Seizures in newborns are one of the most frequent acute neurological conditions among infants admitted to neonatal care units. A study published in Developmental Medicine & Child Neurology indicates that newborns experiencing such neonatal seizures face an elevated risk of developing epilepsy.
For the study, investigators analysed data on all children born in Denmark between 1997 and 2018, with the goal of comparing the risk of epilepsy in children with and without neonatal seizures.
Among 1,294,377 children, the researchers identified 1,998 who experienced neonatal seizures. The cumulative risk of epilepsy was 20.4% among children with neonatal seizures compared with 1.15% among children without. This indicates that 1 in 5 newborns with neonatal seizures will develop epilepsy.
Epilepsy was diagnosed before 1 year of age in 11.4% of children with neonatal seizures, in an additional 4.5% between 1 and 5 years, 3.1% between 5 and 10 years, and 1.4% between 10 and 22 years. Stroke, hemorrhage, or structural brain malformations in newborns, as well as low Apgar scores, were associated with the highest risks of developing epilepsy.
“Our study highlights that there are risk factors that may be used to identify infants for tailored follow-up and preventive measures,” said corresponding author Jeanette Tinggaard, MD, PhD, of Copenhagen University Hospital – Rigshospitalet. “Importantly, four out of five neonatal survivors with a history of neonatal seizures did not develop epilepsy, and we suggest future studies to explore a potential genetic predisposition.”
Researchers have found a potential new way to slow the progression of lung fibrosis and other fibrotic diseases by inhibiting the expression or function of Piezo2, a receptor that senses mechanical forces in tissues including stress, strain, and stiffness. The new study in The American Journal of Pathology, published by Elsevier, sheds light on the underlying mechanisms of pulmonary fibrotic diseases and identifies potential new targets and options for therapy to improve patients’ outcomes.
Pulmonary fibrotic diseases are a group of conditions that cause significant morbidity and sometimes mortality. Idiopathic pulmonary fibrosis (IPF) is a devastating progressive fibrotic lung disease with a median survival of 2.9 years from diagnosis. Lung fibrosis results in dramatic mechanical changes including increased stiffness in the tissue that cells can sense and respond to, making it difficult for the lungs to expand and contract properly during breathing.
Piezo channels are a newly discovered receptor that are sensitive to mechanical signals. Since the 2021 Nobel Prize in Medicine was awarded to Dr Ardem Patapoutian for the discovery of Piezo channels in 2010, interest has increased in their role in tissue homeostasis and disease outside of neuronal signalling, however, little has been published on their possible role in fibrotic lung diseases. A group of researchers driven to understand how mechanical forces in lung tissue contribute to and drive pulmonary fibrosis investigated the role of Piezo2 in pulmonary fibrosis using donor tissue from patients with IPF, mouse models of lung fibrosis, cell culture investigation of lung cells (fibroblasts) that create the fibrosis lesions, and by examining publicly available RNAseq datasets from other research groups.
Investigators found that:
Piezo2 is highly expressed in human lung tissue from patients with IPF and in multiple (different) mouse models of lung fibrosis.
Piezo2 is highly expressed in primary human lung fibroblasts in culture, the cells that are believed to play key roles in producing fibrosis in tissues (by proliferating and laying down matrix proteins, creating scar-like features).
Lung fibroblasts grown on stiffer substrates are reprogrammed to be more profibrotic, by proliferating, producing extra matrix proteins, and differentiating to scar-forming myofibroblasts.
Inhibition of Piezo2 with either RNA silencing or a peptide inhibitor, to prevent them from sensing the stiffness of their environment, reduces profibrotic programming.
Lead investigator Patricia J. Sime, MD, Division of Pulmonary Disease and Critical Care Medicine, Virginia Commonwealth University, says, “We are excited to report that this research that suggests inhibiting expression or function of Piezo2 could be a potential new therapeutic route to treating lung fibrosis and other fibrotic diseases. This is especially important as there is an unmet need for additional therapies for fibrotic diseases.”
Despite the introduction of nintedanib and pirfenidone for therapy of some fibrotic lung diseases, pulmonary fibrosis can remain challenging to effectively treat. This is in part because lung cells can be driven to a profibrotic phenotype by multiple pathways that reinforce each other, so that targeting one pathway alone may not be effective to slow or stop disease progression.
First author Margaret A.T. Freeberg, PhD, Division of Pulmonary Disease and Critical Care Medicine, Virginia Commonwealth University, continues, “Some types of lung fibrosis have been very difficult to treat. For example, IPF is a form of pulmonary fibrosis that often progresses. While there have been advances in therapy, the approved medications for IPF can slow, but do not always halt progression. One of the reasons that fibrosis can be difficult to effectively treat may be explained by the multiple profibrotic disease pathways that reinforce each other. Blocking Piezo2 signaling to prevent fibroblast reprogramming represents a new pathway we can target in our fight against fibrosis.”
Dr. Sime concludes, “This research identifies mechanical forces and a new specific target (Piezo2) that we can block to prevent fibrotic reprogramming of some lung cells. We believe this points to Piezo2 as an important new therapeutic target that might (by itself or in combination with other therapies) slow the progression of pulmonary fibrosis in our patients. Many new investigational drugs that target pulmonary fibrosis receive orphan drug designation from the FDA, and this may accelerate development and increase interest from pharmaceutical partners.”
Tiny fragments of plastic have become ubiquitous in our environment and our bodies. Higher exposure to these microplastics, which can be inadvertently consumed or inhaled, is associated with a heightened prevalence of chronic noncommunicable diseases, according to new research being presented at the American College of Cardiology’s Annual Scientific Session (ACC.25).
Researchers said the new findings add to a small but growing body of evidence that microplastic pollution represents an emerging health threat. In terms of its relationship with stroke risk, for example, microplastics concentration was comparable to factors such as minority race and lack of health insurance, according to the results.
“This study provides initial evidence that microplastics exposure has an impact on cardiovascular health, especially chronic, noncommunicable conditions like high blood pressure, diabetes and stroke,” said Sai Rahul Ponnana, MA, a research data scientist at Case Western Reserve School of Medicine in Ohio and the study’s lead author. “When we included 154 different socioeconomic and environmental features in our analysis, we didn’t expect microplastics to rank in the top 10 for predicting chronic noncommunicable disease prevalence.”
Microplastics—defined as fragments of plastic between 1 nanometre and 5 millimetres across—are released as larger pieces of plastic break down. They come from many different sources, such as food and beverage packaging, consumer products and building materials. People can be exposed to microplastics in the water they drink, the food they eat and the air they breathe.
The study examines associations between the concentration of microplastics in bodies of water and the prevalence of various health conditions in communities along the East, West and Gulf Coasts, as well as some lakeshores, in the United States between 2015-2019. While inland areas also contain microplastics pollution, researchers focused on lakes and coastlines because microplastics concentrations are better documented in these areas. They used a dataset covering 555 census tracts from the National Centers for Environmental Information that classified microplastics concentration in seafloor sediments as low (zero to 200 particles per square meter) to very high (over 40 000 particles per square metre).
The researchers assessed rates of high blood pressure, diabetes, stroke and cancer in the same census tracts in 2019 using data from the U.S. Centers for Disease Control and Prevention. They also used a machine learning model to predict the prevalence of these conditions based on patterns in the data and to compare the associations observed with microplastics concentration to linkages with 154 other social and environmental factors such as median household income, employment rate and particulate matter air pollution in the same areas.
The results revealed that microplastics concentration was positively correlated with high blood pressure, diabetes and stroke, while cancer was not consistently linked with microplastics pollution. The results also suggested a dose relationship, in which higher concentrations of microplastic pollution are associated with a higher prevalence of disease. However, researchers said that evidence of an association does not necessarily mean that microplastics are causing these health problems. More studies are required to determine whether there is a causal relationship or if this pollution is occurring alongside another factor that leads to health issues, they said.
Further research is also needed to determine the amount of exposure or the length of time it might take for microplastics exposure to have an impact on health, if a causal relationship exists, according to Ponnana. Nevertheless, based on the available evidence, it is reasonable to believe that microplastics may play some role in health and we must take steps to reduce exposures, he said. While it is not feasible to completely avoid ingesting or inhaling microplastics when they are present in the environment, given how ubiquitous and tiny they are, researchers said the best way to minimise microplastics exposure is to curtail the amount of plastic produced and used, and to ensure proper disposal.
“The environment plays a very important role in our health, especially cardiovascular health,” Ponnana said. “As a result, taking care of our environment means taking care of ourselves.”
In a separate study presented at ACC.25, researchers from a different group reviewed the scientific literature and found that studies showed a strong correlation between microplastics in plaques in the heart’s arteries and the risk of adverse cardiovascular events, suggesting that the presence of microplastics could play a role in the onset or exacerbation of serious heart problems.
Mass General Brigham and MIT investigators have developed a long-acting contraceptive implant that can be delivered through tiny needles to minimise patient discomfort and increase the likelihood of medication use.
Their findings in preclinical models provide the technological basis to develop self-administrable contraceptive shots that could mimic the long-term drug release of surgically implanted devices.
The new approach, which would reduce how often patients need to inject themselves and prove valuable for patients with less access to hospitals and other medical care providers, is described in Nature Chemical Engineering.
“Needle size and liquid viscosity are crucial considerations for commercial translation of injectables,” said senior author Giovanni Traverso, MD, PhD, MBBCH, of the Division of Gastroenterology in the Department of Medicine at Brigham and Women’s Hospital. “Our engineering challenge was finding a way to maximise comfort for patients by using smaller needles, which cause less bruising or bleeding, and to make the viscosity low enough for easy application with the syringe by hand.”
Traditional contraceptive implants are small, flexible rods that are surgically inserted under the skin to slowly deliver drugs over time, removing the hassle of remembering to take a pill. But the surgery required for implants makes them less accessible to some patients.
Traverso’s team developed a new approach to deliver the contraceptive drug levonorgestrel (LNG) through Self-assembling Long-acting Injectable Microcrystals (SLIM). SLIM act like tiny puzzle pieces that, once injected inside the body, undergo solvent exchange to assemble into a single solid implant that slowly releases the drug as the surface erodes. Unlike similar self-administering technologies, the solvent exchange assembly enables delivery by much smaller needles.
The researchers will continue their work to optimize the dosing, duration, and injectability of the SLIM system, including understanding how it performs in the human body. The design could also be applied to other hydrophobic drugs, which make up most new pharmaceuticals. The researchers plan to investigate how different drug properties impact the SLIM system’s effectiveness.
“We anticipate that SLIM could be a new addition to the current suite of family planning options available to women, especially for people in low-resource settings where options for contraception and health care facilities are limited,” said Traverso.
Developed by the University of South Australia in collaboration with the Medical School at Stanford University, this world first formulation uniquely combines limonene (a citrus essential oil) with a lipid-based drug delivery system to treat dry mouth (xerostomia), a common side effect of radiotherapy.
The new formula demonstrated 180-fold better solubility than pure limonene in lab experiments and boosted relative bioavailability by over 4000% compared to pure limonene in pre-clinical trials.
Dry mouth is the most reported side effect following radiotherapy for the treatment of head and neck cancer, affecting up to 70% of patients due to salivary gland damage. It can lead to difficulty speaking and swallowing, significantly reducing quality of life.
Limonene has protective effects on saliva production during radiotherapy, but its poor solubility means high doses are needed to take effect, and these cause indigestion, abdominal discomfort and unpleasant ‘citrus burps’.
Lead researcher, Professor Clive Prestidge says UniSA’s new limonene-lipid combination creates a ‘super-solubilising’ treatment that reduces dry mouth at lower dose and without uncomfortable side effects.
“The therapeutic benefits of limonene are well known. It’s used as an anti-inflammatory, antioxidant, and mood-enhancing agent, and can also improve digestion and gut function. But despite its widespread use, its volatility and poor solubility have limited its development as an oral therapy,” Prof Prestidge says.
“As limonene is an oil, it forms a film on the top of the stomach contents, causing significant stomach pain and discomfort.
“Our novel formulation combines limonene with healthy fats and oils – called lipids – to create a super-solubilising compound that the body can easily absorb with reduced uncomfortable side effects.
“This increases the dispersion of limonene in the stomach, boosts absorption, and controls biodistribution – all while increasing a patient’s saliva production and reducing dry mouth.”
Co-researcher Dr Leah Wright says the formulation has the potential to significantly improve the quality of life for cancer patients and others suffering dry mouth conditions.
“Cancer patients undergoing radiotherapy and other medical treatments regularly experience dry mouth, which not only prevents them from comfortably swallowing, but can also have other negative and potentially life-threatening outcomes,” Dr Wright says.
“While limonene can be ingested directly, it’s not well tolerated, especially by those with dry mouth. Plus, its poor absorption prevents it from effectively reaching the salivary glands – the target site.
“This inventive and highly impactful limonene-lipid formulation could provide a simple, effective oral solution for dry mouth, offering cancer patients long-lasting relief and comfort, improved oral health, and a higher quality of life during a difficult time.”
Clinical trials for the new formula are ongoing, with next steps to be announced soon.
Photo by Kampus Production: https://www.pexels.com/photo/man-in-blue-and-black-crew-neck-shirt-8638036/
The cells in human bodies are subject to both chemical and mechanical forces. But until recently, scientists have not understood much about how to manipulate the mechanical side of that equation. That’s about to change.
“This is a major breakthrough in our ability to be able to control the cells that drive fibrosis,” said Guy Genin, professor of mechanical engineering in the McKelvey School of Engineering at Washington University in St. Louis, whose research was just published in Nature Materials.
Fibrosis is an affliction wherein cells produce excess fibrous tissue. Fibroblast cells do this to close wounds, but the process can cascade in unwanted places. Examples include cardiac fibrosis; kidney or liver fibrosis, which precedes cancer; and pulmonary fibrosis, which can cause major scarring and breathing difficulties. Every soft tissue in the human body, even the brain, has the potential for cells to start going through a wound-healing cascade when they’re not supposed to, according to Genin.
The problem has both chemical and mechanical roots, but mechanical forces seem to play an outsized role. WashU researchers sought to harness the power of these mechanical forces, using a strategic pull and tug in the right mix of directions to tell the cell to shut off its loom of excess fibre.
In the newly published research, Genin and colleagues outline some of those details, including how to intervene in tension fields at the right time to control how cells behave.
“The direction of the tension these cells apply matters a lot in terms of their activation state,” said Nathaniel Huebsch, an associate professor of biomedical engineering at McKelvey Engineering and co-senior author of the research, along with Genin and Vivek Shenoy at the University of Pennsylvania.
The forces
The human body is constantly in motion, so it should come as no surprise that force can encode function in cells. But what forces, how much force and in which direction are some of the questions that the Center for Engineering MechanoBiology examines.
“The magnitude of tension will affect what the cell does,” Huebsch said. But tension can go in many different directions. “The discovery that we present in this paper is that the way stress pulls in different directions makes a difference with the cell,” he added.
Pulling in multiple directions in a nonuniform manner, called tension anisotropy (imagine a taffy pull) is a key force in kicking off fibrosis, the researchers found.
“We’re showing, for the first time, using a structure with a tissue, we’re able to stop cell cytoskeletons from going down a pathway that will cause contraction and eventual fibrosis,” Genin said.
Huebsch, who pioneered microscopic models and scaffolds for testing these tension fields that act on cells, explained that tentacle-like microtubules establish tension by emerging and casting out in a direction. Collagen around the cell pulls back on that tubule and becomes aligned with it.
“We discovered that if you could disrupt the microtubules, you would disrupt that whole organization and you would potentially disrupt fibrosis,” Huebsch said.
And, though this research was about understanding what goes wrong to cause fibrosis, there is still much to learn about what goes right with fibroblasts, connective tissue cells, especially in the heart, he added.
“In tissues where fibroblasts are typically well aligned, what is stopping them from activating to that wound-healing state?” Huebsch asked.
Personalised treatment plans
Along with finding ways to prevent or treat fibrosis, Genin and Huebsch said doctors can look for ways to apply this new knowledge about the importance of mechanical stress to treatment of injuries or burns. The findings could help address the high fail rate for treatments of elderly patients with injuries that require reattaching tendon to bone or skin to skin.
For instance, in rotator cuff injuries, there is compelling evidence that patients must start moving their arm to recover function, but equally compelling evidence that patients should immobilise the arm for better recovery. The answer might depend on the amount of collagen a patient produces and the stress fields at play at the recovery site.
By understanding the multidirectional stress fields’ impact on the cell structure, doctors may be able to look at specific patients’ repair and determine a personalised treatment plan.
For instance, a patient who has biaxial stress coming from two directions at the site of injury will potentially need to exercise more to trigger cell repair, Genin said. However, another patient showing signs of uniaxial stress, meaning stress is pulling only one direction, any movement could over-activate cells, so in that case, the patient should keep the injury immobilised. All that and more is still to be worked out and confirmed, but Genin is excited to begin.
“The next generation of disease we’re going to be conquering are diseases of mechanics,” Genin said.
Researchers have uncovered a stealth survival strategy that melanoma cells use to evade targeted therapy, offering a promising new approach to improving treatment outcomes.
The study, published in Cell Systems and conducted by researchers at the Institute for Systems Biology (ISB) and Massachusetts Institute of Technology (MIT) identifies a non-genetic, reversible adaptation mechanism that allows melanoma cells to survive treatment with BRAF inhibitors. By identifying and blocking this early response, researchers proposed a combination therapy that could delay resistance and enhance the effectiveness of existing treatments.
Cracking the Code of Melanoma’s Drug Escape
Melanoma, the deadliest form of skin cancer, is often driven by mutations in the BRAF gene, which fuels uncontrolled tumor growth. While BRAF inhibitors (such as vemurafenib) initially halt tumor growth, many tumors quickly adapt and survive treatment, leading to therapy failure.
Unlike traditional resistance driven by genetic mutations, this study uncovers an early, dynamic adaptation process that occurs within hours to days of drug treatment – long before genetic resistance takes hold. Surprisingly, this process does not rely on reactivating the BRAF-ERK pathway, which is the usual resistance mechanism.
Using cutting-edge mass spectrometry-based phosphoproteomics and deep transcriptomics analyses, researchers mapped the molecular shifts in melanoma cells over minutes, hours, and days of BRAF inhibitor treatment.
“We found that while the BRAF-ERK signaling pathway was quickly and durably suppressed, cancer cells did not rely on reactivating ERK to survive. Instead, they triggered an alternative SRC family kinase (SFK) signaling pathway, which promoted cell survival and eventual recovery,” said Chunmei Liu, PhD, a bioinformatics scientist at ISB and co-first author of the paper.
Turning a Weakness Into a Target
A key discovery in this study came when researchers linked SFK activation to reactive oxygen species (ROS), a cellular stress response that builds up under BRAF inhibition. As ROS levels surged, SFK activity spiked, helping melanoma cells withstand treatment. However, this adaptation was reversible – when treatment was removed, cells returned to their original state.
Recognizing this Achilles’ heel, the team tested a combination approach: pairing BRAF inhibitors with the SFK inhibitor dasatinib.
“By adding dasatinib, we blocked this adaptive escape mechanism, significantly reducing melanoma cell survival and stabilising tumours in animal models,” said ISB Associate Professor Wei Wei, PhD, co-corresponding author.
Importantly, SFK inhibition alone had little effect on melanoma cells, highlighting the need for a strategic combination therapy to suppress melanoma adaptation before resistance fully develops.
“This approach has the potential to prolong the effectiveness of BRAF inhibitors and improve patient outcomes,” said ISB President and Professor Jim Heath, PhD, co-corresponding author.
Looking Ahead: A Path to the Clinic
Beyond uncovering a key mechanism of drug adaptation, this research underscores the importance of early intervention to prevent it from happening. It also highlights ROS accumulation and SFK activation as potential biomarkers for identifying patients who may benefit from this combination therapy.
Further preclinical studies and clinical trials will be necessary to validate this combination therapy strategy and determine its potential for broader clinical use.
A new study, recently published in the journal Scientific Reports, has analysed and compared the fatty acids in the blood of individuals with schizophrenia, of those with cannabis use disorder and of those with both diagnoses, with the aim of shedding light on new biomarkers and improving the understanding of the biological relationship between the two disorders. The study also offers a powerful tool for identifying new biomarkers.
Cannabis is one of the most widely used substances in the world, with some 228 million users between the ages of 15 and 64. The risk of developing schizophrenia increases significantly with cannabis use, especially when it starts at a young age. What is more, it is estimated that approximately 10% of cannabis users will develop cannabis use disorder during their lifetime. Curiously, almost a third of individuals diagnosed with schizophrenia also meet the criteria for cannabis use disorder; and cannabis use disorder affects up to 42% of people with schizophrenia.
In this bid to shed light on the biological mechanisms that determine why some individuals develop schizophrenia while others only experience cannabis use disorder, despite similar levels of exposure to cannabis, the UPV/EHU’s Neuropsychopharmacology group has managed to detect “potential biomarkers in the blood that could help predict the risk some people have of developing a psychiatric disorder such as schizophrenia if they use cannabis”, explained Leyre Urigüen, coordinator of the study.
So, the research group compared the fatty acid content in the blood of samples taken from “a group of individuals with schizophrenia who did not use cannabis, a group who used cannabis and have developed a cannabis use disorder, a group with a dual pathology of schizophrenia with cannabis abuse, and a control group of individuals with neither a psychiatric disorder nor drug use”, explained Dr Urigüen. In the study they wanted to shed light on what happens “with people who use cannabis and develop schizophrenia; how do they differ from those who use cannabis and never develop a psychiatric disorder?” she added.
“We found considerable differences between these groups of individuals. By comparing the quantities of certain metabolites (fatty acids), we were able to perfectly differentiate between the three patient populations,” stressed the UPV/EHU researcher. “This indicates that there is an altered or different metabolism between these three groups.” In this study the Neuropsychopharmacology research group at the UPV/EHU detected “that some fatty acids differentiate between the cannabis-using group and the groups with schizophrenia and dual-diagnosis patients. These molecules could potentially be biomarkers”, said Urigüen.
Paving the way forward
The researcher is very hopeful about this finding: “I think it is important to be capable of finding blood biomarkers that can help predict the risk of developing a psychiatric disorder, such as schizophrenia due to cannabis use, and this study has proven to be the start of this way forward. Now this has to be disproved by studies with a larger cohort of people than the one we have analysed.”
In this respect, the researcher stressed that another of the strengths of the study is “the fine-tuning of plasma lipidomics in patients; in other words, the complete study of fatty acids (lipids). We are proposing a way of working that can be replicated by other groups, and that way, headway can be made in the specification of these metabolites”. This approach has been developed by the IBeA research group under the direction of the UPV/EHU professor Nestor Etxebarria. Both groups are working side by side on “various approaches to the study in which they are trying to find answers to these and many other questions”.
Mycobacterium tuberculosis drug susceptibility test. Photo by CDC on Unsplash
By Catherine Tomlinson
Both TB treatment and TB preventive therapy involve taking lots of pills, usually for several months. Researchers are working on new long-acting formulations that might, for example, reduce an entire course of TB preventive therapy to a single injection.
The biggest HIV news of last year was that an injection containing an antiretroviral called lenacapavir provides six months of protection against HIV infection per shot. While it will be several years before the jabs become widely available, experts nevertheless hailed the development as a potential game-changer. In some countries, HIV treatment is already available as injections – containing the antiretrovirals cabotegravir and rilpivirine – administered every two months.
Scientists working on tuberculosis (TB) are trying to replicate the successes of the HIV field and develop similarly long-acting formulations of TB medicines. The good news is that they have several exciting products under development – the bad news is that the research is still at a very early stage and the pivotal studies that will tell us if these products work are likely still years away.
But if they work, they could make a big difference to patients. That is because TB treatment and TB preventive therapy mostly still requires swallowing lots of pills over a long period of time. There is some good evidence that many people would prefer long-acting injections.
The case for long-acting TB medicines
TB preventive therapy is used to stop someone suspected of having latent TB infection from falling ill with TB. In South Africa, such preventive therapy is recommended for all close contacts of someone sick with TB. Typically, it involves taking tablets for three or six months (a one-month course has been shown to work, but is not widely available). There is research that shows that the shorter the regimen the more likely it is to be completed.
The hope is that a long-acting product might do away with swallowing tablets altogether and reduce an entire course of preventive therapy to a single injection. This is likely to be more convenient for patients as well as come with the benefit of perfect treatment completion rates.
TB preventive therapy is a simpler target for long-acting formulations than TB treatment since it typically involves only one or two drugs and treatment durations are shorter. TB treatment typically takes six or more months to complete and usually involves taking four different drugs – often four for two months and then only two for the remaining four months in what is called the continuation phase. Some of the current thinking is that the continuation phase could potentially be replaced by long-acting formulations of TB medicines. This could shorten the duration of TB treatment to just two months of taking tablets.
Not an easy nut to crack
As explained by Dr Eric Nuermberger of Johns Hopkins University, not all TB medicines available as tablets make good candidates for translation to long-acting injectable formulations. He was presenting on long-acting TB drugs at the Conference for Retroviruses and Opportunistic Infections (CROI), recently held in San Francisco.
Nuermberger outlined three key characteristics that are needed for long-acting formulations. These are low water solubility (so the drug doesn’t dissolve to quickly), low clearance in plasma (so that the body doesn’t clear the drug too quickly), and high drug potency (so that a small volume of drug can be effective for a long period of time).
One key challenge, according to Nuermberger, is that scientists do not yet have reliable biomarkers to measure the effectiveness of long-acting TB preventive therapy in phase II trials. Biomarkers, such as blood levels of certain proteins, could in theory offer scientists a faster way to assess if TB preventative therapy is working, without having to monitor clinical trial participants for long periods of time to determine treatment outcomes.
Writing in the journal Clinical Infectious Diseases, scientists working to develop long-acting TB products explained: “The inability to culture or otherwise quantify viable bacteria during latent TB infection and the lack of validated surrogate biomarkers mean that there is no opportunity to obtain initial proof of efficacy… which is usually the domain of phase 2 trials. Instead, the development of new TPT regimens requires bridging directly from preclinical studies and phase 1 trials to phase 3 trials, which are themselves long and require large numbers of participants.”
However, they added that “[t]he search for biomarkers that act as prospective signatures of risk for developing TB disease is a very active research area and an important scientific priority for the field”.
Back at CROI, Nuermberger also told participants that most products in the pipeline remain at pre-clinical stages and are still being tested in mice. He explained that differences in how depot drugs — drugs released slowly over time — work in mice and humans make it hard to apply findings from mice to humans. But modeling is being done to help bridge this gap.
‘Expanded remarkably’
Despite these challenges, Nuermberger said “the number of long-acting drug formulations in development [for TB] has really expanded remarkably in the last few years, which is a very promising development”.
The product that is furthest along in the development pipeline, but still at a very early stage of research, is a long-acting form of bedaquiline. This drug is currently used for the treatment of drug-resistant forms of TB and falls in a class of antibiotics known as diarylquinolines.
The Belgian pharmaceutical company Janssen is currently running a phase I trial of long-acting injectable bedaquiline in Austria. Phase I trials are conducted in a small group of healthy individuals to assess the safety and tolerability of an experimental medicine. In the phase 1 bedaquiline trial, researchers are investigating the safety and tolerability of different doses of long-acting injectable bedaquiline.
Several other long-acting TB medicines are being investigated in preclinical research, including long-acting versions of the TB medicines rifabutin and rifapentine, as well as the second generation diarylquinolines, TBJ-876 and TBA-587, which are under development by the TB Alliance. The second generation diarylquinolines are being tested on their own and in combination with pretomanid and telacebec.
In addition, the University of Liverpool, Johns Hopkins University, University of Southern Denmark, University of North Carolina and the US pharmaceutical company Inflamamasome Therapeutics, are all involved in pre-clinical research on long-acting formulations. These efforts are supported financially by Unitaid, the US National Institutes of Health, and the Gates Foundation.
The treatments being developed include aqueous nanoparticle suspensions, in-situ forming implants, and rod implants. Aqueous nanoparticle suspensions are drugs turned into tiny particles and delivered in a water-based solution via injection. In-situ forming implants are injected as a liquid that then solidifies into an implant under the skin. Rod implants are small, rod-shaped devices inserted under the skin with a needle-like tool after numbing the area with a local anaesthetic.
What users prefer
At CROI, delegates also learned about patient and provider preferences for long-acting TB treatment.
Dr Marcia Vermeulen from the University of Cape Town presented the results of a survey involving over 400 patients in South Africa and India, as well as 94 healthcare providers.
Seventy-five percent of healthcare workers said they would prescribe a long-acting injectable product rather than pills for tuberculosis preventative therapy if it was priced the same or lower. Similarly, 75% of patients said they would try an injectable product for TB prevention if it became available.
“As a TB survivor, I am excited about long-acting TB treatment as it doesn’t require frequent facility visits, saving a person’s time and money, and can thereby increase adherence and improve treatment outcomes,” TB Proof’s Phumeza Tisile told Spotlight.
She added that communities should be at the heart of rollout plans because they understand the needs of people affected by TB and know how to communicate effectively to encourage involvement and adoption.
Disclosure: The Gates Foundation is mentioned in this article. Spotlight receives funding from the Gates Foundation but is editorially independent – an independence that the editors guard jealously. Spotlight is a member of the South African Press Council.
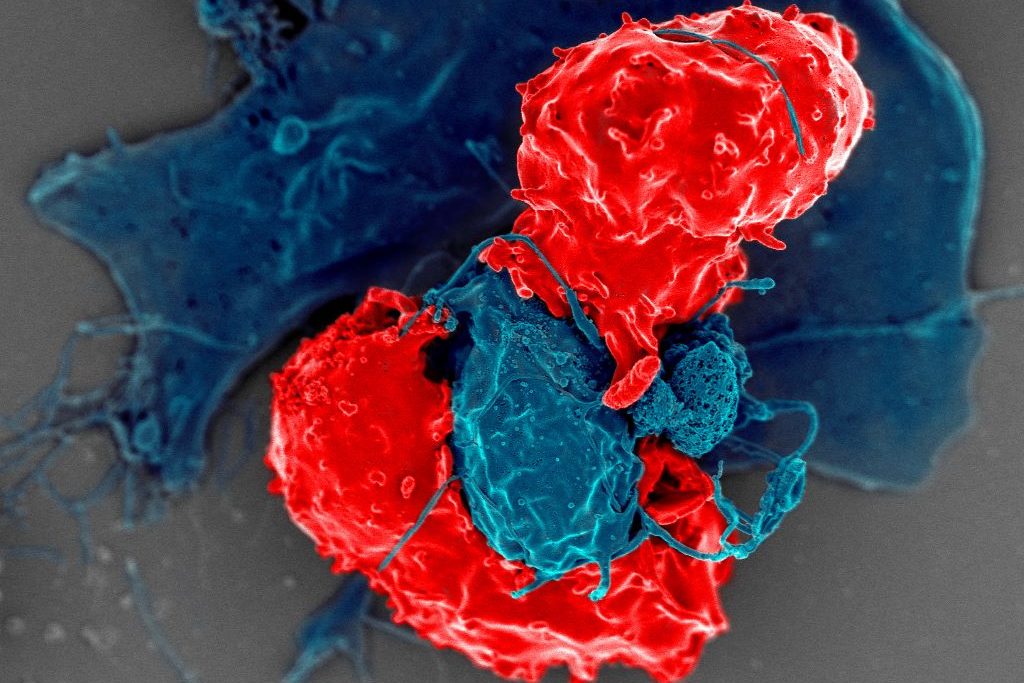
Scanning electron microscope image of T regulatory cells (red) interacting with antigen-presenting cells (blue). T regulatory cells can suppress responses by T cells to maintain homeostasis in the immune system. Credit: National Institute of Allergy and Infectious Diseases/NIH
In the flurry of immune activity in an infection, immune cells need to be prevented from mistakenly attacking each other. New research from the University of Chicago shows how a specially trained population of immune cells keeps the peace by preventing other immune cells from attacking their own. The study, published in Science, provides a better understanding of immune regulation during infection and could provide a foundation for interventions to prevent or reverse autoimmune diseases.
Several groups of white blood cells help coordinate immune responses. Dendritic cells take up proteins from foreign pathogens, chop them up into peptides called antigens, and display them on their surface. CD4+ conventional T (Tconv) cells, or helper T cells, inspect the peptides presented by dendritic cells. If the peptides are foreign antigens, the T cells expand in numbers and transform into an activated state, specialized to eradicate the pathogen. If the dendritic cell is carrying a “self-peptide,” or peptides from the body’s own tissue, the T cells are supposed to lay off.
During an autoimmune response, the helper T cells don’t distinguish between foreign peptide antigens and self-peptides properly and go on the attack no matter what. To prevent this from happening, another group of T cells called CD4+ regulatory T (Treg) cells, are supposed to intervene and prevent friendly fire from the Tconv cells.
“You can think of them [Treg cells] as peacekeeper cells,” said Pete Savage, PhD, Professor of Pathology at UChicago and senior author of the new study. Tregs obviously do their job well most of the time, but Savage said that it has never been clear how they know when to intervene and prevent helper T cells from starting an autoimmune response, and when to hold back and let them fight an infection.
So, Savage and his team, led by David Klawon, PhD, a former graduate student in his lab who is now a postdoctoral fellow at the Massachusetts Institute of Technology (MIT), wanted to explore this property of the immune system, known in the field as self-nonself discrimination. T cells are produced in the thymus, a specialised organ of the immune system. During development, Treg cells are trained to recognise specific peptides, including self-peptides from the body. When dendritic cells present a self-peptide, the Treg cells trained to spot them intervene to stop helper T cells from getting triggered.
For the study, Savage and Klawon worked in close collaboration with co-first author Nicole Pagane, a graduate student at MIT, as well as co-corresponding authors Harikesh Wong at the Ragon Institute of the Massachusetts General Hospital, MIT and Harvard University, and Ron Germain at the National Institutes of Health.
T cell specificity is what the team found makes a crucial difference in self-nonself discrimination. The researchers experimentally depleted Treg cells in mice that were specific to a single self-peptide from the prostate. In healthy mice in the absence of infection, this change did not trigger autoimmunity to the prostate. When the researchers infected mice with a bacterium that expressed the prostate self-peptide, however, the absence of matched, prostate-specific Treg cells triggered prostate-reactive T helper cells and introduced autoimmunity to the prostate.
Interestingly though, this alteration did not impair the ability of helper T cells to control the bacterial infection by responding to foreign peptides.
“It’s like a doppelganger population of T cells. The CD4 helper cells that could induce disease by attacking the self share an equivalent, matched population of these peacekeeper Treg cells,” Savage said. “When we removed Treg cells reactive to a single self-peptide, the T helper cells reactive to that self-peptide were no longer controlled, and they induced autoimmunity.”
The root causes of autoimmune disease are a complex interaction of genetics, the environment, lifestyle, and the immune system. Classic, conventional thinking in the immunology field promoted the idea that the immune system establishes self-nonself discrimination by purging the body of helper T cells that are reactive to self-peptides, thereby preventing autoimmunity. Savage said this study shows that purging is inefficient though, and that specificity matching by Treg cells may be equally as important.
“The idea is that specificity matters, and for a fully healthy immune system, you need to have a good collection of these doppelganger Treg cells,” he said. As long as the immune system generates enough matched Treg cells, they can prevent autoimmune responses without impacting responses to infections.
“It’s like flipping the idea of self-nonself discrimination upside down. Instead of having to delete all helper T cells reactive to self-antigens, you simply generate enough of these Treg peacekeeper cells instead,” Savage said.