Graphical abstract by Montesdeoca et al., JACS 2026.
Most tumours grow so rapidly that vascular growth cannot keep up, and oxygen-depleted areas form within them. A new active agent could make it possible to treat them with photodynamic therapy.
Photodynamic treatment of cancer is based on administering an initially inactive substance that is only activated in the tumour via targeted light irradiation. It then generates reactive oxygen species that kill the cancer cells. However, this method reaches its limits when no oxygen is present, as is the case with many fast-growing tumours. Professor Johannes Karges’ research group at Ruhr University Bochum has achieved a breakthrough that makes the treatment of such tumours possible: When oxygen is absent, an alternative action mechanism comes into effect. This uses hydrogen peroxide, a natural metabolic product of the cells. The researchers report their findings in the Journal of the American Chemical Society from April 6, 2026.
An entirely new action mechanism
Photodynamic therapy, or PDT, is an established method for treating cancer and is widely used in clinical practice. Karges and his team have developed an entirely new action mechanism that functions independently of the oxygen concentration within the tissue: Light converts the ruthenium-based active agent into an excited electronic state. When oxygen is present, energy is transferred to molecular oxygen, creating singlet oxygen, which has a harmful effect on cells. “This process corresponds to the conventional, oxygen-dependent mechanism of photodynamic therapy,” says Karges.
When oxygen is absent, another mechanism comes into effect. The cause is the coordination of intracellular iron to the active agent. This interaction alters the electronic characteristics of the system such that instead of a transfer of energy, an ultra-fast, metal-to-metal transfer of electrons occurs from the excited ruthenium centre to the iron centre. The hydrogen peroxide is thereby converted into highly reactive hydroxyl radicals. “Because hydrogen peroxide is a natural metabolic product of the cell, this process can occur independently of the molecular oxygen,” explains Karges. The hydroxyl radicals that have formed cause oxidative damage to central cellular structures and thus kill the cancer cells.
This means that the substance remains active even under severe conditions where past therapies have failed. In the current study, the researchers demonstrated this with breast cancer cells. “This method can be used for many different types of tumours, in principle,” says Karges. “However, we have not yet begun trying this out with human subjects and are working to develop this.”
A study conducted at the University of São Paulo shows that the pathogen can persist in these tissues for long periods, be transmitted unexpectedly, and trigger new outbreaks of the disease.
The rhinovirus can infect B lymphocytes, which produce antibodies, and CD4 T cells, which conduct the local immune response (image: PDB/Wikimedia Commons)
By Karina Toledo | Agência FAPESP – A study conducted at the University of São Paulo (USP) in Brazil reveals that tissues such as the tonsils and adenoids can serve as hiding places for the rhinovirus, which causes the common cold and is responsible for most respiratory infections worldwide.
Using samples from 293 children who underwent surgery to remove these tissues, the study showed that the pathogen can infect immune cells known as lymphocytes and remain there for long periods without causing symptoms. This allows the virus to potentially be transmitted to others without warning.
“The virus has a ‘date’ with the child population. Every year, about two or three weeks after school starts in temperate regions, there’s a rhinovirus outbreak. And children pass it on to their parents and grandparents. We’ve always wondered: What does the start of school have to do with it? Well, children gather in closed spaces, and some of them with the virus in their throats can spark an outbreak at school, even if they’re asymptomatic,” comments rhinovirologist Eurico de Arruda Neto, a professor at the Ribeirão Preto School of Medicine (FMRP-USP) and coordinator of the research, supported by FAPESP (projects 13/06380‐0, 13/16349‐2 and 17/25654‐4).
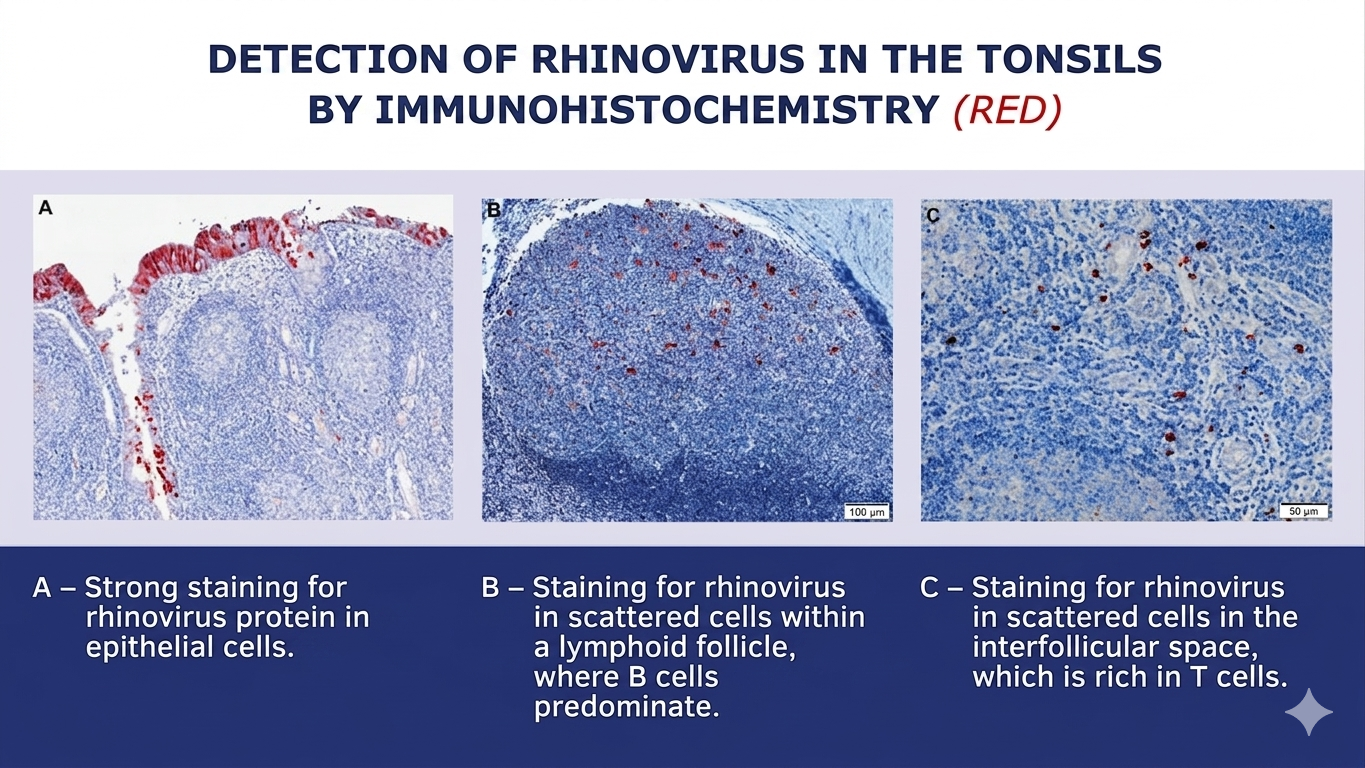
As the researcher explains, it was already known that the rhinovirus infects the epithelium (the outermost layer of the mucosa) of the nose and throat, hijacks the cellular machinery to multiply, and causes the host cell to rupture once this process is complete, releasing progeny capable of generating new infections. For this reason, scientists consider it a lytic virus, one that causes cell lysis, or rupture. This rapid and destructive cycle quickly draws the attention of the immune system, which, in most cases, eliminates the virus from the body within about five to seven days.
The major finding of the study was that the rhinovirus can reach the deeper layers of tonsil and adenoid tissues in addition to the epithelium. There, it can infect B lymphocytes, which produce antibodies, and CD4 T lymphocytes, which conduct the local immune response. These cells have a long lifespan and store the “memory” of the immune system. Rather than killing them, the rhinovirus remains inside these cells for extended periods, in a state of persistence similar to that seen with herpes viruses, HPV, and cytomegalovirus.
“The samples we analyzed are from children who underwent surgery due to snoring, sleep apnea, or recurrent infections related to tonsillar and adenoid hypertrophy. At the time of surgery, they were necessarily asymptomatic. Nevertheless, we detected the rhinovirus in a large number of participants,” says Arruda.
In addition to the tonsils and adenoids, the children’s nasal secretions were analyzed as well. According to data published in the Journal of Medical Virology, the virus was present in at least one of the three sites (tonsil, adenoid, or secretion) in 46% of the volunteers. Viral proteins and other signs that the rhinovirus was replicating – and therefore capable of infecting another person – were also observed in these tissues.
The research was conducted in collaboration with Ronaldo Martins, a virologist from the Ribeirão Preto School of Pharmaceutical Sciences (FCFRP-USP), as well as professors Wilma Anselmo-Lima, Edwin Tamashiro, and Fabiana Valera from the FMRP-USP.
(image: press release)
Virus garden
In previous studies, Arruda’s team detected adenovirus (another cause of the common cold), influenza A (flu), and SARS-CoV-2 (COVID-19) in samples of tonsils and adenoids from children who had undergone surgery. The latter two are known to cause longer-lasting infections in some patients. In the case of the rhinovirus, however, this came as a surprise.
“I get the impression that no matter what common virus we look for, we’ll find it. And not just in the tonsils and adenoids, but in other lymphoid tissues throughout the body, such as lymph nodes. We already have some preliminary evidence that lymphoid tissues are a sort of ‘garden’ for viruses. And our hypothesis is that this is a good thing. It acts as a booster for immune memory, meaning antibodies continue to be produced even long after initial exposure,” says Arruda.
However, in the case of people with asthma, this can be problematic. One hypothesis raised by the authors of the article is that infectious viruses in tonsil CD4 T lymphocytes may release inflammatory substances that act on the lungs and cause asthma attacks. It is already known that colds and the flu are among the most common causes of asthma attacks, especially in young children.
Additionally, a previous study by the group detected respiratory viruses in normal adenoids (without hypertrophy), which are located next to the Eustachian tube. This may explain why some children suffer from recurrent otitis media.
“This virus can pass from the adenoids to the middle ear and cause inflammation there. The child won’t sneeze or cough, but the ear will become inflamed, closing the narrow Eustachian tube and leading to a buildup of fluid in which the local bacterial flora begins to proliferate,” the researcher explains.
Clinical implications
Based on these findings, Arruda believes that pediatricians should be mindful of the possibility of diagnostic confusion regarding the causes of childhood illnesses.
“For example, a child with hypertrophic tonsils arrives at the emergency room with a respiratory infection and bronchiolitis symptoms caused by respiratory syncytial virus, but the throat swab test detects rhinovirus from a previous infection. In other words, tests performed on secretions may not always reflect what’s actually happening in the lungs,” says the researcher. “We have evidence that this viral persistence can also occur in people with normal-sized tonsils and adenoids.”
Another hypothesis to be investigated, Arruda says, is whether viruses that persist in lymphoid tissues can cause problems for immunosuppressed patients. “Patients who undergo bone marrow transplants, for example, frequently develop lung infections and bronchiolitis. Doctors, nurses, and medical students are usually blamed for bringing the virus into the high-risk ward. But could it be that the virus was already present in the patient’s tonsils or adenoids and has now been reactivated due to low immunity? It doesn’t have to be transmission from outside to inside. That’s what we’ve started to investigate in mice,” he explains.
Dartmouth Cancer Center (DCC) researchers have discovered that an existing, widely used blood pressure medication may help improve the effectiveness of certain cancer treatments – potentially expanding their use to many more patients and reducing toxicities.
In a new study led by clinician-scientist Tyler J. Curiel, MD, MPH, FACP, investigators found that the FDA-approved blood pressure drug telmisartan can significantly enhance the cancer-killing activity of the targeted cancer therapy olaparib.
“This study shows that a common, safe, convenient, tolerable, and inexpensive once-daily pill may significantly improve how well an important class of cancer therapies works,” said Curiel.
Exploiting cancer’s weakness
PARP inhibitor drugs, such as olaparib, work by exploiting weaknesses in how some cancer cells repair damaged DNA. PARP inhibitors are particularly effective in tumours with certain gene mutations. However, many tumours lack these mutations, limiting the number of patients who can benefit from these drugs. Cancers can also eventually develop resistance to PARP inhibitors.
In early studies, Curiel’s team discovered that when combined with olaparib, telmisartan can make tumours more vulnerable to PARP inhibitors, even when the tumours lack the gene mutations that usually make this type of drug effective.
The combination also stimulated an immune response within the tumour. Specifically, the combination of the two drugs fuelled the production of a type of molecule that helps the immune system recognize and attack cancer.
“This immune activation appears to be a key reason the combination works so well,” Curiel said.
Unique among blood pressure drugs
Telmisartan belongs to a class of medications called “angiotensin II receptor blockers” (ARBs), commonly prescribed to treat hypertension, or high blood pressure. But the DCC study found that the cancer-treatment-enhancing effects were unique to telmisartan among all of the ARBs tested.
Telmisartan also reduced levels of a protein inside tumour cells that cancers use to evade immune attack – further increasing its therapeutic potential.
“This study was about PARP inhibitors,” Curiel said. “But we also have a lot of evidence that telmisartan makes certain other chemotherapies and immunotherapies more effective through related mechanisms. Its potential could therefore extend to many other types of cancers and treatments.”
Bench to bedside: clinical trials
Telmisartan’s widespread use and high tolerability, even in people without high blood pressure, make it ideal for clinical use. Curiel’s team is already using the combination strategy in patients through two ongoing clinical trials at DCC.
One trial is for men with metastatic, castration-resistant prostate cancer. The first patient enrolled in the study experienced what Curiel described as an exceptional response to treatment. The second trial is in platinum-resistant ovarian cancer, which just enrolled its first patient.
“We are encouraged by what we are seeing so far,” Curiel said. “We have multiple trials in development to determine whether this approach can help more patients benefit from more effective cancer treatments.”
A new Yale study shows how the timing of depression in mothers and fathers affects mental health in their adult children. This includes influences on depression, anxiety, and psychotic disorders.
Timing effects across development
A research team led by Kieran O’Donnell, PhD, at Yale School of Medicine (YSM) found that pregnancy is a sensitive period, and exposure to high levels of maternal depression during pregnancy alone is associated with increased risk of psychosis in adult offspring. The findings highlight the importance of adequate mental health support during pregnancy.
The effects of maternal depression on adult symptoms of depression were detected across childhood, as well as during pregnancy, while paternal effects emerged from mid-childhood. The findings were published online in JAMA Network Open.
Study design and methods
O’Donnell and his team used a statistical framework borrowed from econometrics to analyse the study data. They analysed the effects of parental depression, assessed from pregnancy through 21 years of age, on adult mental health outcomes in a 30-year study of more than 5 000 participants.
“This is one of the most comprehensive studies – if not the most comprehensive – to ask if there are sensitive periods or developmental stages when exposure to parental depression has a particularly strong impact on later mental health,” says O’Donnell, an associate professor at Yale Child Study Center and in the Department of Obstetrics, Gynecology, and Reproductive Sciences at YSM.
Findings and implications for intervention
“Finding that parental mental health was important for long-term mental health outcomes in the next generation was not surprising, and is consistent with previous studies,” says O’Donnell. “What did come as a surprise was the clear difference in the patterns of associations between maternal and paternal depression and each mental health outcome we studied, as well as the distinct timing effects of mother’s versus father’s depression. These findings suggest that multiple and possibly distinct mechanisms underlie the associations between maternal and paternal depression and offspring mental health.”
One of the study’s goals was to investigate key periods of development when parental interventions might be most effective in promoting mental health in the next generation. Study findings suggest that earlier intervention is better, and providing adequate mental health support for parents during pregnancy is important.
“Our findings also highlight the importance of checking in on parents’ mental health across childhood,” O’Donnell adds. “Doing so will benefit parents and may also have a positive benefit on the long-term mental health outcomes of their children.”
International study supports combining advanced imaging to guide diagnosis and care
Photo by Joice Kelly on Unsplash
When Ashley Perlow felt a sharp pain shoot across her chest and into both wrists, she didn’t think it could be a heart attack. She was 36, a new mom, and otherwise healthy.
At the hospital, blood tests showed signs of a heart attack, but her arteries appeared normal.
Now, new research led by clinicians and researchers at NYU Grossman School of Medicine shows that in cases like hers, using two complementary heart imaging tests can identify the underlying cause of these heart attacks in most patients without coronary artery narrowing, helping guide diagnosis and medical treatment in a condition that often leaves patients without clear answers. The study is among the largest and most comprehensive to examine MINOCA, or myocardial infarction with non-obstructive coronary arteries, a condition that accounts for 6 to 15% of heart attacks and is about three times more common in women than men.
“When arteries are not badly blocked, it can be unclear what caused the event,” said Harmony R. Reynolds, MD, lead author and director of the Cardiovascular Clinical Research Center in the Leon H. Charney Division of Cardiology at NYU Langone Health. “What we show is that in most cases, we can find the underlying explanation, and most often it is a true heart attack. Our results support the need to do specialised imaging in all patients with MINOCA, because we could not reliably predict who will have specific imaging findings.”
The findings come from the Heart Attack Research Program (HARP), a large international, prospective study. The latest results were presented by Dr Reynolds as featured clinical research at the American College of Cardiology’s 2026 Annual Scientific Session and simultaneously published March 28 in Circulation.
Dr Reynolds and the team found that combining coronary optical coherence tomography (OCT) and a cardiac magnetic resonance imaging (MRI) identified the underlying cause of the heart event in 79 percent of study participants.
How Advanced Diagnostic Imaging Reveals the Cause
To better understand these cases in both women and men, researchers enrolled 336 patients across 28 international sites in the Unites States, Canada, and the United Kingdom. The median age of participants was 58 years, including 270 women and 66 men.
Using coronary OCT and cardiac MRI, researchers identified underlying causes, assessed how often each test provided a diagnosis, and examined differences between sexes.
During coronary OCT, a thin catheter is placed inside the coronary arteries to capture high-resolution images of the artery wall, helping detect plaque buildup or blood clots that may not appear on a standard angiogram. Cardiac MRI provides detailed images of the heart muscle, showing where damage has occurred and whether it is related to reduced blood flow, inflammation, or another cause.
Using both imaging techniques together, researchers identified a likely cause in 79% of patients.
Most (59%) had a typical heart attack mechanism related to reduced blood flow from plaque buildup, artery spasm or blood clotting, while 20% (67 patients) had conditions that mimic a heart attack, such as myocarditis, takotsubo syndrome, or other cardiomyopathies. These nonischaemic conditions require different treatment approaches than traditional heart attacks.
The new research builds on earlier work by Dr Reynolds and colleagues, published in 2020 in Circulation, that demonstrated the value of using the same imaging methods in a smaller group of women. The current study expands those findings to a larger, more diverse international population.
Implications for Patient Care
The findings provide important support for current clinical guidelines, which recommend additional imaging in these patients but have largely been based on expert consensus rather than large-scale data. The results also highlight the limitations of standard angiography, which shows blood flow but cannot detect problems within the artery wall or subtle heart muscle injuries.
The combination of OCT and cardiac MRI provided a significantly higher diagnostic yield than either test alone. The study also found that doctors cannot reliably predict which patients will benefit from one imaging test versus another based on symptoms, blood tests, or initial findings. Even patients with relatively low levels of cardiac biomarkers frequently had detectable heart damage on imaging.
“We had hoped to be able to tailor testing to individual patients,” said Dr Reynolds. “Instead, we found that comprehensive imaging is often necessary to get the full answer.”
Although MINOCA occurs more frequently in women, researchers found no significant differences in the underlying causes between women and men once the condition developed. This suggests that the disease process itself is similar once it occurs.
For Perlow, that clarity was critical. After months of unanswered questions, she was referred to Dr Reynolds at NYU Langone, where further evaluation and testing helped officially diagnose her condition as MINOCA and guide her care.
G-Chem Aquacare partners with Odyssee Environnement to improve water treatment in Free State hospitals
G-Chem Aquacare and Odyssee project team members on a Free State hospital site during the pre-selection visit in 2025
Local industrial water treatment specialist G-Chem Aquacare is partnering with global specialists to improve water, energy and carbon efficiency within Free State hospitals.
Known as the FASEP ODYAFRICA project, this groundbreaking initiative is supported by the French government through the FASEP (Fonds d’Études et d’Aide au Secteur Privé) programme, investing more than €500 000 (approximately R9.6-million) and led by Odyssee Environnement, a French industrial water treatment company specialising in hydroethical, sustainable industrial water technology and chemistry solutions.
The project represents the first deployment of Odyssee Environnement’s monitoring technologies in South Africa, combining the company’s advanced water treatment solutions with strong local implementation partner G-Chem Aquacare, and institutional collaboration with the Free State public healthcare sector.
Local hospitals rely heavily on water-intensive systems including cooling towers, steam boilers and heating infrastructure, which must be carefully managed. Without correct water treatment and monitoring, scale formation, corrosion and microbiological growth cause infrastructure failure: compromising hygiene, energy efficiency, water consumption, budgets and safety.
According to G-Chem Aquacare’s CEO Shaun Golding, South African hospitals traditionally use manual monitoring and water treatment: “The Odyssee project is data-driven and automated. Specialised monitoring equipment, sensors and smart metering will track key metrics such as water consumption, steam production and system performance in real-time,” Golding explains, adding that flow meters and other instrumentation feed data into a remote monitoring platform, allowing stakeholders to identify inefficiencies and optimise system operation.
After installation and commissioning, the project will kick off with a six-month baseline period using traditional water treatment chemistry. From December, this will transition to Odyssee film-forming amine (FFA) technology.
“This forms a protective molecular film on internal system surfaces, improving heat transfer efficiency while significantly reducing corrosion, scaling and energy losses. During the remaining 18 months, the project team will demonstrate the benefits of the French film-forming technology in a day-to-day hospital environment,” Golding advises.
A partnership built on technical expertise
G-Chem Aquacare’s relationship with Odyssee Environnement dates back to 2018. “From the very beginning, they demonstrated strong technical expertise, a high level of operational discipline, and a clear alignment with our hydroethical approach to water treatment. Together with their local knowledge and reliability, this made G-Chem Aquacare an obvious choice for this project,” explains Xavier Labeille, Export Director of Odyssee Environnement.
Early groundwork for the current project began in 2023 – 2024, with a preliminary site survey at various Free State hospitals. A formal joint site visit by both the French and South African project teams followed in September 2025.
The choice of the healthcare sector was driven by Labeille: “This decision aligns with the FASEP programme requirements, which are dedicated to public sector projects. Hospitals represent a fully public, structured and accessible environment. In addition, Odyssee Environnement has strong operational experience within hospitals in France, making this sector both relevant and technically controlled for deploying advanced monitoring technologies and chemical solutions,” he advises.
Golding explains that the Free State healthcare environment also presents a diverse mix of infrastructure and operational conditions. Initially, five hospitals were identified as potential participants. Detailed site inspections finally shortlisted three – each representing a different operational scenario.
Three Free State hospitals
At the primary site, Universitas Academic hospital in Bloemfontein, the full suite of monitoring and optimisation technologies will be installed across its boiler, cooling tower and closed-loop systems. This includes advanced sensors, specialised monitoring equipment and smart metering to demonstrate the full capability of the technology.
The secondary site – Pelonomi hospital in Bloemfontein – will receive a streamlined version with fewer monitoring devices and a simplified equipment set-up. This will demonstrate that while advanced monitoring can enhance performance, significant improvements can still be achieved through the chemistry programme, particularly through application of the film-forming technology developed by Odyssee Environnement.
At the third site – the Central/ Regional Laundry – the partners will focus on the laundry steam boiler system – which represents another important area of energy and water consumption within the context of healthcare.
Partner on the ground
As the local implementation, technical and operational partner, G-Chem Aquacare will play a vital role in the long-term success of the project. Responsibilities include on-site technical implementation of treatment programmes, system optimisation and operational support, monitoring and performance validation, training of local maintenance teams and ongoing technical collaboration with Odyssee Environnement.
“We understand the operational realities within South African healthcare facilities. Through our local technical teams and service infrastructure, we can provide on-the-ground support, regular monitoring and rapid response,” Golding observes.
The project emphasises knowledge transfer and capacity-building, ensuring that local teams are equipped to sustain improvements. G-Chem Aquacare will therefore liaise with hospital technical teams, engineers, facility managers and maintenance staff.
Training will focus on correct operation of the monitoring equipment, interpretation of system data, and management of the water treatment programme. In addition, G-Chem Aquacare will provide ongoing technical support through regular site visits, performance reviews and remote monitoring of system data.
Scalable and sustainable
Labeille points out that this project demonstrates water, energy and environmental performance: “Our objective is to establish a replicable model that can be deployed across Africa, across institutional infrastructure and industrial applications. The goal is to deliver measurable results and enable scalable, sustainable water management solutions.”
For Golding, the project reflects G-Chem Aquacare’s ongoing commitment to partnering with global technology leaders: ”We are proud to contribute to a project which not only improves operational performance but also supports the broader goals of environmental stewardship and responsible resource management,” he notes.
Technical events and workshops hosted in collaboration with universities, energy management specialists and other industry stakeholders will share the project’s objectives, progress and successes.
“We already consider G-Chem Aquacare as our strategic partner in South Africa. This project strengthens our collaboration and creates a solid foundation for further joint development across the public and industrial sectors,” Labeille concludes.
To limit the damage from the US research cuts, the SAMRC mobilised a rescue fund of about R600 million.
Spotlight Editors
It has been a bruising year or so for medical researchers in South Africa with the US pausing, cancelling, and then resuming some grants. But as bad as things were, what played out wasn’t the worst case scenario, and momentum is now building toward recovery.
For decades, the United States government has been the world’s top funder of medical research. When it started cutting research funding last year, South Africa was caught in the firing line. This is because the US administration decided to specifically target South Africa, but also because South Africa was uniquely exposed due to the sheer volume of US-funded research here.
Over recent decades, South Africa built an impressive network of research groups and infrastructure to support high quality research – all underpinned by a strong regulatory environment, several good universities, and many productive partnerships with research groups from across the world. All this, plus the fact that we have large TB and HIV epidemics, means that South Africa was, and still is, one of the best places in the world to conduct research on these two diseases.
But a weakness of South Africa’s impressive research infrastructure was its overreliance on US funding.
To be clear, this was not an overreliance on aid or charity. South African researchers won grants from the US by coming out on top in rigorous and highly competitive selection processes. Much of the research done here benefited people around the world, including in the US.
Instead, the thing that we overly relied upon was that the US would continue to make medical research grants in a way that is rational and in our common interest.
There was much chaos and uncertainty last year with the pausing, cancellation, and resuming of grants. One small positive is that bad as things were, what played out wasn’t the worst case scenario we seemed to be heading for. At least some projects got their funding flows restored. You can read more about that in this Spotlight article.
But there is no doubt that the situation remains very bleak. While some studies that were already underway will be completed, it seems very unlikely that the US will fund any new studies in South Africa in the coming years. Given the historic scale of US investment here, the total volume of clinical trials conducted in South Africa will almost certainly fall precipitously.
Charting a new course
One ray of light in all this has been the response from the South African Medical Research Council (SAMRC) – probably the best run of all the entities linked to the Department of Health.
To limit the damage from the US research cuts, the SAMRC mobilised a rescue fund of about R600 million. This includes major contributions from National Treasury, the Gates Foundation, the Wellcome Trust and the ELMA Foundation.
Some of this funding has already helped sustain dozens of research projects and protect vital expertise during a period of instability. The current funding supports work in HIV, TB, newborn and child health, as well as non-communicable and other infectious diseases.
One example is a cutting-edge HIV vaccine clinical trial that began in January at the Desmond Tutu Health Foundation’s clinical research site at Groote Schuur Hospital in Cape Town. While still in its early stages, the study aims to help piece together what an effective HIV vaccine might look like.
Beyond the SAMRC’s efforts, universities and research institutions have also stepped in, raising funds to safeguard projects and retain skilled staff whose jobs were at risk.
Even so, we are still facing a massive net loss to money for medical research in South Africa.
What to do?
Funding from international partners will remain vital in South Africa. For now, the US government still invests substantial funds in South Africa, as does several philanthropies and the European Union, through the European & Developing Countries Clinical Trials Partnership. There are also new partnerships such as one we recently reported on between South African and Korean researchers.
Such partnerships are not just about money – science thrives where there is collaboration across national borders. In fact, almost all of the most important TB and HIV clinical trials conducted in South Africa in the last two decades were collaborations between researchers from multiple countries. No matter how you slice it, collaboration with international partners will remain an essential foundation of the medical research landscape in South Africa.
The problem was never that South African researchers took too much money from the US or other donors, or worked too closely with researchers based in other countries. One might quibble on details here and there, but on the whole, US-South African research collaboration in recent decades has been a resounding success.
Rather, the problem was that we invested so little of our own funds that we became overly vulnerable to changes in external funding.
Professor Ntobeko Ntusi, president and CEO of the SAMRC, previously told Spotlight that the SAMRC receives in the region of R2 billion from government per year, including funds from both the Department of Health and the Department of Science and Innovation.
Unlike so many parts of our government, the SAMRC is a well-run entity that got clean audits in each of the last five years. This strongly suggests that money allocated to it won’t be wasted or looted. If we understand recent messaging from the Finance Minister and National Treasury, this is precisely the kind of clean government spending that should be rewarded in future budgets.
Relative to health budgets more generally and to what government has historically spent on entities such as South African Airways, the SAMRC’s budget is tiny. As far as we can tell, the current funding level is largely a product of history – apart from the still widespread atmosphere of austerity, there really isn’t any other reason why the budget shouldn’t be scaled up over the next three years to be double what it is now.
The SAMRC supports a sector in which South Africa has truly world-class capacity – capacity that as we speak remains under threat. More than just the research studies and the jobs for young scientists, what is at stake here is the idea of South Africa as a place where we can do world-class medical research. Allowing funding cuts to extinguish this bright spark, would feel like a victory for Afro-pessimism.
The reality is that if President Cyril Ramaphosa and National Treasury seizes the opportunity, the shock of the US funding cuts could be turned into a bright new beginning for medical research in South Africa – all at a price that in relative terms is very low. Let’s hope they have the vision and ambition to seize the day.
Disclosure: The Gates Foundation is mentioned in this article. Spotlight receives funding from the Gates Foundation, but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council.
Fluoride is a naturally occurring mineral that has been shown to strengthen teeth and reduce cavities. Many municipalities add fluoride to their drinking water – called community water fluoridation – as a public health measure to support dental health. In recent years, however, some have claimed that ingesting fluoride can harm children’s IQ.
Researchers at the University of Minnesota led a team that investigated the connection between fluoride in drinking water and children’s IQ to see if these claims had merit. The study, published in PNAS, examined Wisconsin state testing records, archival information about when Wisconsin cities began to fluoridate their water, and data from the Wisconsin Longitudinal Study, which has followed a random sample of 10,317 high school seniors from 1957 through 2026. Key findings include:
There is no evidence supporting a connection between community water fluoridation and children’s IQ.
There is also no evidence supporting a connection between community water fluoridation and cognitive functioning at various points later in life.
Findings confirm evidence published in previous research which also used a national sample, but considered school achievement test scores instead of actual IQ scores.
“Utah, Florida and many municipalities have chosen to remove fluoride from drinking water based on flawed studies that considered the IQ effects of exposure to massive doses of fluoride,” said lead researcher John Robert Warren, a professor in the College of Liberal Arts. “Because levels of fluoride added to municipal drinking water in the U.S. are so much lower, almost all prior evidence from those international studies is not relevant to U.S. public policy debates.”
Future research will continue examining the benefits and harms of adding fluoride to community drinking water.
Study co-author Gina Rumore, co-director of the Demography and Economics of Aging Coordinating Center at the University of Minnesota, noted that these findings “provide no support for the claim that community water fluoridation has any harmful effect on children’s IQ or on adult cognition.”
Thigh muscle fat identified as a potential modifiable risk factor for knee osteoarthritis
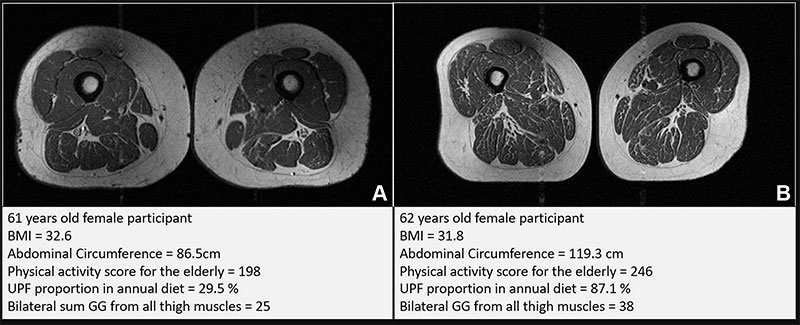
Representative axial T1-weighted spin-echo thigh MRI scans in (A) a 61-year-old female participant and (B) a 62-year-old female participant. Both participants were of similar age and body mass index (BMI, calculated as weight in kilograms divided by height in meters squared). Both had Physical Activity Scale for the Elderly scores above the mean score in the study. According to the World Health Organization definition, the participant in B qualified as having abdominal obesity (abdominal circumference ≥ 88 cm). Abdominal circumference is a measure of central obesity that captures fat distribution and serves as an indicator of cardiometabolic health. Compared with the participant in A, the participant in B had a higher proportion of ultra-processed food (UPF) in their diet (87.1% vs 29.5%) and exhibited fattier thigh muscles bilaterally, with Goutallier grade (GG) for all thigh muscles summing to 25 for the participant in A and 38 for the participant in B.
Researchers found that a diet high in ultra-processed foods is associated with higher amounts of fat stored inside thigh muscles, regardless of calorie or fat intake, physical activity or sociodemographic factors in a population at risk for knee osteoarthritis. Results of the study were published in Radiology.
Ultra-processed foods usually have longer shelf lives and can be highly appealing and convenient. They contain a combination of sugar, fat, salt and carbohydrates which affect the brain’s reward system, making it hard to stop eating.
“Over the past decades, in parallel to the rising prevalences of obesity and knee osteoarthritis, the use of natural ingredients in our diets has steadily diminished and been replaced by industrially-processed, artificially flavored, colored and chemically altered food and beverages, which are classified as ultra-processed foods,” said the study’s lead author, Zehra Akkaya, MD, researcher and consultant for the Clinical & Translational Musculoskeletal Imaging group at University of California, San Francisco, Department of Radiology and Biomedical Imaging.
Dr. Akkaya and the research team set out to assess the relationship of ultra-processed food intake and intramuscular fat in the thigh.
For the study, researchers analyzed data from 615 individuals who participated in the Osteoarthritis Initiative who were not yet affected by osteoarthritis, based on imaging. The Osteoarthritis Initiative is a nationwide research study, sponsored by the National Institutes of Health, that helps researchers better understand how to prevent and treat knee osteoarthritis.
“Osteoarthritis is an increasingly prevalent and costly global health issue,” Dr. Akkaya said. “It constitutes one of the largest non-cancer-related health care costs in the United States and around the world. It is highly linked to obesity and unhealthy lifestyle choice.”
Of the 615 individuals, (275 men, 340 women) the average age was 60 years. On average, participants were overweight with a body mass index (BMI) of 27. Approximately 41% of the foods they consumed over the prior year were ultra-processed.
The researchers found that the more ultra-processed foods people consumed, the more intramuscular fat they had in their thigh muscles, regardless of caloric intake.
“In addition to investigating the quality of our modern diet in relationship to thigh muscle composition, in this study, we used widely available, non-enhanced MRI, making our approach accessible and practical for routine clinical use and future studies,” Dr. Akkaya said. “These MRIs do not require advanced or costly technology, which means they can be easily incorporated into standard diagnostic practices.”
Half of answers to evidence based questions “somewhat” or “highly” problematic
A substantial amount of medical information provided by 5 popular chatbots is inaccurate and incomplete, with half of the answers to clear evidence based questions “somewhat” or “highly” problematic, show the results of a study published in the open access journal BMJ Open.
Continued deployment of these chatbots without public education and oversight risks amplifying misinformation, warn the researchers.
Generative AI chatbots have been rapidly adopted across research, education, business, marketing and medicine, with many people using them like search engines, including for everyday health and medical queries, explain the researchers.
To gauge the level of accuracy provided in areas of health and medicine already prone to misinformation, and therefore with consequences for everyday health behaviour, the researchers probed 5 publicly available and popular generative AI chatbots in February 2025: Gemini (Google); DeepSeek (High-Flyer); Meta AI (Meta); ChatGPT (OpenAI); and Grok (xAI).
Each chatbot was prompted with 10 open ended and closed questions in each of 5 categories of cancer, vaccines, stem cells, nutrition, and athletic performance. The prompts were designed to resemble common ‘information-seeking’ health and medical queries and misinformation tropes online and in academic discourse.
And they were developed to ‘strain’ models towards misinformation or contraindicated advice—a strategy increasingly used for stress testing AI chatbots and picking up behavioural vulnerabilities, note the researchers.
Closed prompts required chatbots to provide pre-defined responses, often with one correct answer, that aligned with the scientific consensus. Open ended prompts typically required chatbots to generate multiple responses in list form.
Responses were categorised as non-, somewhat, or highly problematic, using objective pre-defined criteria. A problematic response was defined as one that could plausibly direct lay users to potentially ineffective treatment or come to harm if followed without professional guidance.
The information was scored for accuracy and completeness, and particular attention was given to whether a chatbot presented a false balance between science and non-science based claims, regardless of the strength of the evidence.
Each response was also graded on readability, ranging from whether it was written in easy, plain English, to difficult, academic language, using the Flesch Reading Ease score.
Half (50%) the responses were problematic: 30% were somewhat, and 20% were highly problematic.
Prompt type was influential: open-ended prompts, for example, produced 40 highly problematic responses—significantly more than expected—and 51 non-problematic responses—significantly fewer than expected. The opposite was true of closed prompts.
While the quality of responses didn’t differ significantly among the 5 chatbots, Grok generated significantly more highly problematic responses than would be expected (29/50; 58%). Gemini generated the fewest highly problematic responses and the most non-problematic ones.
The chatbots performed best in the area of vaccines and cancer, and worst in the area of stem cells, athletic performance, and nutrition.
Answers were consistently expressed with confidence and certainty, with few caveats or disclaimers. Out of the total 250 questions, there were only two refusals to answer, both of which came from Meta AI in response to queries about anabolic steroids and alternative cancer treatments.
Reference quality was poor, with an average completeness score of 40%. Chatbot hallucinations and fabricated citations meant that no chatbot provided a fully accurate reference list.
All readability scores were graded as ‘difficult’, equivalent in complexity to suitability for a college graduate.
The researchers acknowledge that they only assessed 5 chatbots and that commercial AI is rapidly evolving, so their findings might not be universally applicable. And not all real-world queries are deliberately adversarial, an approach they took which may have overstated the prevalence of problematic content.
Nevertheless, “Our findings regarding scientific accuracy, reference quality, and response readability highlight important behavioural limitations and the need to re-evaluate how AI chatbots are deployed in public-facing health and medical communication,” they point out.
“By default, chatbots do not access real-time data but instead generate outputs by inferring statistical patterns from their training data and predicting likely word sequences. They do not reason or weigh evidence, nor are they able to make ethical or value-based judgments,” they explain.
“This behavioural limitation means that chatbots can reproduce authoritative-sounding but potentially flawed responses.”
The data chatbots draw on also includes Q&A forums and social media, and scientific content is typically limited to open access or publicly available articles, which comprise only 30–50% of published studies. While this enhances conversational fluency, it may come at the cost of scientific accuracy, advise the researchers.
“As the use of AI chatbots continues to expand, our data highlight a need for public education, professional training, and regulatory oversight to ensure that generative AI supports, rather than erodes, public health,” they conclude.








{kind=link}