommending routine screening.
“Our study shows that the risk doesn’t go away – it actually increases with age and over time,” Damgacioglu said.
Why the delay? HPV-related cancers often take years, sometimes decades, to develop. In some cases, the virus may linger undetected or have spread from another part of the body.
“It’s a slow process,” Deshmukh said, “and that’s part of why it’s been so hard to detect. By the time symptoms show up, the cancer is often advanced.”
While anal cancer screening is not as routine as screening for other cancers, reliable methods do exist, including anal cytology (a kind of Pap screen) and anoscopy. Unfortunately, access to specialised screening remains limited. In South Carolina, for example, there is currently only one provider trained to perform high-resolution anoscopy.
That is why it is so important to identify and prioritise the highest-risk groups.
“These results tell us that women who had cervical cancer years ago should be considered for routine anal cancer screening,” Damgacioglu said. “Right now, that’s not happening.”
Deshmukh and his team are now working on a project to determine when and how often screening should happen.
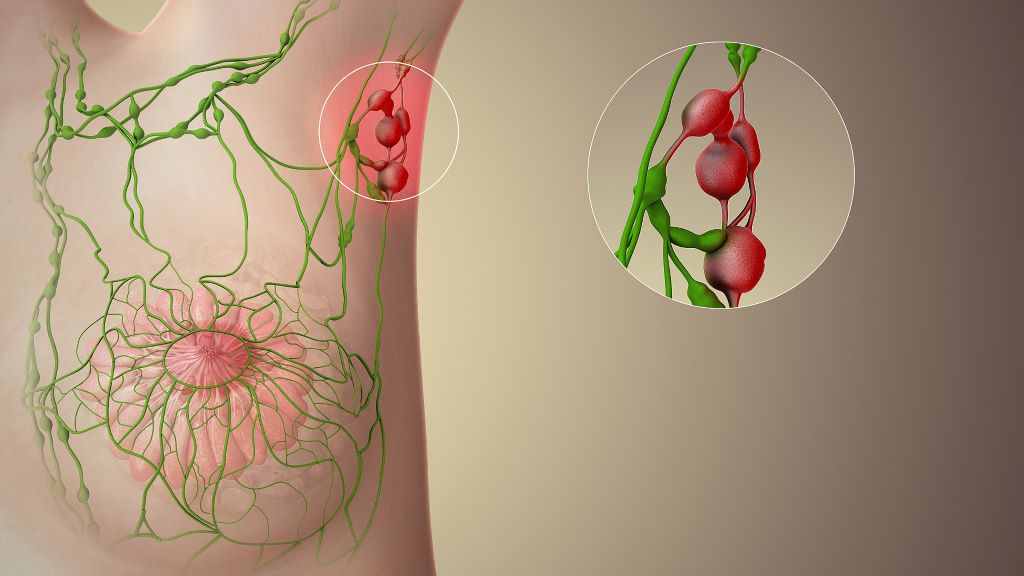
New research has shown why preserving lymph nodes, often removed near tumours to prevent cancer spread, could improve patient outcomes and make immunotherapies more effective.
A team of researchers, led by the Peter Doherty Institute for Infection and Immunity (Doherty Institute), explored the cellular and molecular interactions revealing how lymph nodes play a crucial role in the fight against chronic infection and cancer.
The research, published across two papers in Nature Immunology (references and links below), showed that lymph nodes provide the right environment for stem-like T cells, an important type of immune cell, to survive, multiply and produce killer cells that can fight cancer or viruses. In other immune organs, such as the spleen, these cells don’t develop or proliferate as effectively, making lymph nodes essential for a strong immune response and successful immunotherapy.
The University of Melbourne’s Professor Axel Kallies, Laboratory Head at the Doherty Institute and senior author of both papers, said the findings have important implications for cancer therapy.
“Lymph nodes aren’t just passive waiting rooms for immune cells, they actively train and educate T cells, and send them off to do their job,” said Professor Kallies.
“Our research suggests that removing lymph nodes during cancer surgery, a common practice to prevent tumour spread, may inadvertently reduce the effectiveness of treatments, such as checkpoint blockade and CAR T cell therapies. Preserving lymph nodes could strengthen immune responses and increase the effectiveness of immunotherapy.”
This work may also help explain why some patients respond better to immunotherapy than others. The state and function of lymph nodes influence how well the immune system can produce cancer-fighting T cells, directly impacting the success of immunotherapy.
The University of Melbourne’s Dr Carlson Tsui, Postdoctoral Researcher at the Doherty Institute and first author of one of the papers, said the findings could help to develop new strategies to make immunotherapy more effective.
“Our research identifies molecular signals that are involved in the regulation of stem-like cells and in their capacity to produce effective killer cells. These findings could guide the development and refinement of immune-based treatments for cancer and chronic infection,” said Dr Tsui.
“Furthermore, our research shows that rather than only focusing on the tumour itself, therapies should also be designed to preserve and enhance lymph node function. By targeting these critical immune hubs, we could boost the body’s natural ability to fight cancer, increase the effectiveness of existing immunotherapies and help more patients respond to treatment.”
Together, the two peer-reviewed papers provide a deeper understanding of how lymph nodes shape immune responses. While they are based on work with animal models, they will guide future treatment strategies for chronic infection and cancer treatment.
Professor Shahneen Sandhu, Research Lead for the Melanoma Medical Oncology Service at the Peter MacCallum Cancer Centre, commented on the clinical implications of this work.
“While this research was done in the laboratory with pre-clinical models, we’re excited to study these findings in clinical samples from patients receiving immune checkpoint inhibitors, as part of an ongoing Melanoma Research Victoria collaboration with Professor Kallies,” Professor Sandhu said.
“Combining clinical and preclinical studies will help us translate these discoveries from bench to bedside and back, ultimately improving outcomes for cancer patients.”
Tsui C, Heyden L, et al. Lymph nodes fuel KLF2-dependent effector CD8+ T cell differentiation during chronic infection and checkpoint blockade. Nature Immunology (2025). DOI: https://doi.org/10.1038/s41590-025-02276-7
Wijesinghe SKM, Rausch L, et al. Lymph-node-derived stem-like but not tumor-tissue-resident CD8+ T cells fuel anticancer immunity. Nature Immunology (2025). DOI: https://doi.org/10.1038/s41590-025-02219-2
A Swedish-led research team at Karolinska Institutet and Karolinska University Hospital has shown in a new randomised clinical trial that a low dose of the well-known medicine aspirin halves the risk of recurrence after surgery in patients with colon and rectal cancer with a certain type of genetic alteration in the tumour.
Every year, nearly two million people worldwide are diagnosed with colorectal cancer, and 20–40% develop metastases.
Previous observational studies have suggested that aspirin may reduce the risk of certain cancers and possibly also the risk of recurrence after surgery in patients with colorectal cancer harbouring mutations in genes within the PIK3 signaling pathway. These genes regulate key cellular processes such as growth and division. When mutated, these processes can become dysregulated, leading to uncontrolled cell proliferation and cancer development.
Randomised clinical trials were lacking
Prior findings have been inconsistent and no randomised clinical trials had previously confirmed the association. To address this gap, the ALASCCA trial was initiated, with the results now been published in The New England Journal of Medicine.
The current study included more than 3500 patients with colon and rectal cancer from 33 hospitals in Sweden, Norway, Denmark, and Finland. Patients whose tumours showed a specific genetic mutation in the PIK3 signalling pathway – a mutation found in approximately 40% of patients – were randomised to receive either 160mg of aspirin daily or a placebo for three years after surgery.
For patients with the genetic mutation in PIK3, the risk of recurrence was reduced by 55% in those who received aspirin compared with the placebo group.
“Aspirin is being tested here in a completely new context as a precision medicine treatment. This is a clear example of how we can use genetic information to personalise treatment and at the same time save both resources and suffering,” says first author Anna Martling, professor at the Department of Molecular Medicine and Surgery, Karolinska Institutet, and senior consultant surgeon at Karolinska University Hospital.
Less favourable environment for cancer
So how does aspirin reduce the risk of recurrence of colon and rectal cancer? The researchers believe that the effect is likely due to aspirin acting through several parallel mechanisms – it reduces inflammation, inhibits platelet function and tumour growth. This combination makes the environment less favourable for cancer.
“Although we do not yet fully understand all the molecular links, the findings strongly support the biological rationale and suggest that the treatment may be particularly effective in genetically defined subgroups of patients,” says Anna Martling.
The researchers believe that the results could have global significance and influence treatment guidelines for colon and rectal cancer worldwide. Anna Martling sees the fact that the drug is well established as a major advantage.
“Aspirin is a drug that is readily available globally and extremely inexpensive compared to many modern cancer drugs, which is very positive,” says Anna Martling.
A groundbreaking cancer drug could enhance how patients respond to chemotherapy even in treatment-resistant tumours.
The drug works by disarming a key defence mechanism that tumours use to protect themselves from treatment. In preclinical models, it has already shown promise in making chemotherapy-resistant cancers more responsive to therapy.
Chemotherapy is one of the most widely used cancer treatments, but it doesn’t always work as effectively as hoped. One major reason is that macrophages act as a barrier around tumours. These immune cells surround the blood vessels inside tumours and act like gatekeepers, blocking helpful immune cells from entering and doing their job in supporting the responses to chemotherapy.
The King’s College London scientists, who have launched a spinout company Aethox Therapeutics, found that these macrophages make a protein called heme oxygenase-1 (HO-1), which helps shield the tumour from the immune system and block the effects of chemotherapy. The new drug, KCL-HO-1i, targets this protein.
Professor James Arnold, Head of Tumour Immunology Group, King’s College London, said: “We discovered that these macrophages in cancer play a key role in blocking chemotherapy. By targeting the enzyme they produce using KCL-HO-1i, we were able to help beneficial immune cells and chemotherapy drugs become significantly more effective. In laboratory models, even chemotherapy-resistant tumours became responsive to treatment, which is a really exciting step forward.”
Unlike many cancer treatments that require hospital visits, KCL-HO1i is designed to be taken at home as a tablet between chemotherapy sessions. This makes it easier for patients to incorporate into their treatment plans without adding extra hospital burdens.
In early tests using mouse models of breast cancer, supported by funding by Cancer Research UK and Medical Research Council (MRC), the drug made tumours more responsive to a range of commonly used chemotherapies. These promising results suggest it could be used across a wide variety of cancer types and chemotherapy treatments.
The researchers hope that with funding, clinical trials on breast and other cancers could begin within two years.
Professor James Spicer, Professor of Experimental Cancer Medicine, King’s College London, said: “Chemotherapy remains a key part of treatment for many patients with cancer, but too often it is not as effective or long-lasting as we might like. This research has identified a key reason for these limitations, and discovered a drug that we are keen to test in the clinic alongside established chemotherapy drugs”.
This breakthrough is the result of a multidisciplinary collaboration between researchers including Professors James Arnold, James Spicer, and Miraz Rahman and their research teams at King’s College London.
If human trials are successful, KCL-HO-1i could become a valuable companion drug to existing cancer therapies – helping more patients to benefit from the treatments that are already available and reduce the need for more aggressive cancer therapies in the future.
Professor Miraz Rahman, Professor of Medicinal Chemistry, King’s College London
Study reveals that 1 in 10 will initiate opioid prescriptions long term.
Photo by Anna Shvets on Pexels
New research indicates that many patients who undergo surgery with the intent to cure early-stage cancer continue or start opioid prescriptions in the year following surgery. The findings are published by Wiley online in CANCER, a peer-reviewed journal of the American Cancer Society.
Pain management is essential during cancer care, but prescription opioid practices associated with cancer treatment may lead to unsafe long-term opioid use and adverse outcomes such as opioid use disorder and opioid overdose. To assess the situation, investigators examined rates of new persistent opioid use in the year following surgery for stage 0 to 3 cancers among 9213 U.S. Veterans who were opioid-naïve (not on prescribed opioids the year prior to their cancer diagnosis).
The team found that potentially dangerous co-prescription of opioid and benzodiazepine (a central nervous system depressant that treats anxiety, insomnia, and seizures and should not be combined with opioids) medications occurred in 366 (4.0%) Veterans during follow-up. Persistent opioid use occurred in 981 (10.6%). A higher intensity of exposure to opioid prescriptions during treatment was associated with these outcomes. People with a prior history of chronic pain, greater comorbidities, lower socioeconomic status, and who received adjuvant chemotherapy were at especially high risk of opioid use in the year after surgery.
“Minimising opioid exposure associated with cancer treatment while providing effective pain control will decrease long-term health risks among cancer survivors,” said lead author Marilyn M. Schapira, MD, MPH, of the University of Pennsylvania. “This is important as many patients are living longer after a cancer diagnosis and treatment.”
Gut Microbiome. Credit Darryl Leja National Human Genome Research Institute National Institutes Of Health
About a dozen studies in the past five years have made claims linking nearly every type of human cancer with the presence of microbiomes, “communities” of bacteria, viruses and fungi that live in or on peoples’ bodies. Now, scientists at Johns Hopkins Medicine say a study that sequenced human cancers found far less microbial DNA sequences than earlier studies reported in the same cancer tissue samples.
“It’s the nature of science to validate, confirm and reproduce findings,” says Steven Salzberg, PhD, Professor of Biomedical Engineering, Computer Science, and Biostatistics at The Johns Hopkins University. “Over time, we see a more complete picture of new research, and in this case, we did not find any associations between microbiomes and many types of cancer.”
Salzberg says details of the new study, published Sept. 3 in Science Translational Medicine, surveyed the whole genome sequences generated from 5734 tissue samples collected from 25 cancer types and stored in a large National Cancer Institute-funded database, The Cancer Genome Atlas (TCGA). About half of the samples are from normal tissues and blood, the other half from solid tumours and blood-based cancers.
The TCGA’s whole genome sequencing data contains millions of chopped up pieces of DNA molecules, known as reads, from each tissue sample. The original goal of the TCGA studies was to identify mutations in the DNA sequence of genes that might be associated with various cancer types. Sometimes, though, the original tumors might have microbes in them, and the reads could be used to identify those microbes.
Because reads often contain contaminants from bits of DNA left behind in sequencing machinery or picked up from the air or surfaces, samples can acquire DNA from those sources, as well as from the original tumour tissues. Salzberg says extraordinary efforts were made to identify such contaminants, preventing their study from displaying false results.
To rule out contaminants, Salzberg and his team relied on extensive experience with genomic sequencing and careful analysis of control samples to identify reads belonging to sequences known or highly likely to have contaminated samples.
For the current study, a continuation of one that the Johns Hopkins team published in 2023, Salzberg and first author Yuchen “Peter” Ge, a graduate student in biomedical engineering at Johns Hopkins, removed human DNA sequences from the TCGA data sets by mapping each read against two human reference genomes – one from the Telomere-to-Telomere (T2T) project and another from the Genome Reference Consortium.
After removing human DNA, the research team was left with, on average, 2.4 million reads per sample, or about 0.35% of the total 6.5 billion tumour sample reads. Of these, the research team found 323 million human DNA reads that weren’t eliminated in the first pass and 986 million reads they classified as contaminants.
They next compared the remaining sequencing reads against a database containing 50 651 genomes representing 30,355 species of bacteria, viruses, fungi and archaea (single-celled organisms that aren’t bacteria or viruses).
After removing human DNA sequences and contaminants, the average proportion of microbial DNA reads in solid tumour samples was 0.57% and 0.73% in blood cancers.
The Johns Hopkins researchers then compared their new results to a study published five years ago in the journal Nature [since retracted, because of concerns about contaminants in the microbial data], and found the previous study identified 56 times as many microbial reads as the new study for half of the total microbial reads. And 5% of the time, the previous study found 9,000 times the number of microbial reads as the current Johns Hopkins study. Salzberg says the microbial reads in the retracted study were highly likely to be contaminants.
“This disparity in the number of microbial reads didn’t occur in just a few samples,” says Salzberg. “Over the whole study, the previous researchers found far more microbial reads than we did.”
In another comparison of a study published in Cell in 2022 and the current Johns Hopkins work, the 2022 study reported fungal DNA amounts that were hundreds of times more than what was found in the current Johns Hopkins study, largely due to contaminants.
Among the DNA samples in the current Johns Hopkins study, in which they did find microbiome DNA, the researchers found microbes that have long been linked with human cancer, such as HPV (linked with cervical and some head and neck cancers), Helicobacter pylori (linked to stomach cancer), and Fusobacterium nucleatum and Bacteroides fragilis (linked with GI cancers).
The current Johns Hopkins study and the previous ones published in Cell and Nature reported microbiomes of Saccharomyces cerevisiae, commonly known as baker’s yeast. “It’s one of the most common contaminants in sequencing labs,” says Salzberg. They also found a virus that infects plant fungi, Rosellinia necatrix partitivirus 8, which has no known link to human disease.
Salzberg said the need to carefully document claims about the links between cancer and microbiomes is “especially important” as efforts ramp up to diagnose cancers early using microbiome information.
The Johns Hopkins researchers have made their sequencing analysis data available online to other scientists in the supplementary materials in Science Translational Medicine and online.
In the latest chapter of a long-running legal battle over the Gauteng Department of Health’s obligation to provide people in the province with radiation oncology services, the department has suffered another loss in the courts. Spotlight assesses the legal situation and asks what it means for people still waiting for the life-saving treatment.
With another court loss suffered this August, the Gauteng Department of Health has once again been ordered to urgently provide treatment for cancer patients who have been left in the lurch.
This ruling, handed down on August 5 by Judge Evette Dippenaar, follows urgent legal action brought by the Cancer Alliance. It was in response to the Gauteng health department’s appeal against a ruling handed down on March 27 by acting Judge Stephen van Nieuwenhuizen. That order compelled the department to clear its years-long backlogs in getting cancer treatment to patients.
In its March ruling, the South Gauteng High Court in Johannesburg found the department’s failure to deliver this critical treatment to be unconstitutional and unlawful. The decision follows the department’s failure to spend a R784 million allocation granted by the provincial Treasury in 2023 to reduce the treatment backlog by outsourcing services to the private sector over a three-year period. Due to severe delays, the department was forced to return the first R250 million tranche.
Van Nieuwenhuizen strongly criticised the department, stating: “The provincial health respondents have done nothing meaningful since the money was allocated in March 2023 to actually provide radiation oncology treatment to the cancer patients. Meanwhile, the health and general well-being of the patients has significantly deteriorated. There is clear, ongoing, and irreparable harm being suffered by those still waiting for treatment.”
He also condemned the department for its lack of accountability and poor management of public resources, finding that it had failed to uphold ethical standards, act transparently, or respond to patients’ needs fairly and effectively.
The court instructed the department to:
Take immediate action, including diversion to private facilities, to provide radiation oncology services to all patients on the backlog list,
Update the backlog list within 45 days,
Submit a detailed progress report on efforts to deliver treatment, and
Present a long-term plan for ongoing cancer treatment services within three months.
But Gauteng health MEC Nomantu Nkomo-Ralehoko and the health department challenged the judgment in May, just as their 45 days to act ran out. They chose instead to take the entire matter on appeal to the Supreme Court of Appeal (SCA).
In response, the Cancer Alliance, represented by SECTION27 (*see disclosure), went back to court for an interim order to make the March 27 ruling immediately enforceable, and not suspended until a ruling is made by the SCA. It is in response to this application that Judge Dippenaar ruled on August 5 that the March ruling is indeed immediately enforceable.
Two courts have now sent a clear message to the Gauteng health department, says attorney Khanyisa Mapipa, who heads health rights at SECTION27. She adds: “The Gauteng Department of Health’s action should be in the interest of the person who is seeking treatment. It should not be to deny, deny, deny and then to fight in the courts and not take any accountability.”
The waiting list
The estimated number of people on a waiting list for cancer treatment in 2022 was around 3 000 people. New data on this has not been made publicly available.
There are some signs of progress, although details are hard to pin down. In a statement released on August 24, which reiterates a July 20 statement, the Gauteng health department said it had introduced a strategic partnership with private service providers. “As the beginning of August 2025, 563 patients were receiving radiation oncology care through private partnerships, while 1 076 patients had completed treatment by end of July 2025,” it stated.
Both statements also noted that work was underway to complete new radiotherapy centres at Chris Hani Baragwanath and Dr George Mukhari Academic Hospitals.
But Mapipa says they still don’t have full details that comply with the court order. “What we’re asking for essentially is what the department should be doing anyway and that is for them to go through their patient files to establish who is still on the backlog list; who has passed away, who has received treatment, when patients were last assessed and what treatment they qualify for; and if it was a public facility or were they diverted to a private facility,” she says.
“As the judge pointed out in March, the department has to do this as a constitutional obligation, whether they fight this to the Constitutional Court or not, their obligation is to provide treatment for people who meet the criteria. Those on the backlog list meets the criteria,” she says.
Part of the March order also compelled the department to file progress reports with the court within three months on the measures taken to provide treatment and its long-term plans to resolve the ongoing cancer treatment crisis in Gauteng. Spotlight’s understanding is that these progress reports have not been submitted.
This is an important measure, Mapipa says, given the department’s poor track record. “The court rulings in both judgments found that because they have failed to be transparent throughout this process, the department is compelled to provide these reports to the courts,” she adds.
It is as yet unclear how the Gauteng health department plans to proceed. The department, in its three-paragraph statement following the August judgment, stated that it would review “the contents and implications” to determine and communicate its next steps. Their deadline to appeal the August 5 ruling was 26 August 2025. The department did not respond to questions from Spotlight.
Calls for accountability
Jack Bloom, Democratic Alliance shadow health MEC in Gauteng, says that without a proper audit and update of the backlog list of patients needing care, the “cancer treatment scandal has probably cost more lives than the 144 mental patients who died in the Life Esidimeni tragedy when they were sent to illegal NGOs”.
Bloom is calling for heads to roll, with Nkomo-Ralehoko and head of department Arnold Lesiba Malotana in his crosshairs.
“The DA condemns the department’s legal stalling tactics that harms patients who urgently require lifesaving treatment…Premier [Panyaza] Lesufi should not allow this cancer disaster to continue,” he says.
Salomé Meyer, spokesperson for Cancer Alliance, says that the legal proceedings are a distraction of the realities on the hospital floor. Charlotte Maxeke Johannesburg Academic Hospital for instance, she says, remains in “crisis”. She maintains there is a scarcity of sufficient and operational radiation oncology machinery, as well as extreme shortages in radiation oncology staff to operate the machines.
Meyer says the situation at Charlotte Maxeke Hospital dates back to 2017 when CEO Gladys Bagoshi was made aware of mounting challenges from a shortage of equipment and staffing.
“In 2021, Bagoshi turned down an equipment allocation, which Charlotte Maxeke Hospital desperately needed, so this allocation went to George Mukhari Hospital and Chris Hani Baragwanath Hospital instead. But the cobalt bunkers required to house the machines at these hospitals had not been built and are only expected to be completed in 2026 – so the machines remain in storage. In 2022, an order was finally placed for additional linacs [used for high energy beam radiation treatments] for the existing cobalt bunkers at Charlotte Maxeke Hospital, but that tender is still not finalised,” says Meyer.
She adds: “This is a failure of planning, governance, and accountability and we have to ask who is being held accountable when the same CEO has remained in place all these years.”
Neither Bagoshi nor the health department responded to questions on these assertions.
Disclosure: SECTION27 was involved in the court proceedings described in this article. Spotlight is published by SECTION27, but is editorially independent – an independence that the editors guard jealously. The Spotlight editors gave special attention to maintaining this editorial firewall in the production of this story.