Calorie labels on restaurant menus are negatively impacting people with eating disorders, according to a new study published in the BMJ Public Health.
The review, which is the first of its kind, is led by researchers at King’s College London. It found that individuals who have been diagnosed with an eating disorder changed their behaviours if presented with a menu featuring calorie labels.
This included avoiding restaurants, triggering eating disorder thoughts and paying more attention to calorie labels as identified by eye tracking research.
The research found that some people with eating disorders reported that seeing menu labels reinforced their eating disorder beliefs.
The study evaluated existing research to help build a picture of how nutritional labels on menus impact people with a lived experience of eating disorders or disordered eating. It reviewed 16 studies from the UK, US, Canada and Saudi Arabia which included 8,074 participants in total.
The study highlights that people with eating disorders can feel that eating disorders are perceived as less important in the light of obesity prevention policies.
However, physical health cannot be measured by a single indicator such as weight. Some argue that calorie labels can be seen as a blunt instrument to fix a complicated problem and that people with eating disorders could be losing out.
Food labelling came into force in England in 2022. Restaurants, take-aways and cafes with 250 employees or more must display the calories of the food and drink they sell on menus, online menus and take-away platforms. The measure was an attempt to curb rising obesity levels. The United States and Canada have also made calorie displays mandatory, however, few policies targeting obesity have considered the potential impact on eating disorders.
The eating disorder charity Beat estimates that at least 1.25 million people in the UK have an eating disorder. The number of people admitted to hospital with an eating disorder has risen approximately 7% each year since 2005 – 2006.
Senior author Dr Tom Jewell, Lecturer in Mental Health Nursing at King’s College London, said: “Our study highlights that people with lived experience of eating disorders are frustrated at being left out of the conversation around calorie labels.”
Striking a balance between the positive and harmful impacts of calorie labels on menus is vital in any public health policies.Dr Tom Jewell, Senior author and Lecturer in Mental Health Nursing at King’s College London
“Policymakers should consider the impact on both obesity and eating disorders when making decisions about nutrition labelling. A recent review found that calorie labelling has a modest effect on people’s behaviour but this needs to be counterbalanced with the potential harm it does for people with eating disorders.”
Co-author Dr Nora Trompeter, Research Fellow University College London, said: “Our study provides an important addition to the evidence base around calorie labels.”
Typically, there is a lot of focus on whether policies are effective in reducing obesity, but it is also critical to investigate whether these policies inadvertently harm people with eating disorders.
“Our review also shows that more research is needed to fully understand the impact of calorie labels on individuals with eating disorders. For example, none of the studies included young people.”
Meeting the minimum requirement for vitamin B12, needed to make DNA, red blood cells and nerve tissue, may not actually be enough – particularly if for older adults. It may even put them at risk for cognitive impairment, according to a study published in Annals of Neurology.
The research found that older, healthy volunteers, with lower concentrations of B12, but still in the normal range, showed signs of neurological and cognitive deficiency. These levels were associated with more damage to the brain’s white matter – the nerve fibres that enable communication between areas of the brain – and test scores associated with slower cognitive and visual processing speeds, compared to those with higher B12.
The UC San Francisco researchers, led by senior author Ari J. Green, MD, of the Departments of Neurology and Ophthalmology and the Weill Institute for Neurosciences, said that the results raise questions about current B12 requirements and suggest the recommendations need updating.
“Previous studies that defined healthy amounts of B12 may have missed subtle functional manifestations of high or low levels that can affect people without causing overt symptoms,” said Green, noting that clear deficiencies of the vitamin are commonly associated with a type of anaemia. “Revisiting the definition of B12 deficiency to incorporate functional biomarkers could lead to earlier intervention and prevention of cognitive decline.”
Lower B12 correlates with slower processing speeds, brain lesions
In the study, researchers enrolled 231 healthy participants without dementia or mild cognitive impairment, whose average age was 71. They were recruited through the Brain Aging Network for Cognitive Health (BrANCH) study at UCSF.
Their blood B12 amounts averaged 414.8pmol/L, well above the U.S. minimum of 148pmol/L. Adjusted for factors like age, sex, education and cardiovascular risks, researchers looked at the biologically active component of B12, which provides a more accurate measure of the amount of the vitamin that the body can utilize. In cognitive testing, participants with lower active B12 were found to have slower processing speed, relating to subtle cognitive decline. Its impact was amplified by older age. They also showed significant delays responding to visual stimuli, indicating slower visual processing speeds and general slower brain conductivity.
MRIs revealed a higher volume of lesions in the participants’ white matter, which may be associated with cognitive decline, dementia or stroke.
While the study volunteers were older adults, who may have a specific vulnerability to lower levels of B12, co-first author Alexandra Beaudry-Richard, MSc, said that these lower levels could “impact cognition to a greater extent than what we previously thought, and may affect a much larger proportion of the population than we realize.” Beaudry-Richard is currently completing her doctorate in research and medicine at the UCSF Department of Neurology and the Department of Microbiology and Immunology at the University of Ottawa.
“In addition to redefining B12 deficiency, clinicians should consider supplementation in older patients with neurological symptoms even if their levels are within normal limits,” she said. “Ultimately, we need to invest in more research about the underlying biology of B12 insufficiency, since it may be a preventable cause of cognitive decline.”
Despite many societal changes, including technology such as dating apps and young adults waiting longer to get married, two surveys of college students conducted 10 years apart showed that their expectations about romantic relationships have remained remarkably consistent, according to a new study led from the University of Illinois Urbana-Champaign
According to some popular culture writers and online posts by discouraged singles lamenting their inability to find romantic partners, dating is “broken,” fractured by the social isolation created by technology, pandemic lockdowns and potential partners’ unrealistic expectations.
Yet two studies of college students conducted a decade apart found that their ideas about romantic relationships have remained much the same, although the trajectories of their relationships have changed somewhat, according to study leader Brian Ogolsky, a professor of human development and family studies at the University of Illinois Urbana-Champaign.
“College students in our study did not share this perception of dating as a broken system, despite many massive cultural shifts during this decade,” Ogolsky said. “Their perspectives on relationships today aren’t that different from what they were 10 years ago — or even 10 years before that. Instead, young adults are taking more diverse and multifaceted pathways through romantic partnering and considering a broader range of outcomes.”
Ogolsky surveyed college students ages 18-29 in 2012 and in early 2022, asking them to describe their thoughts and experiences about the typical initiation and progression of romantic relationships.
Published in the journal Personal Relationships, the study was co-written by Jennifer L. Hardesty, a professor in the same department; psychology professor Kiersten Dobson of McMaster University; and U. of I. graduate students Matthew Rivas-Koehl and Ghada Kawas.
More than 250 students were surveyed, about half of whom said they had romantic partners at the time.
Based upon participants’ responses, the researchers identified four stages of romantic relationships. The first stage, which they called “flirtationship,” may occur online or in person and involves the first sparks of attraction, fanning those embers through flirtation and exploring common interests.
If the attraction and level of interest are mutual, the individuals test the waters for “relationship potential” — the second stage in relationship development — by spending increased time together, with a heavy focus on communicative activities that probe whether the relationship should move forward. Study participants repeatedly mentioned friendship as an important basis for romantic partnerships, and they most often mentioned dating in reference to this stage, the data indicated.
“Young adults clearly distinguish dating from being in a relationship,” Ogolsky said. “In our study, we used the term ‘relationship development’ to describe the activities we were investigating, but it became clear that participants did not view early behaviors as part of being in a relationship per se. Instead, they viewed flirting and even dating as part of a broader pattern of interpersonal interaction that may or may not eventually lead to the formation of a relationship.”
If romance does blossom and the union progresses to the third stage — being in a relationship — defining their union becomes important to the partners, such as labeling their status as “official” and identifying themselves as significant others, the researchers said.
Although those in the first study were less likely to mention sexual activity, students in both studies were more likely to talk about it in the context of defining the relationship. And the researchers found that the majority of the students in both studies implied an expectation of exclusivity and monogamy from committed relationships.
Although many studies on young adults’ relationships have focused on hookup culture — casual sex without commitment — only nine of those in the more recent study mentioned it. And the researchers hypothesized that college students may use the term when referring to sexual activity in any context, even that which occurs within a predefined relationship.
Ogolsky said it was during the third stage that the greatest differences emerged between the two groups of students’ beliefs. Those in the 2012 study were more likely to believe that the typical relationship path was for partners to become engaged after becoming official. However, those in the 2022 study rarely mentioned engagement, saying instead that commitment proceeds in more diverse pathways such as moving in together.
“Another difference we found pertained to integrating romantic partners into one’s social circle,” Ogolsky said. “For the students in 2012, this process centered around introducing a new partner to family members. However, those in the more recent study viewed it as integrating the partner into one’s broader social networks of friends as well as family members.”
In the fourth relationship stage — called “commitment or bust” — Ogolsky said that participants described arriving at an eventual crossroads, where the partners either decide to marry or enter into another type of long-term legal commitment or go their separate ways.
Surprisingly, despite the rapid growth in social media, dating apps and other platforms for meeting potential partners that proliferated across the decade between the two surveys, technology did not play as big a role in the minds of the participants as expected, Ogolsky said.
“When we ask people about relationship prototypes, they’re not talking about technology,” he said. “They’re thinking about relationships in broad strokes. And we found it interesting that the centerpiece of relationships was not dating apps, artificial intelligence or robots or all the other things we may have predicted 25 or 40 years ago.”
Staphylococcus aureus is a leading cause of antibiotic resistance associated infections and deaths. It is also the most prevalent bacterial infection among those with diabetes mellitus, a chronic condition that affects blood sugar control and reduces the body’s ability to fight infections.
Microbiologists at the UNC School of Medicine have just shown that people with diabetes are more likely to develop antibiotic-resistant strains of Staph, too. Their results, which were published in Science Advances, show how the diabetic microbial environment produces resistant mutations, while hinting at ways antibiotic resistance can be combatted in this patient population.
“We found that antibiotic resistance emerges much more rapidly in diabetic models than in non-diabetic models of disease,” said Brian Conlon, PhD, associate professor of immunology. “This interplay between bacteria and diabetes could be a major driver of the rapid evolution and spread of antibiotic resistance that we are seeing.”
Staph feeds off the high levels of blood glucose in diabetes, allowing it to reproduce more rapidly. The bacterium can also grow without consequence, as diabetes also impairs the immune system’s ability to destroy cells and control infection.
As the numbers of bacteria increase in a diabetic infection, so does the likelihood of resistance. Random mutations appear and some build up resistance to external stressors, like antibiotics. Once a resistant mutant is present in a diabetic infection, it rapidly takes over the population, using the excess glucose to drive its rapid growth.
“Staphylococcus aureus is uniquely suited to take advantage of this diabetic environment,” said Lance Thurlow, PhD, assistant professor of microbiology and immunology. “Once that resistant mutation happens, you have excess glucose and you don’t have the immune system to clear the mutant and it takes over the entire bacterial population in a matter of days.”
Conlon, an expert on antibiotic treatment failure, and Thurlow, an expert on Staph pathogenesis in diabetes, have long been interested in comparing the effectiveness of antibiotics in a model with and without diabetes. Using their connections within the Department of Microbiology and Immunology, the researchers brought their labs together to perform a study with antibiotics in a diabetic mouse model of S. aureus infection.
First, the team prepared a mouse model with bacterial infection in the skin and soft tissue. The mouse models were divided into two groups: one half was given a compound that selectively kills cells in the pancreas, rendering them diabetic, and the other half was not given the compound. Researchers then infected both diabetic and non-diabetic models with S. aureus and treated them with rifampicin, an antibiotic where resistance evolves at a high rate.
After five days of infection, it was time to observe the results.
Conlon and Thurlow were quick to notice that the rifampicin had practically no effect in diabetic models. So, they took some samples to investigate. Researchers were shocked to find that the bacteria had evolved to become resistant to rifampicin, with the infection harboring over a hundred million rifampicin resistant bacteria. There were no rifampicin resistant bacteria in the non-diabetic models.
Their new findings have left Conlon and Thurlow with many questions; however, they are certain that the evolution of antibiotic resistance in people with diabetes could spell trouble for the population at large.
And, even more surprisingly, the mutation had taken over the entire infection in just four days. They next inoculated diabetic and non-diabetic models with Staphylococcus aureus as before, but this time supplemented with a known number of rifampicin resistant bacteria. Again, these bacteria rapidly took over the diabetic infection, but remained as only a sub-population in non-diabetic models after 4 days rifampicin treatment.
Their new findings have left Conlon and Thurlow with many questions; however, they are certain that the evolution of antibiotic resistance in people with diabetes could spell trouble for the population at large. Antibiotic-resistant strains of bacteria spread from person to person in the same ways as other bacteria and viruses do – in the air, on doorknobs, and the food that we eat – which makes preventing these types of infections a major priority.
So, what can be done to prevent it? Well, the Conlon and Thurlow labs showed that reducing blood sugar levels in diabetic models (through administration of insulin) deprived bacteria of their fuel, keeping their numbers at bay, and reducing the chances of antibiotic-resistant mutations from occurring. Their findings suggest that controlling blood sugar through insulin use could be key in preventing antibiotic resistance.
“Resistance and its spread are not only associated with the prescription of drugs, but also the health status of those that are taking antibiotics,” said Conlon. “Controlling blood glucose then becomes really important. When we gave our mice insulin, we were able to bring their blood sugar back to normal and we didn’t get this rapid proliferation of resistant bacteria.”
Now, Conlon and Thurlow are expanding their efforts to study the evolution of resistance in humans (with and without diabetes) and other antibiotic-resistant bacteria of interest, including Enterococcus faecalis, Pseudomonas aeruginosa, and Streptococcus pyogenes. Recognizing how large a role the host plays a role in the evolution of antibiotic resistance, the researchers plan to perform similar studies in patients undergoing chemotherapy and recent transplant recipients to see if those populations are also prone to antibiotic resistant infections.
Getting at least 30 minutes of daily summer sun in the first year of life may mean a lower relapse risk for children who are diagnosed with multiple sclerosis (MS) later, according to a study published in Neurology® Neuroimmunology & Neuroinflammation, an official journal of the American Academy of Neurology. The study also found if a child’s biological mother had at least 30 minutes of daily sun during the second trimester of pregnancy, the child had a lower risk of MS relapses.
The study does not prove that sun lowers relapse risk for children with MS, it only shows an association. “It is important not to spend too much time in the sun without sun protection, however greater exposure to sun has been tied in previous research to a lower risk of developing MS in childhood,” said Gina Chang, MD, MPH, of The Children’s Hospital of Philadelphia and member of the American Academy of Neurology. “It’s encouraging that our study found that greater sun exposure during early development may also be beneficial in helping to reduce disease activity in children who are later diagnosed with MS.”
For the study, researchers looked at health records from 18 MS clinics across the United States to identify 334 children and young people with childhood-onset MS age four to 21. Participants were within four years of experiencing their first symptoms. The median follow-up time was 3.3 years. To determine sun exposure, participants’ parents or guardians completed questionnaires that asked how much time the participant and their biological mother had spent in the sun at various periods of life, what kind of clothing they typically wore and how often they used sunscreen.
Of the total group, 206, or 62%, experienced at least one relapse during the study. Relapses were defined as new or returning symptoms lasting for at least 24 hours and separated by at least 30 days from the last MS attack, without a fever or infection. They found that of 75 participants who had 30 minutes to an hour of daily summer sun during their first year of life, 34 children, or 45%, had a relapse.
Of the 182 participants who had less than 30 minutes of daily summer sun during their first year of life, 118 children, or 65%, had a relapse. After adjusting for factors such as tobacco exposure in the first year of life, season of birth, the type of MS medication taken and use of sun protection such as sunscreen, hats and clothing, researchers found that 30 or more minutes of daily summer sun during the first year of life was associated with a 33% lower risk of relapse compared to less than 30 minutes of daily summer sun.
Researchers also looked at sun exposure for the biological mothers of the children. They found that 30 minutes or more of daily sun during the second trimester of pregnancy was associated with a 32% reduced risk of relapse for their child with MS.
“Our findings suggest that sun exposure in early childhood may have long-lasting benefits on the progression of childhood-onset MS,” said Chang. “Future studies should look at how time in the sun at other time periods before and after MS diagnosis affects disease course, to better guide sun exposure recommendations for children with MS and to help design potential clinical trials.” A limitation of the study was that it relied on participants’ parents or guardians reporting their sun exposure and use of sun protection, which they may not have remembered accurately.
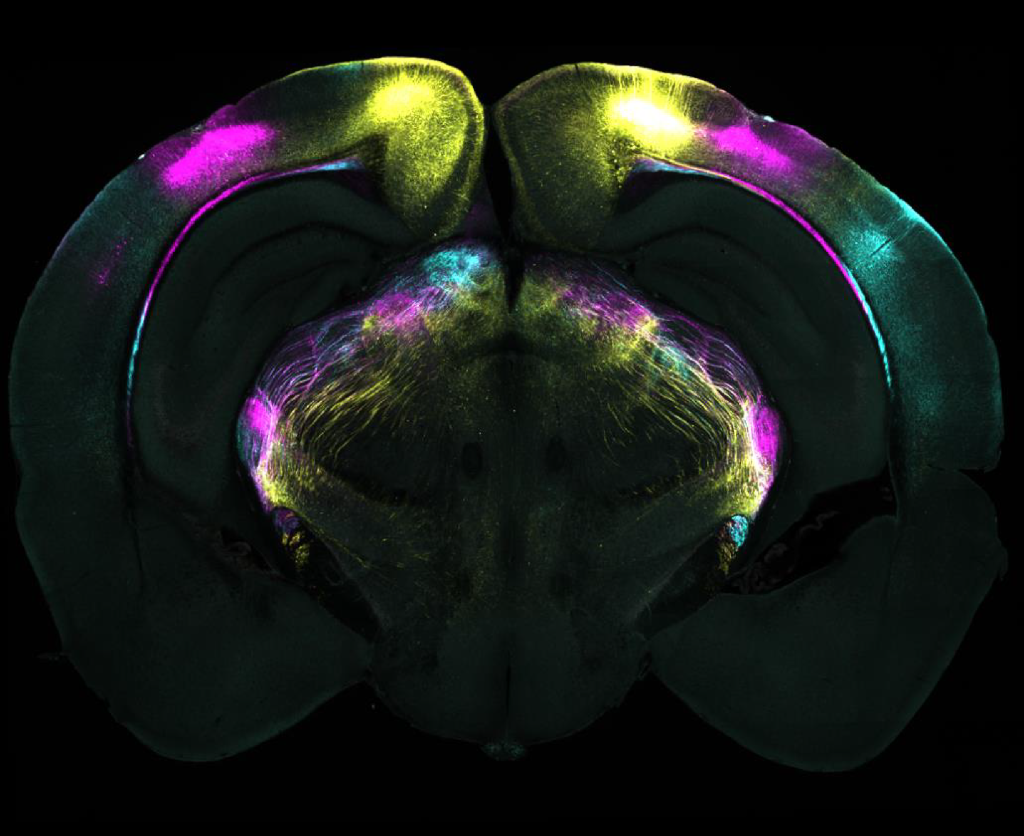
Coronal brain slice showing projections from different visual areas in the cerebral cortex to the ventrolateral geniculate nucleus (vLGN). These pathways are part of the circuit identified as mediating the suppression of instinctive fear responses.
Researchers at the Sainsbury Wellcome Centre (SWC) at UCL have unveiled the precise brain mechanisms that enable animals to overcome instinctive fears. Published today in Science, the study in mice could have implications for developing therapeutics for fear-related disorders such as phobias, anxiety and post-traumatic stress disorder (PTSD).
The research team, led by Dr Sara Mederos and Professor Sonja Hofer, mapped out how the brain learns to suppress responses to perceived threats that prove harmless over time.
“Humans are born with instinctive fear reactions, such as responses to loud noises or fast-approaching objects,” explains Dr Mederos, Research Fellow in the Hofer Lab at SWC. “However, we can override these instinctive responses through experience – like children learning to enjoy fireworks rather than fear their loud bangs. We wanted to understand the brain mechanisms that underlie such forms of learning”.
Using an innovative experimental approach, the team studied mice presented with an overhead expanding shadow that mimicked an approaching aerial predator. Initially, the mice sought shelter when encountering this visual threat. However, with repeated exposure and no actual danger, the mice learned to remain calm instead of escaping, providing researchers with a model to study the suppression of fear responses.
Based on the lab’s previous work, the team knew that the ventrolateral geniculate nucleus (vLGN) could suppress fear reactions when active and was able to track knowledge of previous experience of threat. The vLGN also receives strong input from visual areas in the cerebral cortex, and so the researchers explored whether this neural pathway had a role in learning not to fear a visual threat.
The study revealed two key components in this learning process: (1) specific regions of the visual cortex proved essential for the learning process, and (2) a brain structure called the ventrolateral geniculate nucleus (vLGN) stores these learning-induced memories.
“We found that animals failed to learn to suppress their fear responses when specific cortical visual areas were inactivated. However, once the animals had already learned to stop escaping, the cerebral cortex was no longer necessary,” explained Dr Mederos.
“Our results challenge traditional views about learning and memory,” notes Professor Hofer, senior author of the study. “While the cerebral cortex has long been considered the brain’s primary centre for learning, memory and behavioural flexibility, we found the subcortical vLGN and not the visual cortex actually stores these crucial memories. This neural pathway can provide a link between cognitive neocortical processes and ‘hard-wired’ brainstem-mediated behaviours, enabling animals to adapt instinctive behaviours.”
The researchers also uncovered the cellular and molecular mechanisms behind this process. Learning occurs through increased neural activity in specific vLGN neurons, triggered by the release of endocannabinoids – known to regulate mood and memory. This release decreases inhibitory input to vLGN neurons, resulting in heightened activity in this brain area when the visual threat stimulus is encountered, which suppresses fear responses.
The implications of this discovery extend beyond the laboratory. “Our findings could also help advance our understanding of what is going wrong in the brain when fear response regulation is impaired in conditions such as phobias, anxiety and PTSD. While instinctive fear reactions to predators may be less relevant for modern humans, the brain pathway we discovered exists in humans too,” explains Professor Hofer. “This could open new avenues for treating fear disorders by targeting vLGN circuits or localised endocannabinoid systems.”
The research team is now planning to collaborate with clinical researchers to study these brain circuits in humans, with the hope of someday developing new, targeted treatments for maladaptive fear responses and anxiety disorders.
Harnessing the power of preventative care and incentivised wellness to lessen the burden and cost of disease in South Africa.
By Damian McHugh, Chief Marketing Officer, Momentum Health.
South Africa is at a critical juncture in its healthcare landscape. The burden of disease -primarily driven by non-communicable diseases (NCDs) such as diabetes, hypertension, and mental health disorders – has escalated alarmingly. Over the past two years, NCDs have increased from 51% in 2022 to 55% in 2024, with diabetes rising by 12% and hypertension increasing from 8% to 10%1. Not only straining our healthcare system but also substantially hampering economic productivity and growth.
Current State of our Nation’s Health
It’s estimated that poor health-related absenteeism costs the South African economy up to R19.1 billion annually2. Beyond these direct financial implications, this hidden drain stifles business growth, reduces workforce efficiency, and hinders overall economic progress. Lifestyle-related diseases contribute significantly to rising healthcare costs – with an estimated R270 billion in healthcare claims projected to be linked to preventable conditions in 20253.
However, we have an opportunity to reverse this trend by embracing preventative care and incentivised wellness- two powerful levers that can help shift our healthcare paradigm from sick care to proactive disease prevention.
Why Prevention Is the Key to a Healthier, Wealthier Nation
I’ve always believed in the notion that your health is your wealth. Preventative healthcare is no doubt one of the most effective ways to reduce the burden and cost of disease. Simple lifestyle changes, such as regular exercise, balanced nutrition, deeper connections with loved ones, routine screenings to know one’s numbers, and effective stress management – have all been proven to dramatically lower the risk of chronic conditions. Yet, despite these clear benefits, many South Africans struggle to prioritise their health due to financial constraints, limited access to wellness education, and the ever-evolving demands of daily life.
This is where the private healthcare sector, in collaboration with policymakers and employers, can make a significant impact. By incentivising wellness behaviours, we can empower citizens to take control of their health while alleviating the financial burden on our healthcare system.
The Power of Incentivised Wellness
At Momentum Health, we have witnessed firsthand the positive outcomes driven by wellness rewards programmes. By rewarding members for engaging in preventative health activities—such as completing health screenings, maintaining an active lifestyle, or adopting healthier eating habits, we foster sustainable behaviour change through our wellness rewards programme, Momentum Multiply.
When effectively designed, these programmes offer tangible benefits such as lower healthcare costs through a rewards system and encourage healthier lives that rely less on medical intervention in the first place. There is sound evidence that ahealthier population results in fewer medical claims and lower insurance premiums, benefiting both individuals and employers.
It can also be linked to increased productivity as healthy bodies host healthy minds. We have seen that employees who proactively manage their health take fewer sick days, leading to enhanced workplace performance and reduced absenteeism. As a result, these factors contribute immensely to stronger economic growth asa healthier workforce contributes to improved business efficiency and a more resilient economy. However, to fully realise the potential of preventative care and incentivised wellness, we cannot do it alone. It’s pivotal that we adopt a multi-stakeholder approach.
Stronger and healthier together
A collaborative approach where healthcare insurers & providers expand access to preventative screenings, personalised health coaching, and digital health solutions that track and reward healthy habits and behaviour. Where employers adopt and implement workplace wellness programs that encourage employees to prioritise their health through corporate wellness incentives and adequate mental health support.
Where we, the private sector, work alongside Government & Policymakers strengthen the current system, build capacity for future skills andimplement national awareness campaigns to showcase the importance of preventative care.
As it stands, in 2024 the Gauteng Department of Health (GDoH) set aside R38.1 million in 2024/25 financial year and R119.7 million over the MTEF allocated for health and wellness campaigns, as well as physical activity programmes in prioritised areas such as Townships, Informal Settlement and Hostels and more recently, the GDoH announced a budget of R474.6 million in 2024/25 and R1.4 billion over the MTEF allocated for strengthening mental healthcare services. But ever more importantly, we also need every day South Africans to take proactive steps to manage their health by making better choices in the lives they live.
A Shared Responsibility for a Healthier Future
The numbers are clear. If we don’t act now, the cost of preventable diseases will only continue to rise – jeopardising both the sustainability of our healthcare system and economic stability. By harnessing the power of preventative care and incentivised wellness, we can significantly reduce the burden of disease, improve quality of life, and foster a healthier, more productive South Africa.
We remain committed to leading this change by innovating healthcare solutions that empower South Africans to take charge of their health and provide more health to more South Africans for less when they need it. Together, through collective action and a preventative mindset, we can and must build a healthier nation – one choice at a time.
Recent media reports over the future of NHI have been contradictory and hard to make sense of. Spotlight chased up those in a position to know where things stand – it seems the ANC has not in fact made any major concessions on NHI. There is however agreement that medical schemes won’t be phased out in the next few years, something that likely wouldn’t have happened in any case given the poor state of the economy and the long timeline for NHI implementation.
The ANC is holding firm on the NHI Act with Health Minister Dr Aaron Motsoaledi and the National Health Department “unaware of any compromise deals”, and the President’s office saying engagement with Business Unity SA (BUSA) is “ongoing”.
In spite of recent media reports to the contrary, neither President Cyril Ramaphosa nor Motsoaledi have conceded to any BUSA proposals on amending sections of the NHI Act. BUSA is the country’s apex business association and represents the banking, mining, and retail sectors, including the Health Funders Association, the Hospital Association of South Africa, and the Innovative Pharmaceuticals Association of South Africa.
BUSA, and several other critics of the Act, have argued that provisions should be removed that prohibit medical schemes from covering any health services covered by the NHI fund. The NHI Act has not yet been promulgated. If promulgated in its current form, the role of medical schemes will be dramatically reduced.
The DA’s spokesperson on health, Michele Clarke, told Spotlight that at the establishment of the recent GNU-convened Medium Term Development Plan (MTDP), agreement was reached that the health department would “not de-establish medical aids during the current government’s term of office”.
Spotlight understands that this amounts to a commitment not to promulgate the relevant sections of the Act in the next few years – it does not amount to a commitment to remove those sections from the act.
This is a pyrrhic victory, given that the implementation of NHI was always going to be a long-term project and that even in the most pro-NHI scenarios, the effective phasing out of medical schemes in the next few years was highly unlikely. There are also four legal challenges being brought on procedural and constitutional grounds that may further delay things.
Mist of confusion
Last week’s mist of confusion lifted when both the Presidency and Dr Stavros Nicolaou, speaking to Spotlight on behalf of BUSA, said no concessions have been made on NHI. Motsoaledi’s office also flatly denied reports that there had been any ANC or GNU compromise to remove parts of the NHI legislation that would render medical aids almost obsolete. The Spokesperson for the National Department of Health, Foster Mohale, added that he was unaware of any MTDP agreement on medical aids.
Vincent Magwenya, a spokesperson for the president, told Spotlight he was “unaware of any process leading to the amendment of the NHI Act”, claiming that Maropene Ramokgopa, Minister in the Presidency responsible for Planning, Monitoring and Evaluation, was misquoted last week.
She was quoted in news reports as saying the ANC and the DA had reached an “unofficial understanding on the NHI” following an ANC compromise to remove parts of the NHI legislation that would collapse medical aids. “Ms Ramokgopa tells me she was misreported,” said Magwenya.
Chris Laubscher, the DA’s communications head, told Spotlight: “There was never confirmation by [DA leader who is also Minister of Agriculture] John Steenhuisen that the NHI in its entirety had been excluded from the government’s Medium Term Development Plan.”
The new MTDP has not yet been made public.
Charity Ophelia McCord, the spokesperson for Steenhuisen, said the MTDP had yet to be completed and passed, but was on the Cabinet agenda for Wednesday, February 12. Spotlight was not able to verify if this was discussed.
Meanwhile, Mohale said both the health department and the minister were unaware of any compromise deal, “thus the implementation of the NHI Act continues as per the plans”.
Cannot be changed over night
If at some point the NHI Act is to be amended, the process is likely to take several years, according to Professor Olive Shisana, Social Policy Special Advisor to Ramaphosa on the NHI and health systems strengthening.
“Any process for changing an enacted law normally goes through Parliament, including an amendment from the executive,” Shisana explained. “There would first have to be consultation with the public before it even got to Parliament. Then, when it gets to Parliament there’s more consultation, this time in each of the provincial legislatures, after which it goes to the Portfolio Committee on Health which also takes written submissions. The committee then decides whether to submit it to the National Assembly. If the National Assembly passes it, it goes to the National Council of Provinces which considers each province’s input. Government took five years to get this NHI Act in place, so you can imagine it might take about as long to get parts of it excised or reversed. That’s the normal route it would have to take, I’m afraid.”
However, both the DA and BUSA are adamant that the Act needs to be changed.
Clarke said the DA remained of the view that “multiple parts of the [Act] remain problematic and dangerous for the future of healthcare in South Africa”.
She added: “The DA wants the model underpinning the NHI to be completely reworked and multiple problematic clauses amended by Parliament to ensure that the healthcare model is protected and strengthened.”
BUSA met with Ramaphosa in September last year and tabled a proposal which included striking Section 33 – which effectively collapses private medical aids as they now exist, creating a single national fund – from the NHI Act. It also calls for the implementation of mandatory health insurance which it is argued will take pressure off the public health system and bolster existing medical aids. The president has since passed it on to Motsoaledi’s office.
Neither BUSA nor the responding government parties have given any indication of when they might next meet or pronounce on the proposal.
Rejection of NHI
Meanwhile, the United Healthcare Access Coalition (UHAC), a grouping claiming to represent 80% of all private healthcare stakeholders, lodged a detailed alternative proposal with the president’s office. This entirely rejects the NHI and focuses on rehabilitating the healthcare system based on a synthesis of far-reaching recommendations which various commissions and experts have made over several decades, including the Taylor Commission and the more recent Health Market Inquiry (HMI).
In January this year, Motsoaledi promised to pronounce on the implementation of the HMI recommendations from 2019 “within weeks”. As reported by Business Day, there indeed seems to now finally be some movement on the HMI recommendations with Minister of Trade Industry and Competition Parks Tau having gazetted an exemption that newly opens the door for tariff setting in the private health sector – a move that may help rein in runaway healthcare costs.
UHAC spokesperson Dr Aslam Dasoo described their report as “everything that the NHI is not”.
“Our health pathway requires easy legislative changes and is within current fiscal constraints. We can start the process immediately. It requires a change in governance structure of the provincial health systems where politicians relinquish all direct authority over health care institutions and instead focus on strategic policy,” he previously told Spotlight.
In an online briefing launching the UHAC on Wednesday, February 12, Dasoo warned all parties in the GNU to “consider their options” as they would be “held jointly responsible” should the NHI be implemented to the detriment of South Africa.
Another UHAC executive member and CEO of the SA Private Practitioners Forum, Dr Simon Strachan, said the focus of their universal healthcare plan was on providing equitable, implementable, and sustainable healthcare.
“We need to ensure that those who can look after themselves, do (financially), while subsidising those who cannot afford to. It’s one hundred percent dependent on improving health service delivery within the public sector and creating a competitive market for people to decide where and how they access healthcare,” he said.
The UHAC coalition includes NGO’s, patient advocacy groups, the SA Medical Association, the South African Private Practitioners Forum, and the Progressive Healthcare Forum.
Asked what UHAC’s “Plan B” was if they “hit a brick wall” on their detailed proposals, Dasoo said the GNU was obliged to respond to such a widely representative proposal “otherwise they’re not fit to govern”.
Referring to the ANC, he said the party “neglected the two major healthcare systems, allowing real degradation of the public sector and an unregulated private sector with no market growth, resulting in prices going up”. He added: “If there’s any brick wall, it’s the one they’ve built.”
New postpartum depression research from the School of Medicine and Weill Cornell Medicine could lead to a blood test to identify women at risk and possibly even to a preventive treatment.
The research, published in Neuroposychopharmacology, suggests that pregnant women may have characteristic levels of certain molecules in their blood that can warn that they are at risk of developing postpartum depression (PPD). These molecules, called neuroactive steroids, are derived from progesterone.
Measuring those molecules via a simple blood test could let doctors get women treatment for PPD sooner – possibly even before symptoms appear, the researchers say. “Studying postpartum depression gives us a way to identify biological changes that occur before someone becomes depressed because the timing of postpartum depression is predictable,” said researcher Jennifer Payne, MD, an expert in reproductive psychiatry at UVA Health and the University of Virginia School of Medicine.
Understanding Postpartum Depression
Postpartum depression affects 10% to 15% of new moms.
“Postpartum is the only time in people’s lifespans when we know there is a biological trigger which guarantees that a certain percentage of people will become ill,” said Weill Cornell’s Lauren Osborne, MD, who co-led the study with Payne. “If we can untangle this biology and find predictors for it, not only will we be helping women, but it may give us a step up in trying to find predictors for other psychiatric illnesses also.”
It’s unclear why some women develop postpartum depression, but the new findings suggest that an imbalance in the body’s metabolism of progesterone may be a factor.
About the Study
To better understand the role of progesterone, the researchers focused on the hormone and on its “metabolic pathway” in the body. The scientists measured levels of neuroactive steroids derived from progesterone in the blood of 136 women during their second and third trimesters. Of these, 33 went on to develop postpartum depression after giving birth.
Two neuroactive steroids seem to affect the risk of developing PPD – pregnanolone and isoallopregnanolone. Pregnanolone acts on a particular cellular receptor to reduce stress. Isoallopregnanolone, on the other hand, acts on the same receptor to increase stress.
In the third trimester, women who went on to develop PPD had a lower pregnanolone/progesterone ratio and a higher isoallopregnanolone/pregnanolone ratio compared with those who did not, the researchers found. Elevated progesterone levels in late pregnancy were also associated with a higher risk of PPD.
Next Steps
The researchers plan to attempt to replicate their results in a larger, more diverse group of women in hopes of developing a clinical test to predict the risk of PPD. Further, they say their work could lead to a preventive treatment – possibly one of two prescription drugs, brexanolone and zuranolone, already available to treat PPD.
“We don’t know if these drugs would work as a preventive measure for people who are at risk of developing postpartum depression, but based on our findings, they have the potential to prevent [its] development,” Osborne said.
Researchers at McMaster University have made a groundbreaking discovery in the field of haematology, providing an explanation for spontaneous and unusual blood-clotting that continues to occur despite treatment with full-dose blood thinners.
The discovery, published in The New England Journal of Medicine, is expected to influence how doctors test for, and treat patients with, unusual or recurrent blood clotting, with the potential to improve patient outcomes.
Researchers found this new blood clotting disorder to have certain similarities to vaccine-induced immune thrombocytopenia and thrombosis (VITT) – a rare but aggressive clotting disorder that was caused by certain discontinued COVID-19 vaccines.
The research reveals that certain patients can develop severe blood clotting due to antibodies that closely resemble those that cause VITT, even in the absence of known triggers for such antibodies, such as blood thinners (heparin) or prior vaccination.
The newly identified disorder has been termed VITT-like monoclonal gammopathy of thrombotic significance (MGTS).
“Our study highlights the importance of recognising and diagnosing this new blood-clotting disorder,” said Theodore (Ted) Warkentin, co-first author and corresponding author of the study and professor emeritus in the Department of Pathology & Molecular Medicine at McMaster University.
“By understanding how to diagnose VITT-like MGTS, we can develop more effective treatment strategies that go beyond traditional anticoagulation,” said Warkentin, a hematologist in the Department of Medicine based at Hamilton Health Sciences’ Hamilton General Hospital.
Specialized testing was conducted at the McMaster Platelet Immunology Laboratory within the Michael G. DeGroote Centre for Transfusion Research, the only laboratory in Canada with the full repertoire of testing required to characterize the VITT-like antibodies that target the PF4 protein. Researchers performed a detailed analysis of cases exhibiting unusual blood-clotting despite patients being on full-dose blood thinners, focusing on those patients who had unexplained VITT-like antibodies that were detectable for a year or more.
The analyses identified the presence of M (monoclonal) proteins (which typically indicate plasma cell disorders), and together with the persisting VITT-like reactivities over at least 12 months (which is highly unusual for most anti-PF4 antibodies), thus pointing to an ongoing pathological process rather than a short-term anomaly.
The study included a multinational collaboration, with data collected from five patients treated at institutions in Canada, New Zealand, France, Spain, and Germany.
Collaborator Jing Jing Wang of Flinders University in Australia played a crucial role in proving for each patient that the M proteins are the pathological VITT-like antibodies. Collaborator Andreas Greinacher of Greifswald University in Germany helped in identifying similar cases in his anti-PF4 reference lab.
“The findings of this study underscore our ability to leverage fundamental molecular and biochemical science to unravel disease mechanisms,” said Ishac Nazy, co-lead author of the study and scientific director of the McMaster Platelet Immunology Laboratory and co-director of the Michael G. DeGroote Centre for Transfusion Medicine.
“This approach enables precise patient diagnosis and informs timely treatment strategies, even for previously unidentified diseases, exemplifying true bench-to-bedside translational medicine,” said Nazy, associate professor in the Department of Medicine at McMaster.
A remarkable observation was that each of the patients had failed blood thinning treatment, but they showed some benefit with unusual treatments, such as high-dose intravenous immunoglobulin (IVIG), Bruton tyrosine kinase inhibitors (ibrutinib), and plasma cell–targeted myeloma therapy. The existence of this novel blood clotting disorder has important implications for how health care providers will evaluate patients who develop unusual or difficult to treat blood clots in the future.