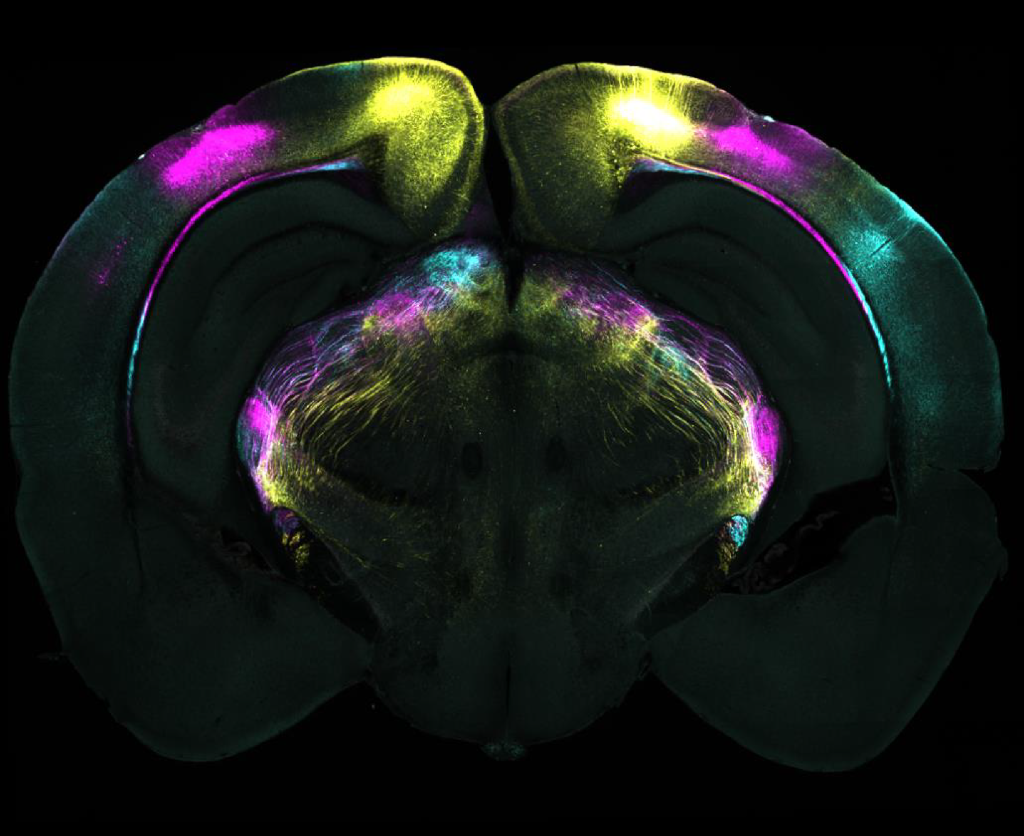
Coronal brain slice showing projections from different visual areas in the cerebral cortex to the ventrolateral geniculate nucleus (vLGN). These pathways are part of the circuit identified as mediating the suppression of instinctive fear responses.
Researchers at the Sainsbury Wellcome Centre (SWC) at UCL have unveiled the precise brain mechanisms that enable animals to overcome instinctive fears. Published today in Science, the study in mice could have implications for developing therapeutics for fear-related disorders such as phobias, anxiety and post-traumatic stress disorder (PTSD).
The research team, led by Dr Sara Mederos and Professor Sonja Hofer, mapped out how the brain learns to suppress responses to perceived threats that prove harmless over time.
“Humans are born with instinctive fear reactions, such as responses to loud noises or fast-approaching objects,” explains Dr Mederos, Research Fellow in the Hofer Lab at SWC. “However, we can override these instinctive responses through experience – like children learning to enjoy fireworks rather than fear their loud bangs. We wanted to understand the brain mechanisms that underlie such forms of learning”.
Using an innovative experimental approach, the team studied mice presented with an overhead expanding shadow that mimicked an approaching aerial predator. Initially, the mice sought shelter when encountering this visual threat. However, with repeated exposure and no actual danger, the mice learned to remain calm instead of escaping, providing researchers with a model to study the suppression of fear responses.
Based on the lab’s previous work, the team knew that the ventrolateral geniculate nucleus (vLGN) could suppress fear reactions when active and was able to track knowledge of previous experience of threat. The vLGN also receives strong input from visual areas in the cerebral cortex, and so the researchers explored whether this neural pathway had a role in learning not to fear a visual threat.
The study revealed two key components in this learning process: (1) specific regions of the visual cortex proved essential for the learning process, and (2) a brain structure called the ventrolateral geniculate nucleus (vLGN) stores these learning-induced memories.
“We found that animals failed to learn to suppress their fear responses when specific cortical visual areas were inactivated. However, once the animals had already learned to stop escaping, the cerebral cortex was no longer necessary,” explained Dr Mederos.
“Our results challenge traditional views about learning and memory,” notes Professor Hofer, senior author of the study. “While the cerebral cortex has long been considered the brain’s primary centre for learning, memory and behavioural flexibility, we found the subcortical vLGN and not the visual cortex actually stores these crucial memories. This neural pathway can provide a link between cognitive neocortical processes and ‘hard-wired’ brainstem-mediated behaviours, enabling animals to adapt instinctive behaviours.”
The researchers also uncovered the cellular and molecular mechanisms behind this process. Learning occurs through increased neural activity in specific vLGN neurons, triggered by the release of endocannabinoids – known to regulate mood and memory. This release decreases inhibitory input to vLGN neurons, resulting in heightened activity in this brain area when the visual threat stimulus is encountered, which suppresses fear responses.
The implications of this discovery extend beyond the laboratory. “Our findings could also help advance our understanding of what is going wrong in the brain when fear response regulation is impaired in conditions such as phobias, anxiety and PTSD. While instinctive fear reactions to predators may be less relevant for modern humans, the brain pathway we discovered exists in humans too,” explains Professor Hofer. “This could open new avenues for treating fear disorders by targeting vLGN circuits or localised endocannabinoid systems.”
The research team is now planning to collaborate with clinical researchers to study these brain circuits in humans, with the hope of someday developing new, targeted treatments for maladaptive fear responses and anxiety disorders.
Harnessing the power of preventative care and incentivised wellness to lessen the burden and cost of disease in South Africa.
By Damian McHugh, Chief Marketing Officer, Momentum Health.
South Africa is at a critical juncture in its healthcare landscape. The burden of disease -primarily driven by non-communicable diseases (NCDs) such as diabetes, hypertension, and mental health disorders – has escalated alarmingly. Over the past two years, NCDs have increased from 51% in 2022 to 55% in 2024, with diabetes rising by 12% and hypertension increasing from 8% to 10%1. Not only straining our healthcare system but also substantially hampering economic productivity and growth.
Current State of our Nation’s Health
It’s estimated that poor health-related absenteeism costs the South African economy up to R19.1 billion annually2. Beyond these direct financial implications, this hidden drain stifles business growth, reduces workforce efficiency, and hinders overall economic progress. Lifestyle-related diseases contribute significantly to rising healthcare costs – with an estimated R270 billion in healthcare claims projected to be linked to preventable conditions in 20253.
However, we have an opportunity to reverse this trend by embracing preventative care and incentivised wellness- two powerful levers that can help shift our healthcare paradigm from sick care to proactive disease prevention.
Why Prevention Is the Key to a Healthier, Wealthier Nation
I’ve always believed in the notion that your health is your wealth. Preventative healthcare is no doubt one of the most effective ways to reduce the burden and cost of disease. Simple lifestyle changes, such as regular exercise, balanced nutrition, deeper connections with loved ones, routine screenings to know one’s numbers, and effective stress management – have all been proven to dramatically lower the risk of chronic conditions. Yet, despite these clear benefits, many South Africans struggle to prioritise their health due to financial constraints, limited access to wellness education, and the ever-evolving demands of daily life.
This is where the private healthcare sector, in collaboration with policymakers and employers, can make a significant impact. By incentivising wellness behaviours, we can empower citizens to take control of their health while alleviating the financial burden on our healthcare system.
The Power of Incentivised Wellness
At Momentum Health, we have witnessed firsthand the positive outcomes driven by wellness rewards programmes. By rewarding members for engaging in preventative health activities—such as completing health screenings, maintaining an active lifestyle, or adopting healthier eating habits, we foster sustainable behaviour change through our wellness rewards programme, Momentum Multiply.
When effectively designed, these programmes offer tangible benefits such as lower healthcare costs through a rewards system and encourage healthier lives that rely less on medical intervention in the first place. There is sound evidence that ahealthier population results in fewer medical claims and lower insurance premiums, benefiting both individuals and employers.
It can also be linked to increased productivity as healthy bodies host healthy minds. We have seen that employees who proactively manage their health take fewer sick days, leading to enhanced workplace performance and reduced absenteeism. As a result, these factors contribute immensely to stronger economic growth asa healthier workforce contributes to improved business efficiency and a more resilient economy. However, to fully realise the potential of preventative care and incentivised wellness, we cannot do it alone. It’s pivotal that we adopt a multi-stakeholder approach.
Stronger and healthier together
A collaborative approach where healthcare insurers & providers expand access to preventative screenings, personalised health coaching, and digital health solutions that track and reward healthy habits and behaviour. Where employers adopt and implement workplace wellness programs that encourage employees to prioritise their health through corporate wellness incentives and adequate mental health support.
Where we, the private sector, work alongside Government & Policymakers strengthen the current system, build capacity for future skills andimplement national awareness campaigns to showcase the importance of preventative care.
As it stands, in 2024 the Gauteng Department of Health (GDoH) set aside R38.1 million in 2024/25 financial year and R119.7 million over the MTEF allocated for health and wellness campaigns, as well as physical activity programmes in prioritised areas such as Townships, Informal Settlement and Hostels and more recently, the GDoH announced a budget of R474.6 million in 2024/25 and R1.4 billion over the MTEF allocated for strengthening mental healthcare services. But ever more importantly, we also need every day South Africans to take proactive steps to manage their health by making better choices in the lives they live.
A Shared Responsibility for a Healthier Future
The numbers are clear. If we don’t act now, the cost of preventable diseases will only continue to rise – jeopardising both the sustainability of our healthcare system and economic stability. By harnessing the power of preventative care and incentivised wellness, we can significantly reduce the burden of disease, improve quality of life, and foster a healthier, more productive South Africa.
We remain committed to leading this change by innovating healthcare solutions that empower South Africans to take charge of their health and provide more health to more South Africans for less when they need it. Together, through collective action and a preventative mindset, we can and must build a healthier nation – one choice at a time.
Recent media reports over the future of NHI have been contradictory and hard to make sense of. Spotlight chased up those in a position to know where things stand – it seems the ANC has not in fact made any major concessions on NHI. There is however agreement that medical schemes won’t be phased out in the next few years, something that likely wouldn’t have happened in any case given the poor state of the economy and the long timeline for NHI implementation.
The ANC is holding firm on the NHI Act with Health Minister Dr Aaron Motsoaledi and the National Health Department “unaware of any compromise deals”, and the President’s office saying engagement with Business Unity SA (BUSA) is “ongoing”.
In spite of recent media reports to the contrary, neither President Cyril Ramaphosa nor Motsoaledi have conceded to any BUSA proposals on amending sections of the NHI Act. BUSA is the country’s apex business association and represents the banking, mining, and retail sectors, including the Health Funders Association, the Hospital Association of South Africa, and the Innovative Pharmaceuticals Association of South Africa.
BUSA, and several other critics of the Act, have argued that provisions should be removed that prohibit medical schemes from covering any health services covered by the NHI fund. The NHI Act has not yet been promulgated. If promulgated in its current form, the role of medical schemes will be dramatically reduced.
The DA’s spokesperson on health, Michele Clarke, told Spotlight that at the establishment of the recent GNU-convened Medium Term Development Plan (MTDP), agreement was reached that the health department would “not de-establish medical aids during the current government’s term of office”.
Spotlight understands that this amounts to a commitment not to promulgate the relevant sections of the Act in the next few years – it does not amount to a commitment to remove those sections from the act.
This is a pyrrhic victory, given that the implementation of NHI was always going to be a long-term project and that even in the most pro-NHI scenarios, the effective phasing out of medical schemes in the next few years was highly unlikely. There are also four legal challenges being brought on procedural and constitutional grounds that may further delay things.
Mist of confusion
Last week’s mist of confusion lifted when both the Presidency and Dr Stavros Nicolaou, speaking to Spotlight on behalf of BUSA, said no concessions have been made on NHI. Motsoaledi’s office also flatly denied reports that there had been any ANC or GNU compromise to remove parts of the NHI legislation that would render medical aids almost obsolete. The Spokesperson for the National Department of Health, Foster Mohale, added that he was unaware of any MTDP agreement on medical aids.
Vincent Magwenya, a spokesperson for the president, told Spotlight he was “unaware of any process leading to the amendment of the NHI Act”, claiming that Maropene Ramokgopa, Minister in the Presidency responsible for Planning, Monitoring and Evaluation, was misquoted last week.
She was quoted in news reports as saying the ANC and the DA had reached an “unofficial understanding on the NHI” following an ANC compromise to remove parts of the NHI legislation that would collapse medical aids. “Ms Ramokgopa tells me she was misreported,” said Magwenya.
Chris Laubscher, the DA’s communications head, told Spotlight: “There was never confirmation by [DA leader who is also Minister of Agriculture] John Steenhuisen that the NHI in its entirety had been excluded from the government’s Medium Term Development Plan.”
The new MTDP has not yet been made public.
Charity Ophelia McCord, the spokesperson for Steenhuisen, said the MTDP had yet to be completed and passed, but was on the Cabinet agenda for Wednesday, February 12. Spotlight was not able to verify if this was discussed.
Meanwhile, Mohale said both the health department and the minister were unaware of any compromise deal, “thus the implementation of the NHI Act continues as per the plans”.
Cannot be changed over night
If at some point the NHI Act is to be amended, the process is likely to take several years, according to Professor Olive Shisana, Social Policy Special Advisor to Ramaphosa on the NHI and health systems strengthening.
“Any process for changing an enacted law normally goes through Parliament, including an amendment from the executive,” Shisana explained. “There would first have to be consultation with the public before it even got to Parliament. Then, when it gets to Parliament there’s more consultation, this time in each of the provincial legislatures, after which it goes to the Portfolio Committee on Health which also takes written submissions. The committee then decides whether to submit it to the National Assembly. If the National Assembly passes it, it goes to the National Council of Provinces which considers each province’s input. Government took five years to get this NHI Act in place, so you can imagine it might take about as long to get parts of it excised or reversed. That’s the normal route it would have to take, I’m afraid.”
However, both the DA and BUSA are adamant that the Act needs to be changed.
Clarke said the DA remained of the view that “multiple parts of the [Act] remain problematic and dangerous for the future of healthcare in South Africa”.
She added: “The DA wants the model underpinning the NHI to be completely reworked and multiple problematic clauses amended by Parliament to ensure that the healthcare model is protected and strengthened.”
BUSA met with Ramaphosa in September last year and tabled a proposal which included striking Section 33 – which effectively collapses private medical aids as they now exist, creating a single national fund – from the NHI Act. It also calls for the implementation of mandatory health insurance which it is argued will take pressure off the public health system and bolster existing medical aids. The president has since passed it on to Motsoaledi’s office.
Neither BUSA nor the responding government parties have given any indication of when they might next meet or pronounce on the proposal.
Rejection of NHI
Meanwhile, the United Healthcare Access Coalition (UHAC), a grouping claiming to represent 80% of all private healthcare stakeholders, lodged a detailed alternative proposal with the president’s office. This entirely rejects the NHI and focuses on rehabilitating the healthcare system based on a synthesis of far-reaching recommendations which various commissions and experts have made over several decades, including the Taylor Commission and the more recent Health Market Inquiry (HMI).
In January this year, Motsoaledi promised to pronounce on the implementation of the HMI recommendations from 2019 “within weeks”. As reported by Business Day, there indeed seems to now finally be some movement on the HMI recommendations with Minister of Trade Industry and Competition Parks Tau having gazetted an exemption that newly opens the door for tariff setting in the private health sector – a move that may help rein in runaway healthcare costs.
UHAC spokesperson Dr Aslam Dasoo described their report as “everything that the NHI is not”.
“Our health pathway requires easy legislative changes and is within current fiscal constraints. We can start the process immediately. It requires a change in governance structure of the provincial health systems where politicians relinquish all direct authority over health care institutions and instead focus on strategic policy,” he previously told Spotlight.
In an online briefing launching the UHAC on Wednesday, February 12, Dasoo warned all parties in the GNU to “consider their options” as they would be “held jointly responsible” should the NHI be implemented to the detriment of South Africa.
Another UHAC executive member and CEO of the SA Private Practitioners Forum, Dr Simon Strachan, said the focus of their universal healthcare plan was on providing equitable, implementable, and sustainable healthcare.
“We need to ensure that those who can look after themselves, do (financially), while subsidising those who cannot afford to. It’s one hundred percent dependent on improving health service delivery within the public sector and creating a competitive market for people to decide where and how they access healthcare,” he said.
The UHAC coalition includes NGO’s, patient advocacy groups, the SA Medical Association, the South African Private Practitioners Forum, and the Progressive Healthcare Forum.
Asked what UHAC’s “Plan B” was if they “hit a brick wall” on their detailed proposals, Dasoo said the GNU was obliged to respond to such a widely representative proposal “otherwise they’re not fit to govern”.
Referring to the ANC, he said the party “neglected the two major healthcare systems, allowing real degradation of the public sector and an unregulated private sector with no market growth, resulting in prices going up”. He added: “If there’s any brick wall, it’s the one they’ve built.”
New postpartum depression research from the School of Medicine and Weill Cornell Medicine could lead to a blood test to identify women at risk and possibly even to a preventive treatment.
The research, published in Neuroposychopharmacology, suggests that pregnant women may have characteristic levels of certain molecules in their blood that can warn that they are at risk of developing postpartum depression (PPD). These molecules, called neuroactive steroids, are derived from progesterone.
Measuring those molecules via a simple blood test could let doctors get women treatment for PPD sooner – possibly even before symptoms appear, the researchers say. “Studying postpartum depression gives us a way to identify biological changes that occur before someone becomes depressed because the timing of postpartum depression is predictable,” said researcher Jennifer Payne, MD, an expert in reproductive psychiatry at UVA Health and the University of Virginia School of Medicine.
Understanding Postpartum Depression
Postpartum depression affects 10% to 15% of new moms.
“Postpartum is the only time in people’s lifespans when we know there is a biological trigger which guarantees that a certain percentage of people will become ill,” said Weill Cornell’s Lauren Osborne, MD, who co-led the study with Payne. “If we can untangle this biology and find predictors for it, not only will we be helping women, but it may give us a step up in trying to find predictors for other psychiatric illnesses also.”
It’s unclear why some women develop postpartum depression, but the new findings suggest that an imbalance in the body’s metabolism of progesterone may be a factor.
About the Study
To better understand the role of progesterone, the researchers focused on the hormone and on its “metabolic pathway” in the body. The scientists measured levels of neuroactive steroids derived from progesterone in the blood of 136 women during their second and third trimesters. Of these, 33 went on to develop postpartum depression after giving birth.
Two neuroactive steroids seem to affect the risk of developing PPD – pregnanolone and isoallopregnanolone. Pregnanolone acts on a particular cellular receptor to reduce stress. Isoallopregnanolone, on the other hand, acts on the same receptor to increase stress.
In the third trimester, women who went on to develop PPD had a lower pregnanolone/progesterone ratio and a higher isoallopregnanolone/pregnanolone ratio compared with those who did not, the researchers found. Elevated progesterone levels in late pregnancy were also associated with a higher risk of PPD.
Next Steps
The researchers plan to attempt to replicate their results in a larger, more diverse group of women in hopes of developing a clinical test to predict the risk of PPD. Further, they say their work could lead to a preventive treatment – possibly one of two prescription drugs, brexanolone and zuranolone, already available to treat PPD.
“We don’t know if these drugs would work as a preventive measure for people who are at risk of developing postpartum depression, but based on our findings, they have the potential to prevent [its] development,” Osborne said.
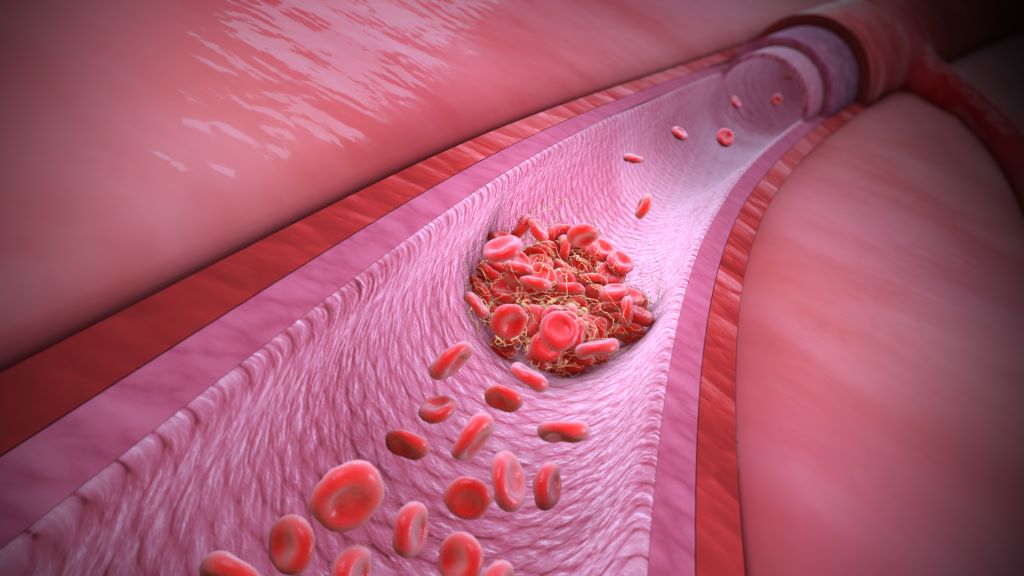
Researchers at McMaster University have made a groundbreaking discovery in the field of haematology, providing an explanation for spontaneous and unusual blood-clotting that continues to occur despite treatment with full-dose blood thinners.
The discovery, published in The New England Journal of Medicine, is expected to influence how doctors test for, and treat patients with, unusual or recurrent blood clotting, with the potential to improve patient outcomes.
Researchers found this new blood clotting disorder to have certain similarities to vaccine-induced immune thrombocytopenia and thrombosis (VITT) – a rare but aggressive clotting disorder that was caused by certain discontinued COVID-19 vaccines.
The research reveals that certain patients can develop severe blood clotting due to antibodies that closely resemble those that cause VITT, even in the absence of known triggers for such antibodies, such as blood thinners (heparin) or prior vaccination.
The newly identified disorder has been termed VITT-like monoclonal gammopathy of thrombotic significance (MGTS).
“Our study highlights the importance of recognising and diagnosing this new blood-clotting disorder,” said Theodore (Ted) Warkentin, co-first author and corresponding author of the study and professor emeritus in the Department of Pathology & Molecular Medicine at McMaster University.
“By understanding how to diagnose VITT-like MGTS, we can develop more effective treatment strategies that go beyond traditional anticoagulation,” said Warkentin, a hematologist in the Department of Medicine based at Hamilton Health Sciences’ Hamilton General Hospital.
Specialized testing was conducted at the McMaster Platelet Immunology Laboratory within the Michael G. DeGroote Centre for Transfusion Research, the only laboratory in Canada with the full repertoire of testing required to characterize the VITT-like antibodies that target the PF4 protein. Researchers performed a detailed analysis of cases exhibiting unusual blood-clotting despite patients being on full-dose blood thinners, focusing on those patients who had unexplained VITT-like antibodies that were detectable for a year or more.
The analyses identified the presence of M (monoclonal) proteins (which typically indicate plasma cell disorders), and together with the persisting VITT-like reactivities over at least 12 months (which is highly unusual for most anti-PF4 antibodies), thus pointing to an ongoing pathological process rather than a short-term anomaly.
The study included a multinational collaboration, with data collected from five patients treated at institutions in Canada, New Zealand, France, Spain, and Germany.
Collaborator Jing Jing Wang of Flinders University in Australia played a crucial role in proving for each patient that the M proteins are the pathological VITT-like antibodies. Collaborator Andreas Greinacher of Greifswald University in Germany helped in identifying similar cases in his anti-PF4 reference lab.
“The findings of this study underscore our ability to leverage fundamental molecular and biochemical science to unravel disease mechanisms,” said Ishac Nazy, co-lead author of the study and scientific director of the McMaster Platelet Immunology Laboratory and co-director of the Michael G. DeGroote Centre for Transfusion Medicine.
“This approach enables precise patient diagnosis and informs timely treatment strategies, even for previously unidentified diseases, exemplifying true bench-to-bedside translational medicine,” said Nazy, associate professor in the Department of Medicine at McMaster.
A remarkable observation was that each of the patients had failed blood thinning treatment, but they showed some benefit with unusual treatments, such as high-dose intravenous immunoglobulin (IVIG), Bruton tyrosine kinase inhibitors (ibrutinib), and plasma cell–targeted myeloma therapy. The existence of this novel blood clotting disorder has important implications for how health care providers will evaluate patients who develop unusual or difficult to treat blood clots in the future.
The American Academy of Neurology (AAN) has developed a new systematic review to summarise for neurologists and other clinicians the evidence for epidural steroid injections and whether they reduce pain and disability for people with certain kinds of chronic back pain. The systematic review is published online in Neurology®.
It updates a 2007 assessment by the AAN. With an epidural steroid injection, a steroid or corticosteroid medication is injected into the epidural space with the aim of helping reduce certain kinds of back pain.
“Chronic back pain is common and can negatively impact a person’s quality of life, making it difficult to move, sleep and participate in daily activities,” said author Carmel Armon, MD, of Loma Linda University School of Medicine in California and a Fellow of the American Academy of Neurology. “In our review, studies show epidural steroid injections may have limited efficacy. They may modestly reduce pain in some situations for up to three months and reduce disability for some people for up to six months or more.”
For the review, researchers analysed all available studies over a 16-year period. A total of 90 studies were examined. The review focused on the use of epidural steroid injections to reduce pain for people with radiculopathy and spinal stenosis. Radiculopathy is a condition caused by a pinched nerve in your spine. Spinal stenosis is a condition where spinal cord or nerves have become compressed because the space around the spinal cord has become too small. For people with radiculopathy, the review says studies show epidural steroid injections may be effective at modestly reducing pain and disability for up to three months after the procedure.
When compared to people not receiving the treatment, 24% more people receiving the treatment reported reduced pain, and 16% more reported reduced disability for up to 3 months. The treatment may also reduce disability for up to six months or more, with 11% more of those treated reporting reduced disability. Most of the reviewed studies looked at people with radiculopathy in their lower backs, so it is unclear how effective the treatment is for those with radiculopathy in their necks. For people with spinal stenosis, studies show epidural steroid injections might modestly reduce disability for up to six months or more after the procedure.
When compared to people not receiving the treatment, 26% more people receiving the treatment reported reduced disability up to three months, and 12% more for up to six months or more. The treatment was not found to reduce pain for up to three months. All studies looked at people with stenosis in their lower backs, so researchers do not know how effective the treatment is for people with stenosis in their necks.
“Our review affirms the limited effectiveness of epidural steroid injections in the short term for some forms of chronic back pain,” said author Pushpa Narayanaswami, MD, of Beth Israel Deaconess Medical Center in Boston and a Fellow of the American Academy of Neurology. “We found no studies looking at whether repeated treatments are effective or examining the effect of treatment on daily living and returning to work. Future studies should address these gaps.”
In a new JAMA Dermatology study, scientists at King’s found that changes in two parts of the genome work together to influence alopecia risk.
Frontal fibrosing alopecia (FFA) is a highly distressing dermatological disorder which is associated with inflammation, scarring and irreversible hair loss. The disease affects an increasing number of patients worldwide and is caused by genetic and environmental factors.
The study authors conducted a meta-analysis of four cohorts of women with FFA across the UK and Europe. When looking into a cluster of immune genes known as the major histocompatibility complex, which help immune systems recognise foreign substances, they identified specific genetic differences that interact with ERAP1 and increase the risk of developing FFA.
This gene-gene interaction is a rare phenomenon in human genetics, known as “epistasis”. This means that the risk associated with one gene is modified by another gene. Different versions of the two genes involved in this interaction have been observed in some other autoimmune diseases, including psoriasis and ankylosing spondylitis.
Previous research has identified that genetic variants in the ERAP1 and ERAP2 genes were associated with survival of the Black Death, a bubonic plague which swept through Europe in the mid-1300s. Such genetic variants, which are associated with protection from infection, may also make people more prone to certain immune conditions. This new study demonstrates that this is the case for FFA.
“Our study is the largest ever genome-wide association study into frontal fibrosing alopecia (FFA), an inflammatory and scarring condition affecting almost exclusively women,” said Dr Christos Tziotzios, Senior Lecturer of the St John’s Institute of Dermatology at King’s and Consultant Dermatologist at Guy’s and St Thomas’ NHS Foundation Trust
He added: “Since the disease was described in 1994, the number of people affected has increased dramatically. Our newest finding sheds more light into the autoimmune basis of the condition and provides direction for further research into drug development.”
As well as improving our understanding of the genetic factors that drive FFA, the authors hope that these findings can be applied to predict risk of its development while paving the way for new treatments.
The team of scientists are now investigating the prospect of predictive genetic test for FFA risk, while exploring the potential of targeting ERAP1 with highly specific drugs as a new way of treating this condition.
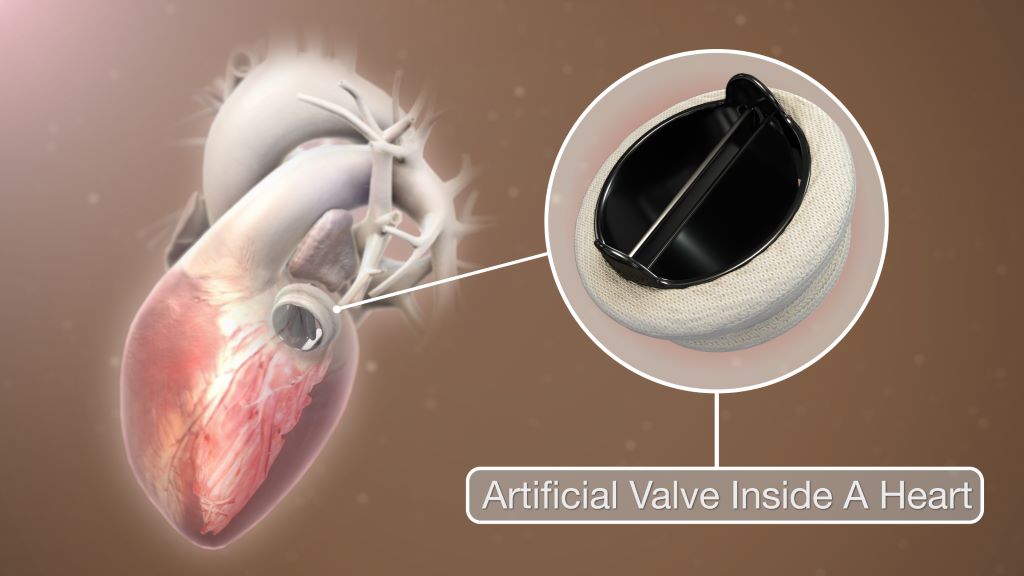
Patients aged between 50 to 70 years with a mechanical heart valve replacement had better long-term survival compared to those with a biological valve, new research led by the University of Bristol has found. The study is published in the European Journal of Cardio-Thoracic Surgery.
The last two decades have seen an increase in the use of biological over mechanical heart valve replacements. However, while short-term clinical outcomes are known to be the same, long-term outcomes are still under debate.
Existing guidelines support the use of mechanical valves made of synthetic materials in patients below the age of 50, while biological valves made of animal tissue are favoured for those above the age of 65 or 70. The guidelines leave the choice to the decision of surgeons and patients who are 50 to 70 years old.
The research team wanted to find out the clinical outcomes for patients aged between 50 to 70 years undergoing elective and urgent heart valve replacement at the Bristol Heart Institute (BHI) over a 27 year period [1996 to 2023].
The researchers also sought to investigate trends, early outcomes and long-term survival rates, the incidence of repeat valve interventions and patient prosthesis mismatch (PPM).
A total of 1708 (61% male) patients with an average age of 63 years were included with 1191 (69.7%) receiving a biological valve replacement.
The research found there were no short-term differences when comparing patients receiving biological and mechanical valves. However, patients who received mechanical valves had better long-term survival up to 13 years after having surgery.
Patients with a size 19mm biological valve replacement (a fairly small valve commonly used in females) had the worse long-term survival. Patients with a size 21mm mechanical valve had better survival compared to both size 19 and 21mm biological valves. The study confirmed that severe PPM is a significant risk factor for poor long-term survival.
Gianni Angelini, BHF Professor of Cardiac Surgery at the Bristol Medical School: Translational Health Sciences (THS), Director of the Bristol Heart Institute and corresponding author, said: “Our study has implications for decision-making in surgical heart valve replacements for patients aged between 50 and 70 years old. The evidence supporting better long-term survival in patients receiving a mechanical heart valve suggests the current trend favouring biological valves in this age bracket should be urgently reconsidered. The survival benefit is especially clear in smaller sized valves.”
The research team recommends the evaluation of the long-term benefits associated with mechanical valves, especially in smaller sizes, despite long-term blood thinners not being needed with biological valves.
Study limitations
The single-institution design, retrospective collection of data, and absence of randomisation make the study open to bias. The lack of echocardiographic information could potentially underestimate the incidence of structural valve failure. In terms of repeat valve interventions, only patients who underwent re-do surgical aortic valve replacement or valve in valve transcatheter aortic valve implantation (TAVI) at the BHI were included.
As the BHI is a supra-regional centre, it is very unlikely that many patients might have undergone reintervention in other institutions. The cause of death (cardiovascular/non cardiovascular) was not available.
South Africa’s National Department of Health is still to outline a clear contingency plan as a United States (US) funding freeze puts lives at risk, spells job losses, and presents threats to keeping HIV and TB under control.
The ripple effects of US President Donald Trump’s 90-day freeze of funding on foreign aid programmes have hit South Africa hard. The damage is being counted at multiple levels – even as some limited funding flows are being restored.
For the country, the fallout has heightened civil society’s calls for a prompt, implementable plan to fill the gaps in care and services. Also needed, they say, is clarity on longer-term strategies for greater self-sufficiency in the country’s HIV responses as donor-funded models look increasingly precarious. Such an argument for increased independence in Africa and the global south was made by president of the South African Medical Research Council (SAMRC), Professor Ntobeko Ntusi, writing in the journal Nature.
South Africa should have been better prepared and not caught off guard to be left in the position it now finds itself in, some beneficiaries of US-funded projects told Spotlight. They were speaking on condition of anonymity, given the risk of public comments jeopardising their prospects of having their funding restored.
The immediate need is to ensure that the country’s overburdened and under-resourced public clinic system is able to absorb the tens of thousands of people living with HIV who will have to use public facilities. This is partly because the NGOs they have relied on have been forced to close shop – virtually overnight. Clinics catering to specific groups, such as men who have sex with men, have been particularly hard hit.
South Africa is the largest global recipient of President’s Emergency Plan for Aids Relief (PEPFAR) funds. These funds make its way to South Africa through the United States Agency for International Development (USAID) and the Centers for Disease Control and Prevention (CDC). Through PEPFAR, USAID has been funding and supporting local NGOs and our Department of Health for around two decades. According to USAID’s website, it invested $5.6 billion (roughly R100 billion at the current rand/dollar exchange rate) between 2004 and 2020 towards prevention and treatment of HIV and TB in South Africa.
Trump’s initial executive order, signed on 20 January, halted funding received via USAID. USAID is an agency of the US government that now falls under the State Department under the leadership of Secretary of State Marco Rubio. Since taking office, Trump has slated USAID as “corrupt” and run by “radical left lunatics”.
The Washington head offices of USAID were closed on Friday 7 February as per Trump’s orders and even as the 90-day review period had just got underway, signage on the building was being removed or taped over. Trump’s actions have now been challenged in courts with successful temporary blocks to his orders to place 2 200 USAID workers in the US on paid leave and to reinstate 500 US-based staff who were already placed on administrative leave from when the order was first signed. The situation is highly fluid and several court actions remain in progress.
Some limited relief
In South Africa, NGOs that received USAID funding remain largely in limbo. Although the United States mission in South Africa confirmed that some PEPFAR-funded services could continue in the country, it is subject to some relatively strict limitations and with no assurances of longer term support. As is clear from reporting by Bhekisisa, the process to get at least some funding to flow again to PEPFAR-supported projects is not straight forward.
There was some good news this week linked to PEPFAR-funding channelled through the CDC – a US federal agency under the Department of Health and Human Services. Following a court order, organisations getting these funds should for now be able to continue their work. However, the court process is far from over and the future prospects of NGOs that depend on CDC funds remains precarious.
Given these ongoing uncertainties and severe disruptions to cash flows, Spotlight understands that some large NGOs may have to close down, while others may have to drastically reduce their services. As reported by Spotlight and GroundUp, several NGOs have appealed to the private sector for assistance. As it stands, thousands of people employed or contracted by local NGOs face the loss of their jobs, cut-backs and deepening anxiety over income security. These people include community health workers, peer counsellors, patient navigators, community activists and advocates, support and administrative staff members, and contract workers who keep these organisations functioning.
At stake too are specialised services for so-called key populations such as sex workers, men who have sex with men, the LGBTQI+ community, and people who use drugs. Until recently, a focus on improving services for key populations was generally accepted, including by PEPFAR, to be the right strategy given the disproportionate risk of HIV infection in these groups. But under the Trump administration’s “anti-woke” agenda, it seems likely that many services aimed at key populations are set to be defunded.
A White House media note on 29 January made clear the US’s stance: “The previously announced 90-day pause and review of U.S. foreign aid is already paying dividends to our country and our people. We are rooting out waste. We are blocking woke programs. And we are exposing activities that run contrary to our national interests. None of this would be possible if these programs remained on autopilot.”
A timeline of the US aid cuts
20 January
90-day pause
In an executive order, US President Donald Trump orders a 90-day pause in US foreign development for “assessment of programmatic efficiencies and consistency with United States foreign policy”.
26 January
USAID funding paused
US Secretary of State Marco Rubio pauses all US foreign assistance funded by or through the State Department and US Agency for International Development (USAID) for review.
28 January
Waiver issued
Subject to certain conditions, Rubio issues a waiver stating: “Implementers of existing life-saving humanitarian assistance programs should continue or resume work if they have stopped.”
1 February
Waiver clarified
The extent of the January 28 waiver is clarified in a memo from the US Department of State.
5 February
Health portfolio committee briefing
South Africa’s Health Minister Dr Aaron Motsoaledi briefs Parliament on the US funding cuts and their impact on healthcare services.
7 February
South Africa singled out
In an executive order applying only to South Africa, Trump orders that “the United States shall not provide aid or assistance to South Africa”.
10 February
Waiver still applies
The US mission in South Africa releases an FAQ in which they state that PEPFAR activities that fall under the limited waiver will resume despite the February 7 executive order.
12 February
CDC grants reinstated
The grants of NGOs receiving support through the CDC are reinstated following a court order issued in a US court.
Crisis of fear, silence, and uncertainty
Spotlight understands that staff of affected NGOs have essentially been forbidden from speaking publicly about the 90-day funding freeze. Many declined to speak on the record to Spotlight, even anonymously – too afraid it might affect the decision on their funding after the 90-day review period.
According to an FAQ by the US mission in South Africa that was published on February 10, they have been communicating with the South African government, though it is not clear when this happened. Five days earlier on 5 February, Health Minister Dr Aaron Motsoaledi told Parliament’s Portfolio Committee that he had not had any official communication from the US government on the matter.
Figures from Motsoaledi’s presentation showed that in 2023/2024, PEPFAR funding to South Africa’s health department amounted to 17% of its spending on HIV. Funding totals R4.6 billion for staffing and R2.9 billion for running costs for NGOs. These NGOs include organisations working directly with people living with HIV, mobile units and youth organisations and programmes. PEPFAR focuses on the 27 districts in South Africa with the highest disease burden.
The health department did not respond to Spotlight’s questions on contingencies, or details of next steps to fill the funding gaps or how capacity and resources will be redirected to avert catastrophe. Motsoaledi did not give any of these details in his presentation to Parliament either.
What he did say was that since Trump’s executive order came into place, the health department had hosted a meeting with the provincial leads on HIV and TB; conducted assessments on the immediate impacts of the executive order; met with people living with HIV and engaged with SANAC to finalise a sustainability framework.
A collective of activist organisations, including the Health Justice Initiative, SECTION27, the Cancer Alliance, Treatment Action Campaign, Sweat, PSAM and the African Alliance, have pressed the Department of Health to create an “urgent co-ordinated emergency plan” along with an increased budget to avert a looming disaster.
The activists highlighted that despite the announcement by the Trump administration that some NGOs could apply for a waiver, many have had no practical way to do so without ways to communicate with their USAID contacts. This as USAID employees were placed under a work stop order and were shut out of their offices and denied access to their work emails.
The appeal from the collective also extends to protecting the work of academic and clinical research in the fields of HIV, TB, and cervical cancer that will also be affected by the funding freeze. As Spotlight reported, around 28% of the South African Medical Research Council’s budget for 2025/2026 was set to come from the United States government.
An ‘unreal world’
Professor Linda-Gail Bekker, chief executive officer at the Desmond Tutu Health Foundation, said Trump’s actions put in jeopardy the goal to finally have epidemic control of HIV – and right at the final hurdles.
“We have made amazing progress. And thank you to PEPFAR that helped us to get this far, but the work is not over. For the US to pull out at this point is a massive loss of investment; it’s also regression. It’s like getting to the end of a book but having the last chapters torn out before you can read it,” said Bekker.
She said PEPFAR funding has made it possible to build a formidable cohort of lay and professional people trained and dedicated to their roles that supported public healthcare in the most critical ways.
“These are individuals who distribute antiretrovirals, distribute pre-exposure prophylaxis, find and trace individuals who’ve been lost to care. They take services into communities, to outside of the health facilities, and made the effort to go the last mile to find those individuals – that is how you close down the epidemic,” Bekker said.
Her caution too is that loosening a grip on HIV control means potential surges in tuberculosis. “HIV and TB track together all the time, and an HIV epidemic that is once again out of control, almost certainly means what will follow is a TB epidemic that is out of control,” Bekker said.
Trump has created an “unreal world”, said Dr Andy Gray of the University of KwaZulu-Natal, who has also worked with the World Health Organization (WHO) in various capacities over two decades. “People are being held to ransom; and people are scared.”
“We have always been used to the oscillation between the United States’ Republican and Democratic administrations; things may be a little uncomfortable or there may be some disruption, but not this ‘let’s burn down the house’ approach taken by the Trump administration,” he said.
“There is no consideration of human rights or for human beings anywhere in the world, including America,” he added, pointing out too that the CDC has for the first time in 60 years been instructed to cease publishing weekly mortality and morbidity data, despite a breakout of avian flu (H5) in the country.
For Gray, South Africa’s strategic health response in the wake of this crisis should be to shift from a donor-funded model. His concern, however, is that with a stretched South African purse and with competing priorities, the HIV response will slip down the list.
Gray said that better self-sufficiency comes from eliminating waste, investing in employing the right people in the right jobs as well as investing in efficient systems.
He added that National Treasury will have to redirect money for the interim shortfall left by the US funding freeze, and provinces will have to step up by getting their houses in order.
South Africa, he warned, should ready itself for the “worst case scenario” once the 90-day review period is up.
SANAC response
The South African National AIDS Council (SANAC) role is meant to bring together government, civil society and the private sector to create a collective response to HIV, TB and STIs in South Africa. But if there is a crisis strategy from the council, it has not yet been announced.
SANAC head of communications, Nelson Dlamini, said that they have been left in a position of not being able to engage publicly because they haven’t had any direct communication with PEPFAR’s and USAID representatives based in Pretoria.
“PEPFAR is a government-to-government agreement and there ought to be official communication with the government of South Africa so we know what this means for our working relationship, but nothing has been forthcoming,” said Dlamini. “SANAC is a co-ordinator so we have to still coordinate. We are engaging in the background with relevant structures but we can’t say we are doing X, Y, Z till we have a sit down with PEPFAR,” he said.
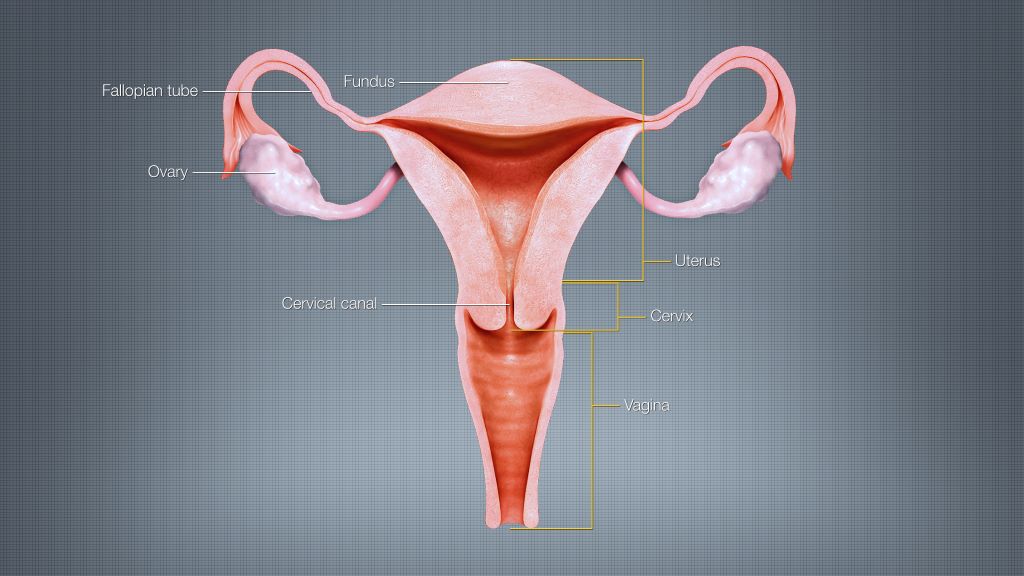
In a randomised clinical trial, researchers from Huntsman Cancer Institute at the University of Utah (the U) have found that short-course, higher dose vaginal brachytherapy for endometrial cancer had similar effectiveness to more frequent, lower dose sessions.
Gita Suneja, MD, MS, physician-scientist at Huntsman Cancer Institute and professor of radiation oncology at the U, is the first author of the SAVE trial report – which stands for, Short-Course Adjuvant Vaginal Cuff Brachytherapy in Early Endometrial Cancer Compared with Standard of Care.
“There isn’t high quality-data on optimal dose and schedule for brachytherapy treatments. Because of this, practice patterns really vary,” says Suneja. “The SAVE trial sought to try to lower the number of treatments that patients were receiving but maintain short-term quality of life and disease control.”
Endometrial cancer is a disease that begins in the lining of the uterus. The primary treatment for endometrial cancer is surgery, including the removal of the uterus, cervix, and upper vagina. Brachytherapy, a form of internal radiation, is used as a secondary treatment to prevent the cancer’s return. Patients receiving vaginal cuff brachytherapy are treated with internal radiation by way of an applicator in the vaginal cavity.
The SAVE trial compared two groups who received different treatment doses over a varying number of sessions. The control group received the standard treatment – between three to five appointments with lower doses. The experimental group received higher doses of radiation in just two sessions.
“The study outcomes will help improve cancer care for Huntsman Cancer Institute patients across the five states of the Mountain West.”
Gita Suneja, MD, MS
The researchers found similarly effective short-term outcomes and few acute toxicities for the patients in the experimental group.
David Gaffney, MD, PhD, FACR, FABS, FASTRO, physician-scientist at Huntsman Cancer Institute and professor of radiation oncology at the U, developed the idea for the SAVE study after seeing patient need. According to the American Cancer Society, endometrial cancer is the most common cancer of the female reproductive organs. Incidence is on the rise, as is the mortality rate.
“It is a big win when we can preserve good outcomes and make cancer care easier,” says Gaffney.