New Year’s Day saw the Gauteng Department of Health welcoming 112 babies into the world, the lion’s share of more than 400 births in total for the country. According to data released by Gauteng Health on X/Twitter, in the province’s public healthcare facilities, there were a total of 59 boys and 53 girls. Thelle Mogoerane Regional Hospital topped the table with 10 babies, followed by Chris Hani Baragwanath Academic Hospital (CHBAH) with 9 babies. But all of this was relatively quiet compared to Christmas Day, which saw more than three times the New Years’ Day number.
MEC Nkomo Nomantu together with MMC for Health Rina Marx joined the postpartum mothers at Dr George Mukhari Academic Hospital on the morning of New Year’s Day in welcoming their new arrivals. Gauteng’s academic hospitals recorded 19 births, while there were 10 births at the tertiary hospitals. Regional and district hospitals had 69 births and community healthcare centres had 14.
Christmas Day saw 387 babies born, 201 of them girls and 186 boys. CHBAH welcomed the most, with 46 births, followed by Tembisa Hospital with 38.
Like many countries, South Africa has a shortage of healthcare workers – particularly of doctors. One response to such shortages is task-shifting – in short, to let doctors focus on the things only they can do, and to shift some other less specialised tasks to other healthcare workers like nurses or pharmacists.
Task-shifting can take many forms. Earlier this year Spotlight reported on a court case that gave the green light to specially trained pharmacists to dispense antiretroviral treatment without a script (the judgement is being appealed). Similarly taking pressure off public sector clinics, the Department of Health has for several years now allowed some people to pick up their medicines at participating private sector pharmacies or other pickup points. Less well implemented, was the introduction of clinical associates in 2008 as a new type of mid-level healthcare worker that can take some of the pressure off of doctors and stand-in for them in some situations.
Probably the most impactful example of task-shifting in South Africa, however, was the introduction of Nurse Initiated and Managed Antiretroviral treatment (NIMART) in 2010.
What is NIMART?
Dr Silingene Ngcobo, a lecturer at the School of Nursing and Public Health at the University of KwaZulu-Natal and a Board Member of the Southern African HIV Clinicians Society, says NIMART is a clinical management program for people living with HIV which is driven by registered nurses. This means that registered nurses can independently manage a person living with HIV, starting from screening and diagnosis, all the way to treating, and monitoring throughout the HIV care continuum in the absence of a medical doctor.
As explained by Mmotsi Moloi, Training Programme Manager at the Aurum Institute (an NGO), prior to the introduction of NIMART in 2010 only doctors were authorised to prescribe antiretroviral therapy.
The rollout of antiretrovirals in South Africa technically started in 2004, but it only gathered momentum after the end of state-backed AIDS denialism in 2008. It soon after became clear that South Africa would not have enough doctors to handle the demand for HIV treatment and nurses would have to be roped in.
“The waiting lists became long, and the doctors could not meet the increasing demand of clients in need of antiretroviral treatment, this led to the death of clients while awaiting to be initiated,” says Moloi. “There was an urgent need to remedy the situation which was to decentralise management of HIV to Primary health care facilities and professional nurses to be trained and authorised to manage HIV infected clients.”
Ngcobo says nurses are often the only healthcare providers available to provide HIV prevention, care, and treatment services. She says the South African healthcare delivery system approach has changed from hospital-centred care to promotion of health and prevention of disease through primary healthcare and the introduction of NIMART fits this shift.
Hard to quantify
According to estimates from Thembisa, the leading mathematical model of HIV in the country, the number of people taking HIV treatment in South Africa increased from 1.2 million in 2010 to 5.7 million in 2022. How big a part NIMART played in this remarkable scale-up of treatment is hard to quantify, but that it played a pivotal role seems clear.
A review study published in 2021 that looked back at 10 years of NIMART in South Africa, found that adequate NIMART training “results in improved knowledge of HIV management, greater confidence and clinical competence, particularly if accompanied by mentoring”.
The review summarised results from several smaller studies conducted in different provinces on NIMART – which show, on a small scale at least, what potential impact NIMART has had. Among other things, the training of nurses to initiate and manage HIV treatment led to feelings of empowerment, and when coupled with appropriate training and support can “lead to increased quality of patient care, confidence and professional development”.
Studies conducted in Johannesburg cited by the review found that NIMART training increased access to HIV treatment, reduced workloads at referral facilities, and reduced referrals to tertiary hospitals. Nurses also saw an “improvement in the quality of life of their patients and the retention of patients in care, which they felt reflected the success of NIMART”.
When asked how many NIMART-qualified nurses we have in the country, Foster Mohale, spokesperson for the National Department of Health, says he can’t provide an exact number since they no longer collect data on NIMART since it has been incorporated in broader HIV training. He also says that provinces are the custodians of data for all trained healthcare workers and points out that the numbers change all the time due to attrition.
What NIMART nurses do
Ngcobo says NIMART nurses assess and screen people living with HIV for treatment eligibility, initiate antiretroviral therapy, provide adherence counselling and monitoring, screen for opportunistic infections, offer various preventative therapies, psychological support, as well as appropriate referrals to other members of the disciplinary team, and oversee repeat visits throughout the healthcare user’s life while managing any other health condition that the person might have.
Nurses also have to support people with tuberculosis and non-communicable diseases (such as diabetes and hypertension) to take treatment as prescribed.
“For effective management of other diseases, NIMART nurses should actually work with all other conditions because a person living with HIV still can gets various other conditions which still need to be managed. Therefore, the role of [the] NIMART nurse is to wholistically manage the patient and provide all the necessary healthcare services that the healthcare user in front of them will be requiring,” says Ngcobo.
Training requirements
The NIMART programme has changed somewhat since its launch back in 2010. Mohale says the programme now also covers the majority of healthcare professionals like medical doctors, pharmacists, registered or professional nurses, and other healthcare professionals who are authorised by their statutory bodies to assess, diagnose, prescribe, and dispense medications. He says in 2017 NIMART was changed to “Basic HIV for Health Care Professionals”, but the name NIMART is still in wide use.
The essence of the programme however remains that a professional nurse, or other qualifying healthcare professional, must complete special training (see this online course for example) before they are authorised to prescribe HIV treatment and manage the treatment and care of people living with HIV. Training typically requires both an exam and some practical work, ideally with the support of a mentor.
All prescribing by nurses in the public sector relies on section 56(6) of the Nursing Act, which allows an exception to the Medicines Act and other health-related laws, explains Andy Gray, Senior Lecturer in pharmaceutical sciences at the University of KwaZulu-Natal. “They therefore do not need section 22A(15) permits or section 22C(1)(a) dispensing licences in terms of the Medicines Act,” he says.
The legalities of how nurse prescribing works in South Africa is set out in a 2016 policy document issued by the National Department of Health. Amongst others, the document states that, “a nurse may only perform the functions authorised by Section 56(6) in public sector facilities in the district or municipality where the authorisation was granted to him/her”. In other words, nurses who move to jobs at other facilities or in other districts will often require new authorisation before they may prescribe medicines such as antiretrovirals.
Some concerns
But there are signs that training and mentorship is not functioning optimally across the board.
“There is non-standardised training and inadequate mentoring as the country doesn’t have enough trainers,” says Mohale. “There are human resource constraints for both trainers and nurses to be trained. Some districts rely on their district support partners to carry out trainings on their behalf.”
“Staff shortage from the facilities also leads to some nurses not being able to be trained due to demand for other health services at their service delivery points. Some challenges include failure to identify and manage drug-drug and drug-food interactions which are important in making sure that the patients are suppressing their viral loads,” he adds.
Mohale’s comments echo several barriers to the success of NIMART that were identified in the 2021 review study, including: “non-standardised training, inadequate mentoring, human resource constraints, health system challenges, lack of support and empowerment, and challenges with legislation, policy and guidelines”.
Mayo Clinic researchers mapped how the measles virus mutated and spread in the brain of a person who succumbed to a rare, lethal brain disease. New cases of this disease, which is a complication of the measles virus, may occur as measles re-emerges among the unvaccinated, say researchers.
Using the latest tools in genetic sequencing, researchers at Mayo Clinic reconstructed how a collective of viral genomes colonised a human brain.
The virus acquired distinct mutations that drove the spread of the virus from the frontal cortex outward.
The highly contagious measles virus infects the upper respiratory tract where it uses the trachea as a trampoline to launch and spread through droplets dispersed when an infected person coughs or sneezes.
Dr Cattaneo pioneered studies on how the measles virus spreads throughout the body. He first began to study the measles virus about 40 years ago and was fascinated by the rare, lethal brain disease called subacute sclerosing panencephalitis (SSPE), which occurs in about 1 in every 10 000 measles cases.
It can take about five to 10 years after the initial infection for the measles virus to mutate and spread throughout the brain.
Symptoms of this progressive neurological disease include memory loss, seizures and immobility.
Dr. Cattaneo studied SSPE for several years until the lethal disease nearly disappeared as more people were vaccinated against measles. But now, measles is resurging due to vaccine hesitancy and missed vaccinations.
During the COVID pandemic, millions of children missed receiving their measles vaccinations, which has resulted in an estimated 18% increase in measles cases and 43% increase in death from measles in 2021 compared to 2022 worldwide, according to a recent Centers for Disease Control and Prevention (CDC) report.
“We suspect SSPE cases will rise again as well. This is sad because this horrible disease can be prevented by vaccination. But now we are in the position to study SSPE with modern, genetic sequencing technology and learn more about it,” says Iris Yousaf, co-lead author of the study and a fifth-year Ph.D. candidate at Mayo Clinic Graduate School of Biomedical Sciences.
Dr Cattaneo and Yousaf had a unique research opportunity through a collaboration with the CDC. They studied the brain of a person who had contracted measles as a child and had succumbed to SSPE years later as an adult.
They investigated 15 specimens from different regions of the brain and conducted genetic sequencing on each region to piece together the puzzle of how the measles virus mutated and spread.
The researchers discovered that, after the measles virus entered the brain, its genome began to mutate in harmful ways over successive generations, creating a population of varied genomes.
“In this population, two specific genomes had a combination of characteristics that worked together to promote virus spread from the initial location of the infection – the frontal cortex of the brain – out to colonise the entire organ,” says Dr Cattaneo.
The next steps in this research are to understand how specific mutations favour virus spread in the brain. These studies will be done in cultivated brain cells brain organoids. This knowledge may help in creating effective antiviral drugs to combat virus spread in the brain. However, pharmacological intervention in advanced disease stages is challenging, and preventing SSPE through measles vaccination remains the best method.
It has long been known that people with diabetes are at a substantially increased risk of developing severe lung disease if they become infected with viruses such as influenza, as well as other pathogens. When the COVID-19 pandemic started in early 2020, it became even more important to understand this mysterious phenomenon. It became clear that people with diabetes were at a significantly higher risk of coming down with severe, even fatal, lung disease after developing severe COVID, but no one understood why. In fact, some 35% of the pandemic’s COVID mortalities had diabetes.
Now, research conducted at the Weizmann Institute of Science and published in Nature has revealed how, in diabetics, high levels of blood sugar disrupt the function of key cell subsets in the lungs that regulate the immune response. It also identifies a potential strategy for reversing this susceptibility and saving lives.
Prof. Eran Elinav‘s team in his lab at Weizmann, headed by Drs. Samuel Nobs, Aleksandra Kolodziejczyk and Suhaib K. Abdeen, subjected multiple mouse models of types 1 and 2 diabetes to a variety of viral lung infections. Just as in diabetic humans, in all these models the diabetic mice developed a severe, fatal lung infection following exposure to lung pathogens such as influenza. The immune reaction, which in nondiabetics eliminates the infection and drives tissue healing, was severely impaired in the diabetic mice, leading to uncontrolled infection, lung damage and eventual death.
Next, to decode the basis of this heightened risk, the team performed an evaluation of gene expression on the level of individual cells, in more than 150 000 single lung cells of infected diabetic and nondiabetic mice. The researchers also performed an extensive array of experiments involving immune and metabolic mechanisms, as well as an in-depth assessment of immune cell gene expression in infected diabetic mice. In the diabetic mice they identified a dysfunction of certain lung dendritic cells, the immune cells that orchestrate a targeted immune response against pathogenic infection. “High blood sugar levels severely disrupt certain subsets of dendritic cells in the lung, preventing these gatekeepers from sending the molecular messages that activate the critically important immune response,” says Nobs, postdoctoral fellow and study first author. “As a result, the infection rages on, uncontrolled.”
Next, they explored ways to prevent the harmful effects of hyperglycaemia in lung dendritic cells, as a means of lowering the infection’s risk in diabetic animals. Indeed, tight control of glycaemic levels by insulin supplementation prompted the dendritic cells to regain their capacity to generate a protective immune response that could prevent the cascade of events leading to a severe, life-threatening viral lung infection. Alternatively, administration of small molecules reversing the sugar-induced regulatory impairment corrected the dendritic cells’ dysfunction and enabled them to generate a protective immune response despite the presence of hyperglycaemia.
“Correcting blood sugar levels, or using drugs to reverse the gene regulatory impairment induced by high sugar, enabled our team to get the dendritic cells’ function back to normal,” says Abdeen, a senior intern who co-supervised the study. “This was very exciting because it means that it might be possible to block diabetes-induced susceptibility to viral lung infections and their devastating consequences.”
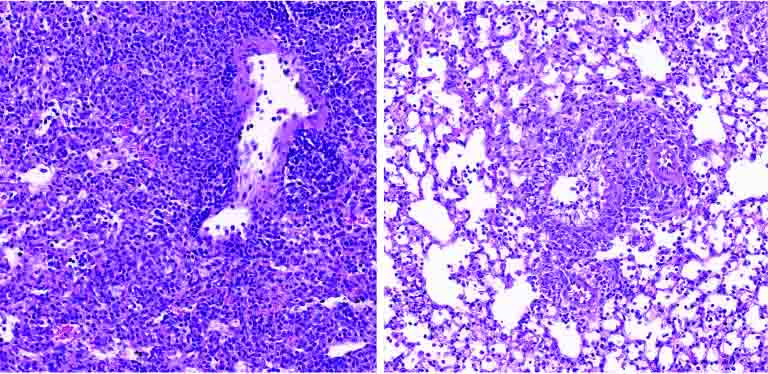
Lung tissue of a diabetic mouse (right) contains fewer immune cells (small purple dots) than that of a non-diabetic animal (left)
With over 500 million people around the world affected by diabetes, and with diabetes incidence expected to rise over the next decades, the new research has significant, promising clinical implications.
“Our findings provide, for the first time, an explanation as to why diabetics are more susceptible to respiratory infection,” Elinav says. “Controlling sugar levels may make it possible to reduce this pronounced diabetes-associated risk. In diabetic patients whose sugar levels are not easily normalized, small molecule drugs may correct the gene alterations caused by high sugar levels, potentially alleviating or even preventing severe lung infection. Local administration of such treatments by inhalation may minimize adverse effects while enhancing effectiveness, and merits future human clinical testing.”