Almost half of patients diagnosed with depression classify as being ‘treatment-resistant’ as new research suggests that many don’t respond to multiple antidepressant options.
The new study, published in the British Journal of Psychiatry was led by academics from the University of Birmingham and Birmingham and Solihull Mental Health NHS Foundation Trust. The study found that 48% of patients whose electronic healthcare records reported a diagnosis of depression had tried at least two antidepressants, and 37% had tried four or more different options.
Treatment-resistant depression (TRD) is typically defined as a form of depression that isn’t effectively managed after a patient tries two different antidepressants. There are currently few guidelines for treating TRD.
Patients who experience TRD were also invited to take part in interviews to share their experiences. Patients talked about a “sense of hopelessness” after trying multiple treatment options for the condition, and many shared their frustrations with a “one size fits all” approach to what works with treatment.
PhD researcher Kiranpreet Gill from the School of Psychology at the University of Birmingham and corresponding author of the study said:
“This paper highlights how widespread treatment-resistant depression is among those who are diagnosed with depression. With nearly half of all patients not responding to multiple drug options, we need better treatment options to be able to support patients for whom first line antidepressant medications don’t make a difference.
“Furthermore, the experiences of patients who took part in this study shows that more awareness and options for treating depression when first line antidepressant medications don’t work well is urgently needed.
“There is an irony that the experience of struggling to treat depression is in itself a risk factor for a worsening sense of ‘hopelessness’ as one patient described it. This should be a clarion call to recognise that treatment-resistant depression needs to be factored into clinical decision making and the ongoing support that patients are offered.”
There are increased risks of other psychiatric disorders among those with TRD such as anxiety, self-harm, and personality disorders, and physical health issues such as heart disease. Data analysis suggests that patients with TRD have 35% higher odds of having a personality disorder and 46% higher odds of cardiovascular disease and the combination with qualitative data suggests that patients have multiple and considerable barriers to achieving good health.
Professor Steven Marwaha, Clinical Professorial Fellow at the Institute for Mental Health at the University of Birmingham, a Consultant Psychiatrist at Birmingham and Solihull Mental Health NHS Foundation Trust, and co-author of the study said:
“This study is important as the data demonstrates people with TRD are at a higher risk of a range of poorer outcomes, and that we need better defined care pathways for helping this population, and are in urgent need of developing and testing new treatments for this group.”
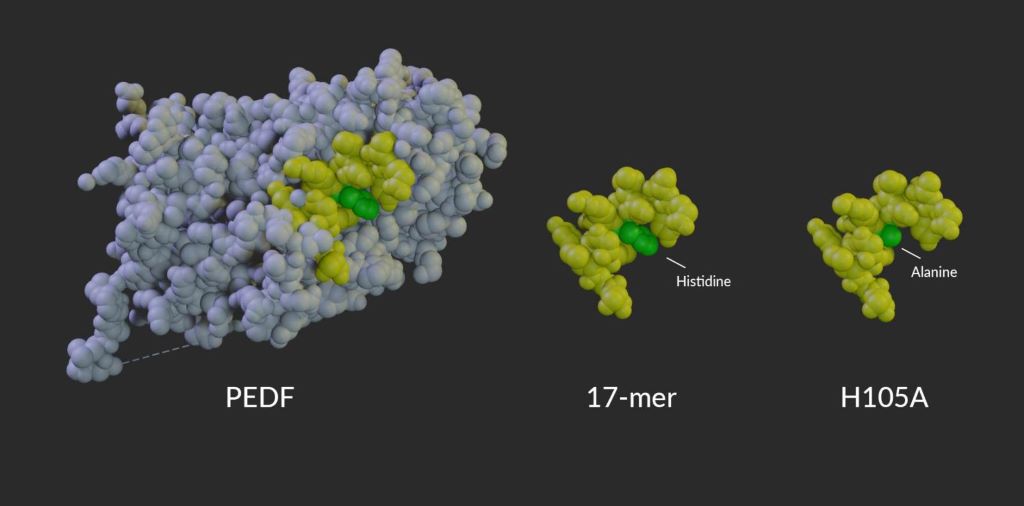
Model of PEDF protein alongside the 17-mer and H105A peptides. Amino acid 105, which is changed from histidine in PEDF and the 17-mer peptide to alanine in the H105A peptide, is shown in green.
Researchers at the National Institutes of Health (NIH) have developed eye drops that extend vision in animal models of a group of inherited diseases that lead to progressive vision loss in humans, known as retinitis pigmentosa. The eye drops contain a small fragment derived from a protein made by the body and found in the eye, known as pigment epithelium-derived factor (PEDF). PEDF helps preserve cells in the eye’s retina. A report on the study is published in Communications Medicine.
“While not a cure, this study shows that PEDF-based eye drops can slow progression of a variety of degenerative retinal diseases in animals, including various types of retinitis pigmentosa and dry age-related macular degeneration (AMD),” said Patricia Becerra, PhD, chief of NIH’s Section on Protein Structure and Function at the National Eye Institute and senior author of the study. “Given these results, we’re excited to begin trials of these eye drops in people.”
All degenerative retinal diseases have cellular stress in common. While the source of the stress may vary—dozens of mutations and gene variants have been linked to retinitis pigmentosa, AMD, and other disorders—high levels of cellular stress cause retinal cells to gradually lose function and die. Progressive loss of photoreceptor cells leads to vision loss and eventually blindness.
Previous research from Becerra’s lab revealed that, in a mouse model, the natural protein PEDF can help retinal cells stave off the effects of cellular stress. However, the full PEDF protein is too large to pass through the outer eye tissues to reach the retina, and the complete protein has multiple functions in retinal tissue, making it impractical as a treatment. To optimize the molecule’s ability to preserve retinal cells and to help the molecule reach the back of the eye, Becerra developed a series of short peptides derived from a region of PEDF that supports cell viability. These small peptides can move through eye tissues to bind with PEDF receptor proteins on the surface of the retina.
Model of PEDF protein alongside the 17-mer and H105A peptides. Amino acid 105, which is changed from histidine in PEDF and the 17-mer peptide to alanine in the H105A peptide, is shown in green.
In this new study, led by first author Alexandra Bernardo-Colón, Becerra’s team created two eye drop formulations, each containing a short peptide. The first peptide candidate, called “17-mer,” contains 17 amino acids found in the active region of PEDF. A second peptide, H105A, is similar but binds more strongly to the PEDF receptor. Peptides applied to mice as drops on the eye’s surface were found in high concentration in the retina within 60 minutes, slowly decreasing over the next 24 to 48 hours. Neither peptide caused toxicity or other side effects.
When administered once daily to young mice with retinitis pigmentosa-like disease, H105A slowed photoreceptor degeneration and vision loss. To test the drops, the investigators used specially bred mice that lose their photoreceptors shortly after birth. Once cell loss begins, the majority of photoreceptors die in a week. When given peptide eye drops through that one-week period, mice retained up to 75% of photoreceptors and continued to have strong retinal responses to light, while those given a placebo had few remaining photoreceptors and little functional vision at the end of the week.
“For the first time, we show that eye drops containing these short peptides can pass into the eye and have a therapeutic effect on the retina,” said Bernardo-Colón. “Animals given the H105A peptide have dramatically healthier-looking retinas, with no negative side effects.”
A variety of gene-specific therapies are under development for many types of retinitis pigmentosa, which generally start in childhood and progress over many years. These PEDF-derived peptide eye drops could play a crucial role in preserving cells while waiting for these gene therapies to become clinically available.
To test whether photoreceptors preserved through the eye drop treatment are healthy enough for gene therapy to work, collaborators Valeria Marigo, PhD and Andrea Bighinati, PhD, University of Modena, Italy, treated mice with gene therapy at the end of the week-long eye drop regimen. The gene therapy successfully preserved vision for at least an additional six months.
To see whether the eye drops could work in humans – without actually testing in humans directly – the researchers worked with Natalia Vergara, PhD, University of Colorado Anschutz, Aurora, to test the peptides in a human retinal tissue model of retinal degeneration. Grown in a dish from human cells, the retina-like tissues were exposed to chemicals that induced high levels of cellular stress. Without the peptides, the cells of the tissue model died quickly, but with the peptides, the retinal tissues remained viable. These human tissue data provide a key first step supporting human trials of the eye drops.
The 5th edition of the Standards for Palliative Healthcare Services has achieved a major milestone: it has secured accreditation from the International Society for Quality in Health Care’s External Evaluation Association (IEEA).
This international endorsement reaffirms the commitment of the Association of Palliative Care Centres (APCC) to deliver world-class palliative care.
As the only internationally accredited framework guiding palliative care institutions in South Africa, these Standards play a crucial role in ensuring quality, safety, and compassionate service delivery. Developed through a long-standing partnership between the Association of Palliative Care Centres (APCC) and COHSASA, the Standards have been shaping palliative care excellence since 2005.
The 5th edition—available for free at APCC’s website—features:
✔A refined presentation structure for easier navigation
✔Removal of outdated or duplicated criteria to streamline compliance
✔Changes in terms of new legislation, particularly as it relates to the POPI act
✔ New essential elements to enhance care quality
Why accreditation matters
According to Warren Oxford-Huggett, National Accreditation Manager for the APCC, earning accreditation requires time, energy and commitment, but the rewards are far-reaching.
He highlights three key benefits:
· Optimal Community Engagement – Accredited palliative service providers gain increased community trust and support, strengthening relationships between institutions, families, and caregivers. “From a patient perspective, knowing that the organisation that is providing care is accredited puts your mind at ease.”
· Better Organisational Performance – Self assessments and internal peer reviews drive higher efficiency, sustainability, credibility and overall service quality. It revolves around the framework that COHSASA sets up.
· A Culture of Excellence – Accreditation fosters a mindset of continuous improvement, embedding best practices within healthcare teams.
Oxford-Huggett also has a role to encourage more palliative care organisations to join APCC’s current 68-member network, particularly as demand grows for structured palliative care in elderly care facilities. Of the five latest institutions that are currently in the process of joining the APCC, four of them are facilities for the aged.
“The market for new APCC members is increasingly swinging to more aged care facilities. What that will mean in terms of cost of care remains to be seen”, says Oxford-Huggett. “Many elderly care institutions advertise or market palliative care, but seldom is anyone adequately trained. It’s early days but we are looking at developing a collaborative model to help these frail care facilities implement structured, high-quality care at an affordable cost. With rising living expenses and an aging population, we must ensure end-of-life care remains accessible without imposing financial strain.”
Mentorship for success
To assist APCC members in meeting these high standards, APCC offers a structured mentorship programme, led by Oxford-Huggett. This initiative guides members through the compliance process, preparing them for COHSASA’s external review and international accreditation.
APCC member, Helderberg Hospice, based in Somerset West, has just achieved their 6th accreditation, with their first accreditation achieved in May 2006. Robert de Wet, the CEO of Helderberg Hospice comments: “In addition to focusing on clinical compliance, the accreditation process assesses criteria across the entire organisation, including areas relating to governance, fundraising, administration, and human resources. Subjecting your organisation to an intensive external accreditation process is important as it serves to both affirm the positive aspects of the work we do and simultaneously makes us aware of areas in which we require more focus.” They achieved a 97% score.
Setting the Standard for Palliative Care
Since 2005, 95 APCC members have undergone COHSASA accreditation, with 117 accreditation decisions issued—ranging from full accreditation to graded recognition.
Palliative care focuses on improving quality of life for patients with serious illnesses such as cancer, HIV/AIDS and TB as well as conditions such as COPD, heart and organ failure. The APCC philosophy of palliative care is the activeholistic care of patients who have received a life-threatening diagnosis. The control of pain, of other symptoms and support for psychosocial and spiritual needs is paramount.
APCC members report that around 90% of palliative care efforts take place in patients’ homes, extending support to loved ones, from diagnosis to after bereavement.
Jacqui Stewart, CEO of COHSASA, affirms:“The international accreditation of this 5th edition confirms that the APCC standards align with global best practices. For over 20 years, the APCC and COHSASA have collaborated to ensure that South Africa’s palliative care remains internationally recognised. COHSASA is committed to driving ongoing improvements in palliative care services.”
A recent essay argues for re-considering cancer as a genetic disease
3D structure of a melanoma cell derived by ion abrasion scanning electron microscopy. Credit: Sriram Subramaniam/ National Cancer Institute
It’s time for researchers to reconsider the current paradigm of cancer as a genetic disease, argued Sui Huang from the Institute for Systems Biology, USA, and colleagues in a new essay published March 18th in the open-access journal PLOS Biology.
The prevailing theory on the origin of cancer is that an otherwise normal cell accumulates genetic mutations that allow it to grow and reproduce unchecked. This paradigm has driven large-scale cancer genome sequencing projects, such as The Cancer Genome Atlas, to identify cancer-driving mutations and develop drugs designed to target aberrant proteins and pathways.
In their new essay, Huang and colleagues argue that this somatic mutation theory of cancer is unproductive. They point to inconsistencies in the sequencing data that contradict the current theory, including the fact that many cancers have no known driver mutations while some normal tissues can harbour cancer-causing mutations.
They propose a broader, more “holistic” view that embraces organismal biology and theory. Specifically, they encourage considering alternative paradigms that encompass non-genetic processes involved in tumorigenesis. For example, they explain the concepts of cancer as a result of disruptions in gene regulatory networks (Huang) — or of tissue organisation, a theory that considers the disturbance of the field generated by neighbouring cells and surrounding tissue (Soto-Sonnenschein). The authors argue that these alternative explanations will guide experiments to advance our understanding of the origins of cancer.
The authors add: “A full embrace of the idea that the origin of cancer lies beyond the realm of genetic mutations will open new vistas on cancer treatment and prevention. Accepting that not all carcinogens are mutagens will strengthen public health policies aimed to prevent exposure to environmental non-mutagenic factors that may promote cancer, such as food additives and plastics and many other toxicants that alter tissue homeostasis.”
Past research has suggested that inflammation may contribute to the development and progression of dementia and that non-steroidal anti-inflammatory (NSAID) medications may help protect against dementia due to their anti-inflammatory effects. A new large prospective study published in the Journal of the American Geriatrics Society provides additional evidence, showing that long-term NSAID use is linked to a decreased risk of developing dementia.
In the population-based study of 11 745 adults with an average follow-up of 14.5 years, 9520 participants had used NSAIDs at any given time, and 2091 participants developed dementia. Long-term NSAID use was associated with a 12% reduced risk of developing dementia. Short- and intermediate-term use did not provide benefits. Also, the cumulative dose of NSAIDs was not associated with decreased dementia risk.
The findings suggest that prolonged, rather than intensive, use of anti-inflammatory medications may help protect against dementia.
“Our study provides evidence on possible preventive effects of anti-inflammatory medication against the dementia process. There is a need for more studies to further consolidate this evidence and possibly develop preventive strategies,” said corresponding author M. Arfan Ikram, MSc, MD, PhD, of Erasmus MC University Medical Center Rotterdam, in the Netherlands.
A review in Clinical & Experimental Allergy concludes that exposing young children to small amounts of foods that they’re allergic to is safer than avoiding the foods altogether, which could be very dangerous if accidental exposure occurs.
The review notes that exposing preschool-aged children to small amounts of food allergens—called oral immunotherapy—can lessen the severity of a reaction following an accidental exposure. Also, delaying exposure until a later age misses the window of opportunity when oral immunotherapy is safest, and it prolongs unnecessary dietary restrictions. Also, after early childhood avoidance, some people who outgrow their allergy will not reincorporate the food into their diet due to fear and anxiety, thus potentially increasing their chance of redeveloping the allergy.
A growing body of evidence indicates that oral immunotherapy is safe and effective in preschoolers, but additional research is needed to clarify its impact on children’s health and quality of life.
“This research highlights a critical shift in how we approach food allergies—moving from strict avoidance to controlled exposure in early childhood, which not only reduces the risk of severe reactions but also helps prevent long-term negative consequences of living with food allergies,” said corresponding author Lianne Soller, PhD, of the University of British Columbia, in Canada.
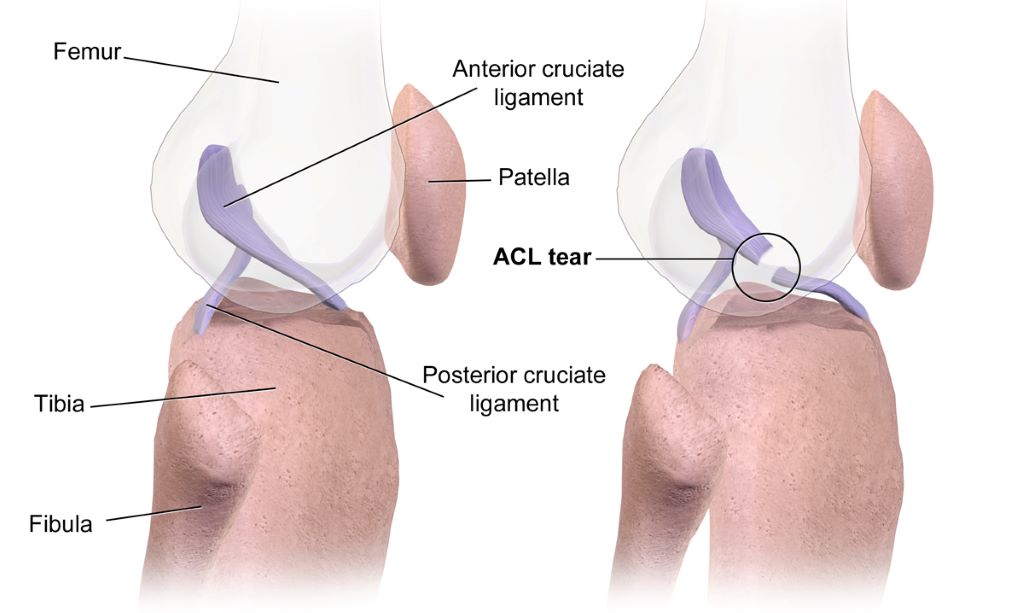
Some individuals who have had anterior-cruciate-ligament reconstruction (ACLR), the kind of surgery often performed on athletes’ knees, may develop early-onset knee osteoarthritis. A new study in the Journal of Orthopaedic Research indicates that altered knee joint movement after ACLR could be a contributing factor.
The study used a unique dynamic X-ray imaging system to accurately measure knee joint movement during walking in people who had undergone ACLR surgery and those with healthy knees. Compared with healthy controls, ACLR patients had a higher vertical position of the patella and a higher location of articular contact between the patella and the femur. A higher riding patella in the ACLR patients was caused by a longer-than-normal patellar tendon, the structure connecting the patella to the tibia. A surprising finding was that a higher riding patella was observed in both the ACLR knee and the uninjured contralateral knee of the ACLR patients.
Investigators suspect that a higher riding patella may contribute to the development of knee osteoarthritis by shifting the load bearing areas between the patella and the femur to regions of cartilage unaccustomed to load and leaving previously loaded regions unloaded.
“We don’t know whether a longer-than-normal patellar tendon that resulted in a higher riding patella existed prior to the ACL injury or resulted from the ACL injury or ACLR surgery. Further research is needed to determine the cause of a longer-than-normal patellar tendon in individuals who have undergone ACLR surgery,” said corresponding author Marcus G. Pandy, PhD, MEngSc, of the University of Melbourne, in Australia.
Patients who have been treated for heart failure and experience an improvement of their pump function, are still at higher risk of heart-related death or hospitalisation if they stop taking heart failure medications. This is according to a new study from Karolinska Institutet published in Circulation.
“Our finding raises awareness about the importance of implementing and not withdrawing medical treatments in daily clinical practice even if patients with heart failure experience an improvement in symptoms and pump function,” says the study’s last author Gianluigi Savarese, docent and senior lecturer at the Department of Clinical Science and Education, Södersjukhuset, Karolinska Institutet, and senior cardiologist at Södersjukhuset.
Using data from the Swedish Heart Failure Registry, RiksSvikt, the researchers have analysed more than 8700 patients with heart failure whose heart pump function, the ejection fraction, was initially impaired (below 40%) but later improved to 40% or more.
By linking RiksSvikt with other national registers, the researchers from Karolinska Institutet and Linköping University, Sweden, and the University of Naples, Italy, among others, were able to track hospitalisations and deaths in patients who stopped or continued various heart failure treatments.
Increased morbidity and mortality
The observational study shows that patients who stopped taking medication of the type RASi (renin-angiotensin system inhibitors), ARNi (angiotensin receptor-neprilysin inhibitors) or MRA (mineralocorticoid receptor antagonists) had between 36 and 38% higher risk of heart-related death or hospitalisation within one year of medication discontinuation.
However, stopping beta-blocker medication was only associated with a higher risk in patients whose heart function had only moderately improved.
“Our results show that heart failure medications continue to provide important benefits even when heart function has improved,” says Gianluigi Savarese. “This supports the current recommendation to continue with RASi/ARNi and MRA treatment, but also opens up the possibility of reconsidering whether beta-blockers can be discontinued in certain patients whose heart function has recovered well.”
More tailored treatment strategies
Since it was an observational study, no firm conclusions can be drawn about causality. It cannot be ruled out that the results were influenced by residual confounding. The researchers are now planning further studies to confirm the results.
“Our goal is to understand how heart failure medications affect patients with improved heart function and to develop guidelines for when/if it is safe to discontinue certain treatments. This can lead to more tailored and effective treatment strategies for heart failure patients,” says Christian Basile, the study’s first author and PhD student in Gianluigi Savarese’s research group.
Brain implants hold immense promise for restoring function in patients with paralysis, epilepsy and other neurological disorders. But a team of researchers at Case Western Reserve University has discovered that bacteria can invade the brain after a medical device is implanted, contributing to inflammation and reducing the device’s long-term effectiveness.
The groundbreaking research, recently published in Nature Communications, could improve the long-term success of brain implants now that a target has been identified to address.
“Understanding the role of bacteria in implant performance and brain health could revolutionize how these devices are designed and maintained,” said Jeff Capadona, Case Western Reserve’s vice provost for innovation, the Donnell Institute Professor of Biomedical Engineering and senior research career scientist at the Louis Stokes Cleveland VA Medical Center.
Capadona’s lab led the study, which examined the presence of bacterial DNA in the brains of mouse models implanted with microelectrodes.
To their surprise, researchers found bacteria linked to the gut inside the brain. The discovery suggests that a breach in what is known as “the blood-brain barrier,” caused by implanting the device, could allow microbes to enter.
“This is a paradigm-shifting finding,” said George Hoeferlin, the study’s lead author, who was a biomedical engineering graduate student at Case Western Reserve in Capadona’s lab. “For decades, the field has focused on the body’s immune response to these implants, but our research now shows that bacteria—some originating from the gut—are also playing a role in the inflammation surrounding these devices.”
In the study, mouse models treated with antibiotics had reduced bacterial contamination and the performance of the implanted devices improved—although prolonged antibiotic use proved detrimental.
The discovery’s implications go beyond device failure. Some of the bacteria found in the brain have been linked to neurological diseases, including Alzheimer’s, Parkinson’s and stroke.
“If we’re not identifying or addressing this consequence of implantation, we could be causing more harm than we’re fixing,” Capadona said. “This finding highlights the urgent need to develop a permanent strategy for preventing bacterial invasion from implanted devices, rather than just managing inflammation after the fact. The more we understand about this process, the better we can design implants that work safely and effectively.”
Capadona said his lab is now expanding the research to examine bacteria in other types of brain implants, such as ventricular shunts used to treat hydrocephalus, an abnormal buildup of fluid in the brain.
The team also examined the faecal matter of a human subject implanted with a brain device and found similar results.
“This finding stresses the importance of understanding how bacterial invasion may not just be a laboratory phenomenon, but a clinically relevant issue,” said Bolu Ajiboye, professor in biomedical engineering at the Case School of Engineering and School of Medicine and scientist at the Cleveland VA Medical Center. “Through our strong translational pipeline between CWRU and the VA, we are now investigating how this discovery can directly contribute to safer, more effective neural implant strategies for patients.”
Finance Minister Enoch Godongwana holding a copy of the 2025 Budget Speech. (Photo: Parliament of RSA via X)
By Charles Parry, Funeka Bango, Tamara Kredo, Wanga Zembe, Michelle Galloway, Renee Street and Caradee Wright
While the 2025 national budget boosts health spending, researchers from the South African Medical Research Council stress the need for strong accountability measures. They also raise concerns about rising VAT and omissions related to US funding cuts and climate change.
The 2025 budget speech by Finance Minister Enoch Godongwana saw a welcome boost to the health budget with an increased allocation from R277 billion in 2024/2025 to R329 billion in 2027/2028. This signals a government that is responding to the dire health needs of the public sector, that serves more than 80% of the South African population.
As researchers at the South African Medical Research Council (SAMRC), we listened with interest and share our reflections on some of the critical areas of spend relevant for health and wellbeing.
We note the increase in investment in human resources for health and allocations for early childhood development and social grants. At the same time, we also raise concern about increasing VAT, with knock-on effects for the most vulnerable in our country. There were also worrying omissions in the speech, such as addressing the impact of the United States federal-funding freeze on healthcare services nationally, and a noticeable absence of comment on government’s climate-change plans.
Health and the link with social development: Recognising the importance of early childhood development
Education and specifically early childhood development (ECD) is known to have critical impacts on children’s health and wellbeing, with longstanding effects into youth and adulthood. In South Africa, eight million children go hungry every day, and more than a third of children are reported to live in households below the food poverty line, that is below the income level to meet basic food requirements, not even covering other basic essentials such as clothes.
While the increase in the number of registered ECDs is laudable, many more ECD centres in low-income areas remain unregistered, which means they do not get support from the government in terms of subsidies and oversight.
Social grants
The increase in social grants is welcomed. However, the marginal increase of the Child Support Grant (CSG) by only R30, from R530 to R560, is too little to impact on the high levels of child hunger and malnutrition. The release of the Child Poverty Review in 2023, which highlighted the eight million children going hungry every day, including CSG recipients, proposed the immediate increase of the CSG to at least the Food Poverty Line (R796 in 2024).
Social relief of distress still too small
The Social Relief of Distress (SRD) Grant is an important source of income for low-income, working-age, unemployed adults. Its continuance in 2025 is welcomed. However, it remains too small at R370 per person per month, and the stringent means-test criteria which disrupt continuous receipt from month-to-month, makes it an unreliable, unpredictable source of income for low-income individuals.
Strengthening the healthcare workforce
The Minister stated that “R28.9 billion is added to the health budget, mainly to keep about 9 300 healthcare workers in our hospitals and clinics”. It will also be used to employ 800 post-community service doctors, and to ensure that our pharmacies do not run out of medicines. The speech highlighted the necessary commitment to strengthening the healthcare system, specifically human resources for health.
Considering the pressures on resources, primarily due to the escalating disease burden and challenges within the health workforce, the proposed budget increase from R179 billion to R194 billion – an increase of 8.2% – to maintain the current workforce and employ additional healthcare workers signifies a positive step forward that will aid in addressing staff shortages.
Despite the gains in health spending, the proposed increase in VAT raises substantial concerns to partially negate the potential benefits to the health sector. As the World Bank reports that approximately 60% of people living in South Africa live below the poverty line, increases to VAT will likely drive poverty levels higher.
A focus on other forms of taxation may be better, more evidence-based, and less likely to disproportionately affect those at the highest levels of poverty.
On the issue of alcohol taxes, often mischaracterised as “sin taxes” rather than “health taxes”, the Minister has proposed excise duties of 6.75% on most products for 2025/26. This is 2% above consumer inflation, which stands at 4.75%.
Raising alcohol prices through higher excise taxes is globally recognised as an effective way to address alcohol-related harms. National Treasury is to be commended for adjusting alcohol excise tax rates above CPI in the 2025/26 Budget. This is a move in the right direction, but it does not address the current anomalies in tax rates across different products. This failure to address shortcomings in the excise tax regime is expected, given the release of a discussion document on alcohol excise taxes in December 2024 with a February 2025 response date. The earliest we can expect substantial changes in excise tax rates is in February 2026.
From a public-health perspective, it makes sense to link alcohol excise taxes to the absolute alcohol content of the product to standardise across products. Ethanol is ethanol. The current differential in excise tax rates on different alcohol products is indefensible. Specifically, it makes no sense to tax wine and beer so much less than spirits in terms of absolute alcohol content. Wine, especially bag-in-box wine, is the cheapest product on the market in South Africa, and its affordability increases consumption, leading to more societal harm.
Beer is the most consumed product in the country and is increasingly sold in larger, non-resealable containers. A 2015 SAMRC study in Gauteng found the highest level of heavy episodic drinking with beer products, largely due to their affordability, especially in larger, non-resealable containers. Heavy episodic drinking is a major public-health concern in South Africa, with 43.0% of current drinkers engaging in heavy episodic drinking at least monthly, 50.9% of male and 30.3% of female drinkers. Increasing the excise tax on beer is a powerful tool that the state can use to reduce the level of such behaviour.
Additionally, it makes sense to have lower taxes on alcohol products with lower alcohol content, as this could shift consumption to less harmful products. The current excise tax regimen does not account for this within a single product type like beer or wine, as all products are taxed at the same rate regardless of their alcohol content.
During the COVID-19 pandemic, we saw the benefits of decreased access to alcohol: fewer injuries, fewer unnatural deaths, and communities less disrupted by patrons visiting liquor outlets. While no one advocates for total liquor sales bans, increasing excise taxes on wine and beer would decrease alcohol consumption and reduce harms on drinkers, on others around them, and on society more broadly.
Acute risk to lives with knock on effects due to US federal funding cuts
We believe the South African government has a responsibility to step into the gap left by the sudden US federal funding freeze on HIV and TB services. The US President’s Emergency Plan for AIDS Relief (PEPFAR) funds 17% of HIV and TB services in South Africa and covers salaries for thousands of health workers, including the vital services of community health workers.
The implications for people living with HIV and TB and affected by the externally funded services will be devastating. It will also have ripple effects on the health system as we see inevitable increases in demand for health services to address advancing illness, effects on families caring for ill relatives or losing income.
This area needs to be addressed and clear communication from the National Department of Health is urgently awaited. The US funding cuts clearly impact on essential research funding available to institutions like the SAMRC and no indication has been given in the budget of any plans to augment or replace such funding.
National Health Insurance for South Africa’s public sector
The Minister addressed budget allocations for NHI implementation, specifically, the mid-term indirect and direct conditional grants for NHI were R8.5 billion and R1.4 billion respectively. Although these amounts in themselves are minor compared to other health-budget allocations, allocations for infrastructure (R37.4 billion over the mid-term economic framework period) and additionally allocations for digital patient health information systems, chronic medicine dispensing and distribution systems, and medicine stock surveillance systems are vital for healthcare efficiency and improved outcomes.
Least said not soonest mended: climate change – ‘no comment’?
From a climate-crisis perspective, although the budget speech did not explicitly mention climate change or its related health challenges, there seems to be positive steps being taken to address these issues. Initiatives such as clean energy projects and efforts to improve water management have the potential to benefit all sectors of society, while helping to mitigate the health risks associated with climate change.
Promising spend on health, but who will measure the impact?
Ultimately, increasing health spend is a promising step to increase access to quality health services for South Africa’s population. However, this is not enough, government must seize the opportunity to translate the budget increase into improved health outcomes. The effectiveness of the additional funds must be maximised through efficiency, transparency, and sound governance. The government can reinforce the integrity of public-health services by aligning these increases with robust accountability measures.
Government-academic partnerships represent an opportunity to share knowledge, technical skills and resources to support evidence-informed decision-making for national health decision-making and strengthen monitoring and evaluation mechanisms. There are many examples of this working well, and we trust that the SAMRC, along with the network of higher education institutions are well placed to provide the necessary support.
*Parry, Bango, Kredo, Zembe, Galloway, Street and Wright are researchers with the SAMRC.
Note: Spotlight aims to deepen public understanding of important health issues by publishing a variety of views on its opinion pages. The views expressed in this article are not necessarily shared by the Spotlight editors.