More than 100 000 people die from snake bites every year. Cobra antivenom is expensive and doesn’t treat the necrosis of flesh caused by the bite, which can lead to amputations. Now, Scientists at the University of Sydney and Liverpool School of Tropical Medicine have made a remarkable discovery: a commonly used blood thinner, heparin, can be repurposed as an inexpensive antidote for cobra venom.
“Our discovery could drastically reduce the terrible injuries from necrosis caused by cobra bites – and it might also slow the venom, which could improve survival rates,” said Professor Greg Neely, a corresponding author of the study from the University of Sydney.
Using CRISPR gene-editing technology to identify ways to block cobra venom, the team, which consisted of scientists based in Australia, Canada, Costa Rica and the UK, successfully repurposed heparin and related drugs and showed they can stop the necrosis caused by cobra bites.
PhD student and lead author, Tian Du, also from the University of Sydney, said: “Heparin is inexpensive, ubiquitous and a World Health Organization-listed Essential Medicine. After successful human trials, it could be rolled out relatively quickly to become a cheap, safe and effective drug for treating cobra bites.”
The team used CRISPR to find the human genes that cobra venom needs to cause necrosis that kills the flesh around the bite. One of the required venom targets are enzymes needed to produce the related molecules heparan and heparin, which many human and animal cells produce. Heparan is on the cell surface and heparin is released during an immune response. Their similar structure means the venom can bind to both. The team used this knowledge to make an antidote that can stop necrosis in human cells and mice.
Unlike current antivenoms for cobra bites, which are 19th century technologies, the heparinoid drugs act as a ‘decoy’ antidote. By flooding the bite site with ‘decoy’ heparin sulfate or related heparinoid molecules, the antidote can bind to and neutralise the toxins within the venom that cause tissue damage.
Joint corresponding author, Professor Nicholas Casewell, Head of the Centre for Snakebite Research & Interventions at Liverpool School of Tropical Medicine, said: “Snakebites remain the deadliest of the neglected tropical diseases, with its burden landing overwhelmingly on rural communities in low- and middle-income countries.
“Our findings are exciting because current antivenoms are largely ineffective against severe local envenoming, which involves painful progressive swelling, blistering and/or tissue necrosis around the bite site. This can lead to loss of limb function, amputation and lifelong disability.”
Snakebites kill up to 138 000 people a year, with 400 000 more experiencing long-term consequences of the bite. While the number affected by cobras is unclear, in some parts of India and Africa, cobra species account for most snakebite incidents.
Working in the Dr John and Anne Chong Laboratory for Functional Genomics at the Charles Perkins Centre, Professor Neely’s team takes a systematic approach to finding drugs to treat deadly or painful venoms. It does this using CRISPR to identify the genetic targets used by a venom or toxin inside humans and other mammals. It then uses this knowledge to design ways to block this interaction and ideally protect people from the deadly actions of these venoms.
A group of more than 70 experts from all branches of medicine say they are all owed money for professional services from the Road Accident Fund – some for as long as seven years.
They have now written to Minister of Transport Barbara Creecy asking for her urgent intervention in what they say is a “disastrous situation”.
“We implore you to intervene and install a leadership in the RAF which is able to carry out its proper functioning with integrity and honesty … we are hopeless and tired,” they said in a letter to the minister.
The letter to Minister Creecy, dated 12 July, was a follow-up to one written in early June to the previous minister Sindisiwe Chikunga. There was no response to that.
Since then, dozens more specialists, including surgeons, psychologists and occupational therapists – who are collectively owed more than R150-million – have added their signatures to the document.
But the fund says it owes them nothing.
“The same people rehash this topic every time there’s a new Minister of Transport,” RAF head of corporate communications, McIntosh Polela said.
He said the experts had not been appointed by the fund but “allegedly by its former panel of attorneys”. The Service Level Agreement with the attorneys specifically stated that medical experts could only be engaged upon written authorisation of the fund. And the fund would not be liable for any fees charged without this authorisation.
He said the vast majority of the experts’ unpaid claims had not been authorised by the fund. This was due to the negligence of former panel attorneys.
In the letter to Creecy, clinical psychologist Monique Kok said the expert appointments were legal.
And, she said, their reports were being used in courts to assist in settling matters.
The fund, she said, was “finding new and cunning ways of explaining and nullifying the expert’s authority to have performed such assessment”.
She said each assessment had been done after some form of written instruction, either from the RAF directly or their panel of attorneys.
“The experts have never acted on their own accord and gone out and somehow magically found the current claimants and performed assessments that cost time and resources without instruction from the RAF or their attorneys.”
Kok said the fund’s refusal to pay their invoices had had a dire impact with some going out of business and losing their homes.
In the follow-up letter to Creecy, psychologist Chris Sampson said the experts wanted a meeting with the minister.
“We have diligently serviced the public for many years by assisting the RAF and the courts in determining appropriate compensation for claimants who were injured in serious motor vehicle accidents.
“It would appear that the organisation (and its leader’s) treatment of its own appointed experts gives us the impression that it has been allowed to become a law unto itself and from court cases it further appears that it refuses to pay claimants, experts or abide by court orders.”
Sampson said the experts conducted “painstaking investigations” and did extensive reports which were being used by the fund and yet were waiting seven years later to be paid.
They had paid out of their own pockets the significant costs of translators, transcribers, equipment and testing material.
“We believe that the state and specifically, your ministry, has a duty to intervene in what has become a well-documented failure, where this statutory body has not carried out its stipulated functions due to either, incompetence, poor leadership, arrogance and/or a fundamental evasion of responsibility and fiduciary duties,” he said.
Speaking to GroundUp, Sampson said he personally was owed about R3-million. Payments had become sporadic since about 2017, and after the Covid pandemic, had completely dried up.
“They come up with a multitude of excuses. They claim we didn’t deliver the reports on time. They repeatedly lose invoices. They say the payments are not loaded on their system , and so there must be something wrong but they don’t tell us what’s wrong. They also accuse us of charging above the tariff when they set the tariff.”
Sampson said litigation, for most, was not an option. “We don’t have deep pockets. And because we have not been paid there is nothing rattling in them.
“But we cannot throw away seven years of hard slog. We have nothing left to lose and we just hope the new minister has the zeal and energy to finally deal with the problems at the fund.”
Creecy’s office has acknowledged receipt of the two letters but attempts by GroundUp to get comment from were unsuccessful.
Most tuberculosis (TB) tests still require a trip to the clinic. Now, new technology has made it possible to test people at home. This could be a big deal for South Africa, where much TB goes undiagnosed. We unpack the findings and implications of a recent study into such TB home testing.
One of the biggest challenges in combatting TB in South Africa is that many people who fall ill with the disease are diagnosed late, or not diagnosed at all.
The World Health Organization (WHO) estimates that 280 000 people fell ill with TB in the country in 2022. Of these, roughly 66 000 were not diagnosed, and accordingly also not treated. Apart from the damage to the health of the people who are not diagnosed and treated, this also has implications for the further spread of TB since untreated TB is often infectious TB – people become non-infectious within a few weeks of starting TB treatment.
Typically, people who fall ill with TB only get diagnosed once they turn up at clinics with TB symptoms – this is called passive case-finding. In recent years, there has been a growing recognition that passive case-finding alone is not good enough if we want to diagnose more people more quickly. As a result, many people in South Africa considered to be at high risk of TB are now offered TB tests whether or not they have symptoms – an approach called targeted universal testing. Screening for TB using new mobile X-ray technology has also been piloted in the country.
Now, in the latest such active case-finding innovation, researchers have been offering people TB tests in the comfort of their own homes.
Dr Andrew Medina-Marino, a senior investigator at the Desmond Tutu Health Foundation (DTHF), tells Spotlight no one in the world was testing for TB at home until they recently started doing so at the DTHF’s new research site in the Eastern Cape.
The testing is done using a molecular testing device, roughly the size of a two litre Coke bottle, called the GeneXpert Edge. The GeneXpert Edge is a portable version of the GeneXpert machines that have been used in labs across the country to diagnose TB for over a decade.
The GeneXpert Edge is a standardised testing device that detects TB DNA in sputum. (Photo: Nasief Manie/Spotlight)
One challenge with the device was that it needed to be plugged into a power outlet in a wall and not all homes in the area have power. “So what we did is, we hooked up a car-like battery to the device and we were able to take it into people’s homes,” says Medina-Marino.
‘Acceptable and feasible’
A study lead by Medina-Marino, and recently published in Open Forum Infectious Diseases, set out to determine the acceptability and feasibility of in-home testing of household contacts of people with TB.
The study was conducted among 84 households in Duncan Village, a township in the Buffalo City Metropolitan Municipality in the Eastern Cape. The Metro had an estimated TB incidence of 876 cases per 100 000 population in 2019, according to the National Institute for Communicable Diseases. This number is much higher than the latest WHO estimate of 468 per 100 000 for South Africa as a whole.
From July 2018 to May 2019, people diagnosed with pulmonary TB were recruited from six government health clinics in the area. They were asked for permission to visit their homes to screen their household contacts for TB. Household contacts were verbally assessed for signs or symptoms of TB, including night sweats, weight loss, persistent cough and a fever.
Households where people had any signs or symptoms of TB were randomised to either be referred to a local clinic for TB testing or tested immediately in their home. Of the eighty-four randomised households, 51 household contacts were offered in-home testing. Everyone accepted the offer for in-home testing.
For the test with the GeneXpert Edge, Medina-Marino says household contacts had to produce a sputum sample. About 47% (24/51) were able to produce sputum. This was then mixed with a reagent containing the required components for a polymerase chain reaction test. This solution was then loaded into a disposable cartridge/test module and inserted into the Edge device. Results were available in about 90 minutes. Anyone who received a positive test result in their home were immediately referred to a clinic for TB treatment.
Regarding the 47 household contacts referred for testing at the clinic, only 15% (7 people) presented for clinic-based TB evaluation, 6 were tested, and 4 out of 6 returned for their results.
Ultimately, the study found that in-home testing of household contacts for TB was acceptable and feasible.
“It’s feasible. If you compare the rate of uptake of treatment versus the rate of uptake for testing, it looks like it’s performing much better when you do home based testing versus referral for testing at the clinic,” says Medina-Marino.
Risk of stigma?
Similar to when HIV home-based testing studies were carried out, Medina-Marino says prior to their study, community members expressed concerns about stigmatising houses that were visited. “[A] lot of people were saying: ‘If you go to people’s houses, you’re going to stigmatise the household.’”
But what they actually found was that people didn’t feel stigmatised. Household contacts of people with TB felt that coming to the house to test people brought a sense of security in the home. He adds that it was easy for people to believe the results because everything was done in front of them.
In instances where people didn’t have TB, Medina-Marino says household contacts were comforted that they didn’t have to be scared of the person tested. In instances where people did have TB, he says the attitude of household contacts was supportive to start treatment.
How the test compares to other tests
Apart from testing for TB, the GeneXpert Edge can also detect whether someone’s TB is resistant to rifampicin. This is one of the medicines in the standard four-drug combination used to treat TB.
Unlike the latest lab-base GeneXpert tests, the GeneXpert Edge does not detect resistance to any TB medicines other than rifampacin. “It is hard to fit the probes needed to detect other forms of resistance into the cartridge,” says study co-author Professor Grant Theron, head of the Clinical Mycobacteriology and Epidemiology Research group at Stellenbosch University’s Molecular Biology and Human Genetics Unit.
Theron notes that the sensitivity and specificity of GeneXpert Edge is similar to that of lab-based GeneXpert machines if the tests are done on specimens from the same type of patient and the same test cartridge. (High sensitivity means the likelihood of false negatives is low wile high specificity means the likelihood of false positives is low.)
Performance may however differ because of differences between people who test at home and people who test at the clinic. Theron explains that in their study they tested people who did not yet feel sick enough to go to get tested at the clinic. People who are sicker, and who are accordingly more likely to go to the clinic, are likely to have more pathogen in their sputum samples and be easier to diagnose.
‘A breakthrough for TB’
Home-based tests is a significant breakthrough in TB because of its crucial role in detecting cases early and enabling timely tracing and testing of household contacts, says Dr Ntokozo Mzimela, a lecturer in integrated pathology in the Faculty of Health Sciences at Nelson Mandela University.
She tells Spotlight it also offers several advantages over clinic-based tests. “They are highly accessible, facilitate mass testing, reduce the risk of disease transmission, and address patient reluctance by allowing testing in the comfort and privacy of one’s home.”
Mzimela adds the GeneXpert Edge and portable X-ray screening serve complementary roles in TB diagnosis. “While the X-ray reveals lung abnormalities, the Edge confirms the presence of TB bacteria. Both tools are essential and should be used in conjunction to provide comprehensive diagnostic insights and ensure accurate and timely treatment for patients,” she says.
Professor Keertan Dheda agrees that home-based testing could link up neatly with portable X-ray, but adds it is still too early to determine where home-based TB testing will fit into the country’s TB testing programme. Dheda heads up the Division of Pulmonology at Groote Schuur Hospital and the University of Cape Town.
“We don’t yet know whether testing everyone is the right approach or whether reflex testing based on chest x-ray abnormalities is the right approach,” Dheda says. “Now that feasibility has been established, it means that more studies can be undertaken, and operational research can be commenced.”
Further studies are already underway, Medina-Marino tells Spotlight.
He says the study in Duncan Village found that about 60% of household contacts who had TB symptoms could not cough up a sputum sample. His team therefore decided to combine in-home testing with an oral swab.
“So in the study that we’re doing now in households, we found an additional 12 people who cannot produce sputum but on their swab test, they showed a positive swab result. Tongue swabs increase yield of case finding among those unable to produce sputum,” he says.
Creative artwork featuring colourised 3D prints of influenza virus (surface glycoprotein hemagglutinin is blue and neuraminidase is orange; the viral membrane is a darker orange). Note: Not to scale. Credit: NIAID
A new study shows that about one in 50 people develop autoantibodies against type 1 interferons, mostly later in life, rendering them more susceptible to viral diseases like COVID-19. The study, published in the Journal of Experimental Medicine, is based on an analysis of a large collection of historical blood samples.
Virus infections trigger the cells of the immune system to release type 1 interferons. These proteins act as early messengers that warn uninfected cells and tissues that a virus is spreading. This allows cells to prepare themselves so that they are ready to fight the virus when it reaches them.
In individuals with a compromised type 1 interferon system, severe viral infections can occur because the body cannot mount a full defense. Recent research has shown that about 5 to 15% of people who are in hospital with severe COVID or influenza have a deficiency in their type 1 interferon response. This is because their blood contains autoantibodies – antibodies that target a person’s own structures – that bind type 1 interferons and stop the messenger from functioning.
Unique samples for blood analysis
“With our study, we wanted to find out what causes the immune systems of some people to turn against themselves and to also understand the consequences of having autoantibodies against type 1 interferons,” says study head Benjamin Hale, professor at the Institute of Medical Virology of the University of Zurich (UZH).
His research team utilized a very large collection of frozen blood samples from the Swiss HIV Cohort Study, originally donated for research on HIV infection. They analysed the samples of around 2000 adults who had donated blood samples twice a year for several decades. “This study was only possible because of this unique biobank of stored longitudinal blood samples and well-curated clinical data,” says Hale. The fact that the donors were people living with HIV had no relevance for the results, because in this cohort the virus was suppressed by treatment.
Ageing population is vulnerable
First, the UZH team analysed the blood samples for the presence of autoantibodies against type 1 interferons to find out who had developed the autoantibodies, when this occurred, and how long these autoantibodies lasted in the blood.
The analysis revealed that around 2% of individuals produced autoantibodies against type 1 interferons in their lifetime and that this typically occurred between the ages of 60 to 65. This confirms prior studies that reported that the prevalence of autoantibodies against type 1 interferons might increase with age.
Next, by studying clinical data, researchers at the Department of Infectious Diseases and Hospital Epidemiology of the University Hospital Zurich (USZ) were also able to understand which factors contributed to the development of autoantibodies against type 1 interferons. The individuals who developed them appeared to be prone to also producing antibodies against other proteins formed by their own bodies. This so-called loss of self-tolerance can occur in some people as they age. “These individuals may produce antibodies against their own type 1 interferons because they are both prone to making autoantibodies and are exposed to high levels of type 1 interferons, for example because their immune system produces interferons against other infections at the time,” supposes Hale.
Lifelong consequences of autoantibodies
Importantly, the study found that once developed, these autoantibodies remained detectable in the blood of individuals for the rest of their lives. People with autoantibodies against type 1 interferons, even when they had developed them as far back as in 2008, were more likely to suffer from severe COVID in 2020. “These autoantibodies have consequences for individuals decades later, leading to a compromised type 1 interferon system and reduced immunity against viruses,” says Hale.
Understanding these risk factors might lead to future diagnostic tests that can identify older individuals who are more prone to developing this deficiency, and therefore help with measures to prevent autoantibodies ever developing. Identifying individuals with autoantibodies against type 1 interferons could also help to prioritize these people for vaccines or antivirals to prevent severe viral infections.
Retina showing reticular pseudodrusen. Although they can infrequently appear in individuals with no other apparent pathology, their highest rates of occurrence are in association with age-related macular degeneration (AMD), for which they hold clinical significance by being highly correlated with end-stage disease sub-types, choroidal neovascularisation and geographic atrophy. Credit: National Eye Institute
In a new analysis of data, researchers at the National Institutes of Health (NIH) have found that taking a daily supplement containing antioxidant vitamins and minerals slows progression of late-stage dry age-related macular degeneration (AMD), potentially helping people with late-stage disease preserve their central vision.
Age-related macular degeneration affects the macula, the part of the retina that provides central vision.
Researchers reviewed the original retinal scans of participants in the Age-Related Eye Diseases Studies (AREDS and AREDS2) and found that, for people with late-stage dry AMD, taking the antioxidant supplement slowed expansion of geographic atrophy regions towards the central foveal region of the retina. The study was published in the journal Ophthalmology.
“We’ve known for a long time that AREDS2 supplements help slow the progression from intermediate to late AMD. Our analysis shows that taking AREDS2 supplements can also slow disease progression in people with late dry AMD,” said Tiarnan Keenan, MD, PhD, of NIH’s National Eye Institute (NEI) and lead author of the study. “These findings support the continued use of AREDS2 supplements by people with late dry AMD.”
In their new analysis, the researchers reviewed the original retinal scans of participants in the AREDS (total 318 participants, 392 eyes) and AREDS2 (total 891 participants, 1210 eyes) trials who developed dry AMD, calculating the position and expansion rate of their regions of geographic atrophy. For those people who developed geographic atrophy in their central vision, the supplements had little benefit. But for the majority who developed geographic atrophy far from the fovea, the supplements slowed the rate of expansion towards the fovea by approximately 55% over an average of three years.
In early and intermediate AMD, the light-sensing retina at the back of the eye develops small yellow deposits of fatty proteins called drusen. When the disease progresses to the late stage, people can develop leaky blood vessels (“wet” AMD) or can lose regions of light-sensitive cells in the retina (“dry” AMD). The geographic atrophy in these regions slowly expands over time, causing people to progressively lose their central vision.
The original AREDS trial found that a supplement formula containing antioxidants (vitamin C, E, and beta-carotene), along with zinc and copper, could slow progression of intermediate to late-stage AMD. The subsequent AREDS2 trial found that substituting the antioxidants lutein and zeaxanthin for beta-carotene improved the efficacy of the supplement formula and eliminated certain risks. At the time, neither trial detected any further benefit once participants had developed late-stage disease.
However, that original analysis did not account for a phenomenon in the dry form of late AMD called “foveal sparing.” While all regions of the retina are sensitive to light, the region that gives us the highest acuity central vision is called the fovea. Many people with dry AMD first develop geographic atrophy outside this foveal region, and they only lose their central vision when the geographic atrophy regions expand into the foveal area.
“Our high acuity central vision is essential for tasks like reading and driving. Given that there are few therapeutic options for people with late-stage dry AMD to retain or restore their vision, antioxidant supplementation is a simple step that may slow central vision loss, even for those with late disease,” Keenan said. “We plan to confirm these findings in a dedicated clinical trial in the near future.”
Researchers from ETH Zurich and Empa have developed a hydrogel implant that can help prevent endometriosis. This innovation, which is described in Advanced Materials, also acts as a contraceptive.
A hydrogel is a gel made of a type of plastic that can bind water. Hydrogels have a variety of use cases, including contact lenses, delivering doses of medication within the body, moisturisers, water storage in soil, cleaning polluted water and as gelling and thickening agents. Now, the researchers have developed the first hydrogel implant designed for use in fallopian tubes. This innovation performs two functions: one is to act as a contraceptive, the other is to prevent the recipient from developing endometriosis in the first place or to halt the spread if they do.
Around four years ago, Inge Herrmann made a new addition to her research group at the Department of Mechanical and Process Engineering at ETH and Empa. The new member was a senior physician specialising in gynaecology who was keen to pursue clinically-inspired research. This kind of interdisciplinary collaboration was an experiment for the whole team. Their initial goal had been to turn a hydrogel into a new kind of contraceptive for women. However, after the research team began talking to the gynaecologist, they realised that implanting a hydrogel to occlude the fallopian tubes could also help prevent endometriosis.
Preventing endometriosis by occluding the fallopian tubes
Around 10 percent of women suffer from endometriosis. However, it is still unclear exactly what causes this condition. The assumption is that during menstruation, blood flows back along the fallopian tubes and into the abdominal cavity. This blood contains cells from the uterine lining (endometrium), which settle in the abdominal cavity and as a result can cause inflammation, pain and the formation of scar tissue.
The researchers found a way to create a hydrogel implant capable of successfully occluding the fallopian tubes and thus preventing retrograde menstruation. “We discovered that the implant had to be made of an extremely soft gel – similar in consistency to a jelly baby – that does not impact native tissue and is not treated and rejected as a foreign body,” explains Alexandre Anthis, lead author of the study.
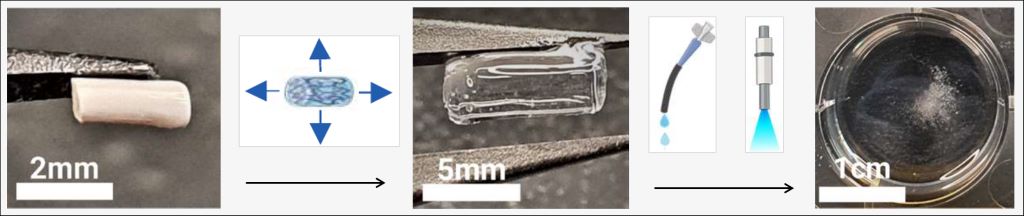
The hydrogel implant swells to around twice its original size when it comes into contact with liquid (arrow 1 left to centre) and can be easily and painlessly destroyed using UV light or a special solution (arrow 2 centre to right). (Graphic: adapted from Anthis AHC et al., Advanced Materials, 2024)
An advantage of hydrogels is that they swell when brought into contact with liquid. As a result, this new implant starts off at approximately 2mm in length. But once implanted in the fallopian tubes as part of a non-surgical procedure using a hysteroscope – an instrument for inspecting the uterine cavity – the implant swells to more than double its original size. The hydrogel then acts as a barrier to both sperm and blood. “Our hydrogel implant can be easily and quickly destroyed, either with UV light or a special solution, so that recipients don’t have to have an invasive and risky operation should they decide to reverse the procedure,” Herrmann says.
Many cancer medications, from chemotherapy to modern immunotherapies, attack the nerves as well as the tumour cells. Some therapies, such as oxaliplatin or vinca alkaloids, leave 70 to 90% of patients complaining of pain, balance issues, or feelings of numbness, burning or tingling. These symptoms can be very debilitating. They can disappear following cancer treatment, but in around 50% they become chronic. Specialists call it chemotherapy-induced peripheral neuropathy, or CIPN for short.
A research team led by sports scientist Dr Fiona Streckmann from the University of Basel and the German Sport University Cologne has now shown that specific exercise, concomitant to cancer therapy, can prevent nerve damage in many cases. The researchers have reported their findings in JAMA Internal Medicine.
Exercise alongside chemo
The study involved 158 cancer patients, both male and female, who were receiving treatment either with oxaliplatin or vinca-alkaloids. The researchers divided the patients at random into three groups. The first was a control group, whose members received standard care. The other two groups completed exercise sessions twice a week for the duration of their chemotherapy, with each session lasting between 15 and 30 minutes. One of these groups carried out exercises that focused primarily on balancing on an increasingly unstable surface. The other group trained on a vibration plate.
Regular examinations over the next five years showed that in the control group around twice as many participants developed CIPN as in either of the exercise groups. In other words, the exercises undertaken alongside chemotherapy were able to reduce the incidence of nerve damage by 50 to 70%. In addition, they increased the patients’ subjectively perceived quality of life, made it less necessary to reduce their dose of cancer medications, and reduced mortality in the five years following chemotherapy.
The participants receiving vinca-alkaloids and performing sensorimotor training, had the largest benefit.
Ineffective medications
A lot of money has been invested over the years in reducing the incidence of CIPN, explains Streckmann. “This side effect has a direct influence on clinical treatment: for example, patients may not be able to receive the planned number of chemotherapy cycles that they actually need, the dosage of neurotoxic agents in the chemotherapy may have to be reduced, or their treatment may have to be terminated.”
Despite the investments made, there is no effective pharmacological treatment to date: various studies have shown that medications can neither prevent nor reverse this nerve damage. However, according to the latest estimates, USD 17 000 are spent per patient every year in the USA on treating nerve damage associated with chemotherapy. Streckmann’s assumption is that “doctors prescribe medications despite everything, because patients’ level of suffering is so high.”
Study ongoing in children’s hospitals
In contrast, the sports scientist emphasises, the positive effect of exercise has been substantiated, and this treatment is very cheap in comparison. At the moment she and her team are working on guidelines for hospitals, so that they can integrate the exercises into clinical practice as supportive therapy. In addition, since 2023 a study has been ongoing in six children’s hospitals in Germany and Switzerland (Project PrepAIR), which is intended prevent sensory and motor dysfunctions in children receiving neurotoxic chemotherapy.
“The potential of physical activity is hugely underestimated,” says Fiona Streckmann. She very much hopes that the results of the newly published study will lead to more sports therapists being employed in hospitals, in order to better exploit this potential.
The former manager of an operating theatre at Universitas Hospital has successfully sued Netcare for failing to protect her and take action against an abusive surgeon because, she claimed, it was well known that he was a “money spinner” for the company.
Tilana Alida Louw also sued Dr Stephen Paul Grobler but, following his sudden death in June 2022, entered into a confidential settlement agreement with the executor of his estate.
She then pursued her case against Netcare Universitas Hospital.
In a ruling this month, Bloemfontein High Court Judge Ilsa van Rhyn directed Netcare to pay her R300 000 for damages, past and future medical expenses, and to pay part of her costs on a punitive scale.
Louw was appointed as surgical theatre manager at the hospital in 2005. Her role was to oversee and manage operating theatres and theatre staff and monitor patient care.
At that time, she was warned by the then hospital manager, and others, that Grobler had an “aggressive type personality”.
She said she soon experienced first hand his temper tantrums.
In her claim, she said he had verbally abused her continually, hurling profanities, insults, using blasphemous language and obscenities at her in the presence of other operating theatre staff and even members of the public.
She said Netcare had failed to come to her assistance, in spite of her numerous requests and complaints.
Netcare had also failed to act against Grobler, even though it was common knowledge that he behaved this way.
Louw alleged that Netcare had failed in its legal duty to create a work environment free from verbal abuse and intimidation and to take reasonable care of her safety and protect her from psychological harm.
As a result she was humiliated, degraded and suffered shock, anguish, fear and anxiety. She experienced post-traumatic stress syndrome.
She wanted to be compensated for this. And she wanted Netcare to publish a written apology in a local newspaper.
Netcare defended the action. It denied that it had breached its duty to Louw and said it had taken action against Grobler.
After Louw and her witness, labour law expert Professor Halton Cheadle, testified, Netcare offered to pay her for damages and to apologise.
Louw accepted the financial offer, but she was not happy with the wording of the apology and the scale of costs tendered.
Judge van Rhyn said Louw had testified that her complaints and those of others had been largely ignored by management.
“She explained that several of the scrub nurses refused to work with Dr Grobler and she would step in and assist him during surgeries. Her sense of duty and pity for the patients, many of them being cancer patients who were in dire need of urgent and timeous surgeries, caused her to bear the brunt and endure the constant abuse.”
Louw had said she and other personnel were “not allowed” to lay complaints against Grobler because he was a “so-called money-spinner for Netcare”.
Cheadle, in his evidence, said given the number of grievances lodged against Grobler and given Netcare’s professed zero-tolerance approach to harassment, a reasonable employer would have warned Grobler about his behaviour after the first complaint and would have terminated his contract at the very least, after the third complaint.
Judge van Rhyn said Netcare’s offer of damages during the trial had been made after Louw had endured years of abuse at the hands of Grobler and eight years of litigation.
“I also agree with argument on behalf of the Plaintiff (Louw) that Netcare evidently allowed its employees to be abused by Dr Grobler for its own financial interests. Netcare was acquainted with Dr Grobler’s disgusting behaviour even prior to her (Louw’s) appointment as the unit manager,” she said.
This conduct was deserving of a punitive costs order, the judge said.
Louw had rejected the proposed apology because it contained the words “we apologise sincerely that you felt that Netcare did not sufficiently support you”.
The judge said she agreed with Louw’s perception that this did not, in its plain and ordinary meaning, convey a sincere regret and remorseful apology.
She said she had been informed during argument that Netcare had published the apology in the local newspaper.
However, she said, she would not make any order regarding the apology, because it would not be lawful in a case which was not based on defamation.
There are many drugs that anaesthesiologists can use to induce unconsciousness in patients. Exactly how these drugs cause the brain to lose consciousness has been a longstanding question, but MIT neuroscientists have now answered that question for the commonly used drug propofol.
Using a novel technique for analysing neuron activity, the researchers discovered that the drug propofol induces unconsciousness by disrupting the brain’s normal balance between stability and excitability. The drug causes brain activity to become increasingly unstable, until the brain loses consciousness.
“The brain has to operate on this knife’s edge between excitability and chaos. It’s got to be excitable enough for its neurons to influence one another, but if it gets too excitable, it spins off into chaos. Propofol seems to disrupt the mechanisms that keep the brain in that narrow operating range,” says Earl K. Miller, the Picower Professor of Neuroscience and a member of MIT’s Picower Institute for Learning and Memory.
The new findings, published in Neuron, could help researchers develop better tools for monitoring patients as they undergo general anaesthesia.
Miller and Ila Fiete, a professor of brain and cognitive sciences, the director of the K. Lisa Yang Integrative Computational Neuroscience Center (ICoN), and a member of MIT’s McGovern Institute for Brain Research, are the senior authors of the new study. MIT graduate student Adam Eisen and MIT postdoc Leo Kozachkov are the lead authors of the paper.
Losing consciousness
Propofol is a drug that binds to GABA receptors in the brain, inhibiting neurons that have those receptors. Other anaesthesia drugs act on different types of receptors, and the mechanism for how all of these drugs produce unconsciousness is not fully understood.
Miller, Fiete, and their students hypothesised that propofol, and possibly other anaesthesia drugs, interfere with a brain state known as “dynamic stability.” In this state, neurons have enough excitability to respond to new input, but the brain is able to quickly regain control and prevent them from becoming overly excited.
Previous studies of how anaesthesia drugs affect this balance have found conflicting results: Some suggested that during anaesthesia, the brain shifts toward becoming too stable and unresponsive, which leads to loss of consciousness. Others found that the brain becomes too excitable, leading to a chaotic state that results in unconsciousness.
Part of the reason for these conflicting results is that it has been difficult to accurately measure dynamic stability in the brain. Measuring dynamic stability as consciousness is lost would help researchers determine if unconsciousness results from too much stability or too little stability.
In this study, the researchers analysed electrical recordings made in the brains of animals that received propofol over an hour-long period, during which they gradually lost consciousness. The recordings were made in four areas of the brain that are involved in vision, sound processing, spatial awareness, and executive function.
These recordings covered only a tiny fraction of the brain’s overall activity, so to overcome that, the researchers used a technique called delay embedding. This technique allows researchers to characterize dynamical systems from limited measurements by augmenting each measurement with measurements that were recorded previously.
Using this method, the researchers were able to quantify how the brain responds to sensory inputs, such as sounds, or to spontaneous perturbations of neural activity.
In the normal, awake state, neural activity spikes after any input, then returns to its baseline activity level. However, once propofol dosing began, the brain started taking longer to return to its baseline after these inputs, remaining in an overly excited state. This effect became more and more pronounced until the animals lost consciousness.
This suggests that propofol’s inhibition of neuron activity leads to escalating instability, which causes the brain to lose consciousness, the researchers say.
Better anesthesia control
To see if they could replicate this effect in a computational model, the researchers created a simple neural network. When they increased the inhibition of certain nodes in the network, as propofol does in the brain, network activity became destabilized, similar to the unstable activity the researchers saw in the brains of animals that received propofol.
“We looked at a simple circuit model of interconnected neurons, and when we turned up inhibition in that, we saw a destabilization. So, one of the things we’re suggesting is that an increase in inhibition can generate instability, and that is subsequently tied to loss of consciousness,” Eisen says.
As Fiete explains, “This paradoxical effect, in which boosting inhibition destabilises the network rather than silencing or stabilising it, occurs because of disinhibition. When propofol boosts the inhibitory drive, this drive inhibits other inhibitory neurons, and the result is an overall increase in brain activity.”
The researchers suspect that other anesthetic drugs, which act on different types of neurons and receptors, may converge on the same effect through different mechanisms – a possibility that they are now exploring.
If this turns out to be true, it could be helpful to the researchers’ ongoing efforts to develop ways to more precisely control the level of anaesthesia that a patient is experiencing. These systems, which Miller is working on with Emery Brown, the Edward Hood Taplin Professor of Medical Engineering at MIT, work by measuring the brain’s dynamics and then adjusting drug dosages accordingly, in real-time.
“If you find common mechanisms at work across different anaesthetics, you can make them all safer by tweaking a few knobs, instead of having to develop safety protocols for all the different anaesthetics one at a time,” Miller says. “You don’t want a different system for every anesthetic they’re going to use in the operating room. You want one that’ll do it all.”
The researchers also plan to apply their technique for measuring dynamic stability to other brain states, including neuropsychiatric disorders.
“This method is pretty powerful, and I think it’s going to be very exciting to apply it to different brain states, different types of anaesthetics, and also other neuropsychiatric conditions like depression and schizophrenia,” Fiete says.
High-protein diets, known as ‘‘Paleolithic diets’’, are popular. Using mouse models, scientists at the University of Geneva (UNIGE) have studied their impact. While effective in regulating weight and stabilizing diabetes, these diets are not without risks. Excess protein greatly increases ammonium production, overwhelming the liver. Excess ammonium can cause neurological disorders and, in severe cases, lead to coma. These results, published in the Journal of Biological Chemistry, suggest caution when following these diets.
While current treatments help control the progression of the type 2 diabetes, they do not cure it. Losing weight is often an essential part of the treatment.
‘‘Diets rich in animal and/or plant proteins, known as Paleolithic diets, can be used to stabilise type 2 diabetes and regulate weight,’’ explains Pierre Maechler, full professor at the Department of Cell Physiology and Metabolism at the UNIGE Faculty of Medicine, who led this research. These diets are inspired by the meat-based diets of pre-agricultural time. ‘‘But what impact do they have on the body? Are they harmless? That’s what we set out to find out.’’
Liver under Pressure
Ammonium is a normal waste product of protein breakdown, essentially eliminated in the liver by the enzyme glutamate dehydrogenase (GDH). In the event of protein overload, the GDH enzyme comes under pressure. To study the impact of high-protein diets, Pierre Maechler’s team fed healthy mice and mice lacking the GDH enzyme in their liver a diet with a protein content mimicking the so-called Paleolithic diet.
Scientists observed that in healthy mice, although excess protein increased ammonium production, the liver managed this excess due to the action of the GDH enzyme, which detoxifies ammonium before it can cause damage. ‘‘In contrast, in mice lacking the GDH enzyme, the liver is unable to eliminate the excess of toxic ammonium derived from proteins. No need to wait for weeks or months; a change of diet lasting a few days is enough to observe major consequences,’’ explains Karolina Luczkowska, a former PhD student at the Department of Cell Physiology and Metabolism at the UNIGE Faculty of Medicine, and the study’s first author.
Caution is Advised
These results suggest that in case of dysfunctional GDH enzyme, high-protein diets may cause a harmful excess of ammonium. Ammonium not eliminated by the liver can cause severe disorders, particularly neurological ones. A blood test could assess GDH activity to avoid overloading the metabolism with proteins in people whose GDH enzyme is deficient. ‘‘It is therefore important to be well informed before following a high-protein diet,’’ concludes Pierre Maechler.