One in eight patients in hospitals in Africa is critically ill, and one in five of the critically ill die within a week, according to a new study in The Lancet.The researchers behind the largest study of critical illness in Africa to date conclude that many of these lives could have been saved with access to cheap life-saving treatments.
The study is the first large-scale mapping of critically ill patients in Africa. Nearly 20 000 patients in 180 hospitals in 22 African countries were surveyed in the study.
Being critically ill means having severely affected vital functions, such as extremely low blood pressure or low levels of oxygen in the blood. In the new study, researchers show that one in eight patients in African hospitals, 12.5%, is in this condition. Of these, one in five, 21%, die within a week, compared to 2.7% of those who are not critically ill.
A large proportion of critically ill patients, 69%, are treated in general wards rather than intensive care units. More than half of critically ill patients, 56%, do not receive even the basic critical care they need, such as oxygen therapy, intravenous fluids or simple airway management.
“Our study shows that there is a large and often neglected group of patients with critical illness in Africa,” says first author Tim Baker, Associate Professor at the Department of Global Public Health at Karolinska Institutet.
The researchers behind the study emphasise that these are basic but crucial health interventions that can make a big difference.
“If all patients had access to essential emergency and critical care, we could significantly reduce mortality. Moreover, these interventions are inexpensive and can be provided in general wards,” says Carl Otto Schell, researcher at the Department of Global Public Health at Karolinska Institutet and one of the initiators of the study.
From early ocean dips to ice-cold polar plunges, cold-water immersion is increasingly popular among athletes and wellness warriors. But how much of the hype is backed by science?
In the most comprehensive systematic review and meta-analysis of its kind, University of South Australia researchers have taken a deep dive into the effects of cold-water immersion on health and wellbeing.
Analysing data from 11 studies with 3177 participants, researchers found that cold-water immersion may lower stress, improve sleep quality, and boost quality of life.
UniSA researcher Tara Cain says the study, which appears in PLOS ONE, reveals time-dependant and nuanced effects on health and wellbeing measures.
“Cold-water immersion has been extensively researched and used in sporting contexts to help athletes recover, but despite its growing popularity among health and wellbeing circles, little is known about its effects on the general population,” Cain says.
“In this study, we noted a range of time-dependant results. Firstly, we found that cold-water immersion could reduce stress levels, but for only about 12 hours post exposure.
“We also noted that participants who took 20, 60, or 90 second cold showers reported slightly higher quality of life scores. But again, after three months these effects had faded.
“Benefits may be gained from cold showers as well, with one study reporting that participants who took regular cold showers experiencing a 29% reduction in sickness absence.
“We also found some links to cold-water immersion and better sleep outcomes, but the data was restricted to males, so its broader application is limited.
“And while there have been many claims that cold-water immersion experiences can boost your immunity and mood, we found very little evidence to support these claims.”
Cold-water immersion involves immersing the body partially or fully in cold water, in temperatures typically ranging from 10-15°C, and in this study, data was only included if exposure was at or above chest level, and for a minimum time of 30 seconds. It included cold showers, ice baths and cold plunges.
Co-researcher, UniSA’s Dr Ben Singh says the study also showed that cold-water immersion caused a temporary increase in inflammation.
“At first glance this seems contradictory, as we know that ice baths are regularly used by elite athletes to reduce inflammation and muscle soreness after exercise,” Dr Singh says.
“The immediate spike in inflammation is the body’s reaction to the cold as a stressor. It helps the body adapt and recover and is similar to how exercise causes muscle damage before making muscles stronger, which is why athletes use it despite the short-term increase.
“Knowing this, people with pre-existing health conditions should take extra care if participating in cold-water immersion experiences as the initial inflammation could have detrimental health impacts.”
Researchers say that while the findings highlight the potential benefits of cold-water immersion, they also underscore the highly time-dependent and contextual nature of its effects.
“Whether you are an elite athlete or everyday wellness seeker – it’s important to understand the effects of what you put your body through,” Cain says.
“Right now, there isn’t enough high-quality research to say exactly who benefits most or what the ideal approach is to cold-water immersion. More long-term studies, among more diverse populations, are needed to understand its lasting effects and practical applications.”
The government took its first steps towards the implementation of the recommendation of Health Market Inquiry into the private healthcare sector.
By Chris Bateman
Medical aid schemes will be given collective power to negotiate prices, according to draft regulations published last week. While some see the move as an important step toward reining in private healthcare prices, others argue that they do not go far enough and are legally unsound. We spoke to several leading experts about the proposed reforms.
Complaints about the high cost of private healthcare services in South Africa are nothing new. For the last two decades, above inflation increases to medical aid scheme premiums have been the norm. Added to this, many of the 16 or so percent of the population who are members of a scheme will have been asked to pay unexpected out-of-pocket co-payments at some point.
To understand why all this is happening, the Competition Commission launched a Health Market Inquiry (HMI) in 2014. The final HMI report, published in 2019, found that government had failed in its duty to regulate the private health sector, which it described as “neither efficient [nor] competitive”.
This failure in regulation has resulted in a private healthcare market that is “highly concentrated”, “characterised by high and rising costs of healthcare and medical scheme cover, and significant over utilisation without stakeholders being able to demonstrate associated improvements in health outcomes”, Justice Sandile Ngcobo, chairperson of the HMI panel, said at the time.
A key regulatory failure identified by the HMI was the absence of any effective mechanisms to keep prices under control. Medical aid schemes would set a price that they would cover – but there is nothing stopping healthcare providers from charging much higher prices. This is particularly a problem for prescribed minimum benefits (PMBs) – a set of healthcare services that schemes have to cover in full.
The HMI recommended the establishment of a supply side regulatory authority (SSRA) that would be independent from both government and the private sector. Among others, the SSRA would set maximum tariffs for PMBs as well as reference tariffs for all other health services.
In September 2020, around a year after the HMI report was released, the Competition Commission published a notice that seemed to set the ball rolling on establishing a new tariff negotiating framework along the lines of the HMI recommendation. Their proposed multilateral negotiating forum would have been governed by the Council for Medical Schemes until the SSRA could be established. But things then largely went silent, until earlier this month.
A new tariff-setting framework
On 14 February 2025, draft regulations published by the Minister of Trade Industry and Competition, Parks Tau, set out a new tariff determination framework for private healthcare in South Africa. At its core are two structures. The Tariffs Governing Body (TGB), consisting mainly of experts responsible for providing oversight in the tariff determination process, and the Multilateral Negotiating Forum (MLNF) made up of multiple stakeholders “which shall serve as the primary forum for collectively determining the maximum tariffs for prescribed and non-prescribed minimum benefits for healthcare services”.
In short, the work of negotiating and determining tariffs will be done by the MLNF, with the TGB providing some oversight and support. The TGB is also empowered to make a tariff determination when the MLNF fails to reach agreement.
The National Department of Health will have substantial control over both structures. Members of the MLNF will be appointed by the Director General of Health, and will include representatives of government, associations representing healthcare practitioners, healthcare funders, civil society, patient and consumer rights organisations, and any other regulatory body within the healthcare sector. The TGB will be located in the National Department of Health and will be chaired by an official of the department.
The regulations came in the form of a draft interim “block exemption” from certain provisions in the Competition Act. Such an exemption is required in order to enable the tariff governing body and the multilateral negotiating forum to function legally. The stated purpose of the exemption is to “contribute to the affordability of quality healthcare services…reduce costs and prevent the overutilization of healthcare services”.
In addition to the “collective determination of healthcare services tariffs”, the exemption also provides for “the collective determination of standardised diagnosis, procedure, medical device and treatment codes”, and “the collective determination of quality measurements/metrics, medicines formularies and treatment protocols/guidelines with the purpose of contributing to affordability of quality healthcare services across both PMBs and non-PMBs, contributing to reducing costs and contributing to the prevention of overutilization of healthcare services”.
The exemption doesn’t apply to everyone in the health sector. While healthcare providers like GPs and specialists are included, hospitals are not included.
Not an independent entity
While generally in favour of implementing the HMI recommendations, several experts Spotlight consulted are critical of how the government is going about it.
One line of criticism has been that the new framework is not sufficiently independent from the health department, as recommended in the HMI report.
Professor Alex van den Heever, Chair of Social Security Systems Administration and Management Studies at the University of the Witwatersrand (Wits), said the regulations deviate from the requirement for independence of any price regulator from political interference – which he points out is expressly addressed by the HMI.
In a media conference on Monday, Health Minister Dr Aaron Motsoaledi cited financial constraints for failing to set up an independent regulatory body. He also said that the department had a “mandate to manage healthcare systems”.
“We’re still looking at various options on an independent regulator, but National Treasury has severe constraints,” he said.
The exemption is for a period of three years and has been described as an interim measure.
Piecemeal implementation?
Another line of criticism is that only some HMI recommendations are being implemented, whereas the HMI stressed the need for an “inter-related” approach. While the tariff-determinations may bring down prices, it will not prevent doctors from, for example, sending people for medically unnecessary scans (a form of overutilisation).
Sharon Fonn, a professor in the School of Public Health at Wits and who was part of the HMI panel, said implementing aspects of the HMI piecemeal will neither foster competition nor protect the consumer.
“Controlling prices achieves little in the absence of the recommended holistic framework, which addresses the incentives of schemes to contract on cost, quality and demand,” she said.
Costs are influenced by both price and demand. The HMI did extensive work to show that supplier-induced demand was a problem – clearly indicating that price controls would achieve nothing in the absence of broader interventions, said Van den Heever.
“You’ll be hard pressed to find tariffs rising much faster than CPI (Consumer Price Index),” said Van den Heever. “Costs rise because of claims volumes, not the tariffs. This is because the frequency of patient consultations or in-patient days can rise in response to a fixing of prices. Providers are in a position to influence this demand. Annually you could have a 3% actual cost increase, with only a third of the increase (one percentage point) due to original price (tariff) changes. This is fully addressed in the HMI,” he added.
In response to criticism over the piecemeal implementation of HMI recommendations, Motsoaledi stressed that the HMI conceded that its recommendations would be implemented in phases.
Questions of scope
Elsabe Klink, an independent healthcare legal consultant and former advisor to the South African Medical Association, said government is mixing up the coding, protocols and Health Technology Assessments (HTA) which, on the HMI recommendations, are not up for negotiation in the MNLF.
“The HMI recommended that those functions be separate. How on earth can people negotiate on how a diabetic patient can be treated. That is a scientific question,” she said.
Klink said the HTA seems to be a veiled attempt at price control, directly for healthcare professionals and indirectly, to bar from the market devices and medications that did not make it onto the protocols or formularies.
“It [the draft regulations] purports to implement Health Market Inquiry recommendations but seems to stray into issues that are integral to NHI implementation as well, notably the HTA Committee,” said Dr Andy Gray, pharmaceutical sciences expert at the University of KwaZulu-Natal and Co-Director of the WHO Collaborating Centre on Pharmaceutical Policy and Evidence Based Practice.
Justifying the HTA measures, Motsoaledi said it was to prevent “the medical arms race” where healthcare practitioners prioritised patient volumes to enable them to beat their opponents in offering the latest technology. “This behaviour ruled by a medical arms race must end,” he said. He did not specifically explain why HTA was included in the exemption and not addressed through other regulations.
Questions of legality
Questions have also been raised over the legality of the regulations and whether or not they’d be vulnerable to litigation.
Van den Heever described the new regulations as “quite strange and extremely untidy, exposing the entire enterprise to legal challenge from the outset”. He said that the exemption bypasses normal legislative processes, that require evidence-based motivations and wide consultation.
He said the exemption went beyond competition concerns by establishing new governance structures that resembled a regulatory framework rather than a competition-related exemption.
“Furthermore, the structures and framework apply to a different minister (Health) – who has the legal authority to establish such a framework – not the Minister of Trade Industry and Competition. The Competition Act provides for exemptions, but only to facilitate competition-related objectives,” he said.
Dr Rajesh Patel, the Head of the Health System Strengthening Department at the Board of Healthcare Funders, had similar concerns. He said he finds it strange that “you need the Department of Trade Industry and Competition to tell the Department of Health to do their work”.
Could providers opt out?
Another contentious, and not entirely clear, aspect of the new framework is whether healthcare providers will be able to charge higher prices than those agreed through the MLNF.
“Perhaps one of the most problematic elements is that to protect patients, there needs to be some system to prevent opting out. It is likely that providers will opt out of this system and pass on additional costs to patients,” warned Fonn.
But, when asked about healthcare providers potentially opting out, Motsoaledi said that if that happened, “we’d be back to square one where everybody can charge whatever they want. I don’t think the HMI wanted that.” He didn’t specifically clarify how the current reforms would prevent healthcare professionals from opting out.
According to the draft regulations, the tariffs determined by the MLNF are “binding on all parties to the agreement”. It does however leave the door open for bilateral negotiations outside of the MLNF, but “only for the purpose of concluding an agreement on reductions, but not increases, on the tariffs for PMBs and non-PMBs as determined by the MLNF process”. There appears to be nothing in the regulations that would prevent healthcare providers from opting out altogether and charging what they like – although it is unclear to what extent, if at all, schemes would reimburse in such instances.
Concerns over timing
On timing, there are both concerns over how long the process has taken so far, and how long it might take going forward. This month’s draft regulations were published roughly five and a half years after the publication of the HMI report. For most of this period, Motsoaledi was not health minister.
Motsoaledi blamed the COVID-19 pandemic and the national elections that followed shortly afterward for the delay.
Health Minister Dr Aaron Motsoaledi. (Photo: Kopano Tlape/GCIS)
Patel expressed serious reservations about the ability of the health department to implement the block exemption process. “If their history is anything to go by, we will see similar delays and consequently, rising healthcare costs,” he said.
Patel said that the quickest solution to render private healthcare more affordable would be if the Competition Commission granted exemptions to allow medical schemes to collectively negotiate tariffs with willing healthcare providers. The health department, he said, need not be involved at all.
“We have serious reservations about the Department of Trade, Industry and Competition putting the power in the Department of Health’s hands to manage the block exemption process. They have actively kept private healthcare expensive and inaccessible to justify the implementation of the NHI,” he claimed.
Spotlight sent written questions to the Department of Health last week and during Monday’s media conference. Though some of our questions were addressed in the media conference, others had not been responded to by the time of publication.
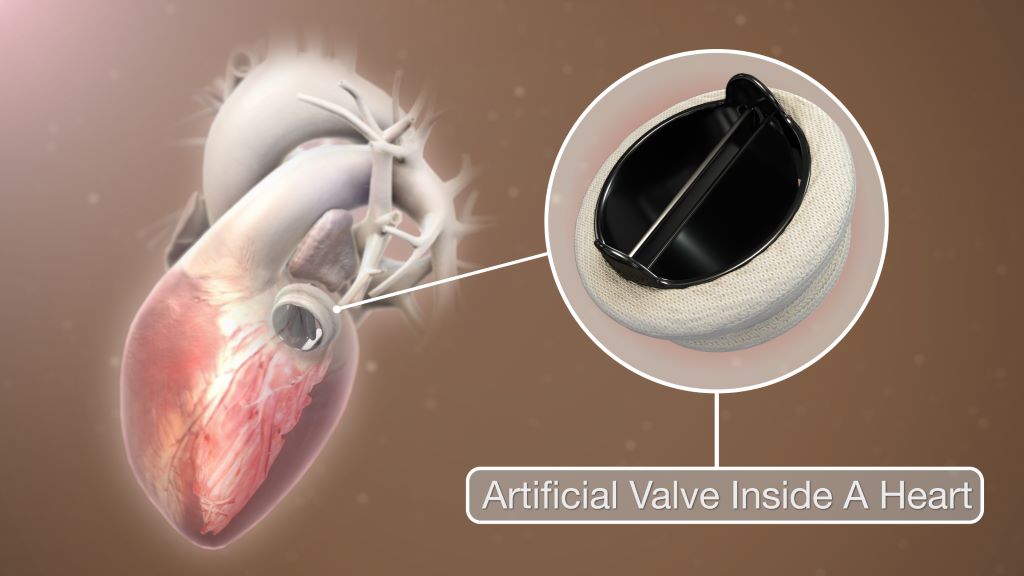
Researchers at Mayo Clinic are exploring the use of a new drug called ataciguat to manage aortic valve stenosis (AVS). Results from preclinical and clinical studies, published in Circulation, show that ataciguat has the potential to significantly slow disease progression. The final step to establish the drug’s long-term effectiveness and safety is a phase 3 trial, and efforts to launch that pivotal trial are soon to be underway with an industry partner.
In AVS, calcium deposits build up and narrow the aortic valve, forcing the heart to work harder to move blood. The condition typically progresses over time, with symptoms like chest pain, shortness of breath and fatigue affecting people over age 65. The current standard of care, watchful waiting, often leads to reduced quality of life before the condition is severe enough for the patient to have a surgical or interventional valve replacement.
“This research represents a significant advancement in the treatment of aortic valve stenosis,” says Jordan Miller, PhD, director of the Cardiovascular Disease and Aging Laboratory at Mayo Clinic. “Ataciguat has the potential to substantially delay or even prevent the need for valve replacement surgery, significantly improving the lives of millions.”
Dr Miller notes that the impact extends beyond simply delaying surgery. Younger patients with aggressive disease or congenital valve defects may develop symptoms in midlife. If a patient requires valve replacement before the age of 55, there is a more than 50% likelihood they will require multiple valve replacement surgeries over their lifetime due to recalcification of the implanted valve. Ataciguat, which slowed progression of native aortic valve calcification in the clinical trial, offers the potential for a once-in-a-lifetime procedure if they can reach the age of 65. The older a patient is, the less likely the implanted valve is to calcify.
Over the past decade, Mayo Clinic’s research revealed that ataciguat reactivates a pathway crucial in preventing valvular calcification and stenosis. Preclinical studies in mice showed that this drug substantially slowed disease progression even when treatment began after the disease was established.
Clinical trials in patients with moderate AVS demonstrated that once-daily ataciguat dosing was well tolerated, with minimal side effects compared to placebo. This latest phase 2 trial in 23 patients showed a 69.8% reduction in aortic valve calcification progression at six months compared to placebo, and patients receiving ataciguat tended to maintain better heart muscle function. Crucially, the research team confirmed that, despite its profound effect on slowing valve calcification, ataciguat did not negatively impact bone formation.
Photo by Christina Morillo: https://www.pexels.com/photo/software-engineer-standing-beside-server-racks-1181354/
Artificial Intelligence (AI) is reshaping healthcare globally, and Africa stands to benefit immensely. AI-driven telemedicine is revolutionising access to care, offering innovative solutions to overcome healthcare challenges across the continent. From remote diagnostics to virtual consultations, AI is enhancing medical services, improving efficiency, and ultimately making healthcare more accessible to millions.
Understanding Telemedicine and AI
Telemedicine leverages telecommunications technology to provide remote healthcare services. It includes virtual consultations, remote patient monitoring, electronic health records, and AI-powered diagnostics. AI, through machine learning and natural language processing, analyses vast amounts of data rapidly, identifies patterns, and provides valuable insights. With AI doing the heavy lifting in healthcare, medical professionals can focus on patient care while benefiting from advanced decision-making support.
The Importance of Healthcare Access in Africa
The World Health Organization (WHO) estimates that over 60% of Africans lack access to essential healthcare services. A shortage of healthcare professionals and inadequate infrastructure exacerbates this challenge.
In South Africa alone, 50 million people rely on state healthcare, making cost-effective, high-quality solutions a necessity. Addressing healthcare access issues is crucial for improving public health, reducing mortality rates, and enhancing overall well-being.
The Role of AI in Telemedicine
AI-driven tools are enhancing medical diagnostics, improving accuracy and efficiency. For example, AI algorithms can analyse imaging scans, such as X-rays and MRIs, to detect conditions like tuberculosis and cancer. In South Africa, AI solutions developed by Qure.ai and EnvisionIT have demonstrated remarkable accuracy in interpreting chest X-rays, often surpassing general radiologists in detecting tuberculosis.
Velocity Skin Scanning further enables rapid dermatological screenings, providing timely and accurate diagnoses.
AI-powered chatbots, such as those used in Ghana’s mPharma initiative, assist in symptom assessment, medication stock predictions, and patient guidance. Virtual consultation platforms like DabaDoc in Nigeria and CareFirst, Unu Health, and Hello Doctor in South Africa enable seamless patient-doctor interactions, particularly in underserved areas. AI streamlines these services, ensuring better patient screening, appointment scheduling, and treatment accuracy.
Challenges in AI-Driven Telemedicine Adoption
Many African regions face limited internet connectivity, device accessibility issues, and electricity shortages, hindering telemedicine implementation. Satellite internet solutions, such as Starlink and solar-powered connectivity, present potential solutions.
Supportive regulatory frameworks are crucial for AI-driven healthcare success. Governments must develop policies that encourage innovation while safeguarding patient data. Collaborative efforts between policymakers and tech companies can facilitate AI integration into healthcare systems. The African Medical Council (AMCOA) plays a key role in shaping such regulations.
Educating healthcare professionals on AI technologies is essential for effective implementation. Upskilling programs empower medical staff to utilise AI tools efficiently. Additionally, cultural acceptance of telemedicine varies, making community outreach and education initiatives vital for overcoming skepticism.
Technology costs often pose adoption challenges, particularly when solutions are not developed locally. However, virtual primary healthcare services are cost-effective and can serve as an entry point for widespread AI adoption. Strategies to enhance affordability include subscription models, public education, media promotion, healthcare practitioner reimbursement, cross-border medical registration, and economic incentives for AI adoption.
AI-Driven Solutions in Practice
CareFirst offers on-demand virtual doctor consultations, available 24/7 via video calls, telephonic consultations, and AI-driven vital scans.
Patients can access AI-driven vital scans to measure stress levels, blood pressure, heart rate, respiratory rate, glucose levels (HbA1C), and oxygen saturation. These tools provide real-time health insights, aiding proactive healthcare management.
Powered by Belle AI and endorsed by WHO, this AI-driven technology enables real-time dermatological assessments, facilitating early detection of skin conditions.
ER Consulting Inc. has adopted Scribe MD to improve medical record-keeping. This AI solution reduces doctor burnout, enhances patient interactions, lowers documentation time, mitigates medicolegal risks, and improves clinical data analysis.
Conclusion
AI-driven telemedicine has the potential to revolutionise healthcare accessibility in Africa. By addressing critical adoption barriers, fostering collaborations between governments, tech companies, and healthcare organizations, and leveraging AI-powered innovations, we can create a more connected, efficient, and inclusive healthcare ecosystem.
The future of healthcare in Africa is digital, and AI is paving the way toward a healthier, more accessible future for all.
The genetically modified CAR-T cells meant to treat the cancer themselves turned cancerous
Depiction of multiple myeloma. Credit: Scientific Animations
Some forms of blood cancer, such as multiple myeloma and lymphoma, are malignant diseases that originate from immune cells, specifically lymphocytes. In recent years, CAR-T cell therapies have become an essential part of the treatment of patients whose lymphoma or multiple myeloma has relapsed. This involves genetically modifying the patient’s own T lymphocytes (T cells) in order to specifically recognise and eliminate the cancer cells using a chimeric antigen receptor (CAR).
One special case is the subject of an article published in Nature Medicine. A 63-year-old patient with multiple myeloma developed T cell lymphoma in the blood, skin and intestine nine months after undergoing CAR-T cell therapy at the University Hospital of Cologne. The tumour developed from the genetically modified T cells that were used in the treatment.
The initiators of this collaborative project, Professor Marco Herling, managing senior physician at the University of Leipzig Medical Center and Dr Till Braun, research group leader at the University Hospital of Cologne, have world-renowned expertise in understanding the rare but difficult-to-treat T cell lymphomas. “This is one of the first documented cases of such lymphoma following CAR-T cell therapy. The findings of this study will help us to better understand the risks associated with the therapy and possibly prevent them in the future,” says Professor Maximilian Merz, who led the current study as corresponding author together with Professor Marco Herling from the University of Leipzig Medical Center.
The researchers discovered that it was not just current genetic alterations of the T cells that caused the tumour. Pre-existing genetic changes in the patient’s haematopoietic cells also played a role. The researchers used cutting-edge technologies to study the tumour’s development in detail. Various methods of next-generation sequencing – an advanced, high-throughput technology for analysing DNA and RNA sequences – were used to study the phenomenon. Whole-genome sequencing was used to identify genetic alterations, while single-cell RNA sequencing analysed the transcriptome of the CAR-T cells to investigate genes and signalling pathways.
These methods had previously been developed in close collaboration between the research groups of Professor Merz at the University of Leipzig Medical Center and Dr Kristin Reiche at the Fraunhofer IZI. The close collaboration between clinicians and basic scientists in the field of CAR-T cell therapy allowed for the case to be analysed in a very short time. The University of Leipzig Medical Center is one of the leading centres in Europe for the treatment of multiple myeloma with CAR-T cells and of T cell lymphoma. “This case provides valuable insights into the emergence and development of CAR-bearing T cell lymphoma following innovative immunotherapies and highlights the importance of genetic predispositions for potential side effects,” says Professor Merz, Senior Physician at the Department for Hematology, Cell Therapy and Hemostaseology at the University of Leipzig Medical Center.
The researchers are planning further scientific studies to better understand similar cases and identify risk factors. The aim is to be able to predict and prevent such side effects after CAR-T cell therapies, which are currently being used more and more widely, in the future. The high relevance of the topic of secondary tumours after CAR-T cell therapy has now been highlighted in a second scientific paper. The same research team submitted a manuscript to the high-impact journal Leukemia that systematically summarises this patient case and the nine other recently published cases of T cell lymphoma from CAR-T cells worldwide. Normally, it takes several weeks to months for peer reviewers to accept a scientific paper for publication. In this case, the manuscript was accepted for publication within a day. “It is important to create a real, data-based awareness of the rarity of this complication, at far less than one per cent, and the mechanisms by which it occurs,” says Professor Herling.
Continuous Glucose Monitors (CGMs) are growing in popularity but new peer-reviewed research, published in The American Journal of Clinical Nutrition, from the University of Bath, suggests they may not be as accurate as many believe. Originally designed to help people living with diabetes manage their blood sugar, these devices are now being used by the health-conscious to track how different foods affect their glucose levels.
The research measured blood sugar responses in healthy volunteers (non-diabetic, within a healthy BMI range) using two methods: a CGM (the Abbot Freestyle Libre 2, a commercially available device, also provided on the NHS) and the gold standard finger-prick test.
The research aimed to assess the accuracy of CGMs in measuring responses to various fruit-based products, ranging from whole fruit to smoothies.
The findings were striking. The CGM consistently reported higher blood sugar levels compared to finger-prick tests.
Key Findings
When participants consumed a smoothie, the Abbott Freestyle Libre 2 CGM overestimated the GI by 30%, reporting a GI of 69 (medium) compared to the traditional test result of 53 (low).
Whole fruit was misclassified as medium or high-GI foods by CGMs, while the finger-prick test showed they were low-GI. This could lead users to mistakenly believe that fruit could cause harmful spikes in blood sugar.
CGMs overestimated the time spent above the blood sugar level threshold recommended by Diabetes UK, by nearly 400%, potentially causing unnecessary worry for people whose blood sugar is actually well-controlled.
The research also debunked the common myth that blending fruits into a smoothie raises their GI. Whether eaten whole or blended, fruits like apples, bananas, mangoes, and oranges remained low on the glycaemic index.
The research concludes that CGMs are unlikely to be a valid method to determine whether a food is high or low-GI.
Professor Javier Gonzalez from the Department for Health said: “CGMs are fantastic tools for people with diabetes because even if a measurement isn’t perfectly accurate, it’s still better than not having a measurement at all. However, for someone with good glucose control they can be misleading based on their current performance. For healthy individuals, relying on CGMs could lead to unnecessary food restrictions or poor dietary choices. If you want to assess your blood sugar accurately, traditional methods are still the way to go. We want to better identify the sources of the error in CGMs so that we can improve their performance in the future and have active research on this topic.”
According to Professor Javier Gonzalez from the University of Bath, the inaccuracy of CGMs can be attributed to several factors:
“CGMs may be inaccurate because they measure glucose in the fluid surrounding your cells, not directly in your blood. This can lead to discrepancies due to factors like time delays, blood flow, and how glucose moves between different parts of the body.”
A tardigrade, otherwise known as a “water bear”. Credit: NIH
Drawing inspiration from a tiny organism that can withstand huge amounts of radiation, researchers have developed a new strategy that may protect patients from this kind of damage. Their approach makes use of a protein from tardigrades, often also called “water bears,” which are usually less than a millimetre in length.
When the researchers injected messenger RNA encoding this protein into mice, they found that it generated enough protein to protect cells’ DNA from radiation-induced damage. If developed for use in humans, this approach could benefit many cancer patients, the researchers say.
“Radiation can be very helpful for many tumours, but we also recognise that the side effects can be limiting. There’s an unmet need with respect to helping patients mitigate the risk of damaging adjacent tissue,” says Giovanni Traverso, an associate professor of mechanical engineering at MIT and a gastroenterologist at Brigham and Women’s Hospital.
Traverso and James Byrne, an assistant professor of radiation oncology at the University of Iowa, are the senior authors of the study, which appears in Nature Biomedical Engineering. The paper’s lead authors are Ameya Kirtane, an instructor in medicine at Harvard Medical School and a visiting scientist at MIT’s Koch Institute for Integrative Cancer Research, and Jianling Bi, a research scientist at the University of Iowa.
Extreme survival
Radiation is often used to treat cancers of the head and neck, where it can damage the mouth or throat, making it very painful to eat or drink. It is also commonly used for gastrointestinal cancers, which can lead to rectal bleeding. Many patients end up delaying treatments or stopping them altogether.
“This affects a huge number of patients, and it can manifest as something as simple as mouth sores, which can limit a person’s ability to eat because it’s so painful, to requiring hospitalization because people are suffering so terribly from the pain, weight loss, or bleeding. It can be pretty dangerous, and it’s something that we really wanted to try and address,” Byrne says.
Currently, there are very few ways to prevent radiation damage in cancer patients. There are a handful of drugs that can be given to try to reduce the damage, and for prostate cancer patients, a hydrogel can be used to create a physical barrier between the prostate and the rectum during radiation treatment.
For several years, Traverso and Byrne have been working on developing new ways to prevent radiation damage. In the new study, they were inspired by the extraordinary survival ability of tardigrades. Found all over the world, usually in aquatic environments, these organisms are well known for their resilience to extreme conditions. Scientists have even sent them into space, where they were shown to survive extreme dehydration and cosmic radiation.
One key component of tardigrades’ defence systems is a unique damage suppressor protein called Dsup, which binds to DNA and helps protect it from radiation-induced damage. This protein plays a major role in tardigrades’ ability to survive radiation doses 2000 to 3000 times higher than what a human being can tolerate.
When brainstorming ideas for novel ways to protect cancer patients from radiation, the researchers wondered if they might be able to deliver messenger RNA encoding Dsup to patient tissues before radiation treatment. This mRNA would trigger cells to transiently express the protein, protecting DNA during the treatment. After a few hours, the mRNA and protein would disappear.
For this to work, the researchers needed a way to deliver mRNA that would generate large amounts of protein in the target tissues. They screened libraries of delivery particles containing both polymer and lipid components, which have been used separately to achieve efficient mRNA delivery. From these screens, they identified one polymer-lipid particle that was best-suited for delivery to the colon, and another that was optimized to deliver mRNA to mouth tissue.
“We thought that perhaps by combining these two systems – polymers and lipids – we may be able to get the best of both worlds and get highly potent RNA delivery. And that’s essentially what we saw,” Kirtane says. “One of the strengths of our approach is that we are using a messenger RNA, which just temporarily expresses the protein, so it’s considered far safer than something like DNA, which may be incorporated into the cells’ genome.”
Protection from radiation
After showing that these particles could successfully deliver mRNA to cells grown in the lab, the researchers tested whether this approach could effectively protect tissue from radiation in a mouse model.
They injected the particles into either the cheek or the rectum several hours before giving a dose of radiation similar to what cancer patients would receive. In these mice, the researchers saw a 50 percent reduction in the amount of double-stranded DNA breaks caused by radiation.
The researchers also showed that the protective effect of the Dsup protein did not spread beyond the injection site, which is important because they don’t want to protect the tumour itself from the effects of radiation. To make this treatment more feasible for potential use in humans, the researchers now plan to work on developing a version of the Dsup protein that would not provoke an immune response, as the original tardigrade protein likely would.
If developed for use in humans, this protein could also potentially be used to protect against DNA damage caused by chemotherapy drugs, the researchers say. Another possible application would be to help prevent radiation damage in astronauts in space.
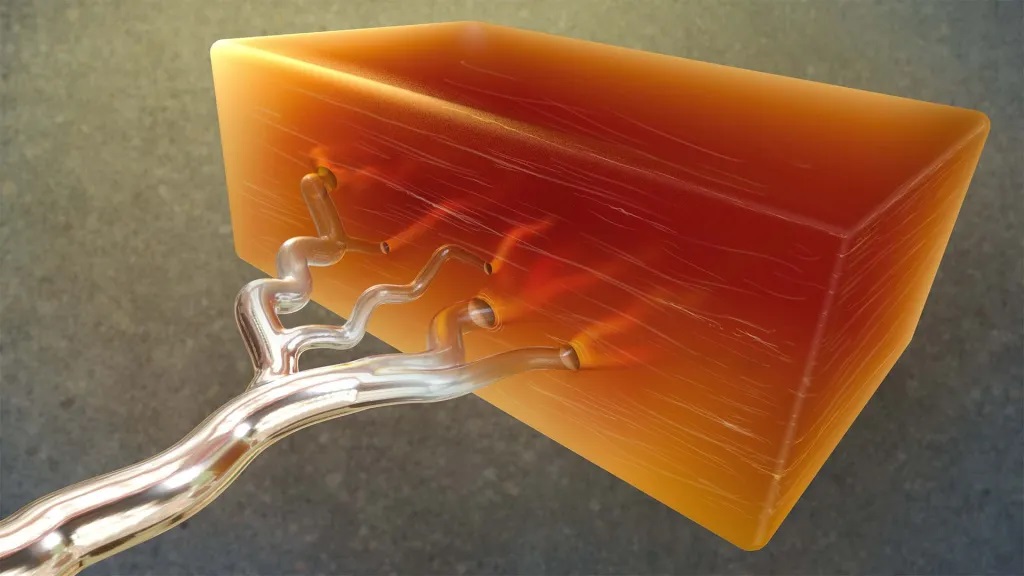
Artist’s representation of an approach for moulding biological structures in the lab using a metal called gallium. The image shows a metallic branching structure (gallium) and then empty vessels running through a block of organic tissue. Credit: Donny Bliss/NIH
The ability to engineer complex biological tissues, such alveoli or blood vessels, has vast potential to help us unlock fundamental biological insights, test new therapeutics, and one day even build fully functional replacement tissues or whole organs. But researchers have found it challenging to use current technologies such as 3D printing to produce living tissues using natural biological materials that include larger organ structures accurately constructed down to the tiny, cellular level. It has been too complex to recreate the many different tissue architectures of the human body in the lab.
A recent, NIH-supported study reported in Nature suggests a clever solution. The key is taking advantage of the natural properties of a silvery metal known as gallium, which is notable for melting at about 30°C, below body temperature, meaning it can be melted by body temperature. The new study demonstrated the metal’s use as a moulding material for generating soft biological structures complete with hollowed-out internal forms in the wide range of intricate shapes and sizes that would be needed to support the growth of larger, lifelike tissues from cells.
The team behind the new approach called ESCAPE (engineered sacrificial capillary pumps for evacuation), is led by Christopher Chen at Boston University and the Wyss Institute at Harvard University in Boston. The research team realised they needed a single process that could handle fragile biological materials while also building well at both large and extremely tiny scales.
How does ESCAPE achieve this? The strategy is much like traditional metal-casting, which has long been used to make intricate jewelry or sculptures from metals, but in reverse. In this process, a template is made from wax inside a rigid material. When the wax is melted away by molten metal, the desired form is left behind.
The researchers realized that gallium was an ideal material to work with for fashioning scaffolds for use in tissue engineering. Gallium is easy to handle and cast into desired shapes. Its low melting point and biocompatibility also made it especially appealing. In the ESCAPE approach, the researchers start by coming up with a desired shape. They then make a solid metal cast of the shape out of gallium. Next, they form a soft biomaterial around the gallium cast. When the temperature is raised, the gallium can be melted and cleanly removed, leaving behind a perfect scaffold. This works well because gallium also has a high surface tension state, which means that it can be made to readily pump itself out of a confined space. Finally, the researchers add cells to the biomaterial scaffold and grow them to form the desired tissue structure.
To demonstrate the potential of ESCAPE, the researchers chose to create blood vessel networks, including lengths at many different scales. They showed they could make complex, cell-laden vascular networks out of collagen, modelling healthy blood vessel structures, as well as some with dead ends found in disease states such as vascular malformations. The structures included 300 micrometre arterioles, as well as microvasculature ten times smaller than that. For context, the diameter of a human hair is around 75 micrometres.
The team went on to show they could produce distinct and interwoven tissue networks like those in the circulatory system. They also built cavities packed with cardiac cells lined with the blood vessels needed to feed them.
While it’s still early, the researchers say that the ESCAPE moulding approach could pave the way for producing a wide range of tissue architectures that had been previously impossible to make in the lab. They’re continuing to explore the approach with various cell types and shapes found in different organs throughout the body. The hope is that these fabricated tissues could help researchers in numerous ways, including for drug testing, the development of new treatments, and potentially one day with organ replacement.
Hormones may be leveraged to treat and prevent signs of aging such as wrinkles and hair greying, according to a new study published in the Endocrine Society journal Endocrine Reviews.
Until now, only a limited number of hormones, mainly topical retinoids (retinol and tretinoin) and oestrogen which is typically used to treat side effects of menopause, have been used in clinical practice as anti-skin aging compounds. This study reviews a new class of hormones and their anti-aging properties.
“Our paper highlights key hormone players that orchestrate pathways of skin aging such as degradation of connective tissue (leading to wrinkling), stem cell survival and loss of pigment (leading to hair greying),” said lead author Markus Böhm, MD, of the University of Münster in Germany. “Some of the hormones we studied have anti-aging properties and may be used in the future as agents to prevent skin aging.”
The skin is the largest organ and undergoes both intrinsic (chronological) and extrinsic aging which is caused by environmental factors such as sun exposure.
“Skin is not only a target for various hormones that control pathways of skin aging but itself is certainly the largest and richest site for hormone production besides classical endocrine glands,” Böhm said.
To better understand the connection between hormones and skin aging, the researchers studied the pivotal hormones controlling skin aging, including insulin-like growth factor 1, growth hormone, oestrogens, retinoids and melatonin. Melatonin is especially interesting as a potential anti-skin aging substance as it is a small molecule, inexpensive, well-tolerated and a direct and indirect antioxidant as well as a regulator of mitochondrial metabolism. Some of the studied hormones, moreover, have astonishing and unexpected biological effects on skin function and hair aging as highlighted by distinct genetic deficiency syndromes.
They also reviewed the emerging roles of additional endocrine players, including α-melanocyte-stimulating hormone (responsible for skin pigmentation), members of the hypothalamic-pituitary-thyroid axis, oxytocin, endocannabinoids (found in CBD products) and peroxisome proliferator-activated receptor modulators and found they have very promising effects, eg on UV-induced genotoxic stress crucially involved in the development of photoaging and pigment synthesis within skin and hair.
“Further research into these hormones may offer opportunities to develop new therapeutics for treating and preventing skin aging,” Böhm said.