Human colon cancer cells. Credit: National Cancer Institute
Colorectal cancer often metastasises to the liver, and for some patients, surgical removal of their liver tumours is not an option. A new study led by researchers at the Wilmot Cancer Institute and University of Rochester Medical Center (URMC) shows that a select group of patients with colorectal cancer that has spread to the liver tend to fare better if they receive a liver transplant as opposed to other common therapies.
In the study, published in JAMA Surgery, patients who had liver transplants tended to live longer without cancer progression than patients who opted for other treatments. While previous studies have shown the benefits of liver transplants for these patients, this is the first study to compare liver transplants to other treatment options.
“In any cancer treatment, it’s very easy to describe the outcomes of the patients who received the intervention, but similar patients that did not undergo the intervention can serve as a good comparison,” said Matthew Byrne, MD, a surgery resident at URMC and author of the study. “Without randomised, controlled trial data, this study offers the best evidence that is available to understand whether liver transplant provides better outcomes over other treatments.”
The study followed 33 patients whose colorectal cancer was under control, but who had liver tumours that could not be surgically removed. All 33 patients were eligible for liver transplantation, but only 20 chose to have a transplant, while 13 opted for other classical therapies, like removal of part of the liver, chemotherapy, or liver-directed therapies.
Compared to the classical therapy group, the liver transplant group had significantly higher progression-free survival rates across three years of follow-up. One year after liver transplant, 90% of patients showed no signs of cancer progression. That number dropped to 73% after two years and to 36% at three years. On the other hand, only 42% of patients who opted for other therapies were cancer-progression-free after one year, which dropped to roughly 10% after two and three years.
The transplant group also had higher overall survival rates than the standard therapy group, though the difference wasn’t statistically significant. At the three-year follow-up, 90% of transplant patients had survived, compared to 73% of patients who received other therapies.
Though this study provides solid evidence, larger clinical trials will be needed to fully understand the added benefit of liver transplant compared to other treatments for these patients, and to better refine which patients benefit most.
Researchers in Belgium have discovered a new population of macrophages, important innate immune cells that populate the lungs after injury caused by respiratory viruses. These macrophages are instrumental in repairing the pulmonary alveoli. This groundbreaking discovery promises to revolutionise our understanding of the post-infectious immune response and opens the door to new regenerative therapies.
Respiratory viruses, typically causing mild illness, can have more serious consequences, as shown during the COVID pandemic, including severe cases requiring hospitalisation and the chronic sequelae of “long Covid.” These conditions often result in the destruction of large areas of the lungs, particularly the alveoli responsible for gas exchanges. Ineffective repair of these structures can lead to ARDS or a permanent reduction in the lungs’ ability to oxygenate blood, causing chronic fatigue and exercise intolerance.
While the role of macrophages during the acute phase of respiratory viral infections is well known, their function in the post-inflammatory period has been largely unexplored. This study by the GIGA Institute at the University of Liège reveals that atypical macrophages, characterised by specific markers and transiently recruited during the early recovery phase, play a beneficial role in regenerating pulmonary alveoli.
Led by Dr Coraline Radermecker and Prof. Thomas Marichal from the Immunophysiology Laboratory, the study was conducted by Dr Cecilia Ruscitti and benefited from the ULiège’s advanced technological platforms, including flow cytometry, fluorescence microscopy, and single-cell RNA sequencing. “Our findings provide a novel and crucial mechanism for alveolar repair by these atypical macrophages,” explains Coraline Radermecker. “We have detailed their characteristics, origin, location in the damaged lung, the signals they require to function, and their role in tissue regeneration, specifically acting on type 2 alveolar epithelial cells, the progenitors of alveolar cells.” The scientific community had overlooked these macrophages because they express a marker previously thought to be specific for another immune cell population, the neutrophils, and because they appear only briefly during the repair phase before disappearing.
“Our study highlights the reparative role of these macrophages, countering the prevailing idea that macrophages following respiratory viral infections are pathogenic,” adds Thomas Marichal. “By targeting the amplification of these macrophages or stimulating their repair functions, we could develop therapies to improve alveolar regeneration and reduce complications from serious respiratory infections and ARDS.”
To illustrate, consider the lungs as a garden damaged by a storm (viral infection). These newly discovered macrophages act like specialised gardeners who clear debris and plant new seeds, enabling the garden to regrow and regain its vitality.
Pressure from ageing populations, stagnant growth and growing medical costs will mean that medical aid schemes will make above-inflation rate hikes, reveals Momentum Health marketing officer Damian McHugh. He made the comments at Momentum Health Solutions’ virtual Healthcare Insights Summit on Tuesday (30 July), where he also noted that the same demands on medical funds are serving to put NHI even further out of reach, estimating a budget of some R1.3 trillion.
If one take’s McHugh’s figures and projects into the coming years, these above-inflation hikes make the target an ever increasing-one, steadily sending the current estimates even further from the realms of affordability. This is a situation which national health schemes of far wealthier countries are now encountering.
This comes as the Council for Medical Schemes advised the 1st of August of inflation plus “reasonable utilisation estimates” resulting in a recommendation to keep under 8.5%. But it given the pressures on medical aid schemes, this is unlikely to be adhered to, as last year already saw increases in excess of this.
Medical aid cost pressures
The CMS acknowledged that above-inflation medical cost increases are inevitable due to “unique industry factors such as technological advancement, the ageing population, and the increasing prevalence of chronic diseases.”
Last year, Discovery Health Medical Scheme (DHMS) announced a weighted average increase of 7.5%, for 2024 – but its comprehensive “premium” segment rose by 13%. Both Momentum and BestMed announced weighted increases of 9.6% for 2024, while Bonitas managed to contain its increases to 6.9% (though its comprehensive cover rose to 9.6%). MediHelp surged to 15.96%, though it justified this increase as its options were the lowest-priced on the market.
Medical aid scheme growth is slow, at best around 0.5% per annum, while there is considerable pressure on subscriber income. Low income brackets only spend around 4% on healthcare, while middle and high income brackets spent 6% and 7%, respectively.
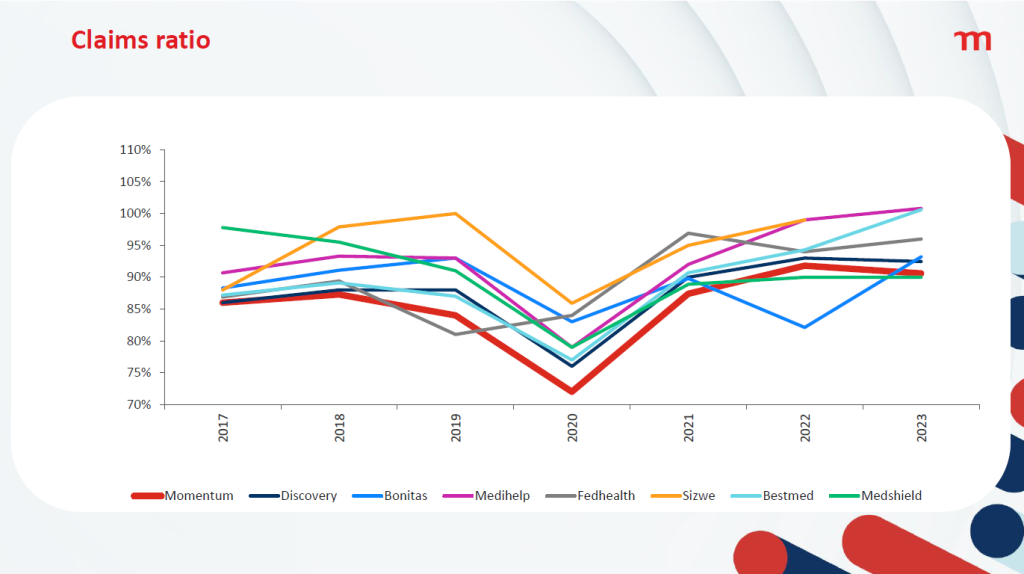
But with claims on the increase, many medical aids are having to tap into reserves and reducing solvency. Many medical aids are running close to 100% claims ratio – obviously a very bad situation for them to find themselves in.
These cost pressures result in a reduction in benefits, with the burden being shifted by reducing day-to-day benefits and members moving to Efficiency Discount Options (EDOs) – in turn, reducing the risk contribution income received by the schemes.
Rate hikes inevitable
In its recommended guidelines for 2025 released in Circular 35 of 2024, the CMS advised that medical aid schemes limit their contribution increases in line with CPIThis was based on the Reserve Bank’s latest inflation forecast which expects headline inflation to average 4.4% and 4.5% in 2025 and 2026, respectively. With last year’s estimated of an additional 3.2% to 3.8%, that works out to about 8.5%. But the CMS noted that medical aid schemes have historically had increases in excess of CPI+4%.
The COVID pandemic bucked the trend, resulting in – though many medical aid schemes saw record profits as procedures were deferred. Price increases were deferred, with increases kept below inflation for 2021 and 2022, with an uptick in 2023.
McHugh pointed out that growth in medical aid schemes has remained largely flat, and the ageing of the insured lives was linked to increasing claims costs as health problems became more complex. He revealed that claims costs per life had risen from about R15 000 in 2017 to R21 000 in 2022. This, spread across the population of South Africa, would require an NHI budget of R1.3 trillion.
Source: CMS Circular 35 of 2024
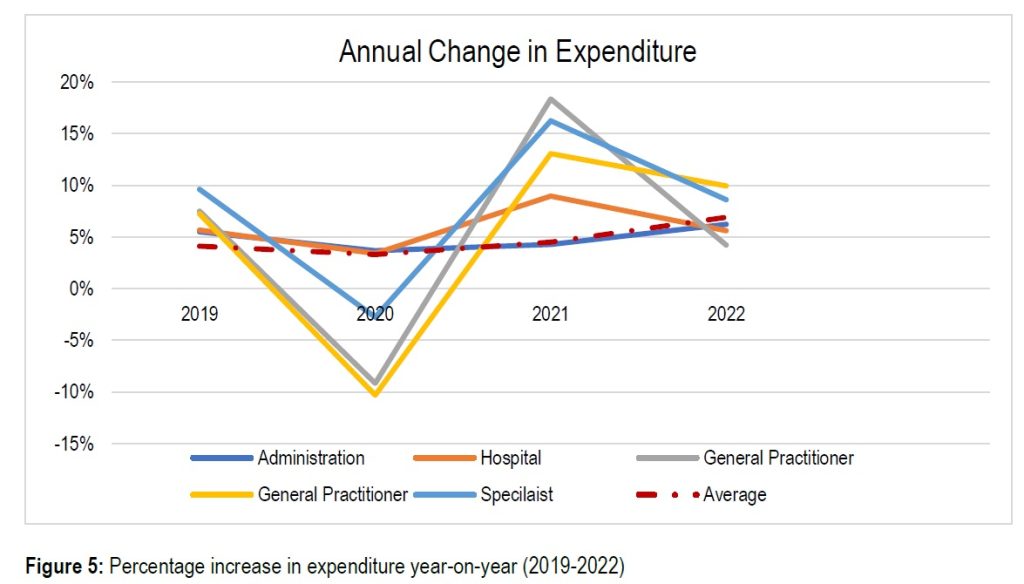
Breaking down the expenditures, McHugh said that medical schemes spent 37% on hospitals and 28% on specialists, while medicine accounted for 16% and GPs a mere 5%. The CMS also noted that hospitals and specialists had seen greater relative increases than other areas. For the essential coverage of hospitals, medicines, GPs, and dentists, that would amount to R363 billion.
Looking ahead with a little maths
One can take simple compound interest to McHugh’s figures, and even applying the CMS’ best-case “reasonable utilisation estimate” of 3.2%, for say 20 years from will mean that costs rise by 87% in today’s rands. That means the NHI’s ‘basic’ coverage would rise to R682 billion and the full coverage amounting to an incredible R2.4 trillion.
But this nothing special to South Africa. The UK’s NHS costs have similarly grown, at 3.6% per annum in real terms. And that growth has to come out of the GDP: from 3.6% of the GDP in 1949-50 to 8.2% in 2022-23, with a surge to 10.5% in the COVID pandemic.
The UK has now put measures in place to constrain cost growth to 1%, but it remains to be seen whether this will be effective without compromising service delivery. How South Africa can even contemplate an NHI where, 20 years from now, private scheme medical costs run to R39 000 per person in the best case scenario.
While McHugh did not mention the recent High Court blow to the NHI Act that found a key part of it unconstitutional, he described the legal challenge process that would see that part sent back to the National Assembly and the president.
McHugh however struck a note of optimism, noting that the public-private partnerships of the COVID pandemic showed a way forward for NHI and universal healthcare in South Africa. The 2024 elections bring the possibility of the same historic benefits for the population as the 1994 ones.
While thousands of South Africans have registered as potential bone marrow stem cell donors, a critical challenge looms: donor attrition. These dropout rates, ranging from 23% to 56%, can significantly delay finding a suitable match for blood cancer patients in desperate need of a potentially life-saving transplant. This can unfortunately impact their chances of survival.
The good news is that donating stem cells is a safe and relatively simple process. With Bone Marrow Stem Cell Donation and Leukaemia Awareness Month taking place between 15 August and 15 October 2024, DKMS Africa aims to address some misconceptions that might deter registered donors from following through with donations.
Palesa Mokomele, Head of Community Engagement and Communications, unpacks these below:
Myth 1: Donating stem cells is a painful surgical procedure.
Fact: For over 90% of donors the process entails Peripheral Blood Stem Cell (PBSC) collection, a non-surgical procedure similar to donating blood. During PBSC, donors will rest comfortably while a needle is placed in each arm. Blood is drawn from one arm, passed through a machine that separates the stem cells, and the remaining blood is returned to the body through the other arm. While not painful, some donors may experience mild side effects like headaches, fatigue, or muscle aches, which typically resolve quickly.
For a small percentage of donors (around 2%), stem cells might be collected directly from the bone marrow in the pelvic bone. This minimally invasive procedure is performed under general anaesthesia. Although some donors experience temporary discomfort or soreness at the extraction site, the feeling is usually comparable to a bruise.
Myth 2:Donating takes too long and disrupts my life too much.
Fact: While the donation process involves some steps, it’s designed to be manageable. You’ll likely have a briefing call to explain the process, a health check to confirm your suitability, and an informative session about donation itself. The actual donation typically takes less than a day (4-6 hours) for the PBSC method.
For the bone marrow donation method, a hospital stay is involved, but it’s usually just three days. This includes check-in on day one, the procedure on day two, and discharge on day three.
Myth 3:Donating stem cells means missing a lot of work.
Fact: The good news is that most donors can get back to work quickly. For PBSC donation, donors will likely be able to return within two days. If they donate bone marrow, a bit more recovery time is needed, so they should plan for about one week of leave.
Myth 4: My boss won’t be okay with me taking time off to donate.
Many employers are incredibly supportive of staff who donate stem cells. In our experience, most react positively to this selfless act. If your company doesn’t offer paid leave for donation, DKMS has a financial assistance programme that deals with lost wage compensation.
Myth 5: Donating stem cells will cost me money.
Fact: Donation is completely free of charge for the donor. DKMS covers all donation-related expenses, including travel, meals, and accommodation if needed. Financial support is also provided for a companion to join them at the hospital. The donor’s health insurance will never be involved, and DKMS handles the costs of any follow-up care that might be necessary.
“Seventeen-year-old Anele who was diagnosed with Acute Lymphoblastic Leukaemia (ALL), a type of cancer that affects the production of healthy blood cells, is just one of many patients in need of a stem cell transplant from a matching donor,” says Mokomele. “His father, Lawrence, is devastated, with his son now hanging on for dear life, waiting for that one person to be a match.”
“Every registered donor brings hope to a patient battling blood cancer. By staying committed to the cause, you help to ensure a readily available pool of potential matches, increasing a patient’s chance of receiving a transplant. Let’s give them a second chance at life!” she concludes.
Pro Secure fails in bid to stop Special Investigating Unit going after it to recover millions of rands
Photo by J Castellon on Unsplash
A company accused of unlawfully benefiting from a multi-million rand contract to supply personal protective equipment (PPE) during the Covid pandemic, has failed in a bid to quash a summons issued against it by the Special Investigating Unit to recover the money.
Pro Secure raised several objections to the formulation of the case against it in the papers. But Special Tribunal Judge Kate Pillay has dismissed the company’s objections and ordered the company to pay the costs.
The SIU investigation uncovered irregularities in the Limpopo Department of Health’s appointment of service providers including Pro Secure, Clinipro and Ndia Business Trading, which resulted in about R182-million irregular and wasteful expenditure. The SIU initiated action against Pro Secure, alleging the company had made “secret profits”, and also instituted civil proceedings against the former head of health in the province, Dr Thokozani Florence Mhlongo.
In October 2022, the SIU secured an order from the Special Tribunal, effectively freezing Mhlongo’s pension fund until the outcome of the civil action against her. Mhlongo resigned in June that year while facing disciplinary charges.
In its application to the Tribunal, Pro Secure challenged the SIU’s legal standing, the fact that the Limpopo health department was not a party to the SIU action. Pro Secure also claimed that there was no allegation that its bid for the contract was not lawful.
Judge Pillay found there was no substance to any of the company’s arguments.
She said the particulars of claim in the civil action set out how Pro Secure had received a payment “significantly exceeding their initial bid”.
She said that according to the SIU, the request for quotation sent by the department was for 5000 automated hand sanitisers. Pro Secure had submitted a quote for 5000 white electronic hand disinfectant dispensers and for 5000 liquid sanitisers, the total amount being just over R7-million. Ultimately, the company had delivered 30 000 dispenser holders at R420 per unit and 900 000 litres of hand sanitiser at R170 a litre and had been paid almost R162-million.
In a statement, SIU spokesperson Kaizer Kganyago said: “This ruling supports the SIU’s stance on the irregular procurement of PPE by the Limpopo Department of Health during the pandemic.”