A study published in Nature Microbiology has uncovered startling connections between micronutrient deficiencies and the composition of gut microbiomes in early life that could help explain why resistance to antibiotics has been rising across the globe.
A University of British Colombia team investigated how deficiencies in crucial micronutrients such as vitamin A, B12, folate, iron, and zinc affected the community of bacteria, viruses, fungi and other microbes that live in the digestive system.
They discovered that these deficiencies led to significant shifts in the gut microbiome of mice – most notably an alarming expansion of bacteria and fungi known to be opportunistic pathogens.
Importantly, mice with micronutrient deficiencies also exhibited a higher enrichment of genes that have been linked to antibiotic resistance.
“Micronutrient deficiency has been an overlooked factor in the conversation about global antibiotic resistance,” said Dr. Paula Littlejohn, a postdoctoral research fellow with UBC’s department of medical genetics and department of pediatrics, and the BC Children’s Hospital Research Institute. “This is a significant discovery, as it suggests that nutrient deficiencies can make the gut environment more conducive to the development of antibiotic resistance, which is a major global health concern.”
Bacteria naturally possess these genes as a defence mechanism. Certain circumstances, such as antibiotic pressure or nutrient stress, cause an increase in these mechanisms. This poses a threat that could render many potent antibiotics ineffective and lead to a future where common infections could become deadly.
Antibiotic resistance is often attributed to overuse and misuse of antibiotics, but the work of Dr. Littlejohn and her UBC colleagues suggests that the ‘hidden hunger’ of micronutrient deficiencies is another important factor.
“Globally, around 340 million children under five suffer from multiple micronutrient deficiencies, which not only affect their growth but also significantly alter their gut microbiomes,” said Dr. Littlejohn. “Our findings are particularly concerning as these children are often prescribed antibiotics for malnutrition-related illnesses. Ironically, their gut microbiome may be primed for antibiotic resistance due to the underlying micronutrient deficiencies.”
The study offers critical insights into the far-reaching consequences of micronutrient deficiencies in early life. It underscores the need for comprehensive strategies to address undernutrition and its ripple effects on health. Addressing micronutrient deficiencies is about more than overcoming malnutrition, it may also be a critical step in fighting the global scourge of antibiotic resistance.
Newly announced results of a pivotal phase 3 trial have demonstrated the effectiveness of a new one-dose treatment for gonorrhoea. The medicine, called zoliflodacin, is the first new drug developed to treat gonorrhoea in over 30 years. More than half of the 930 patients included in the trial were from South Africa, including women, adolescents, and people living with HIV.
Zoliflodacin, which was shown to be non-inferior to (as good as) the currently used treatment in treating uncomplicated gonorrhoea, provides an important new tool to combat rising rates of drug resistant gonorrhoea. It was found to be generally well tolerated and there were no serious adverse events or deaths recorded in the trial. So far, only top line results have been shared in a media release and the findings have not yet been published in a medical journal. (You can see some technical details of the study design on ClinicalTrials.gov)
The World Health Organization raised the alarm about increasing rates of drug resistant gonorrhoea in 2017, noting the emergence of cases of untreatable gonorrhoea resistant to all available antibiotics. According to the United States Centers for Disease Control and Prevention “medication to treat gonorrhoea has been around for decades, but the bacteria has grown resistant to nearly every drug ever used to treat it”. They say: “only one class of antibiotics known as cephalosporins remains to treat the infection”.
As a drug from a new class of antibiotics, zoliflodacin, offers a new potential treatment for patients whose gonorrhoea was previously untreatable, as well as a new tool for safeguarding the ongoing effectiveness of currently available antibiotics.
How zoliflodacin may change gonorrhoea treatment
Professor Sinead Delany-Moretlwe, Director of Research for Wits RHI and the National Principal Investigator for the trial in South Africa, told Spotlight that while zoliflodacin may be used to treat drug resistant gonorrhoea, it also provides an attractive new treatment option for first-line treatment of gonorrhoea in some countries (in other words, gonorrhoea that is not resistant to other treatments).
Zoliflodacin, which is taken as a single oral dose, is simpler to administer than the current standard of care, which involves a combination of injectable ceftriaxone and oral azithromycin. Removing the need for an injection could simplify the administration of gonorrhoea treatment and improve its uptake.
Using zoliflodacin as first-line gonorrhoea treatment can also help safeguard the ongoing effectiveness of cephalosporins (including ceftriaxone), according to Delany-Moretlwe, which she adds are needed not just for treatment of gonorrhoea, but also other infections.
According to Delany-Moretlwe, because zoliflodacin is the first of a new class of antibiotics with novel mechanisms of action and without existing cross resistance, the hope is that widespread use of zoliflodacin as first-line gonorrhoea treatment will slow the emergence of resistance compared with the medicines currently being used.
The Global Antibiotic Research and Development Partnership (GARDP), a non-profit that sponsored the trial, points out that: “Antimicrobial resistance [AMR] has been around for millions of years, long before the first man-made antibiotics. So, drug-resistant bacteria are inevitable and will eventually affect all antibiotics”. They state: “to beat AMR we need a steady supply of new antibiotics to be developed that are effective against drug-resistant bacteria, particularly for priority pathogens that have the greatest public health impact.”
Gonorrhoea in South Africa
South Africa has incredibly high rates of gonorrhoea, with an estimated 2 million new cases annually. While data on rates of drug resistance in the country is limited, the data that is available indicates that ceftriaxone resistance in the country is low, but azithromycin resistance is concerningly high in some parts of the country.
As there is no routine screening for gonorrhoea in South Africa, linkage to treatment remains a challenge. Currently, diagnosis is largely done through symptomatic reporting by patients. But this approach misses many cases as some patients do not self-report symptoms and some cases of gonorrhoea are asymptomatic.
In 2022, the Southern African HIV Clinicians Society released new guidelines for the management of sexually transmitted infections which called for provider-initiated symptomatic screening and provider-initiated diagnostic screening in high-risk populations.
The country’s new National Strategic Plan on HIV, TB and STIs has set a target to increase the number of pregnant women tested for gonorrhoea from 10% in 2023 to 80% by 2028 and has committed to implementing diagnostic testing in other priority populations, including adolescent girls and young women.
How will new gonorrhoea treatments be commercialised?
Zoliflodacin was developed by GARDP in collaboration with the company Innoviva Specialty Therapeutics. According to GARDP, it holds the rights to register and commercialise zoliflodacin in more than three-quarters of the world’s countries, including all low-income countries, most middle-income countries, and several high-income countries. While, Entasis Therapeutics Limited, an affiliate of Innoviva Specialty Therapeutics, “retains the commercial rights for zoliflodacin in the major markets in North America, Europe, Asia-Pacific, and Latin America”.
South Africa is one of the countries in which GARDP holds the rights to register and commercialise zoliflodacin. It is anticipated that this will be done through selection and licensing of companies to manufacture and supply zoliflodacin in South Africa and other countries where GARDP holds commercialisation rights.
GARDP recently launched a request for proposals from partners that are interested in commercialising zoliflodacin. GARDP has also signed a memorandum of understanding with two generic producers to explore opportunities to commercialise the medicine in low-and-middle-income countries.
While the price that will be offered by commercial partners for the product remains to be seen, it is anticipated that products will be made available at affordable prices in line with GARDP’s goal to ensure that “all GARDP products are available, affordable, and appropriately used across populations that need them”.
“This is the first study to address a World Health Organization priority pathogen that has been sponsored and led by a non-profit organization,” says GARDP.
“This demonstrates that GARDP’s model can play a crucial role in helping to fix the public health failure at the heart of the global AMR crisis,” says Professor Glenda Gray, GARDP board member and President of the South African Medical Research Council.
SA involvement
According to GARDP, South Africa had the highest number of participants in the global trial, across six sites in four provinces: Wits RHI in Hillbrow, Johannesburg; the Desmond Tutu HIV Foundation in Masiphumelele, Cape Town; Setshaba Research Centre in Soshanguve, Gauteng; the SAMRC’s clinical research sites in Botha’s Hill and Tongaat in KwaZulu-Natal; and Ndlovu Research Centre in Groblersdal, Limpopo.
“We have also been able to leverage our HIV experience to build capacity for trials of novel STI technologies, a previously neglected area. Undertaking this vital work on a new treatment for gonorrhoea has also given us the opportunity to focus sharply on the local situation in South Africa,” says Delany-Moretlwe.
High rates of antibiotic resistance now meant that drugs to treat common infections in children and babies are no longer effective in large parts of the world, according to findings published in Lancet South East Asia.
The University of Sydney led study found many antibiotics recommended by the World Health Organization (WHO) had less than 50% effectiveness in treating childhood infections such as pneumonia, sepsis (bloodstream infections) and meningitis. The findings show global guidelines on antibiotic use are outdated and need updates.
The most seriously affected regions are in South-East Asia and the Pacific, including neighbouring Indonesia and the Philippines, where thousands of unnecessary deaths in children resulting from antibiotic resistance occur each year.
The WHO has declared antimicrobial resistance (AMR) is one of the top 10 global public health threats facing humanity. In newborns, an estimated three million cases of sepsis occur globally each year, with up to 570 000 deaths: many of these are due to lack of effective antibiotics to treat resistant bacteria.
The findings add to mounting evidence that common bacteria responsible for sepsis and meningitis in children are often resistant to prescribed antibiotics.
The research reveals the urgent need for global antibiotic guidelines to be updated, to reflect the rapidly evolving rates of AMR. The most recent guideline from The World Health Organization was published in 2013.
The study found one antibiotic in particular, ceftriaxone, was likely to be effective in treating only one in three cases of sepsis or meningitis in newborn babies. Ceftriaxone is also widely used in Australia to treat many infections in children, such as pneumonia and urinary tract infections.
Another antibiotic, gentamicin, was found likely to be effective in treating fewer than half of all sepsis and meningitis cases in children.
Gentamicin is commonly prescribed alongside aminopenicillins, which the study showed also has low effectiveness in combating bloodstream infections in babies and children.
Lead author Dr Phoebe Williams from the University’s School of Public Health and Sydney Infectious Diseases Institute is an infectious disease specialist whose research focuses on reducing AMR in high-burden healthcare settings in Southeast Asia.
She also works as a clinician in Australia. Dr Williams says there are increasing cases of multidrug-resistant bacterial infections in children around the world.
AMR is more problematic for children than adults, as new antibiotics are less likely to be trialled on, and made available to, children.
Dr Williams says the study should be a wake-up call for the whole world, including Australia.
“We are not immune to this problem – the burden of anti-microbial resistance is on our doorstep,” she said.
“Antibiotic resistance is rising more rapidly than we realise. We urgently need new solutions to stop invasive multidrug-resistant infections and the needless deaths of thousands of children each year.”
The study analysed 6,648 bacterial isolates from 11 countries across 86 publications to review antibiotic susceptibility for common bacteria causing childhood infections.
Dr Wiliams said the best way to tackle antibiotic resistance in childhood infections is to make funding to investigate new antibiotic treatments for children and newborns a priority.
“Antibiotic clinical focus on adults and too often children and newborns are left out. That means we have very limited options and data for new treatments.”
Dr Williams is currently looking into an old antibiotic, fosfomycin, as a temporary lifeline to treat multidrug-resistant urinary tract infections in children in Australia.
She is also working with the WHO’s Paediatric Drug Optimisation Committee to ensure children have access to antibiotics to treat multidrug-resistant infections as soon as possible, to reduce deaths due to AMR among children.
“This study reveals important problems regarding the availability of effective antibiotics to treat serious infections in children,” says senior author Paul Turner, director of the Cambodia Oxford Medical Research Unit at Angkor Hospital for Children, Siem Reap and professor of paediatric microbiology at the University of Oxford, UK.
“It also highlights the ongoing need for high quality laboratory data to monitor the AMR situation, which will facilitate timely changes to be made to treatment guidelines.”
A study published in PLOS Biology reveals that different strains of Escherichia coli can outcompete one another to take over the gut. The researchers found that a particular strain, known as MDR ST131, can readily colonise new hosts, even if those hosts are already have commensal E.coli in their healthy gut.
The international team, led by experts at the University of Birmingham, used a mouse model to help understand why strains of E.coli that live in a healthy gut are rapidly overtaken of when challenged with a multi-drug resistant strain.
Lead author Professor Alan McNally, from the Institute of Microbiology and Infection at the University of Birmingham, commented: “Antibiotic resistance has been hailed as one of the biggest health problems of our time by the World Health Organisation. There are further problems looming unless we get a better understanding of what is happening so that further drug resistance can be halted in its tracks.
“Scientists have long questioned what makes certain types of E. coli successful multi-drug resistant pathogens. It seems that extra-intestinal pathogenic E. coli, which cause urinary tract and bloodstream infections, are particularly successful when it comes to developing resistance and are therefore especially tricky to treat. Our study provides evidence that certain types of E. coli are more prone to develop antibiotic resistance than others.”
According to previous research, multi-drug resistance alone is not sufficient to drive strains to complete dominance. This most recent study demonstrates that regardless of multi-drug resistant status, certain types of E.coli will outcompete others to live in the human gut.
The work was completed in parts. First, both multi-drug resistant and non-resistant gut-dwelling E. coli were found to easily colonise a mammalian gut. In a second part of the study, the multi-drug resistant strain was found to efficiently displace an already established gut-dwelling E. coli from the mouse intestinal tract. The study provided further details to demonstrate that multidrug resistant lineages of extraintestinal E. coli have particular genetic differences that appear to give them a competitive advantage.
Successful strains of E.coli need to be able to spread between individuals or from the environment into individual hosts. The new study demonstrates that a particular strain, known as MDR ST131, can readily colonise new hosts, even if those hosts are already have E. coli in their healthy gut.
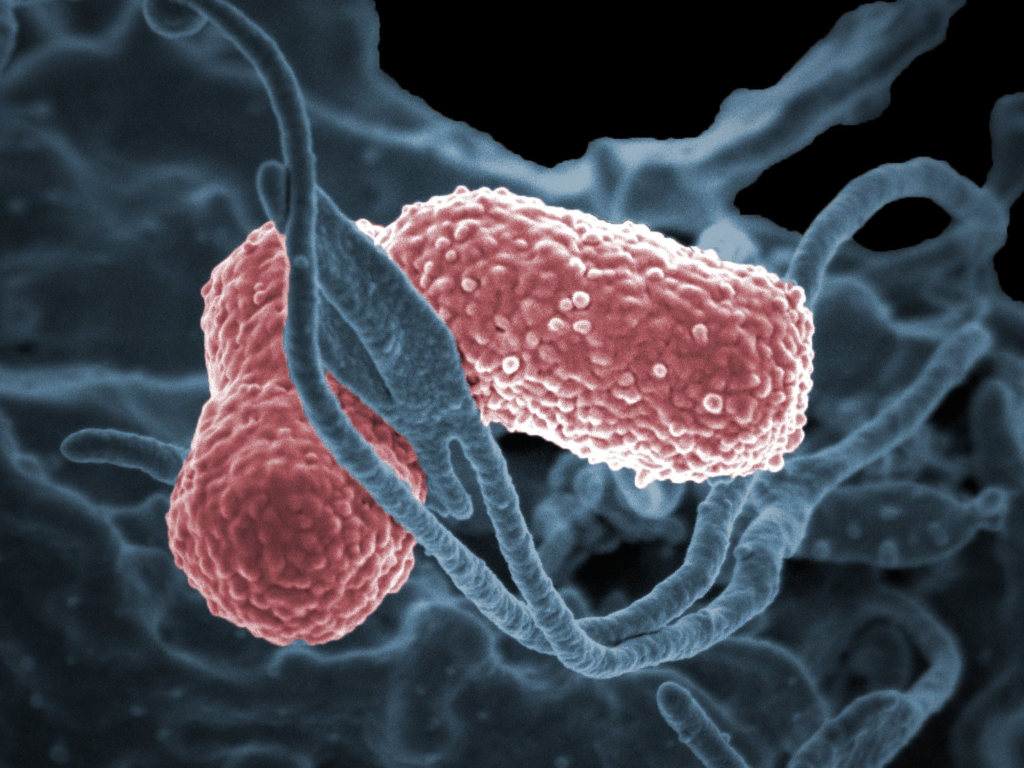
A human neutrophil interacting with Klebsiella pneumoniae (pink), a multidrug–resistant bacterium that causes severe hospital infections.
Credit: National Institute of Allergy and Infectious Diseases, National Institutes of Health
New “hypervirulent” strains of the bacterium Klebsiella pneumoniae have emerged in healthy people in community settings, prompting researchers to investigate how the human immune system defends against infection by it. After exposing the strains to components of the human immune system in vitro, they found that some strains were more likely to survive in blood and serum than others, and that neutrophils are more likely to ingest and kill some strains than others. The study, published in mBio, was led by researchers at NIH’s National Institute of Allergy and Infectious Diseases (NIAID).
“This important study is among the first to investigate interaction of these emergent Klebsiella pneumoniae strains with components of human host defence,” Acting NIAID Director Hugh Auchincloss, MD, said. “The work reflects the strength of NIAID’s Intramural Research Program. Having stable research teams with established collaborations allows investigators to draw on prior work and quickly inform peers about new, highly relevant public health topics.”
K. pneumoniae was identified over a hundred years ago as a cause of serious, often fatal, human infections, mostly in already ill or immunocompromised patients and especially if hospitalised. Over decades, some strains developed resistance to multiple antibiotics. Often called classical Klebsiella pneumoniae (cKp), this bacterium ranks as the third most common pathogen isolated from hospital bloodstream infections. Certain other Klebsiella pneumoniae strains cause severe infections in healthy people in community settings (outside of hospitals) even though they are not multidrug-resistant. They are known as hypervirulent Klebsiella pneumoniae, or hvKp. More recently, strains with both multidrug resistance and hypervirulence characteristics, so-called MDR hvKp, have emerged in both settings.
NIAID scientists have studied this general phenomenon before. In the early 2000s they observed and investigated virulent strains of methicillin-resistant Staphylococcus aureus (MRSA) bacteria that had emerged in US community settings and caused widespread infections in otherwise healthy people.
Now, the same NIAID research group at Rocky Mountain Laboratories in Hamilton, Montana, is investigating similar questions about the new Klebsiella strains, such as whether the microbes can evade human immune system defenses. Their findings were unexpected: the hvKp strains were more likely to survive in blood and serum than MDR hvKp strains. And neutrophils had ingested less than 5% of the hvKp strains, but more than 67% of the MDR hvKp strains – most of which were killed.
The researchers also developed an antibody serum specifically designed to help neutrophils ingest and kill two selected hvKp and two selected MDR hvKp strains. The antiserum worked, though not uniformly in the hvKp strains. These findings suggest that a vaccine approach for prevention/treatment of infections is feasible.
Based on the findings, the researchers suggest that the potential severity of infection caused by MDR hvKp likely falls in between the classical and hypervirulent forms. The work also suggests that the widely used classification of K. pneumoniae into cKp or hvKp should be reconsidered.
The researchers also are exploring why MDR hvKp are more susceptible to human immune defences than hvKp: Is this due to a change in surface structure caused by genetic mutation? Or perhaps because combining components of hypervirulence and antibiotic resistance reduces the bacterium’s ability to replicate and survive in a competitive environment.
As a next step, the research team will use mouse models to determine the factors involved in MDR hvKp susceptibility to immune defences. Ultimately, this knowledge could inform treatment strategies to prevent or decrease disease severity.
A US study found that, despite prescriptions for the antibiotic ciprofloxacin dropping by two-thirds between 2015 and 2021, the rates of ciprofloxacin-resistant E. coli bacteria circulating in the community did not decline.
In fact, a study of women over age 50 who had not taken any antibiotics for at least a year discovered that the incidence of gut-colonising ciprofloxacin-resistant E. coli actually increased. About 1 in 5 women in the study were affected.
Scientists at the University of Washington School of Medicine, Kaiser Permanente Washington Health Research Institute and Seattle Children’s Hospital conducted the study. Their findings appear in Communications Medicine.
Their results are consistent with theoretical models indicating that, once a drug-resistant form of E.coli emerges, it will continue to spread by taking up long-term residence in individuals’ gut microbiomes. E. coli is among an alarming number of disease-causing bacteria that have become resistant to several types of antibiotics. Resistance means that the antibiotics can’t kill the bacteria.
Pathogenic E. coli from the gut occasionally enters the urinary tract opening and causes infections. The female pelvic anatomy makes women more vulnerable to these mobile bacteria. Postmenopausal women are especially susceptible to severe, drug-resistant infection. Some drug-resistant E. coli infections are associated with considerable risk of hospitalization and death from sepsis.
Urinary tract infections from antibiotic-resistant E. coli can be frustrating to treat, even with third-generation cephalosporins, the newer types of antibiotics that are being prescribed more frequently for some populations of patients. Resistance to cephalosporins among ciprofloxacin-resistant E. coli also rose between 2015 and 2021.
Ciprofloxacin and similar drugs in its class were once the most prescribed antibiotic for urinary tract infections. In 2015, recommendations from the Centers for Disease Control and Prevention, Food and Drug Administration and Infectious Disease Society of America discouraged broad use of this class of drugs for uncomplicated urinary tract infections, partly due to rising resistance.
“However, it appears to be questionable whether a reduction in antibiotic use can be effective in reducing the rates of resistance in E. coli infections,” the research paper’s authors noted.
“Evidence from studies such as this one may be changing lots of paradigms on how to fight the rise in antibiotic resistance,” said physician scientist Dr. Evgeni V. Sokurenko, professor of microbiology at the University of Washington School of Medicine, who headed this latest research.
In the study, the scientists examined participants’ positive samples to determine which antibiotic-resistant strains of E. coli were present.
They found that the rate of a particularly virulent strain, ST1193, rose during the study period. Together with E. coli strain ST131-H30, these strains are the major causes of a global pandemic of multi-drug-resistant urinary tract infections among all women.
If ST1193 makes its home in more people’s guts, the situation could lead to more urinary tract infections with this more virulent strain, regardless of the curbing of fluoroquinolones prescriptions.
Another strain with a troubling increase in the participant samples was ST69, known to more frequently cause urinary tract infections in children.
tize discovering better ways to control drug-resistant E. coli’s ability to colonize the gut before it causes these infections, the authors wrote. They mentioned potential strategies of deploying probiotic bacteria and anti-bacterial viruses (bacteriophages).
The researchers added that these approaches might be offered to high-risk patients or deployed against the most clinically relevant strains. More investigation is needed on the epidemiology and ecology of antibiotic-resistant gut E. coli, they said, to help determine how these bacteria skillfully colonize human guts and how to target them most effectively to reduce antibiotic-resistant infections.
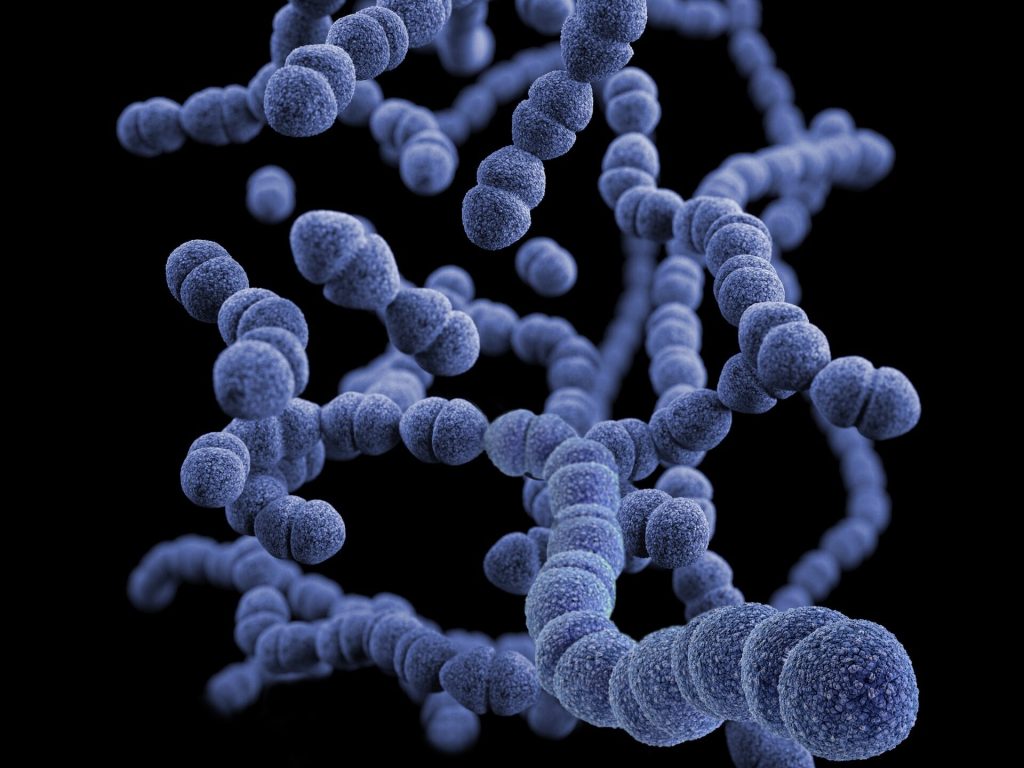
This illustration depicted a three-dimensional (3D), computer-generated image, of a group of Gram-positive, Streptococcus pneumoniae bacteria. The artistic recreation was based upon scanning electron microscopic (SEM) imagery.
Doctors typically treat paediatric ear infections with antibiotics, but children don’t always complete the full course, accelerating resistance to these medications. Today, researchers report developing a single-use nanoscale system that’s unlikely to generate resistance. Using a compound similar to bleach in test animals, they show it can kill off Streptococcus pneumoniae, a common cause of ear infections, and it could someday be easily applied as a gel.
The researchers will present their results at the meeting of the American Chemical Society (ACS).
“We initially conceived of this idea by looking at the household cleaner bleach. Even though it has been used since the 19th century, bacteria do not appear to have developed any widespread resistance to this cleaner,” says Rong Yang, PhD, the project’s principal investigator.
But Yang quickly warns that people should not treat infections with bleach. The solution sold at stores is highly concentrated and caustic, but when used in a properly controlled manner at extremely low concentrations, the active ingredient in bleach is considered compatible with living tissue.
After realising that the active ingredient in the household cleaner could circumvent antibiotic resistance, the Cornell University researchers, set out to tackle a nearly universal childhood scourge: acute ear infections. These infections affect more than 95% of children in the US, and treatment typically requires taking antibiotics for five to 10 days. However, these regimens can cause problematic side effects, leading some families to discontinue the medication prematurely, particularly if symptoms resolve. But using these medications improperly can speed up the development of antibiotic resistance, which makes infections more difficult, if not impossible, to treat. This issue ranks among the biggest threats to global health, according to the World Health Organization.
Bacteria have more success fighting against some substances than others. Hypochloric acid from bleach belongs to a family of compounds, known as hypohalous acids, to which bacteria have yet to develop any significant resistance; most likely because of the numerous ways these highly reactive acids damage microbial cells, Yang says.
Because these substances break down quickly, Yang and her colleagues sought to generate one of them on an as-needed basis behind the eardrum in the middle ear, where ear infections occur. They found inspiration in an enzyme from giant kelp, which converts hydrogen peroxide (H2O2) to hypobromous acid (HOBr), a chemical relative of bleach.
Streptococcus pneumoniae, a frequent cause of ear infections, produces H2O2 to fight off other microbes. To mimic the kelp enzyme, which contains the metal vanadium, Yang and her colleagues designed nanowires made of vanadium pentoxide (V2O5). These produce HOBr only in the presence of the H2O2-producing bacteria, and their rod-like shape helps to keep them in place by reducing their ability to diffuse into body fluids.
In tests on chinchillas, which contract ear infections from the same pathogens as human children, they succeeded in eliminating most of the S. pneumoniae. Yang and colleagues found that after treatment with the nanowires, the animals’ once-inflamed eardrums returned to normal. Meanwhile, tests in healthy animals found evidence that the treatment did not interfere with hearing.
For these experiments, the researchers injected the nanowires directly into the middle ear. In more recent work in chinchillas, they developed a less invasive, more practical method for delivering the wires. By decorating the nanowires with peptides known to transport small particles across the eardrum, Yang and her team found they could deliver the treatment topically as a gel deposited into the ear canal. Once the gel was applied, the nanowires within it went through the intact tissue. They are also exploring other approaches for passing the nanowires through the eardrum.
Because other ear-infection-causing bacteria do not produce H2O2, the researchers are currently examining whether this system is effective in the presence of microbes other than S. pneumoniae, and how they might adapt it to fight the other bugs.
The researchers have not yet done studies to determine how long the system stays in place, although their evidence suggests the nanowires drain out of the middle ear after the infection clears. However, Yang suspects they could adapt the nanowires’ properties to stay in place for long periods afterward. This latter approach could make it possible to prevent recurrent infections that plague many children.
“If the bacteria return, the system could restart, so children wouldn’t need antibiotics repeatedly and breed more resistance along the way,” Yang says.
A new analysis shows that infectious bacteria exposed to the promising antibiotic albicidin rapidly develop up to a 1000-fold increase in resistance via a gene amplification mechanism. Mareike Saathoff of Freie Universität Berlin, Germany, and colleagues presented these findings in the open access journal PLOS Biology.
Bacterial resistance to antibiotics is a growing problem associated with millions of deaths around the world every year. Understanding how bacteria evolve resistance is key to developing more effective antibiotics and strategies for using them.
In recent years, albicidin has emerged as a promising antibiotic capable of killing a wide range of bacterial species by disrupting their DNA replication. Researchers are working to develop new albicidin-based medications; yet, despite its promise, some bacteria are able to develop resistance to albicidin.
To further investigate albicidin resistance mechanisms, Saathoff and colleagues conducted a suite of experiments employing a broad set of tools, including RNA sequencing, protein analysis, X-ray crystallography, and molecular modeling. They found that two bacteria often associated with human infection, Salmonella typhimurium and Escherichia coli, develop resistance to albicidin when exposed to increasingly higher concentrations of the compound. Their analysis narrowed down the source of this resistance to an increase in the number of copies of a gene known as STM3175 (YgiV) in the bacterial cells, which is amplified in each new generation of cells as they multiply. STM3175 encodes a protein that interacts with albicidin in such a way that protects the bacteria from it.
Further experiments showed that the same albicidin-resistance mechanism is widespread among both pathogenic and harmless bacteria, including the microbes Vibrio vulnificus, which can infect wounds, and Pseudomonas aeruginosa, which can cause pneumonia and other infections. These findings could help inform the ongoing development of albicidin-based antibiotic strategies.
The authors add, “Our study reveals a gene duplication and amplification-based mechanism of a transcriptional regulator in Gram-negative bacteria, that mediates resistance to the peptide antibiotic albicidin.”
In children with suspected sinusitis, a nasal swab to test for three types of bacteria can tell whether antibiotics are likely to be effective or not, according to a new JAMAstudy by researchers at the University of Pittsburgh and UPMC. They also found that nasal discharge colour was no help in differentiating a viral or bacterial infection.
“Sinusitis is one of the most common diseases we see in children, but it’s difficult to diagnose because it’s based on the duration of symptoms: If the child has a runny nose or congestion for more than 10 days, we suspect sinusitis,” said said lead author Nader Shaikh, MD. “For an ear infection, we can look inside the ear; for pneumonia, we listen to the lungs. But for sinusitis, we have nothing to go on from a physical exam. That was very unsatisfying to me.”
With the goal of developing a better tool to diagnose bacterial sinusitis, Shaikh and his team enrolled about 500 children with sinusitis symptoms from six centres across the US and randomly assigned them to receive either a course of antibiotics or placebo. The researchers also took nasal swabs from each child and tested for the three main types of bacteria involved in sinusitis.
Children who tested positive for the bacteria had better resolution of symptoms with antibiotic treatment compared to those who did not have bacteria. These findings suggest that testing for bacteria could be a simple and effective way to detect children who are likely to benefit from antibiotics and avoid prescribing antibiotics to those who wouldn’t.
“If antibiotics aren’t necessary, then why use them?” said Shaikh. “These medications can have side effects, such as diarrhoea, and alter the microbiome, which we still don’t understand the long-term implications of. Overuse of antibiotics can also encourage antibiotic resistance, which is an important public health threat.”
According to Shaikh, a common belief among parents and doctors is that yellow or green snot signals a bacterial infection. Although several small studies have suggested that nasal discharge colour is not meaningful, Shaikh and his team formally tested this idea by asking parents to identify the hue of their child’s snot on a colour card.
“If kids with green or yellow discharge benefitted more from antibiotics than those with clear-coloured discharge, we would know that colour is relevant for bacterial infection,” explained Shaikh. “But we found no difference, which means that colour should not be used to guide medical decisions.”
The researchers are now looking at how to best roll out nasal testing in the clinic. A major challenge is that bacterial culture-based tests used in the study are not easy for most family doctors to order and can take several days to get results. A more practical approach could be commercially available molecular testing, which could return results overnight, said Shaikh.
Another possibility could be development of rapid antigen tests that work like COVID-19 at-home testing kits. The researchers also plan to delve deeper into the data from this study to see whether there could be another type of biomarker in nasal discharge indicating the presence of bacteria that would be easier to test for.
An innovative treatment paves the way for reducing antimicrobial resistance in the treatment of a deadly infection in chickens, according to a new study in Veterinary Microbiology. The ground-breaking study investigated the effectiveness of a novel metal-derived complex in treating Avian Pathogenic Escherichia coli (APEC), a serious respiratory infection of chickens which has become increasingly more resistant to antibiotics. A growing body of evidence indicates that the APEC could potentially spread to humans.
University of Surrey’s Professor Roberto La Ragione said: “Antimicrobial resistance is one of the biggest threats to human and animal health. Not being able to use antibiotics to treat an infection not only prolongs an illness and associated welfare issues, but also increases the likelihood of it spreading.
“Coronavirus demonstrated how easily a pandemic can happen, and the threat of another is looking more likely as antibiotics to treat simple bacterial infections are no longer working.”
To test the effectiveness of the metal complex, manganese carbonyl, researchers worked with the Greater Wax Moth larvae and APEC. Split into two groups, the first received manganese carbonyl, whilst the second, the controls, received either a phosphate-buffered saline (PBS) or dimethyl sulfoxide (DMSO). After four days, the survival rate for the larvae which received manganese carbonyl was between 56–75%, whereas in the control group, the survival rate was between 25–45% (PBS) and 19-45 per cent (DMSO), demonstrating the protective effect of the complex.
The test was repeated in chickens infected with APEC, who again received either manganese carbonyl or PBS. Bacterial shedding identified in the faeces of the chickens was significantly lower 24 hours post-treatment in those who received manganese carbonyl compared to the PBS control group, indicating bacterial killing induced by the compound. This is supported by caecal samples taken three days post-treatment which again found significantly fewer bacteria in those that received manganese carbonyl. Examination of tissue samples from the livers of the birds indicated no toxic effects from the metal compound, which was observed in the larvae.
Dr Jonathan Betts, a Research Fellow at the University of Surrey School of Veterinary Medicine, said:
“The development of alternatives to antibiotics is vital to safeguard our future health. Metal complexes such as manganese carbonyl could do this, as we have shown not only are they effective, but they are much cheaper to produce than traditional antibiotics.
“Discovering the effectiveness of manganese carbonyl in treating APEC is a monumental step forward in tackling antimicrobial resistance as it shows we don’t necessarily need more antibiotics; we just need to think more innovatively in developing treatments.”
The international research team also included the University of Surrey, the Animal and Plant Health Agency, the University of Connecticut, the University of Sheffield and Institut für Anorganische Chemie, Julius-Maximilians-Universität Würzburg.
This study was made possible by a BBSRC grant to Professor La Ragione and Professor Poole.