Glucagon-like peptide 1 receptor agonists (GLP1RA) – medications for type 2 diabetes and obesity that have recently been making headlines due to a rise in popularity as weight loss agents – have been linked with behavioural side effects. A large population-based analysis in Diabetes, Obesity and Metabolismassessed whether certain genetic variants might help explain these effects.
GLP1RA mimic the GLP-1 hormone in the body that helps control insulin and blood glucose levels and promotes feelings of satiety. GLP-1 binds to GLP1R on cells in the brain and pancreas.
Observational and epidemiological studies have shown that there may be neutral or protective effects of GLP1RAs on mental health symptoms. However, a study based on individuals taking GLP1RA suggests there is increased prescription of anti-depressants when used for treatment of diabetes. Early evidence in animal models suggest GLP1RA may decrease depressive and anxious symptoms, potentially presenting new treatment pathways; however, comparing these studies to human clinical evidence will not be possible for some time.
For the analysis, investigators examined common genetic variants in the GLP1R gene in 408 774 white British, 50 314 white European, 7 667 South Asian, 10 437 multiple ancestry, and 7641 African-Caribbean individuals.
Variants in the GLP1R gene had consistent associations with cardiometabolic traits (body mass index, blood pressure, and type 2 diabetes) across ancestries. GLP1R variants were also linked with risk-taking behavior, mood instability, chronic pain, and anxiety in most ancestries, but the results were less consistent. The genetic variants influencing cardiometabolic traits were separate from those influencing behavioral changes and separate from those influencing expression levels of the GLP1R gene.
The findings suggest that any observed behavioral changes with GLP1RA are likely not acting directly through GLP1R.
“Whilst it is not possible to directly compare genetic findings to the effects of a drug, our results suggest that behavioural changes are unlikely to be a direct result of the GLPRAs. Exactly how these indirect effects are occurring is currently unclear,” said corresponding author Rona J. Strawbridge, PhD, of the University of Glasgow, in the UK.
A study conducted at Turku PET Centre in Finland and published in showed that changes in the functioning of opioid neurotransmitters in the brain may underlie anorexia.
Anorexia nervosa is a serious psychiatric disorder characterised by restricted eating, fear of gaining weight, and body image disturbances, which may lead to severe malnutrition, depression and anxiety. This new study from Turku PET Centre, published in Molecular Psychiatry, shows how changes in neurotransmitter function in the brain may underlie anorexia.
“Opioid neurotransmission regulates appetite and pleasure in the brain. In patients with anorexia nervosa, the brain’s opioidergic tone was elevated in comparison with healthy control subjects. Previously we have shown that in obese patients the activity of the tone of this system is lowered. It is likely that the actions of these molecules regulate both the loss and increase in appetite,” says Professor Pirjo Nuutila from the University of Turku.
Number of opioid receptors in the brain (top row) and sugar intake (bottom row) in patients with anorexia nervosa. Credit: University of Turku
In addition, the researchers measured the brain’s glucose uptake. The brain accounts for about 20% of the body’s total energy consumption, so the researchers were interested in how a reduction in the energy intake affects the brain’s energy balance in anorexia.
“The brains of patients with anorexia nervosa used a similar amount of glucose as the brains of the healthy control subjects. Although being underweight burdens physiology in many ways, the brain tries to protect itself and maintain its ability to function for as long as possible,” says Professor Lauri Nummenmaa from Turku PET Centre and continues:
“The brain regulates appetite and feeding, and changes in brain function are associated with both obesity and low body weight. Since changes in opioid activity in the brain are also connected to anxiety and depression, our findings may explain the emotional symptoms and mood changes associated with anorexia nervosa.”
Researchers following nearly 1000 people with post-COVID-19 syndrome found few changes to their symptoms in the second year of illness
Photo by Usman Yousaf on Unsplash
Two-thirds of people with post-COVID-19 syndrome have persistent, objective symptoms – including reduced physical exercise capacity and reduced cognitive test performances – for a year or more, with no major changes in symptom clusters during the second year of their illness, according to a new study published January 23rd in the open-access journal PLOS Medicineby Winfried Kern of Freiburg University, Germany, and colleagues.
Self-reported health problems following SARS-CoV-2 infection have commonly been described and may persist for months. However, the long-term prognosis of post-COVID-19 syndrome (PCS) is unknown.
In the new study, researchers studied 982 people aged 18 to 65 who had previously been identified as having PCS, as well as 576 controls. All participants visited one of several university health centers in southwestern Germany for comprehensive assessments, including neurocognitive, cardiopulmonary exercise, and laboratory testing.
The predominant symptom clusters among people with PCS were fatigue/exhaustion, neurocognitive disturbances, chest symptoms/breathlessness, and anxiety/depression/sleep problems. Nearly 68% of people who originally reported PCS still struggled with symptoms in the second year. Exercise intolerance with post-exertional malaise was reported by 35.6% of people with persistent PCS, and these people had worse outcomes and more severe symptoms. People with lower educational attainment, obesity, or more severe illness during the initial COVID-19 infection were also at higher risk of prolonged symptoms.
When they looked at objective measures of health and cognition, the team found that people with persistent PCS had significant reductions in handgrip strength, maximal oxygen consumption, and ventilatory efficiency. Patients with persistent PCS and post-exertional malaise scored lower than control patients on cognitive tests measuring memory, attention, and processing speed; however, the researchers point out that they had no data on cognition before acute COVID-19 infection. The team was not able to identify differences in cardiac function or laboratory values, including tests of viral persistence.
“The results call for the inclusion of cognitive and exercise testing in the clinical evaluation and monitoring of patients with suspected PCS,” the authors say. “Observational studies with longer follow-up are urgently needed to evaluate factors for improvement and non-recovery from PCS.”
The authors add, “Grave symptoms with mental and physical exercise dysfunction, but no laboratory markers in Long Covid/post-Covid syndrome.”
Red Blood Cell Infected with Malaria Parasites
Colourised scanning electron micrograph of red blood cell infected with malaria parasites (teal). The small bumps on the infected cell show how the parasite remodels its host cell by forming protrusions called ‘knobs’ on the surface, enabling it to avoid destruction and cause inflammation. Uninfected cells (red) have smoother surfaces. Credit: NIAID
Indiana University School of Medicine researchers and their collaborators in Uganda at the Makerere University School of Medicine have uncovered a significant connection between elevated uric acid levels and life-threatening outcomes in children with severe malaria.
Published in Nature Medicine, the study identified hyperuricaemia – high uric acid levels – as a potential contributor to increased mortality and long-term neurodevelopmental challenges in children with severe malaria. These findings open the door to future research that could improve treatment strategies for children affected by severe malaria, a disease caused by mosquito-transmitted parasites and a leading cause of death in African children.
“Our findings show that hyperuricemia is strongly associated with death in the hospital and after discharge and with long-term cognitive impairment in children with severe malaria,” said Chandy C. John, MD, paediatrics professor at IU School of Medicine, who co-led the study. “We also showed several mechanisms by which hyperuricaemia may lead to these outcomes, suggesting that hyperuricaemia is not just associated with bad outcomes but may contribute to them.”
The researchers analysed data from two independent groups of children with severe malaria in Uganda and found that 25% had hyperuricaemia. This condition is caused by excess uric acid, which is a harmful body waste substance found in blood. The primary drivers of hyperuricaemia in study participants were broken-down infected red blood cells and kidney injury, which reduces the body’s ability to get rid of the extra uric acid.
In the study, hyperuricemia was linked to four negative outcomes in children with severe malaria: serious health complications like coma and anaemia, a higher risk of death during hospitalisation, a higher risk of death after discharge from the hospital, and long-term cognitive impairment in survivors.
The study also revealed that children with hyperuricemia had more harmful gut bacteria, which can cross the injured gut lining and cause sepsis. Together, these findings highlight a need for clinical trials to test the effectiveness of uric acid-lowering medications as an additional treatment for severe malaria.
“Additional studies are needed to determine whether lowering uric acid in children with severe malaria might reduce hospital deaths, post-discharge deaths and long-term cognitive impairment,” said Andrea Conroy, PhD, associate professor of paediatrics at the IU School of Medicine and co-leader of the study. “Our hope is that these studies will provide new insights and potentially lead to improved treatments that save lives.”
This research builds on the team’s recent discovery of partial resistance to the primary treatment for malaria in African children with severe malaria. Both studies underscore the importance of prioritizing new strategies to combat malaria, which affected 263 million people and caused nearly 600,000 deaths worldwide in 2023.
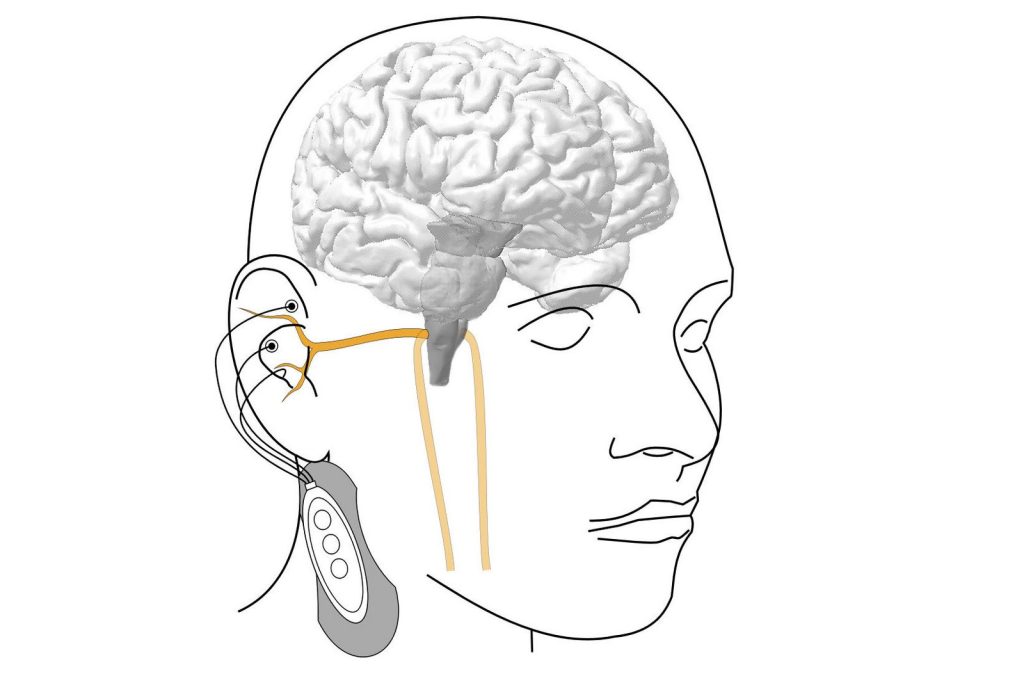
A small device worn on the body can stimulate the nervous system via electrodes on the ear. Credit: Vienna University of Technology.
Various diseases can be treated by stimulating the vagus nerve in the ear with electrical signals, but the results can be ‘hit or miss’. A study recently published in Frontiers in Physiology has now shown that the electrical signals must be synchronised with the body’s natural rhythms – heartbeat and breathing.
Some health problems, from chronic pain and inflammation to neurological diseases, can also be treated by nerve stimulation, for example with the help of electrodes that are attached to the ear and activate the vagus nerve. This method is sometimes referred to as an ‘electric pill’.
However, vagus nerve stimulation does not always work the way it is supposed to. A study conducted by TU Wien (Vienna) in cooperation with the Vienna Private Clinic now shows how this can be improved: Experiments demonstrate that the effect is very good when the electrical stimulation is synchronised with the body’s natural rhythms – the actual heartbeat and breathing.
The ‘electric pill’ for the parasympathetic nervous system
The vagus nerve plays an important role in our body: it is the longest nerve of the parasympathetic nervous system, the part of the nervous system that is significantly involved in the precise control of the internal organs and blood circulation, and is responsible for recovery and building up the body’s own reserves. A branch of the vagus nerve also leads from the brain directly into the ear, which is why small electrodes in the ear can be used to activate the vagus nerve, stimulate the brain and thus influence various functions of the body.
“However, it turns out that this stimulation does not always produce the expected results,” says Prof Eugenijus Kaniusas from the Institute of Biomedical Electronics at TU Wien. “The electrical stimulation does not have an effect on the nervous system at all times. You could say that the brain is just not always listening. It’s as if there is a gate to the control centre of the nervous system that is sometimes open and then closed again, and this can change in less than a second.”
Five people have now been examined in a pilot study. Their vagus nerve was electrically activated to lower their heart rate. It is already known from previous studies that heart rate is a potential indicator of whether stimulation therapy is beneficial or not.
It was shown that the temporal connection between the stimulation and the heartbeat plays a decisive role. If the vagus nerve is stimulated at a rhythm that is not synchronised with the heartbeat, hardly any effect can be observed. However, if the stimulation signals are always applied when the heart is contracting (during systole), a strong effect can be observed – much stronger than if stimulation is applied during the relaxation phase of the heart, diastole.
Breathing is also important in this context: the stimulation was significantly more effective during the inhalation phase than during the exhalation phase.
“Our results show that synchronising vagus nerve stimulation with the heartbeat and breathing rhythm significantly increases effectiveness. This could help to improve the success of treatment for chronic illnesses, especially for those who have not previously responded to this therapy for reasons that are as yet unexplained,” says Eugenijus Kaniusas.
Larger clinical studies to follow
If nerve stimulation can be customised electronically so that it is tailored to the body’s own individual rhythms at any given time, it should be possible to achieve significantly greater successes than has been possible to date. Future studies should examine larger and clinically relevant patient groups and develop even more precise algorithms in order to be able to tailor the stimulation even more precisely to individual needs.
“This technology could be an effective and non-invasive way of modulating the autonomic nervous system in a targeted and gentle manner – a potential milestone in the neuromodulatory treatment of various chronic diseases,” believes Dr Joszef Constantin Szeles from the Vienna Private Clinic.
Dermoscopy of an approximately 16mm nodular basal cell carcinoma showing telangiectatic vessels. Source: Wikimedia CC4.0
Basal cell carcinomas, the most common form of skin cancer, occur in chronically sun-exposed areas such as the face. Locally advanced tumours in particular can be difficult to treat surgically. A research team from MedUni Vienna and University Hospital Vienna has now investigated the effectiveness of a new type of therapy and achieved promising results: The active substance TVEC led to a reduction in the size of the basal cell carcinoma in all study participants, which not only improved surgical removal, but also led to a complete regression of the tumour in some of the patients. The study was published in the top journal Nature Cancer.
In the study Talimogene Laherparepvec (TVEC) was used, which has so far only been approved for the treatment of superficial melanoma metastases. TVEC is a genetically modified herpes simplex virus that specifically destroys tumour cells and simultaneously activates the immune system. The aim of the study was to reduce the size of the tumour before a planned operation so that patients would not suffer any functional or cosmetic restrictions after the procedure. The study included 18 patients who would have required a flap or skin graft due to the size and localisation of their basal cell carcinoma. They each received six intralesional injections of TVEC over a period of 13 weeks before the tumour was surgically removed.
“This enabled the tumour to be reduced in size in half of the patients to such an extent that surgery with direct wound closure was possible. In a third of the cases, the subsequent histological examination even showed no more living tumour cells. All treated tumours at least became smaller, and no tumour grew further under the therapy. The treatment was well tolerated by the patients,” says the principal investigator Christoph Höller, Head of the Skin Tumour Centre at the Department of Dermatology, summarising the results. “The new treatment option for basal cell carcinoma can not only simplify surgery, but also help to avoid disfiguring operations and functional limitations,” adds first author Julia Ressler, also from the Department of Dermatology. In addition to the clinical studies, the researchers from the Department of Dermatology, in cooperation with the St. Anna Children’s Hospital, carried out comprehensive analyses that show that the immune defence in the tumour tissue is strengthened in the course of therapy with TVEC.
These results suggest that TVEC could be a promising option for the neoadjuvant, i.e. pre-surgical, treatment of basal cell carcinoma, particularly in patients for whom major surgery should be avoided. Further studies are to follow in order to confirm the benefits of this new option in a larger patient population.
A study based on interviews with primary care physicians has found that treating patients who were adopted is challenging due to limited access to their family medical history. The study, published in Annals of Family Medicine, also found that there was a desire by physicians to fill the information using genetic testing.
Adopted individuals often only have limited information about their biological family, or even none at all, complicating their treatment. The growing availability and popularity of direct-to-consumer genetic testing kits amplifies the need for physicians to be prepared to address genetic testing for adoptees with limited family medical history. To address this, the present study explored the approaches of primary care physicians when caring for adult adopted patients with limited family medical history.
In-depth interviews were conducted by the researchers, including hypothetical clinical scenarios, with 23 primary care physicians from Rhode Island and Minnesota to understand their experiences, practices, knowledge, and training gaps when addressing limited family medical history and adoption-related issues.
The researchers found that primary care physicians report knowledge gaps and receive little training or resources on adult adoptees with limited family medical history. As a result, they seek guidance around appropriate preventative screening and genetic testing. Limited interaction with adoptees compared to non-adopted patients also influenced perceptions. There was also an over-reliance on stereotypes and the danger of inaccurate media representation affecting how physicians interacted with adoptee patients. Likewise, those physicians who had experience with adoption might be at risk of over-generalising those experiences, especially given how heterogeneous adoptees are as a population.
Furthermore, the researchers found that mental illness and trauma are under-recognised and under-addressed. Care for adoptees includes trauma-informed care which can address factors such as loss, grief, identity development, and to helping adoptees in searching for biological family, reunion, or with complex family dynamics.
To make matters worse, primary care physicians often obtain family medical history imprecisely, risking miscommunication, microaggressions, and damage to the patient-physician relationship.
The findings of this study highlight the significant gaps in knowledge and training for primary care physicians caring for adult adopted patients with limited family medical history. Addressing these gaps may improve the quality of care and strengthen physician-patient relationships.
A randomised crossover trial found minimal difference between blood pressure (BP) readings obtained in public spaces versus those taken in private offices. These findings suggest that public spaces can be an acceptable setting for BP screenings, despite prior clinical guideline recommendations advising quiet settings for BP measurement. The results are published in Annals of Internal Medicine.
Researchers from Johns Hopkins University randomly assigned 108 adults in Baltimore, MD to the order in which they had triplicate BP measurements in each of 3 settings: 1) private quiet office (private quiet [reference]); 2) noisy public space (public loud); and 3) noisy public space plus earplugs (public quiet) to evaluate the effect of noise and public environment on BP readings. The primary outcomes were differences between the mean BPs obtained in each public setting with those obtained in the private setting. The average noise level in the private quiet setting was 37 decibels (dB) and the average noise level in the public setting was 74dB.
In the private quiet setting, the average systolic BP (SBP) and diastolic BP (DBP) were 128.9 and 74.2mmHg, respectively. In the public loud setting, the mean SBP and DBP were 128.3 and 75.9mmHg and in the public quiet setting, the mean SBP and DPB were 129.0 and 75.7mmHg. The results indicate that the differences in BP readings in public, loud spaces versus the clinically recommended setting of a private office are small and not clinically significant. The researchers say these results support the implementation of mass hypertension-screening programs in settings including supermarkets, places of worship and schools.
SCP – Dr Winter performing a CT-guided interventional procedure
World Cancer Day, observed every 4 February, aims to raise awareness about cancer, encourage prevention and look at ways of improving a cancer patient’s quality of life. Interventional radiology plays a significant role in pain management for cancer patients.
Traditionally, radiology was used for diagnosing the cause of the pain but interventional radiology has changed this paradigm. Since American radiologist Charles Dotter, first used a guidewire and catheter to perform an interventional procedure in 1964, radiologists have become actively involved in intervention, including interventions for pain management. Today, many minimally invasive procedures are routinely performed in busy radiology departments.
Dr Arthur Winter, a radiologist at SCP Radiology says, ‘Interventional radiology has developed rapidly. Pain management procedures are becoming a daily part of busy radiology departments and play a crucial role in managing pain for cancer patients.
‘Cancer-related pain can be a significant burden, affecting patients’ quality of life and hindering their ability to carry out daily activities,’ says Dr Winter. ‘Radiology offers various techniques and treatments that help alleviate this pain effectively. These therapeutic interventions in pain management include image-guided interventional radiology procedures and radiation therapy.’
Understanding pain
Pain is a signal from the nervous system to let you know that something is wrong in your body. It is transmitted in a complex interaction between specialised nerves, the spinal cord and the brain. It can take many forms, be localised to one part of the body or appear to be widespread.
The nature of cancer pain
Cancer pain can arise from multiple sources, including the tumour itself, which may invade or compress surrounding tissues, organs or nerves. Metastases, the spread of cancer to other parts of the body, can also cause significant pain. Additionally, pain can result from the treatment of cancer, such as chemotherapy and radiation therapy.
Multidisciplinary approach to pain management
Effective pain management for cancer patients requires a comprehensive, multidisciplinary approach. Oncologists, radiologists, pain specialists and other healthcare providers collaborate to develop individualised care plans. Radiology is essential in both the diagnostic and therapeutic phases of this process, providing crucial insights and treatment options.
These personalised care plans, tailored to each patient’s needs, ensure:
Accurate diagnosis and identification of pain source or sources
Targeted and effective treatment interventions
Ongoing monitoring and adjustment of pain management strategies
Imaging techniques
Diagnostic radiology initially uses various imaging techniques to identify the source and extent of pain in cancer patients. These techniques include: X-rays, CT scans, MRI, PET scans and ultrasound.
By identifying the precise location and cause of pain, radiology can help:
Determine the most appropriate interventions, such as surgery, radiation therapy or minimally invasive interventional procedures
Monitor the effectiveness of pain management strategies and make necessary adjustments
Avoid unnecessary treatments that may not address the underlying cause of pain
Interventional radiology
Interventional radiology uses minimally invasive techniques to diagnose and treat various conditions and, for cancer patients experiencing pain, it offers several effective treatments:
Radiofrequency ablation (RFA): This uses heat, generated by radiofrequency energy to destroy cancerous tissues – often to treat painful bone metastases or tumours that are difficult to reach surgically
Cryoablation: Involves freezing cancerous tissues to destroy them. It is particularly useful for treating painful bone or soft tissue tumours, providing rapid pain relief
Nerve blocks: Involve the injection of anaesthetic agents or steroids near specific nerves to block pain signals. They can provide significant pain relief for patients with nerve-related pain
Palliative radiation therapy
In this instance, radiologists are involved with planning imaging only. The actual radiotherapy is performed by the radiation therapist, who works under the supervision of a radiation oncologist. Palliative radiation therapy is specifically designed to relieve symptoms and improve the quality of life for cancer patients. It focuses on pain control and symptom management rather than curing the disease.
Radiation oncologists deliver targeted doses of radiation to cancerous tissues, this palliative radiation therapy can help:
Reduce tumour size, alleviating pressure on surrounding tissues and nerves
Control bleeding or ulceration caused by tumours
Provide rapid pain relief, often within days to weeks of treatment
Improving quality of life
Dr Winter highlights that chronic pain can significantly diminish quality of life and contribute to depression, particularly in patients with underlying cancer. ‘These patients, in particular, should be considered for interventional procedures. For instance, there are highly effective treatments available to manage pain associated with pancreatic and pelvic cancers’.
‘Specialists, such as oncologists and neurologists, acknowledge the significant role of interventional radiology in pain management and collaborate closely with us to support their patients. As a rapidly advancing branch of radiology, it provides minimally invasive solutions and it is incredibly rewarding to witness patients regain their quality of life through effective symptom relief.’
Among the 85 000 undergraduate applications for 2025 Wits received for 2025, the single most-applied for degree was for the Bachelor of Medicine and Bachelor of Surgery (MBBCh). Of these applications, the university could only register around 6000 first-year students. These students represent the best of the best, earning their place in one of Africa’s most competitive academic environments, with an average of over five distinctions per student in their matric results.
From KZN, Glenwood High School’s Brydyn Le’Jean Barnabas, who was offered a place to study MBBCh, says, “I’ve been hearing from friends and family that this is such a prestigious university. It’s not only backed by impressive statistics but also has a rich culture and heritage, having been around for decades. Compared to other universities, it’s truly a privilege to be here. When I received my acceptance letter, my heart dropped – not just with joy but with gratitude for this opportunity.”
Bachelor of Pharmacy was also a popular degree, coming in at the fifth most applied-for.
Recent enrolment trend assessments indicate that the majority of students offered a place at Wits have achieved an Admission Point Score (APS) exceeding 30, with most scoring 34 or higher. The minimum APS required for degree programmes at Wits is 30, making entry into the university a significant accomplishment.
Wits continues to uphold its reputation as a hub for academic excellence and innovation, attracting top-performing students from across the country and the continent. The university remains committed to nurturing the next generation of leaders, thinkers, and innovators.
For more information about the experiences of first-year students and why they chose Wits, read more here: Wits News.