An international clinical trial has found three new safe and effective drug regimens for tuberculosis that is resistant to rifampin, the most effective of the first-line antibiotics used to treat TB. The research, published in the New England Journal of Medicine, was led by researchers at Harvard Medical School and other members of the endTB project.
The newly identified regimens take advantage of recently discovered drugs to expand the treatment arsenal and give physicians new ways to shorten and personalise treatment, minimise side effects, and treat patients using only pills instead of daily injections. They also offer alternatives in case of drug intolerance, medication shortages or unavailability, or drug resistance, the researchers said.
The endTB trial is one of four recent efforts to use randomised controlled trials to test new, shorter, less toxic regimens for drug-resistant TB. endTB uses two new drugs – bedaquiline and delamanid — which, when brought to market in 2012-2013, were the first new TB medicines developed in nearly 50 years.
To find shorter, injection-free drug combinations for people infected with TB resistant to rifampin, endTB tested five new, all-oral 9-month regimens using the two new drugs in combination with older medications.
A third drug, pretomanid, received emergency authorisation from the FDA for specific use within a regimen against highly drug-resistant TB in 2019, after the endTB clinical trial was underway, and is not included in the regimens used in these trials.
Trial regimens were considered effective if they performed at least as well as the control group, which received a well-performing standard of care composed in accordance with a stringent interpretation of World Health Organization (WHO) recommendations.
The three successful new regimens were successful for between 85 and 90% of patients, compared with 81% success for people in the control group. The control group was treated with longer treatments, which also included the recently discovered medicines.
The trial launched in 2017 and enrolled 754 patients across seven countries: Georgia, India, Kazakhstan, Lesotho, Pakistan, Peru, and South Africa. The goal was to improve treatment for patients with tuberculosis resistant to rifampin. The WHO estimates that some 410 000 people become sick with rifampin-resistant TB each year, including people who have multidrug-resistant TB (MDR-TB). Only 40% are diagnosed and treated, 65%of them successfully.
The study population included children as well as people infected with HIV or hepatitis C, both common in populations with high rates of TB. In another innovation, women who became pregnant while on treatment were included in the endTB trial. These groups are often excluded from clinical trials. In a special report published in August 2024, the WHO added the three noninferior regimens from the endTB trial to the list of treatment options for rifampin-resistant and multidrug-resistant TB (MDR-TB) treatment; the recommendations extend to these neglected groups as well as to pregnant women.
With recent efforts to end patent exclusivity on bedaquiline, two of the endTB regimens and the WHO-recommended pretomanid-containing regimen can all be purchased for less than $500, an access target set by activists more than 10 years ago, which has only just now been achieved. All of these innovations together mean the new shortened, all-oral regimens are available to more people than ever.
Photo by Pixabay: https://www.pexels.com/photo/view-of-operating-room-247786/
Increased use of ventilation and air cleaners, designed to mitigate the spread of viral infections in hospitals, is likely to have unpredictable effects and may cause viral particles to move around more, according to a new study from researchers at UCL and UCLH.
In the study, published in Aerosol Science & Technology, researchers investigated the effect of using built-in mechanical ventilation and portable air cleaners (PACs)1 upon the spread of airborne particles, which are similar to those breathed out by a person with a viral respiratory infection such as SARS-CoV-2 or influenza.
The team tracked the movement of airborne particles around a typical hospital outpatients’ clinic at UCLH in central London using an aerosol generator and particle counters2. A variety of scenarios were simulated, including particle movement to a neighbouring room, throughout the whole clinic, and from one room to another room at the far side of the clinic.
They also tested whether factors such as closing doors, or the position of ventilation and PACs within a room, had an effect on the spread of particles.
The researchers found that while use of built-in ventilation and PACs can reduce particle spread in some scenarios, in some experiments the use of PACs increased aerosol spread by up to 29% between neighbouring rooms. Built-in ventilation potentially increased aerosol migration across the clinic by up to 5.5 times more than if no ventilation was used.
Professor Laurence Lovat, senior author of the study from UCL Surgery & Interventional Science and UCLH, said: “The COVID-19 pandemic really highlighted the risk of picking up airborne viral infections in hospitals, which naturally led to efforts to reduce this risk. In many hospitals, the use of ventilation systems and portable air cleaners has increased.
“While the urgency of the situation demanded a rapid response, since then we’ve been studying precisely how viral particles move around in real spaces and have been surprised by what we’ve found.
“Putting air cleaners in rooms led to unexpected increases in the circulation of aerosols in some cases, but it took months to understand what we were seeing. Each scenario produced different, unexpected results, depending on the spaces and airflow sources involved.
“Even at UCLH, a modern hospital built less than 20 years ago, airflow patterns were not predictable. In older hospitals, which often have natural draughts, the situation would likely be even more complex.”
The study concluded that using airflow devices in hospitals to try to limit the movement of airborne pathogens requires careful consideration of airflow dynamics and device placement to reduce the risk of exacerbating the problem.
The clinic where the experiments took place consisted of a large central waiting room (154 m3,split into A and B for the purpose of the study), eight surrounding consulting rooms and a nurses’ station (all approximately 35 m3). The clinic was connected via a permanently open passageway to a corridor leading to the rest of the hospital. Experiments took place at night and weekends when no staff or patients were present.
A number of experiments were conducted by placing aerosol generators dispersing saline solution in certain rooms, with particle detectors sited in other rooms to track the movement of particles around the clinic.
In one experiment, the researchers simulated particle spread from a medical professional or patient in one consulting room to a neighbouring room. A baseline measurement was taken in the consulting room with the aerosol source when all doors were open and no ventilation or PACs were in use.
Closing the room door that contained the source was found to reduce particle spread significantly and closing both room doors reduced it by 97%.
But when doors were opened and large PACs in the adjacent waiting room were turned on, the spread to the neighbouring consulting room increased by 29%. When small desktop PACs were added to both consulting rooms and the nurses’ station, the spread was lower than the baseline, but only slightly.
Dr Jacob Salmonsmith, first author of the study and an Honorary Research Fellow from UCL Mechanical Engineering, said: “The results of this experiment might seem counterintuitive if you take the view that changing the air in a room more often reduces the spread of viral particles.
“While it’s true that air cleaners do remove viral particles from the air and can reduce overall spread, they can also have unintended consequences. In particular, this experiment suggests that larger air cleaners, which have larger exhaust vents that introduce their own air currents, can cause particles that haven’t been filtered out to spread further than they would have if the cleaner wasn’t there.
“In any given space you have complex interactions between many different air currents, such as ventilation, doors closing and people’s movement. Our findings indicate that the whole picture needs to be considered when choosing when and where to introduce air cleaners.”
In another experiment, the team observed highly complex patterns of particle spread when all consulting room doors were open.
This included one scenario where the highest concentrations of particles were detected in rooms furthest away from an aerosol source situated in a consulting room where a PAC was in operation. Particle levels in the room furthest from this aerosol source were 184% higher than average, while in the room directly opposite the source they were 68% below average.
There were also 247% more particles in the waiting room furthest away from the consulting room, where a PAC was in operation, than in the waiting room right next door to it. The nurses’ station had a higher concentration of particles than any room on the same side of the clinic as the room where the aerosol generator was situated.
Professor Andrea Ducci, an author of the study from UCL Mechanical Engineering, said: “Our experiments demonstrated that high volume of particles can be corralled into particular areas as a result of airflow dynamics. This obviously isn’t ideal, particularly if that place is a key location, such as the nurses’ station that staff members who’re treating patients will likely visit often during their shift.
“The good news is that we’re rapidly expanding our knowledge of this phenomenon. The project that we are currently working on aims to simulate the entire airflow within a clinic and assess the efficacy of different devices positioned in different locations. This will allow us to identify relatively simple interventions, such as better positioning of ventilation devices to reduce the spread of particles, thus decreasing the risk of picking up an infection in hospital.”
Given the unpredictability of how aerosol particles move around spaces and the difficulty in measuring them, the team are currently building an AI system to help to do this and hope to start testing within the next 18 months.
The authors say the study holds great promise to inform governmental action on ensuring that NHS standards for ventilation and infection are fit for purpose, in line with efforts to prevent future pandemics.
1 Portable air cleaners, or purifiers, are devices that filter dust and fine particles out of the air. The devices used in this study all conformed to the HEPA standard, meaning they are designed to filter out almost all (99.7%) of the fine particles that pass through them. The PACs placed in the waiting room were large (around the size of a kitchen bin) and the ones used in smaller room were around the size of a desktop lamp.
2 The aerosol particles were created from a harmless saline solution and disbursed at a constant rate by an aerosol generator at roughly the face height of a seated person (1.2 metres). The particles were designed to mimic those breathed out by a person with an airborne respiratory infection, such as influenza.
Flossing your teeth at least once a week may be linked to a lower risk of stroke caused by blood clotting and atrial fibrillation, according to a preliminary study to be presented at the American Stroke Association’s International Stroke Conference 2025. The meeting is in Los Angeles, Feb. 5-7, 2025, and is a world premier meeting for researchers and clinicians dedicated to the science of stroke and brain health.
“A recent global health report revealed that oral diseases – such as untreated tooth decay and gum disease – affected 3.5 billion people in 2022, making them the most widespread health conditions,” said study lead author Souvik Sen, MD, MS, MPH, chair of the Department of Neurology, Prisma Health Richland Hospital and the University of South Carolina School of Medicine in Columbia, South Carolina. “We aimed to determine which oral hygiene behaviour – dental flossing, brushing or regular dentist visits – has the greatest impact on stroke prevention.”
The Atherosclerosis Risk in Communities (ARIC) study, one of the first large-scale investigations of this kind in the US, assessed the home use of dental floss through a structured questionnaire of more than 6000 people. Among those who reported flossing, 4092 had not experienced a stroke, and 4050 had not been diagnosed with atrial fibrillation (AFib).
Participants were asked about their status regarding high blood pressure, diabetes, high cholesterol, smoking, body mass index, education, regular brushing and dentist visits. During the 25 years of follow-up, 434 participants were identified as having strokes, of which 147 were larger artery brain clots, 97 were heart-driven clots and 95 were hardening of the smaller arteries. Additionally, 1291 participants were noted to have experienced AFib.
The analysis found:
Flossing was associated with a 22% lower risk of ischaemic stroke, 44% lower risk of cardioembolic stroke (blood clots traveling from the heart) and 12% lower risk of AFib.
The associated lower risk was independent of regular brushing and routine dental visits or other oral hygiene behaviours.
Increasing the frequency of flossing had a greater chance of stroke risk reduction.
Flossing was also associated with a lower chance of cavities and periodontal disease.
Researchers were surprised by the reduction of irregular heartbeats, or AFib. AFib is the most common form of irregular heartbeat. It can lead to stroke, heart failure or other cardiovascular complications.
“Oral health behaviours are linked to inflammation and artery hardening. Flossing may reduce stroke risk by lowering oral infections and inflammation and encouraging other healthy habits,” Sen said. “Many people have expressed that dental care is costly. Flossing is a healthy habit that is easy to adopt, affordable and accessible everywhere.”
Study limitations include that data were based on answers to a questionnaire, and the 25-year follow-up appears to have focused on stroke and heart outcomes only. There was no follow-up concerning flossing or other oral behaviours over the years, Sen said.
Propranolol, a drug often used to treat hypertension and prevent migraines was associated with a reduction in ischaemic stroke risk among women – but not men – using the drug for migraine prevention, according to a preliminary study to be presented at the American Stroke Association’s International Stroke Conference 2025. The meeting is in Los Angeles, Feb. 5-7, 2025, and is a world premier meeting for researchers and clinicians dedicated to the science of stroke and brain health.
The beta blocker propranolol had a stronger protective effect for ischaemic stroke risk in women with migraine, particularly those without aura. The medication did not have the same protective effect on men.
Migraine headaches are common in the general population, but they occur three times more often in women than in men. This debilitating condition is associated with an increased risk of stroke. While the beta blocker propranolol can be used to prevent migraines, its effectiveness in reducing overall stroke risk is still uncertain.
“Migraine is an often-ignored risk factor for cardiovascular issues. Until recently, preventive treatments for people who have migraines were not available,” said lead study author Mulubrhan Mogos, PhD, MSc, FAHA, an assistant professor at Vanderbilt University School of Nursing. “Many women suffer from migraines, and it’s important to note that propranolol may be beneficial for these women, particularly those who experience migraine without aura. This is an important discovery for those dealing with migraines.”
Mogos also noted that migraine disproportionately affects women from historically under-resourced communities, and this disparity may impact the ability to achieve education goals or maintain stable employment, creating a vicious cycle. While new treatments have proven effective, they may not be accessible to women in these groups due to high costs.
For the study, researchers reviewed more than 3 million electronic health records from two large databases. In separate analyses, researchers identified people with migraine who developed stroke and a control group of those with migraine who did not develop stroke. They then assessed whether the individuals were treated with propranolol for migraine and whether that treatment had impacted stroke risk.
“We initially looked at overall stroke and then ischemic stroke specifically. We refined our analysis further by controlling for possible confounders and found the association is significant and stronger for ischaemic stroke,” Mogos said.
After adjusting for potential variables, such as demographics (age, sex, race), other conditions (high blood pressure, diabetes, etc) and hormonal factors (use of birth control, pregnancy – considered separately for each woman) that might affect results the analysis found:
Propranolol was significantly associated with a reduced risk of ischaemic stroke in women with migraine, particularly in those without aura. The risk of developing a stroke was 52% lower for women taking the medication in one database analysis and 39% lower in the other. No stroke risk reduction was seen in men in either analysis group.
The protective effect of propranolol was stronger for ischaemic stroke and in women with migraine without aura. Migraine aura can include disturbances, such as flashing lights, blind spots, zigzag patterns or seeing coloured spots. Other symptoms include tingling or numbness in the face or hands, difficulty speaking, dizziness or confusion.
Secondary analyses showed lower overall stroke rates in women taking propranolol at multiple time points in both databases.
“Our findings indicate that women and health care professionals should discuss the advantages of preventive migraine interventions. For under-resourced individuals who bear a greater burden from this condition and may lack access to new treatments, we must ensure these treatments are available to them. This approach can help reduce health disparities,” Mogos said.
The main limitation is that this was a review of past data using electronic health records, which may introduce biases, such as misclassification errors from reliance on ICD codes (codes used to classify and report health conditions and diseases). These findings highlight the need for studies that look forward in time to confirm these results.
Doctors could soon reduce epilepsy misdiagnoses by up to 70% using a new tool that turns routine electroencephalogram, or EEG, tests that appear normal into highly accurate epilepsy predictors, a Johns Hopkins University study has found.
By uncovering hidden epilepsy signatures in seemingly normal EEGs, the tool could significantly reduce false positives, seen in around 30% of cases globally, and spare patients from medication side effects, driving restrictions, and other quality-of-life challenges linked to misdiagnoses.
“Even when EEGs appear completely normal, our tool provides insights that make them actionable,” said Sridevi V. Sarma, a Johns Hopkins biomedical engineering professor who led the work. “We can get to the right diagnosis three times faster because patients often need multiple EEGs before abnormalities are detected, even if they have epilepsy. Accurate early diagnosis means a quicker path to effective treatment.”
Epilepsy causes recurrent, unprovoked seizures triggered by bursts of abnormal electrical activity in the brain. Standard care involves scalp EEG recordings during initial evaluations. These tests track brainwave patterns using small electrodes placed on the scalp.
Clinicians partly rely on EEGs to diagnose epilepsy and decide whether patients need anti-seizure medications. However, EEGs can be challenging to interpret because they capture noisy signals and because seizures rarely occur during the typical 20 to 40 minutes of an EEG recording. These characteristics makes diagnosing epilepsy subjective and prone to error, even for specialists, Sarma explained.
To improve reliability, Sarma’s team studied what happens in the brains of patients when they are not experiencing seizures. Their tool, called EpiScalp, uses algorithms trained on dynamic network models to map brainwave patterns and identify hidden signs of epilepsy from a single routine EEG.
“If you have epilepsy, why don’t you have seizures all the time? We hypothesized that some brain regions act as natural inhibitors, suppressing seizures. It’s like the brain’s immune response to the disease,” Sarma said.
The new study analyzed 198 epilepsy patients from five major medical centers: Johns Hopkins Hospital, Johns Hopkins Bayview Medical Center, University of Pittsburgh Medical Center, University of Maryland Medical Center, and Thomas Jefferson University Hospital. Out of these 198 patients in the study, 91 patients had epilepsy while the rest had non-epileptic conditions mimicking epilepsy.
When Sarma’s team reanalysed the initial EEGs using EpiScalp, the tool ruled out 96% of those false positives, cutting potential misdiagnoses among these cases from 54% to 17%.
“This is where our tool makes a difference because it can help us uncover markers of epilepsy in EEGs that appear uninformative, reducing the risk of patients being misdiagnosed and treated for a condition they don’t have,” said Khalil Husari, co-senior author and assistant professor of neurology at Johns Hopkins. “These patients experienced side effects of the anti-seizure medication without any benefit because they didn’t have epilepsy. Without the correct diagnosis, we can’t find out what’s actually causing their symptoms.”
In certain cases, misdiagnosis happens due to misinterpretation of EEGs, Husari explained, as doctors may overdiagnose epilepsy to prevent the dangers of a second seizure. But in some cases, patients experience nonepileptic seizures, which mimic epilepsy. These conditions can often be treated with therapies that do not involve epilepsy medication.
In earlier work, the team studied epileptic brain networks using intracranial EEGs to demonstrate that the seizure onset zone is being inhibited by neighboring regions in the brain when patients are not seizing. EpiScalp builds on this research, identifying these patterns from routine scalp EEGs.
Traditional approaches to improve EEG interpretation often focus on individual signals or electrodes. Instead, EpiScalp analyses how different regions of the brain interact and influence one another through a complex network of neural pathways, said Patrick Myers, first author and doctoral student in biomedical engineering at Johns Hopkins.
“If you just look at how nodes are interacting with each other within the brain network, you can find this pattern of independent nodes trying to cause a lot of activity and the suppression from nodes in a second region, and they’re not interacting with the rest of the brain,” Myers said. “We check whether we can see this pattern anywhere. Do we see a region in your EEG that has been decoupled from the rest of the brain’s network? A healthy person shouldn’t have that.”
Right side heart failure. Credit: Scientific Animations CC4.0
Pathways to new treatments for heart failure take time – as long as four decades for two now accepted therapies. So, new attempts to repair scar tissue in infarcted hearts using cells or cell products need more time to develop clinical therapies that can reduce risk of death from heart failure after a heart attack.
This message is part of a critical review of cell-based and cell product-based therapies for the treatment of heart failure. The review details 20 years of completed and ongoing clinical trials. While none has gained medical approval, they have proven safe and some have shown beneficial effects.
More importantly, the reviewers note, it took longer, nearly 40 years, to optimise two current therapies to reduce mortality in heart failure: implantable cardioverter–defibrillators and guideline-directed medical therapy.
“The history of the development of life-saving medical therapies for heart failure serves as an important lesson that we should remain hopeful of the promise of cell therapy in heart failure,” Jianyi “Jay” Zhang, MD, PhD, and colleagues write in the review, “Trials and tribulations of cell therapy for heart failure: an update on ongoing trials,” published in Nature Reviews Cardiology. Zhang is professor and chair of the University of Alabama at BirminghamDepartment of Biomedical Engineering.
Heart failure is responsible for 13% of deaths worldwide. Half of patients with heart failure die within five years. The most common cause of heart failure is blockage of coronary arteries leading to death of the cardiomyocyte heart muscle cells. When that muscle tissue is replaced by dense scar tissue with little blood circulation, the infarcted heart loses contractile power, leading to heart enlargement, progressive loss of pumping ability, increased chance of ventricular arrhythmias and clinical end-stage heart failure.
The problem is that shortly after birth, human heart muscle cells lose their ability to divide, so a damaged infarcted heart cannot repair itself by growing new muscle cells. Thus, the simple idea behind initial cell therapies was to add or inject replacement cells to the scar area to restore muscle tissue.
The two decades since has been a long road, with bumps and turns. The three parts of the Nature Reviews Cardiology paper describe the journey.
First is a history of the slow development, obstacles, setbacks and scepticism for two current heart failure therapies, implantable cardioverter–defibrillators and guideline-directed medical therapy. The next two sections, and main focus of the review, survey 13 completed clinical trials published in the last 12 years and 10 very recently initiated and ongoing clinical trials that are based on the lessons learned from the past 20 years of research, to assess the safety and efficacy of cell- and cell products-based therapy approaches.
While several randomised, double-blind, multicentre phase II or III trials published in the past 20 years support the concept that even a single dose of cell products has beneficial effects in patients with heart failure on optimal medical therapy, the ongoing trial are taking novel directions, Zhang says.
These include:
New cell types — pluripotent stem cell-derived cardiomyocytes/ spheroids and umbilical cord-derived mesenchymal stem cells
Repeated intravenous injections as a noninvasive cell delivery method
New cell products, such as engineered epicardial cardiomyocyte patches
Novel cell-free products — extracellular vesicle-enriched or exosome-enriched secretomes.
“The results of these trials will continue to define and refine our understanding of cell and cell product therapy as a novel addition in the treatment of patients with heart failure,” Zhang said.
The review acknowledges scientific criticism during the slow but consistent progress and evolution of cell therapy. Some have questioned the use of public funding to support cell therapy research for heart failure treatment, due to poorly designed or underpowered clinical trials and very modest improvements in cardiac function in preclinical studies that are not always substantiated in large-scale clinical trials.
“These criticisms must be addressed in future trials that are adequately powered and rigorously designed to ensure continued progress of the field,” Zhang said. “Critique is an essential part of science, and the basis for growth, innovation and evolution – this is no less true for the field of cell therapy.”
Yet Zhang is confident that current research will yield clinical translation. “In the past 20 years, cell therapy has emerged and evolved as a promising avenue for cardiac repair and regeneration,” he said. “Cell therapy has encountered substantial barriers in both preclinical studies and clinical trials, but the field continues to progress and evolve through lessons learned from such research.”
3D structure of a melanoma cell derived by ion abrasion scanning electron microscopy. Credit: Sriram Subramaniam/ National Cancer Institute
A research team at the Medical University of Vienna led by Maria Sibilia has investigated a new combination therapy against cancer. This therapy employs systemic administration of the tissue hormone interferon-I combined with local application of Imiquimod. Promising results were seen in topically accessible tumours like melanoma and breast cancer models: the therapy led to the death of tumour cells at the treated sites and simultaneously activated the adaptive immune system to fight even distant metastases. The findings, published in Nature Cancer, could improve the treatment of superficial tumours such as melanoma and breast cancer.
In recent years, immunotherapies have had significant success in the treatment and cure of a wide range of cancers. However, for some patients, these agents are still not sufficiently effective. As part of a preclinical study, Maria Sibilia, Head of the Center for Cancer Research at the Medical University of Vienna, therefore investigated the effects of a combination immunotherapy consisting of systemic administration of the tissue hormone interferon (IFN)-I and local imiquimod therapy. Imiquimod is an active substance that activates the innate receptors TLR7/8 and used to treat basal cell carcinomas. The researchers employed various preclinical mouse tumour models of melanoma and breast cancer. What both tumours have in common is that they are accessible to local therapy and often form distant metastases.
Effective for local tumours and distant metastases
Immunotherapies use the body’s own immune system to fight cancer cells. Plasmacytoid dendritic cells (pDCs), which are activated by Imiquimod via TLR7/8, play an important role in this process. The study showed that oral imiquimod stimulates pDCs to produce the tissue hormone IFN-I. This sensitised other dendritic cells and macrophages in the tumour environment to topical imiquimod therapy, which inhibited the formation of new blood vessels via the cytokine IL12 leading to the death of tumour cells. The combination immunotherapy not only had an effect on the treated tumours, but also on distant metastases. It reduced the formation of new metastases thus preventing tumour relapses and increasing the sensitivity of melanomas to checkpoint inhibitors.
“These findings illustrate that the combination of systemic treatment with imiquimod or IFN-I and topical therapy with imiquimod has the potential to expand treatment options for patients and improve therapy outcomes in locally accessible tumors such as melanoma or breast cancer,” emphasizes Maria Sibilia. “Topical treatment of the primary tumor with imiquimod is essential for this combination therapy with systemic IFN-I to be effective at the treated site and also to clear distant metastases,” adds Philipp Novoszel, MedUni Vienna, one of the first authors of the study.
The results suggest that this therapeutic strategy has the potential to improve treatment outcomes in superficial and thus locally accessible tumors such as melanoma and breast cancer – on the one hand through therapy-associated cancer cell death at the locally treated tumors, but also through the induction of a T cell-induced anti-tumor immune response at distant metastases, which is further enhanced by checkpoint inhibitors.
“Our aim is to continue developing immunotherapeutic strategies in order to improve the long-term prospects for patients who are not yet responding well to these agents,” says Maria Sibilia, who is also Deputy Head of the Comprehensive Cancer Center of MedUni Vienna and University Hospital Vienna. “As systemic interferon is a well-known cancer therapy and dendritic cells are activated in a similar way to our preclinical models, we believe that the new combination therapy can show an effect in patients,” adds Martina Sanlorenzo, dermato-oncologist at MedUni Vienna and co-first author of the study.
Publication: Nature Cancer Systemic IFN-I combined with topical TLR7/8 agonists promotes distant tumor-suppression by c-Jun-dependent IL-12 expression in dendritic cells Sanlorenzo M, Novoszel P, Vujic I, Gastaldi T, Hammer M, Fari O, De Sa Fernandes C, Landau AD, Göcen-Oguz BV, Holcmann M, Monshi B, Rappersberger K, Agnes Csiszar A, Sibilia M DOI: 10.1038/s43018-024-00889-9; https://www.nature.com/articles/s43018-024-00889-9
A new study led by researchers at Moffitt Cancer Center shows that asymptomatic brain metastasis is more common in stage 4 breast cancer patients than previously believed. The study, published in Neuro-Oncology, suggests that doctors may need to rethink current screening guidelines for detecting brain metastasis in patients without symptoms.
Researchers examined 101 asymptomatic patients diagnosed with stage 4 breast cancer, including triple-negative, HER2-positive and hormone receptor-positive/HER2-negative breast cancer. These patients underwent MRI scans to check for brain metastasis, with a follow-up MRI six months later if the initial scan showed no signs of cancer spread.
Of the patients who completed the initial MRI, 14% had brain metastasis. The rates by subtype were:
18% in triple-negative breast cancer
15% in HER2-positive breast cancer
10% in hormone receptor-positive/HER2-negative breast cancer
After the second MRI, the number of patients with brain metastasis grew to about 25% in each subtype. Following diagnosis, patients went on to receive early treatment for their brain metastases, including changes in systemic therapy and local therapies.
“Our study suggests that asymptomatic brain metastasis is quite common in stage 4 breast cancer,” said Kamran Ahmed, MD, associate member and section chief for Breast Radiation Oncology at Moffitt and principal investigator of the study. “Although larger studies are needed to confirm our findings, given the improvements in systemic and local therapies for breast cancer brain metastasis, the time may be appropriate to reconsider current guidelines that recommend against routine MRI surveillance in late stage breast cancer.”
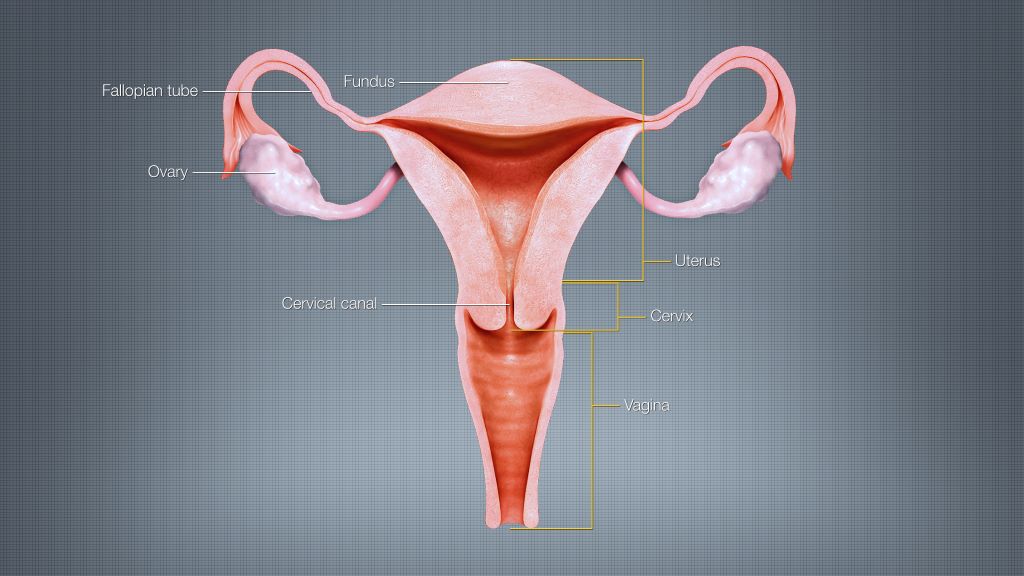
A mathematical modelling study conducted in Germany suggests that ovarian cancer incidence could be reduced and healthcare savings boosted if women who have already completed their families were offered fallopian tube removal during any other suitable abdominal surgeries. Angela Kather and Ingo Runnebaum of Jena University Hospital, Germany, and colleagues present these findings on January 30th in the open-access journal PLOS Medicine.
Some of the most widespread and serious forms of ovarian cancer begin in the fallopian tubes, and removing them may reduce ovarian cancer risk. While women at average risk of ovarian cancer are not recommended to have surgery solely to remove their fallopian tubes, many surgeons offer “opportunistic” tube removal during other gynaecologic surgeries such as hysterectomy or tubal sterilisation. Opportunistic removal may also be feasible during other abdominal surgeries, such as gallbladder removal.
However, the overall potential benefits of opportunistic fallopian tube removal have been unclear. To help clarify, Kather and colleagues developed a mathematical model that incorporates real-world patient statistics to predict population-level risks of ovarian cancer after opportunistic fallopian tube removal, as well as the potential healthcare cost savings.
By applying the model to statistics from Germany, the researchers predicted that opportunistic fallopian tube removal during every hysterectomy and tubal sterilisation could reduce ovarian cancer cases by 5% across the female population of Germany. Removal during every suitable abdominal surgery for women who are done having children could reduce nationwide cancer cases by 15%, the analysis suggests, and it could save more than €10 million in healthcare costs annually.
Ovarian cancer is the third most common gynaecologic cancer in the world and has a mortality rate of 66%. Overall, these findings suggest that opportunistic fallopian tube removal during appropriate abdominal surgeries could not only lower population-level ovarian cancer risks and prevent ovarian cancer deaths, but also provide economic benefits. This study could help inform health policy and insurance costs for the procedure.
The authors add, “We developed a mathematical model to estimate the likelihood of women undergoing surgeries that offer an opportunity for fallopian tube removal and the potential for reducing their ovarian cancer risk. Applying this model to the entire female population of Germany revealed that 15% of ovarian cancer cases could be prevented if fallopian tubes were removed during every suitable abdominal surgery in women who have completed their families. This approach has the potential to extend healthy years of life and significantly save healthcare costs.”
Credit: Darryl Leja National Human Genome Research Institute National Institutes Of Health
Traditional approaches to prostate cancer screening involve blood tests, MRI, and biopsies. Besides being uncomfortable, some of these procedures result in overdiagnosis of low-grade cancers.
Prostate cancers are categorised based on their Gleason Grade or Grade Group. Those with Gleason 3+4=7, or Grade Group 2, or higher are more likely to grow and cause harm in comparison with Gleason 6 or Grade Group 1 prostate cancers, which are considered non-aggressive.
The urine test, called MyProstateScore 2.0, or MPS2, looks at 18 different genes linked to high-grade prostate cancer.
The researchers had previously demonstrated that the test was effective in identifying GG2 or higher cancers, helping patients avoid unnecessary biopsies. But in that study, urine samples were obtained after a digital rectal examination.
“The process requires the prostate to be compressed, causing the release of cellular debris into a urine sample that the patient provides after the rectal exam,” said Ganesh S. Palapattu, MD, a professor of urology.
Its primary benefit is that the test can accurately predict your probability of developing aggressive prostate cancer, putting both the patient and physician at ease.”
-Ganesh Palapattu, MD
Such an examination may not be practical for many and is associated with some discomfort.
Developing a potential at-home test
In the study, the team modified the urine collection approach so that the MPS2 test could detect markers for prostate cancer, without requiring a prior rectal exam.
Using urine samples from a cohort of 266 men who did not undergo a rectal exam, they found that the test could detect 94% of GG2 or higher cancers and was more sensitive than blood tests.
Further, the team used mathematical models to demonstrate that the use of MPS2 would have avoided up to 53% of unnecessary biopsies.
“These results show that MPS2 has promise as an at-home test,” Palapattu said.
“Its primary benefit is that the test can accurately predict your probability of developing aggressive prostate cancer, putting both the patient and physician at ease.”
MPS2 can also help patients save on healthcare costs since it is significantly cheaper than an MRI.
The team is interested in repeating the study and corroborating their results with a larger, diverse population of men.
They’re also hoping to study the test’s performance in men as a surveillance screen for low-risk prostate cancer.
“MPS2 could potentially improve the health of our patients by avoiding overdiagnosis and overtreatment and allowing us to focus on those who are most likely to have aggressive cancers,” Palapattu said.