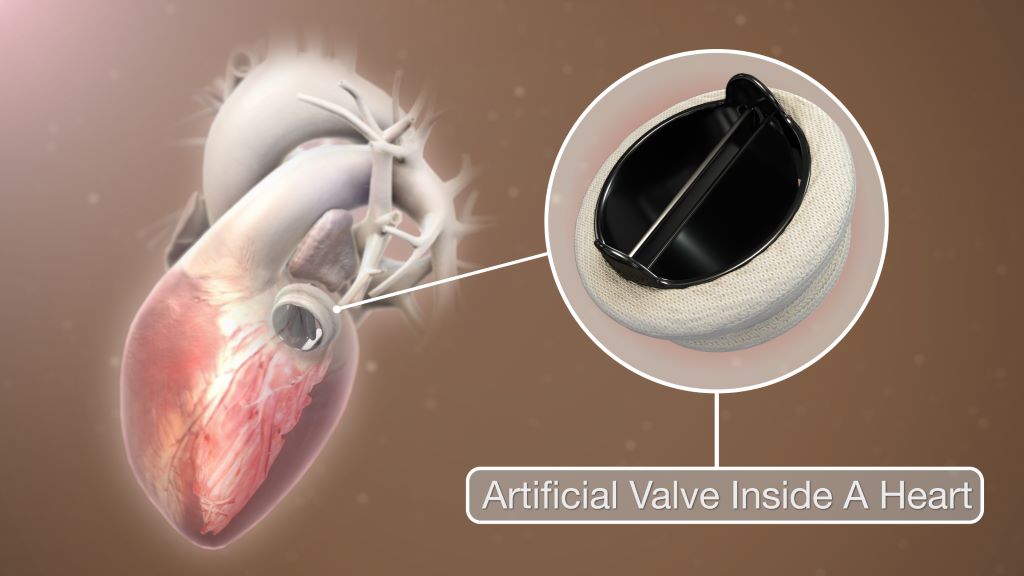
Patients aged between 50 to 70 years with a mechanical heart valve replacement had better long-term survival compared to those with a biological valve, new research led by the University of Bristol has found. The study is published in the European Journal of Cardio-Thoracic Surgery.
The last two decades have seen an increase in the use of biological over mechanical heart valve replacements. However, while short-term clinical outcomes are known to be the same, long-term outcomes are still under debate.
Existing guidelines support the use of mechanical valves made of synthetic materials in patients below the age of 50, while biological valves made of animal tissue are favoured for those above the age of 65 or 70. The guidelines leave the choice to the decision of surgeons and patients who are 50 to 70 years old.
The research team wanted to find out the clinical outcomes for patients aged between 50 to 70 years undergoing elective and urgent heart valve replacement at the Bristol Heart Institute (BHI) over a 27 year period [1996 to 2023].
The researchers also sought to investigate trends, early outcomes and long-term survival rates, the incidence of repeat valve interventions and patient prosthesis mismatch (PPM).
A total of 1708 (61% male) patients with an average age of 63 years were included with 1191 (69.7%) receiving a biological valve replacement.
The research found there were no short-term differences when comparing patients receiving biological and mechanical valves. However, patients who received mechanical valves had better long-term survival up to 13 years after having surgery.
Patients with a size 19mm biological valve replacement (a fairly small valve commonly used in females) had the worse long-term survival. Patients with a size 21mm mechanical valve had better survival compared to both size 19 and 21mm biological valves. The study confirmed that severe PPM is a significant risk factor for poor long-term survival.
Gianni Angelini, BHF Professor of Cardiac Surgery at the Bristol Medical School: Translational Health Sciences (THS), Director of the Bristol Heart Institute and corresponding author, said: “Our study has implications for decision-making in surgical heart valve replacements for patients aged between 50 and 70 years old. The evidence supporting better long-term survival in patients receiving a mechanical heart valve suggests the current trend favouring biological valves in this age bracket should be urgently reconsidered. The survival benefit is especially clear in smaller sized valves.”
The research team recommends the evaluation of the long-term benefits associated with mechanical valves, especially in smaller sizes, despite long-term blood thinners not being needed with biological valves.
Study limitations
The single-institution design, retrospective collection of data, and absence of randomisation make the study open to bias. The lack of echocardiographic information could potentially underestimate the incidence of structural valve failure. In terms of repeat valve interventions, only patients who underwent re-do surgical aortic valve replacement or valve in valve transcatheter aortic valve implantation (TAVI) at the BHI were included.
As the BHI is a supra-regional centre, it is very unlikely that many patients might have undergone reintervention in other institutions. The cause of death (cardiovascular/non cardiovascular) was not available.
South Africa’s National Department of Health is still to outline a clear contingency plan as a United States (US) funding freeze puts lives at risk, spells job losses, and presents threats to keeping HIV and TB under control.
The ripple effects of US President Donald Trump’s 90-day freeze of funding on foreign aid programmes have hit South Africa hard. The damage is being counted at multiple levels – even as some limited funding flows are being restored.
For the country, the fallout has heightened civil society’s calls for a prompt, implementable plan to fill the gaps in care and services. Also needed, they say, is clarity on longer-term strategies for greater self-sufficiency in the country’s HIV responses as donor-funded models look increasingly precarious. Such an argument for increased independence in Africa and the global south was made by president of the South African Medical Research Council (SAMRC), Professor Ntobeko Ntusi, writing in the journal Nature.
South Africa should have been better prepared and not caught off guard to be left in the position it now finds itself in, some beneficiaries of US-funded projects told Spotlight. They were speaking on condition of anonymity, given the risk of public comments jeopardising their prospects of having their funding restored.
The immediate need is to ensure that the country’s overburdened and under-resourced public clinic system is able to absorb the tens of thousands of people living with HIV who will have to use public facilities. This is partly because the NGOs they have relied on have been forced to close shop – virtually overnight. Clinics catering to specific groups, such as men who have sex with men, have been particularly hard hit.
South Africa is the largest global recipient of President’s Emergency Plan for Aids Relief (PEPFAR) funds. These funds make its way to South Africa through the United States Agency for International Development (USAID) and the Centers for Disease Control and Prevention (CDC). Through PEPFAR, USAID has been funding and supporting local NGOs and our Department of Health for around two decades. According to USAID’s website, it invested $5.6 billion (roughly R100 billion at the current rand/dollar exchange rate) between 2004 and 2020 towards prevention and treatment of HIV and TB in South Africa.
Trump’s initial executive order, signed on 20 January, halted funding received via USAID. USAID is an agency of the US government that now falls under the State Department under the leadership of Secretary of State Marco Rubio. Since taking office, Trump has slated USAID as “corrupt” and run by “radical left lunatics”.
The Washington head offices of USAID were closed on Friday 7 February as per Trump’s orders and even as the 90-day review period had just got underway, signage on the building was being removed or taped over. Trump’s actions have now been challenged in courts with successful temporary blocks to his orders to place 2 200 USAID workers in the US on paid leave and to reinstate 500 US-based staff who were already placed on administrative leave from when the order was first signed. The situation is highly fluid and several court actions remain in progress.
Some limited relief
In South Africa, NGOs that received USAID funding remain largely in limbo. Although the United States mission in South Africa confirmed that some PEPFAR-funded services could continue in the country, it is subject to some relatively strict limitations and with no assurances of longer term support. As is clear from reporting by Bhekisisa, the process to get at least some funding to flow again to PEPFAR-supported projects is not straight forward.
There was some good news this week linked to PEPFAR-funding channelled through the CDC – a US federal agency under the Department of Health and Human Services. Following a court order, organisations getting these funds should for now be able to continue their work. However, the court process is far from over and the future prospects of NGOs that depend on CDC funds remains precarious.
Given these ongoing uncertainties and severe disruptions to cash flows, Spotlight understands that some large NGOs may have to close down, while others may have to drastically reduce their services. As reported by Spotlight and GroundUp, several NGOs have appealed to the private sector for assistance. As it stands, thousands of people employed or contracted by local NGOs face the loss of their jobs, cut-backs and deepening anxiety over income security. These people include community health workers, peer counsellors, patient navigators, community activists and advocates, support and administrative staff members, and contract workers who keep these organisations functioning.
At stake too are specialised services for so-called key populations such as sex workers, men who have sex with men, the LGBTQI+ community, and people who use drugs. Until recently, a focus on improving services for key populations was generally accepted, including by PEPFAR, to be the right strategy given the disproportionate risk of HIV infection in these groups. But under the Trump administration’s “anti-woke” agenda, it seems likely that many services aimed at key populations are set to be defunded.
A White House media note on 29 January made clear the US’s stance: “The previously announced 90-day pause and review of U.S. foreign aid is already paying dividends to our country and our people. We are rooting out waste. We are blocking woke programs. And we are exposing activities that run contrary to our national interests. None of this would be possible if these programs remained on autopilot.”
A timeline of the US aid cuts
20 January
90-day pause
In an executive order, US President Donald Trump orders a 90-day pause in US foreign development for “assessment of programmatic efficiencies and consistency with United States foreign policy”.
26 January
USAID funding paused
US Secretary of State Marco Rubio pauses all US foreign assistance funded by or through the State Department and US Agency for International Development (USAID) for review.
28 January
Waiver issued
Subject to certain conditions, Rubio issues a waiver stating: “Implementers of existing life-saving humanitarian assistance programs should continue or resume work if they have stopped.”
1 February
Waiver clarified
The extent of the January 28 waiver is clarified in a memo from the US Department of State.
5 February
Health portfolio committee briefing
South Africa’s Health Minister Dr Aaron Motsoaledi briefs Parliament on the US funding cuts and their impact on healthcare services.
7 February
South Africa singled out
In an executive order applying only to South Africa, Trump orders that “the United States shall not provide aid or assistance to South Africa”.
10 February
Waiver still applies
The US mission in South Africa releases an FAQ in which they state that PEPFAR activities that fall under the limited waiver will resume despite the February 7 executive order.
12 February
CDC grants reinstated
The grants of NGOs receiving support through the CDC are reinstated following a court order issued in a US court.
Crisis of fear, silence, and uncertainty
Spotlight understands that staff of affected NGOs have essentially been forbidden from speaking publicly about the 90-day funding freeze. Many declined to speak on the record to Spotlight, even anonymously – too afraid it might affect the decision on their funding after the 90-day review period.
According to an FAQ by the US mission in South Africa that was published on February 10, they have been communicating with the South African government, though it is not clear when this happened. Five days earlier on 5 February, Health Minister Dr Aaron Motsoaledi told Parliament’s Portfolio Committee that he had not had any official communication from the US government on the matter.
Figures from Motsoaledi’s presentation showed that in 2023/2024, PEPFAR funding to South Africa’s health department amounted to 17% of its spending on HIV. Funding totals R4.6 billion for staffing and R2.9 billion for running costs for NGOs. These NGOs include organisations working directly with people living with HIV, mobile units and youth organisations and programmes. PEPFAR focuses on the 27 districts in South Africa with the highest disease burden.
The health department did not respond to Spotlight’s questions on contingencies, or details of next steps to fill the funding gaps or how capacity and resources will be redirected to avert catastrophe. Motsoaledi did not give any of these details in his presentation to Parliament either.
What he did say was that since Trump’s executive order came into place, the health department had hosted a meeting with the provincial leads on HIV and TB; conducted assessments on the immediate impacts of the executive order; met with people living with HIV and engaged with SANAC to finalise a sustainability framework.
A collective of activist organisations, including the Health Justice Initiative, SECTION27, the Cancer Alliance, Treatment Action Campaign, Sweat, PSAM and the African Alliance, have pressed the Department of Health to create an “urgent co-ordinated emergency plan” along with an increased budget to avert a looming disaster.
The activists highlighted that despite the announcement by the Trump administration that some NGOs could apply for a waiver, many have had no practical way to do so without ways to communicate with their USAID contacts. This as USAID employees were placed under a work stop order and were shut out of their offices and denied access to their work emails.
The appeal from the collective also extends to protecting the work of academic and clinical research in the fields of HIV, TB, and cervical cancer that will also be affected by the funding freeze. As Spotlight reported, around 28% of the South African Medical Research Council’s budget for 2025/2026 was set to come from the United States government.
An ‘unreal world’
Professor Linda-Gail Bekker, chief executive officer at the Desmond Tutu Health Foundation, said Trump’s actions put in jeopardy the goal to finally have epidemic control of HIV – and right at the final hurdles.
“We have made amazing progress. And thank you to PEPFAR that helped us to get this far, but the work is not over. For the US to pull out at this point is a massive loss of investment; it’s also regression. It’s like getting to the end of a book but having the last chapters torn out before you can read it,” said Bekker.
She said PEPFAR funding has made it possible to build a formidable cohort of lay and professional people trained and dedicated to their roles that supported public healthcare in the most critical ways.
“These are individuals who distribute antiretrovirals, distribute pre-exposure prophylaxis, find and trace individuals who’ve been lost to care. They take services into communities, to outside of the health facilities, and made the effort to go the last mile to find those individuals – that is how you close down the epidemic,” Bekker said.
Her caution too is that loosening a grip on HIV control means potential surges in tuberculosis. “HIV and TB track together all the time, and an HIV epidemic that is once again out of control, almost certainly means what will follow is a TB epidemic that is out of control,” Bekker said.
Trump has created an “unreal world”, said Dr Andy Gray of the University of KwaZulu-Natal, who has also worked with the World Health Organization (WHO) in various capacities over two decades. “People are being held to ransom; and people are scared.”
“We have always been used to the oscillation between the United States’ Republican and Democratic administrations; things may be a little uncomfortable or there may be some disruption, but not this ‘let’s burn down the house’ approach taken by the Trump administration,” he said.
“There is no consideration of human rights or for human beings anywhere in the world, including America,” he added, pointing out too that the CDC has for the first time in 60 years been instructed to cease publishing weekly mortality and morbidity data, despite a breakout of avian flu (H5) in the country.
For Gray, South Africa’s strategic health response in the wake of this crisis should be to shift from a donor-funded model. His concern, however, is that with a stretched South African purse and with competing priorities, the HIV response will slip down the list.
Gray said that better self-sufficiency comes from eliminating waste, investing in employing the right people in the right jobs as well as investing in efficient systems.
He added that National Treasury will have to redirect money for the interim shortfall left by the US funding freeze, and provinces will have to step up by getting their houses in order.
South Africa, he warned, should ready itself for the “worst case scenario” once the 90-day review period is up.
SANAC response
The South African National AIDS Council (SANAC) role is meant to bring together government, civil society and the private sector to create a collective response to HIV, TB and STIs in South Africa. But if there is a crisis strategy from the council, it has not yet been announced.
SANAC head of communications, Nelson Dlamini, said that they have been left in a position of not being able to engage publicly because they haven’t had any direct communication with PEPFAR’s and USAID representatives based in Pretoria.
“PEPFAR is a government-to-government agreement and there ought to be official communication with the government of South Africa so we know what this means for our working relationship, but nothing has been forthcoming,” said Dlamini. “SANAC is a co-ordinator so we have to still coordinate. We are engaging in the background with relevant structures but we can’t say we are doing X, Y, Z till we have a sit down with PEPFAR,” he said.
In a randomised clinical trial, researchers from Huntsman Cancer Institute at the University of Utah (the U) have found that short-course, higher dose vaginal brachytherapy for endometrial cancer had similar effectiveness to more frequent, lower dose sessions.
Gita Suneja, MD, MS, physician-scientist at Huntsman Cancer Institute and professor of radiation oncology at the U, is the first author of the SAVE trial report – which stands for, Short-Course Adjuvant Vaginal Cuff Brachytherapy in Early Endometrial Cancer Compared with Standard of Care.
“There isn’t high quality-data on optimal dose and schedule for brachytherapy treatments. Because of this, practice patterns really vary,” says Suneja. “The SAVE trial sought to try to lower the number of treatments that patients were receiving but maintain short-term quality of life and disease control.”
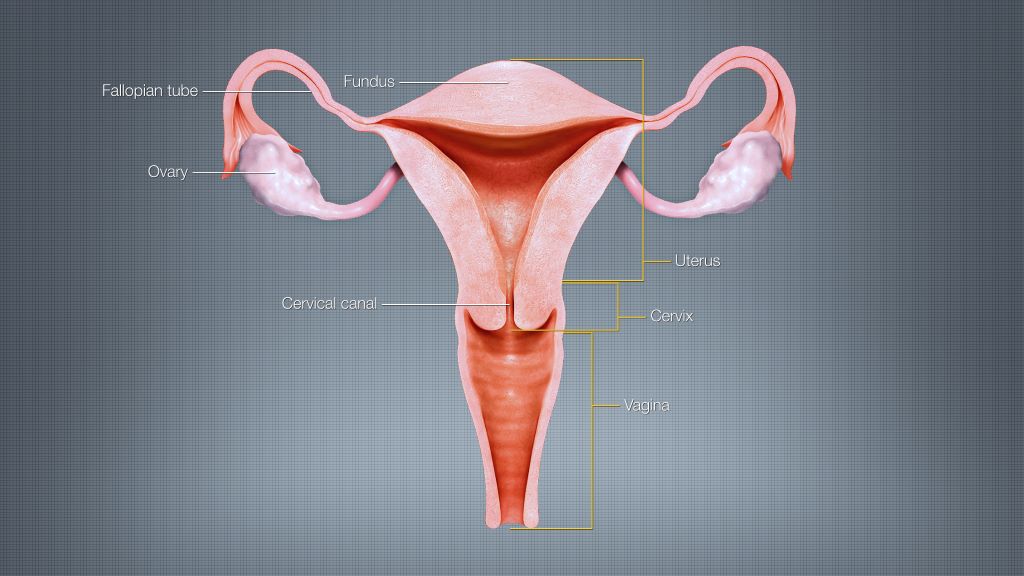
Endometrial cancer is a disease that begins in the lining of the uterus. The primary treatment for endometrial cancer is surgery, including the removal of the uterus, cervix, and upper vagina. Brachytherapy, a form of internal radiation, is used as a secondary treatment to prevent the cancer’s return. Patients receiving vaginal cuff brachytherapy are treated with internal radiation by way of an applicator in the vaginal cavity.
The SAVE trial compared two groups who received different treatment doses over a varying number of sessions. The control group received the standard treatment – between three to five appointments with lower doses. The experimental group received higher doses of radiation in just two sessions.
“The study outcomes will help improve cancer care for Huntsman Cancer Institute patients across the five states of the Mountain West.”
Gita Suneja, MD, MS
The researchers found similarly effective short-term outcomes and few acute toxicities for the patients in the experimental group.
David Gaffney, MD, PhD, FACR, FABS, FASTRO, physician-scientist at Huntsman Cancer Institute and professor of radiation oncology at the U, developed the idea for the SAVE study after seeing patient need. According to the American Cancer Society, endometrial cancer is the most common cancer of the female reproductive organs. Incidence is on the rise, as is the mortality rate.
“It is a big win when we can preserve good outcomes and make cancer care easier,” says Gaffney.
People with type 1 diabetes require continuous insulin treatment and must regularly measure their glucose levels. With open-loop therapies*, insulin administration is manually controlled, while hybrid closed-loop systems* automatically regulate insulin delivery. A study with the involvement of the German Center for Diabetes Research showed that hybrid closed-loop systems offer improved long-term blood sugar values (HbA1c levels) and a lower risk of hypoglycaemic coma, but lead to a higher rate of diabetic ketoacidosis. The results were published in The Lancet Diabetes & Endocrinology.
Despite advances in insulin therapy, many people do not achieve their blood glucose targets and have a high risk of complications. Until now, the effect of insulin delivery in hybrid closed-loop systems on the risk of acute diabetes complications in people with type 1 diabetes has been unclear. Researchers have therefore now investigated whether the rates of severe hypoglycaemia and diabetic ketoacidosis are lower with hybrid closed-loop insulin therapy compared with sensor-augmented (open-loop) pump therapy.
Study with Nearly 14 000 Participants
In order to answer this question, the researchers, led by Professor Beate Karges, Faculty of Medicine at the RWTH Aachen, examined the data of nearly 14 000 participants. The study involved young people with type 1 diabetes from 250 diabetes centres in Germany, Austria, Switzerland, and Luxembourg. The participants were aged 2 to 20 years and had a type 1 diabetes duration of more than one year. They were identified from the Diabetes Prospective Follow-up Registry (DPV)**. The primary objectives of the study were to determine the rates of severe hypoglycaemia and ketoacidosis. Differences in HbA1c levels, time in the target range of 3.9 to 10.0mmol/L (70–180mg/dL), and fluctuations in blood sugar were also investigated. The data of 13 922 patients (51% male) were included in the analysis. Median age was 13.2 years; 7088 used a hybrid closed-loop system and 6834 used an open-loop system. The median observation time was 1.6 years.
Lower Rate of Hypoglycaemic Coma and More Ketoacidosis Events with Hybrid Closed-Loop Therapies
The results: People using hybrid closed-loop therapy had a significantly lower rate of rate of hypoglycaemic coma (0.62 per 100 patient-years) than those using open-loop therapy (0.91 per 100 patient-years). Furthermore, patients in the hybrid closed-loop group had a significantly lower HbA1c level (7.34% versus 7.50%). They had a higher percentage of time in the target glucose range of 3.9 to 10.0 mmol/L (64% versus 52% of the time). Their glycaemic variability was also lower (coefficient of variation of 35.4% versus 38.3%). There was no significant difference in the rate of severe hypoglycaemia.
However, individuals using a hybrid closed-loop system had a higher rate of ketoacidosis (1.74 events per 100 patient-years) than those using open-loop therapy (0.96 per 100 patient-years). The rate of ketoacidosis was particularly high in people with an HbA1c level of 8.5% or higher in the closed-loop therapy group (5.25 per 100 patient-years). In the comparison group, a rate of 1.53 events per 100 patient-years was observed.
Recommendation: Monitor Ketone Bodies Closely
Due to the higher risk of ketoacidosis, it is important to provide patients with targeted information and, in case of potential metabolic decompensation, to closely monitor ketone bodies in the blood or urine in order to prevent such adverse events, emphasize the authors of the study.
Data from 8843 women diagnosed with preeclampsia during pregnancy showed that existing risk prediction models are most accurate only in the days after diagnosis
Photo by Shvets Production on Pexels
The existing prediction models for severe complications of preeclampsia are most accurate only in the two days after hospital admission, with deteriorating performance over time, according to a new study published February 4th in the open-access journalPLOS Medicineby Henk Groen of University of Groningen, the Netherlands, and colleagues.
Preeclampsia is a potentially life-threatening condition that can occur during pregnancy; of women diagnosed with preeclampsia, 5-20% will develop severe complications. Two existing PIERS (Pre-eclampsia Integrated Estimate of RiSk) models, PIERS Machine Learning (PIERS-ML) and the logistic-regression-based fullPIERS, are designed to identify individuals at greatest or least risk of adverse maternal outcomes in the 48 hours following hospital admission for preeclampsia. However, both models are regularly used for ongoing assessment beyond the first 48 hours.
In the new study, researchers used data from 8843 women diagnosed with preeclampsia at a median gestational age of 36 weeks between 2003 and 2016. Data included PIERS-ML and fullPIERS assessments as well as health outcomes.
The study found that neither the PIERS-ML nor fullPIERS model maintained good performance over time for repeated risk stratification in women with preeclampsia. The PIERS-ML remained generally good at identifying the very high-risk and very-low risk groups over time, but performance of the larger high-risk and low-risk groups deteriorated significantly after 48 hours. The fullPIERS model underperformed compared to the PIERS-ML model.
“Since there are no better options, clinicians may still use these two models for ongoing assessments after the first admission with pre-eclampsia, but the predictions should be treated with increasing caution as the pregnancy progresses,” the authors say. More prediction models are needed that perform well over time, they add.
The authors add, “Pregnancy hypertension outcome prediction models were designed and validated for initial assessment of risks for mothers; this study shows that such ‘static’ models if used repeatedly over days yield increasingly inaccurate predictions.”