Scientists at Université de Montréal and its affiliated Montreal Clinical Research Institute (IRCM) have uncovered unique roles for a protein complex in the structural organisation and function of brain cell connectivity, as well as in specific cognitive behaviours.
The work by a team led by Hideto Takahashi, director of the IRCM’s synapse development and plasticity research unit, in collaboration with Steven Connor’s team at York University and Masanori Tachikawa’s team at Japan’s Tokushima University is published in The EMBO Journal.
Although defects in synapse organisation are linked to many neuropsychiatric conditions, the mechanisms responsible for this organisation are poorly understood. The new study’s findings could provide valuable therapeutic insights, the researchers believe.
Two goals are important to bear in mind with this research, said Takahashi, an associate research medical professor in molecular biology and neuroscience at UdeM.
“One is to uncover novel molecular mechanisms for brain cell communication,” he said. “The other is to develop a new unique animal model of anxiety disorders displaying panic disorder- and agoraphobia-like behaviours, which helps us develop new therapeutic strategies.”
Understanding the mechanisms
Synapses are essential for neuronal signal transmission and brain functions. Defects in excitatory synapses, which activate signal transmission to target neurons, and those in synaptic molecules predispose to many mental illnesses.
Takahashi’s team has previously discovered a new protein complex within the synaptic junction, called TrkC-PTPσ, which is only found in excitatory synapses. The genes coding for TrkC (NTRK3) and PTPσ (PTPRS) are associated with anxiety disorders and autism, respectively. However, the mechanisms by which this complex regulates synapse development and contributes to cognitive functions are unknown.
The work carried out in the new study by first author Husam Khaled, a doctoral student in Takahashi’s laboratory, showed that the TrkC-PTPσ complex regulates the structural and functional maturation of excitatory synapses by regulating the phosphorylation, a biochemical protein modification, of many synaptic proteins, while disruption of this complex causes specific behavioural defects in mice.
Building blocks of the brain
Neurons are the building blocks of the brain and the nervous system that are responsible for sending and receiving signals that control the brain and body functions. Neighbouring neurons communicate through synapses, which act like bridges that allow the passage of signals between them.
This process is essential for proper brain functions such as learning, memory and cognition. Defects in synapses or their components can disrupt communication between neurons, and lead to various brain disorders.
By generating mice with specific genetic mutations that disrupt the TrkC-PTPσ complex, Takahashi’s team uncovered the unique functions of this complex. They demonstrated that this complex regulates the phosphorylation of many proteins involved in synapse structure and organisation.
High-resolution imaging of the mutant mice brains revealed abnormal synapse organisation, and further study of their signaling properties showed an increase in inactive synapses with defects in signal transmission. Observing the behaviour of the mutant mice, the scientists saw that they exhibited elevated levels of anxiety, especially enhanced avoidance in unfamiliar conditions, and impaired social behaviours.
Attention deficit/hyperactivity disorder – also known as ADHD – is typically thought of as a childhood condition. But more adults are realising that their struggles with attention, focus and restlessness could in fact be undiagnosed ADHD, thanks in large part to trending social media videos racking up millions of views.
A new national survey of 1000 American adults commissioned by The Ohio State University Wexner Medical Center and College of Medicine finds that 25% of adults now suspect they may have undiagnosed ADHD. But what worries mental health experts is that only 13% of survey respondents have shared their suspicions with their doctor.
That’s raising concerns about the consequences of self-diagnosis leading to incorrect treatment.
“Anxiety, depression and ADHD – all these things can look a lot alike, but the wrong treatment can make things worse instead of helping that person feel better and improving their functioning,” said psychologist Justin Barterian, PhD, clinical assistant professor in Ohio State’s Department of Psychiatry and Behavioral Health.
An estimated 4.4% of people ages 18 to 44 have ADHD, and some people aren’t diagnosed until they’re older, Barterian said.
“There’s definitely more awareness of how it can continue to affect folks into adulthood and a lot of people who are realising, once their kids have been diagnosed, that they fit these symptoms as well, given that it’s a genetic disorder,” Barterian said.
The survey found that younger adults are more likely to believe they have undiagnosed ADHD than older generations, and they’re also more likely to do something about it.
Barterian said that should include seeing a medical professional, usually their primary care provider, to receive a referral to a mental health expert to be thoroughly evaluated, accurately diagnosed and effectively treated.
“If you’re watching videos on social media and it makes you think that you may meet criteria for the disorder, I would encourage you to seek an evaluation from a psychologist or a psychiatrist or a physician to get it checked out,” Barterian said.
What is Adult ADHD?
Adults struggling with ADHD will have problems with paying attention, hyperactivity and impulsivity that are severe enough to cause ongoing challenges at school, work and home. These symptoms are persistent and disruptive and can often be traced back to childhood.
Adult ADHD occurs in:
Adults who were diagnosed as children, but symptoms continue into adulthood.
Adults who are diagnosed for the first time, despite experiencing symptoms since they were younger that had been ignored or misdiagnosed.
Hyperactivity as a symptom is typically less present in adults than in children. Many adults with ADHD struggle with memory and concentration issues. Symptoms of ADHD often worsen with stress, conflict or increased demands in life.
What are common types of ADHD?
The three types of ADHD are:
Inattentive ADHD – Inability to pay attention and distractibility. This also is known as attention-deficit disorder (ADD).
Hyperactive and impulsive ADHD – Hyperactivity and impulsivity.
Combined ADHD – This type causes inattention, hyperactivity and impulsivity.
ADHD can be difficult to diagnose in adults, because some of the symptoms are similar to those in other mental health conditions, such as depression or anxiety.
“Symptoms of ADHD can look different between different people,” Barterian said. “Some people might have more difficulty focusing on lectures or with organisation, while others may have more social difficulties with impulsivity and trouble following along in conversations.”
A persistent infection could explain why some people experience long COVID symptoms, according to a new study led by researchers at Brigham and Women’s Hospital. The team found evidence of persistent infection in 43% of participants with cardiopulmonary, musculoskeletal or neurologic symptoms of long COVID. The results are published in Clinical Microbiology and Infection.
“If we can identify a subset of people who have persistent viral symptoms because of a reservoir of virus in the body, we may be able to treat them with antivirals to alleviate their symptoms,” said lead author Zoe Swank, PhD, a postdoctoral research fellow in the Department of Pathology at Brigham and Women’s Hospital.
The study analysed 1569 blood samples collected from 706 people, including 392 participants from the National Institutes of Health-supported Researching COVID to Enhance Recovery (RECOVER) Initiative, who had previously tested positive for a COVID infection. With a highly sensitive test they developed, researchers looked for whole and partial proteins from the SARS-CoV-2 virus. They also analysed data from the participants’ long COVID symptoms, using electronic medical chart information or surveys that were gathered at the same time as the blood samples were taken.
Compared to people who didn’t report long COVID symptoms, those who reported persisting symptoms many organ systems were approximately twice as likely to have SARS-CoV-2 proteins circulating in their blood. The research team was able to detect the spike protein and other components of the SARS-CoV-2 virus using Simoa, an ultrasensitive test for detecting single molecules. Commonly reported long COVID symptoms included fatigue, brain fog, muscle pain, joint pain, back pain, headache, sleep disturbance, loss of smell or taste, and gastrointestinal symptoms.
Specifically, 43% of those with long COVID symptoms affecting three major systems in the body, including cardiopulmonary, musculoskeletal, and neurologic systems, tested positive for viral proteins within 1 to 14 months of their positive COVID test. But only 21% of those who didn’t report any long COVID symptoms tested positive for the SARS-CoV-2 biomarkers in this same period.
It’s possible that a persistent infection explains some – but not all – of the long COVID sufferers’ symptoms. If this is the case, testing and treatment could aid in identifying patients who may benefit from treatments such as antiviral medications.
A Condition with More Than One Cause
One of the questions raised by the study is why more than half of patients with wide-ranging long COVID symptoms tested negative for persistent viral proteins.
“This finding suggests there is likely more than one cause of long COVID,” said David Walt, PhD, a professor of Pathology at Brigham and Women’s Hospital and Principal Investigator on the study. “For example, another possible cause of long-COVID symptoms could be that the virus harms the immune system, causing immune dysfunction to continue after the virus is cleared.”
To better understand whether an ongoing infection is behind some people’s long COVID symptoms, Swank, Walt and other researchers are currently conducting follow-up studies. They’re analyzing blood samples and symptom data in larger groups of patients, including people of wide age ranges and those with compromised immune symptoms. This way, they can also see if some people are more likely to have persistent virus in the body.
“There is still a lot that we don’t know about how this virus affects people,” said David C. Goff, MD, PhD, a senior scientific program director for the RECOVER Observational Consortium Steering Committee and director of the Division of Cardiovascular Sciences at the National Heart, Lung, and Blood Institute (NHLBI), part of NIH. “These types of studies are critical to help investigators better understand the mechanisms underlying long COVID – which will help bring us closer to identifying the right targets for treatment.”
Goff added that these results also support ongoing efforts to study antiviral treatments.
The SARS-CoV-2 blood test developed by Brigham and Women’s researchers is also currently being used in a national study, called RECOVER-VITAL, that is testing whether an antiviral drug helps patients recover from long COVID. The RECOVER-VITAL trial will test the patients’ blood before and after treatment with an antiviral to see if treatment eliminates persistent viral proteins in the blood.
The idea that a virus can stay in the body and cause ongoing symptoms months after an infection isn’t unique to COVID. “Other viruses are associated with similar post-acute syndromes,” said Swank. She noted animal studies have found Ebola and Zika proteins in tissues post-infection, and these viruses have also been associated with post-infection illness.
Promising findings by researchers at Baylor College of Medicine and collaborating institutions could lead to the development of a non-invasive stool test and a new therapy for endometriosis, a painful condition that affects nearly 200 million women worldwide. The study appeared in the journal Med.
“Endometriosis develops when lining inside the womb grows outside its normal location, for instance attached to surrounding intestine or the membrane lining the abdominal cavity. This typically causes bleeding, pain, inflammation and infertility,” said corresponding author Dr Rama Kommagani, associate professor in the Department of Pathology and Immunology at Baylor. “Generally, it takes approximately seven years to detect endometriosis and is often diagnosed incorrectly as a bowel condition. Thus, delayed diagnosis, together with the current use of invasive diagnostic procedures and ineffective treatments underscore the need for improvements in the management of endometriosis.”
“Our previous studies in mice have shown that the microbiome, the communities of bacteria living in the body, or their metabolites, the products they produce, can contribute to endometriosis progression,” Kommagani said. “In the current study, we took a closer look at the role of the microbiome in endometriosis by comparing the bacteria and metabolites present in stools of women with the condition with those of healthy women. We discovered significant differences between them.”
The findings suggested that stool metabolites found in women with endometriosis could be the basis for a non-invasive diagnostic test as well as a potential strategy to reduce disease progression.
The researchers discovered a combination of bacterial metabolites that is unique to endometriosis. Among them is the metabolite called 4-hydroxyindole. “This compound is produced by ‘good bacteria,’ but there is less of it in women with endometriosis than in women without the condition,” said first author Dr Chandni Talwar, postdoctoral associate in Kommagani’s lab.
“These findings are very exciting,” Talwar said. “There are studies in animal models of the disease that have shown specific bacterial metabolite signatures associated with endometriosis. Our study is the first to discover a unique metabolite profile linked to human endometriosis, which brings us closer to better understanding the human condition and potentially identifying better ways to manage it.”
Furthermore, extensive studies also showed that administering 4-hydroxyindole to animal models of the disease prevented the initiation and progression of endometriosis-associated inflammation and pain.
“Interestingly, our findings also may have implications for another condition. The metabolite profile we identified in endometriosis is similar to that observed in inflammatory bowel disease (IBD), revealing intriguing connections between these two conditions,” Kommagani said. “Our findings support a role for the microbiome in endometriosis and IBD.”
The researchers are continuing their work toward the development of a non-invasive stool test for endometriosis. They are also conducting the necessary studies to evaluate the safety and efficacy of 4-hydroxyindole as a potential treatment for this condition.
Skin pigmentation may act as a “sponge” for some medications ranging from antibiotics to nicotine patches, potentially influencing the speed with which active drugs reach their intended targets, a pair of scientists report in a perspective article published in the journal Human Genomics.
There has been a growing awareness of genetic susceptibility or tolerance to medications. Redheads for example had been shown to need more inhalational anaesthetic than dark-haired individuals. The researchers argue that a sizable proportion of drugs and other compounds can bind to melanin pigments in the skin, leading to differences in how bioavailable and efficacious these drugs and other compounds are in people with varying skin tones.
“Our review paper concludes that melanin, the pigment responsible for skin colour, shows a surprising affinity for certain drug compounds,” said paper coauthor Simon Groen, an assistant professor of evolutionary systems biology at the University of California, Riverside. “Melanin’s implications for drug safety and dosing have been largely overlooked, raising alarming questions about the efficacy of standard dosing since people vary a lot in skin tones.”
According to Groen and coauthor Sophie Zaaijer, a consultant and researcher affiliated with UC Riverside who specialises in diversity, equity, and inclusion (DEI) in preclinical R&D and clinical trials, current FDA guidelines for toxicity testing fail to adequately address the impact of skin pigmentation on drug interactions.
“This oversight is particularly concerning given the push for more diverse clinical trials, as outlined in the agency’s Diversity Action Plan,” Zaaijer said. “But current early-stage drug development practices still primarily focus on drug testing in white populations of Northern European descent.”
In one example, the researchers found evidence of nicotine affinity for skin pigments, potentially affecting smoking habits across people with a variety of skin tones and raising questions about the efficacy of skin-adhered nicotine patches for smoking cessation.
“Are we inadvertently shortchanging smokers with darker skin tones if they turn to these patches in their attempts to quit?” Groen said.
Groen and Zaaijer propose utilising a new workflow involving human 3D skin models with varying pigmentation levels that could offer pharmaceutical companies an efficient method to assess drug binding properties across different skin types.
“Skin pigmentation should be considered as a factor in safety and dosing estimates,” Zaaijer said. “We stand on the brink of a transformative era in the biomedical industry, where embracing inclusivity is not just an option anymore but a necessity.”
According to the researchers, skin pigmentation is just one example. Genetic variations among minority groups can lead to starkly different drug responses across races and ethnicities, affecting up to 20% of all medications, they said.
“Yet, our molecular understanding of these differences remains very limited,” Zaaijer said.
For example, a study on acetaminophen – a drug that binds melanin – found no difference in total plasma levels of acetaminophen between individuals of African- and European-American ancestries. Oxidation clearance of acetaminophen did however show ancestry-based differences and was 37% lower in African–versus European-Americans, which could have been partially explained by polymorphisms in CYP2E1.
The researchers point out that a shift towards inclusive drug development is set to take place as instigated by a new law, the Food and Drug Omnibus Reform Act, enacted in 2022, which will mandate considering patient diversity in R&D and clinical trials.
The researchers hope to activate the pharmaceutical industry and academia to start doing systematic experimental evaluations in preclinical research in relation to skin pigmentation and drug kinetics. They also encourage patients and advocacy groups to start asking about ancestry-related testing and efficacy of drugs.
The magnetic core of the nanodisc is magnetostrictive, which means it changes shape when magnetised. The rainbow nanodisc on the right is changing shape, allowing for the pink brain neuron to be stimulated. Image: Courtesy of the researchers
Novel magnetic nanodiscs could provide a much less invasive way of stimulating parts of the brain, paving the way for stimulation therapies without implants or genetic modification, MIT researchers report in Nature Nanotechnology.
The scientists envision that the tiny discs – about 250nm across – would be injected directly into the chosen brain location. From there, they could be activated at any time simply by applying an external magnetic field. The new particles could quickly find applications in biomedical research, and eventually, after sufficient testing, might be applied to clinical uses.
The research is described in the paper by Polina Anikeeva, a professor in MIT’s departments of Materials Science and Engineering and Brain and Cognitive Sciences, graduate student Ye Ji Kim, and 17 others at MIT and in Germany.
Deep brain stimulation (DBS) uses electrodes implanted in the target brain regions to treat symptoms of neurological and psychiatric conditions such as Parkinson’s disease and obsessive-compulsive disorder. Despite its efficacy, the surgical difficulty and clinical complications associated with DBS limit the number of cases where such an invasive procedure is warranted. The new nanodiscs could provide a much more benign way of achieving the same results.
Over the past decade other implant-free methods of producing brain stimulation have been developed, but were limited by spatial resolution or access. Other magnetic approaches studied needed genetic modifications to work, ruling it out for humans.
Since all nerve cells are sensitive to electrical signals, Kim, a graduate student in Anikeeva’s group, hypothesised that a magnetoelectric nanomaterial that can efficiently convert magnetisation into electrical potential could offer a path toward remote magnetic brain stimulation.
To this end, the researchers created nanodiscs with a magnetic core and piezolectric shell. When the core was squeezed by a magnetic field, strain in the shell produces a varying electrical polarisation. This enables the particles to deliver electrical pulses to neurons. The disc shape enhances the magnetostriction effect more than 1000-fold compared to spherical particles used previously.
After testing the nanodiscs with neurons in vitro, the researchers then injected small droplets of nanodisc-bearing solution into specific regions of the brains of mice. With an electromagnet, they turned on and off the stimulation in that region. That electrical stimulation “had an impact on neuron activity and on behaviour,” Kim says.
The team found that the magnetoelectric nanodiscs could stimulate a deep brain region, the ventral tegmental area, that is associated with feelings of reward.
The team also stimulated another brain area, the subthalamic nucleus, associated with motor control. “This is the region where electrodes typically get implanted to manage Parkinson’s disease,” Kim explains. The researchers were able to successfully demonstrate the modulation of motor control through the particles. Specifically, by injecting nanodiscs only in one hemisphere, the researchers could induce rotations in healthy mice by applying magnetic field.
The nanodiscs could trigger the neuronal activity comparable with conventional implanted electrodes delivering mild electrical stimulation. The authors achieved subsecond temporal precision for neural stimulation with their method yet observed significantly reduced foreign body responses as compared to the electrodes, potentially allowing for even safer deep brain stimulation.
The multilayered chemical composition and physical shape and size of the new multilayered nanodiscs is what made precise stimulation possible.
While the researchers successfully increased the magnetostrictive effect, the second part of the process, converting the magnetic effect into an electrical output, still needs more work, Anikeeva says. While the magnetic response was a thousand times greater, the conversion to an electric impulse was only four times greater than with conventional spherical particles.
“This massive enhancement of a thousand times didn’t completely translate into the magnetoelectric enhancement,” says Kim. “That’s where a lot of the future work will be focused, on making sure that the thousand times amplification in magnetostriction can be converted into a thousand times amplification in the magnetoelectric coupling.”
Further work is need before studies involving humans can begin, Kim says.
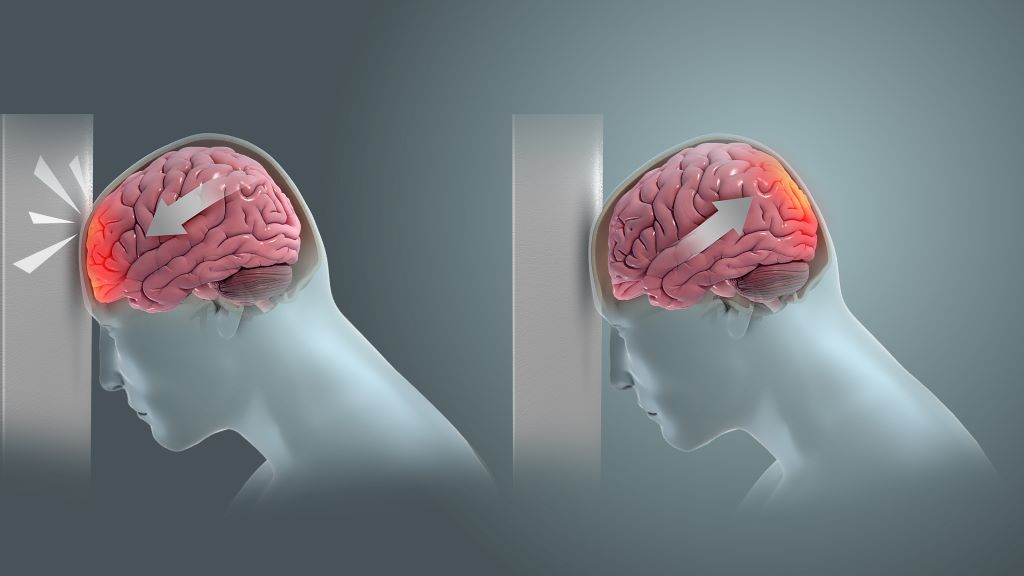
Coup and contrecoup brain injury. Credit: Scientific Animations CC4.0
Birmingham scientists have shown light therapy delivered transcranially can aid tissue repair after mild traumatic brain injury (mTBI). Their research, published in Bioengineering & Translational Medicine, indicates that this novel method could result in a new treatment option in an area of medicine that currently has few, if any, treatment options.
Traumatic brain injury (mTBI) results when the initial trauma of head injury is magnified by a complex set of inflammatory changes that occur in the brain. These secondary processes, which take place from minutes to hours after head injury, can dramatically worsen outcomes for patients.
The method invented by scientists at the University of Birmingham, UK and patented by University of Birmingham Enterprise aims to protect against this secondary damage, and stimulate faster, and better recovery for patients.
We want to develop this method into a medical device that can be used to enhance recovery for patients with traumatic brain or spinal cord injury, with the aim of improving outcomes for patients.
Professor Zubair Ahmed, College of Medicine & Health
In the study, the Birmingham team, comprising researchers Professor Zubair Ahmed, Professor Will Palin, Dr Mohammed Hadis and surgeons Mr Andrew Stevens and Mr David Davies, examined the effect of two wavelengths of near infrared light (660nm and 810nm) on recovery following injury.
The study in preclinical models used daily two-minute bursts of infrared light, delivered by a laser, for three days post-injury.
The findings showed significant reductions in the activation of astrocytes and microglial cells, which are heavily implicated in the inflammatory processes in the brain that follow head trauma, and significant reductions in biochemical markers of apoptosis (cell death).
At four weeks, there were significant improvements in performance in functional tests involving balance and cognitive function. The red light therapy also accelerated recovery compared to controls, with superior outcomes for light with a wavelength of 810nm.
The study builds on research published earlier this year which showed near infrared light delivered directly to the site of spinal cord injury both improves survival of nerve cells and stimulates new nerve cell growth.
Professor Ahmed, who led the study, said: “We want to develop this method into a medical device that can be used to enhance recovery for patients with traumatic brain or spinal cord injury, with the aim of improving outcomes for patients.”
The researchers are seeking commercial partners to co-develop the device and take it to market.
Fluorescein angiography capable of assessing neural blood flow in chronic nerve compression neuropathy
Fluorescein-enhanced contrast imaging shows a rabbit’s normal sciatic nerve, left, and a damaged one. Credit: Osaka Metropolitan University
In the modern office, it’s a daily struggle against the onset of carpal tunnel syndrome. The worst case could mean needing surgery to alleviate compression of the nerves or to repair damaged nerves. Helping surgeons visually check the areas where neural blood flow has decreased due to chronic nerve compression can lead to improvements in diagnostic accuracy, severity assessments, and outcome predictions.
With this in mind, an Osaka Metropolitan University-led research team involving Graduate School of Medicine student Kosuke Saito and Associate Professor Mitsuhiro Okada investigated the use of fluorescein angiography, a method employed in neurosurgery and ophthalmology to highlight blood vessels, to visualise neural blood flow in chronic nerve compression neuropathies like carpal tunnel syndrome. The findings were published in Neurology International.
The team found that fluorescein angiography could detect a decrease in neural blood flow in rats and rabbits with chronic nerve compression neuropathy. The results also correlated with electrodiagnostic findings.
Then fluorescein angiography was used for human patients undergoing open carpal tunnel release surgery, and the data also correlated strongly with electrodiagnostic testing. The findings indicate that fluorescein angiography might possess high diagnostic capabilities to assess neural blood flow during surgery.
“In surgery for severe chronic nerve compression neuropathy, the surgeon’s experience plays a big role in judging whether the surgical range is appropriate or whether additional treatment is necessary,” graduate student Saito noted. “This research has shown that fluorescein angiography can visualise impaired areas and assess the impairment severity, so we believe that it has the potential to contribute to improving accuracy for related surgeries.”
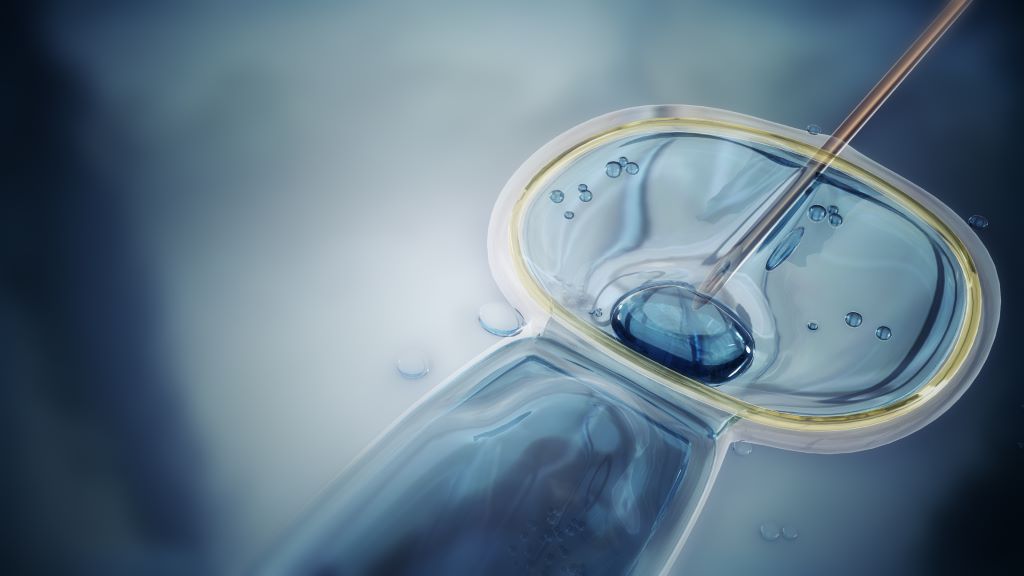
For the first time, researchers have linked specific frequent defects in sperm to risk of pregnancy complications and negative impacts on the health of the baby. The study from Lund University in Sweden shows that a high proportion of father’s spermatozoa possessing DNA strand breaks is associated with a doubled risk of preeclampsia in women who have become pregnant by IVF. It also increases the risk of the baby being born prematurely.
Infertility is a growing problem and the number of in vitro fertilisation procedures is increasing rapidly. It is already known that women who become pregnant by assisted reproduction techniques have an increased risk of preeclampsia, repeated miscarriages and the baby being born prematurely and with a lower birth weight. Yet, the reasons behind this have not been fully understood.
“Before a planned in vitro fertilisation, the man’s sperm sample is analysed for concentration, motility and morphology. But there are men who, according to this analysis, have normal sperm, but still have reduced fertility,” says Amelie Stenqvist, lecturer at Lund University and first author of the study published in Fertility and Sterility. She received her PhD from Lund and now works as a specialist in gynaecology and obstetrics at Skåne University Hospital in Malmö.
Around 20-30% of babies born through IVF have fathers with damaged DNA in their sperm, as shown by elevated levels of DNA fragmentation. The DNA fragmentation index (DFI) is a measure of the amount of strand breaks in the DNA and is used to provide important new information about male fertility. Sperm with DNA damage may still be fertile, but the chances of fertilisation are lower and if the percentage of DFI exceeds 30%, the chances of natural conception are close to zero.
Although current in vitro techniques mean that men with a high DFI can become fathers, until now very little has been known about the impact of DNA fragmentation on pregnancy and the health of the baby. It has been difficult to research the topic because the DFI value is not included in the standard measurements currently taken by Sweden’s fertility clinics. It also requires a large study population and access to national medical registries.
“Since half of the placenta’s DNA comes from the father and placental development and function play a central role in preeclampsia, we wanted to investigate whether a high percentage of DNA damage in the sperm affected the risk of preeclampsia,” says Aleksander Giwercman.
He is a professor of reproductive medicine at Lund University, a consultant at Skåne University Hospital in Malmö. Aleksander Giwercman also led a research study that included 1660 children conceived through IVF and ICSI at the Reproductive Medicine Centre in Malmö over the period 2007-2018.
The results showed that in the 841 couples who underwent IVF, a DFI of over 20% doubled the risk of the woman developing preeclampsia (10.5%) and also increased the risk of premature birth. In the IVF group with a DFI below 20%, there was a 4.8% risk of preeclampsia, which is comparable to pregnancies that occur naturally. For couples undergoing ICSI, there was no association with preeclampsia.
“Today, DFI analysis is only performed at some fertility clinics in Sweden, but we think that it should be introduced as standard at all clinics. It can give couples answers as to why they are not getting pregnant and can influence the chosen method of assisted fertilisation. Not only that, our latest results show that a DFI analysis could be used to identify high-risk pregnancies,” says Aleksander Giwercman.
What makes this finding even more interesting is that high DNA fragmentation in sperm is linked to the overall health of the father and is potentially treatable. Most DNA damage is caused by oxidative stress, which is an imbalance between harmful molecules and the antioxidants that protect cells. Other factors that increase DNA fragmentation include the man’s age, smoking, obesity and infections.
“The next step is to identify which group of men respond best to methods to prevent and treat sperm DNA damage, and to test these methods to prevent pregnancy complications,” concludes Amelie Stenqvist.
South Africa’s medical schemes industry is taking a strong, zero-tolerance stance against fraud, waste, and abuse – practices that are undermining the healthcare system. Fraudulent claims, unnecessary procedures, and mismanagement of resources are costing billions of rand, inflating healthcare costs, and putting additional financial strain on members. Instead of supporting essential treatments and care, these resources are being misused and misallocated, writes Dr Katlego Mothudi, Managing Director at the Board of Healthcare Funders (BHF).
At the recent BHF Healthcare Collab Hub, industry leaders highlighted the need for immediate reforms to curb these harmful practices and safeguard the future of medical schemes. As healthcare costs continue to rise, tackling fraud (deliberate deception), waste (inefficient use of resources), and abuse (excessive or improper use of services) is essential for ensuring that medical schemes remain affordable and sustainable. Without swift action, members may face higher premiums, with fewer resources available for the critical care they depend on.
Fraud, waste, and abuse (FWA) in the healthcare sector is not just a regulatory issue or an administrative headache, but a direct assault on the wellbeing of medical scheme members. Every fraudulent claim, and every misuse of resources, drains the pool of funds that are meant to ensure that individuals have access to necessary healthcare services. For millions of members, the repercussions of unchecked FWA include increased premiums, reduced benefits, and the potential for schemes to become financially unsustainable. It is a burden borne by all members, regardless of whether they have directly engaged with healthcare services or not.
The healthcare industry, specifically medical schemes and their administrators, has a significant responsibility to address this problem head-on. Their duty extends beyond managing funds – they are custodians of a system designed to protect individuals’ access to essential healthcare services.
If these schemes fail to adequately combat FWA, the entire medical scheme ecosystem becomes compromised, undermining trust in healthcare funding and leaving members exposed to higher costs and decreased quality of care.
The ripple effect of FWA
The scale of FWA in the medical schemes sector is staggering. According to industry reports, billions of rands are lost annually to fraudulent activities. Whether through inflated billing, unnecessary procedures, or outright false claims, these actions take funds directly from the pockets of members. Medical schemes are forced to increase premiums to cover these losses, meaning that honest, hardworking individuals are paying more for their healthcare – not because of rising medical costs, but because of the unethical behaviour of a few.
Moreover, the administrative costs associated with managing and investigating FWA claims are significant. These costs divert funds that could otherwise be used to enhance member benefits or improve healthcare services.
The long-term impact is even more worrying. If left unchecked, FWA can destabilise the entire medical scheme system. Ultimately, it is the members who suffer the most, facing financial uncertainty and diminished healthcare support when they need it most.
What the industry can do: Curbing FWA
The healthcare industry has both the tools and the responsibility to take decisive action against FWA. Key stakeholders, including medical schemes, administrators, and regulatory bodies, must collaborate to develop comprehensive strategies that can curtail the losses associated with these unethical practices. Here are some key strategies:
1. Enhanced use of technology and data analytics
The industry is already moving towards the use of automated systems and data analytics to detect unusual patterns and potential fraud. However, the systems need continuous improvement to keep up with the evolving tactics of fraudsters. Schemes should invest in advanced algorithms and artificial intelligence (AI) tools that can analyse claims in real-time, flagging high-risk transactions before they are paid. Machine learning models, for instance, could identify patterns that suggest fraudulent behaviour, such as repeated claims for the same procedure or suspiciously high billing from certain providers.
This not only helps in early detection but also ensures that members who follow the rules aren’t unfairly penalised. It is essential, however, that these systems remain transparent to avoid unintended biases or discriminatory practices.
2. Collaboration across the healthcare ecosystem
The fight against FWA cannot be won by medical schemes alone. There needs to be greater collaboration between schemes, healthcare providers, and regulatory bodies. Sharing data across schemes and industries can help to identify serial offenders who hop between schemes, committing fraud on a wide scale.
Additionally, healthcare providers themselves play a critical role. They should be incentivised to report fraudulent activities or billing irregularities they observe within their network. Schemes can establish anonymous reporting systems and offer rewards for whistleblowers who help to uncover fraud. By creating a network of accountability, the industry can make it more difficult for fraudsters to operate with impunity.
3. Member education and engagement
Members are the first line of defence against fraud. If they are empowered with the right information, they can help to identify fraudulent or abusive practices. Medical schemes should launch educational campaigns that inform members about how to scrutinise their healthcare bills and understand their benefits better.
Simple actions such as checking that all billed procedures were performed or verifying service dates can catch many fraudulent claims early. Members who understand the importance of vigilance are less likely to be unwittingly complicit in fraud and can help schemes prevent abuse of the system.
4. Improved consequent management
Strong consequent management is one sure way of deterring this fraudulent behaviour. The Health Professions Council should impose appropriate penalties on healthcare professionals found guilty. Schemes should not hesitate to take legal action against individuals or providers who commit fraud.
Stronger penalties, including prison sentences and significant fines, can serve as a deterrent.
Moreover, schemes must ensure that once a provider or member has been found guilty of fraud, they are blacklisted across all schemes. Allowing repeat offenders to continue exploiting the system is a failure that impacts all members.
At the heart of any medical scheme is the promise to its members that they will be provided with financial protection when they need healthcare. Fraud, waste, and abuse erode this promise, making it harder for schemes to deliver on their commitments. To safeguard the integrity of the system and ensure that members receive the care they deserve, the healthcare industry must step up its efforts to curb these damaging practices.
By embracing technology, fostering collaboration, educating members, and enforcing strict penalties, the industry can make significant strides in reducing FWA. In doing so, they will not only protect their financial stability but also uphold the trust and confidence that members place in them. This, above all, is the most important goal.








{kind=link}